140 results in Exploration of Neuroscience
Latest
Sort by :
- Latest
- Most Viewed
- Most Downloaded
- Most Cited
Open Access
Original Article
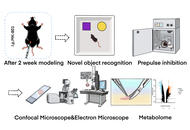
MK-801-induced cognitive dysfunction in a schizophrenia model: mechanistic links between interstitial fluid drainage impairment and neural metabolic disturbances
Xin Mao ... Ren Long
Published: July 02, 2026 Explor Neurosci. 2026;5:1006140
Open Access
Review
Type 2 diabetes in dementia and Alzheimer’s disease: Intertwined global health issues brewing on the horizon
Zsolt G. Venkei, Masha G. Savelieff
Published: July 01, 2026 Explor Neurosci. 2026;5:1006139

Open Access
Protocol
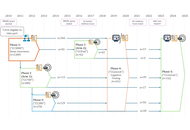
The Cambridge Centre for Ageing and Neuroscience (Cam-CAN) longitudinal study protocol: Phase 4 (“Enrichment”) and Phase 5 (“Rescan”)
Ina Demetriou ... Richard Henson
Published: June 29, 2026 Explor Neurosci. 2026;5:1006138
Open Access
Review
Thymoquinone in Alzheimer’s disease: experimental evidence and neuroprotective mechanisms
Jamil A. Chahrour ... Akram Hijazi
Published: May 14, 2026 Explor Neurosci. 2026;5:1006137
This article belongs to the special issue Medicinal Plants and Bioactive Phytochemicals in Neuroprotection (Vol II)

Open Access
Review
Protein aggregation in progressive myoclonus epilepsies and related syndromes
Eva Žerovnik
Published: May 08, 2026 Explor Neurosci. 2026;5:1006136
This article belongs to the special issue Advances in Epilepsy Research

Open Access
Original Article
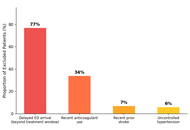
Stroke burden and epidemiological trends in Saudi Arabia: 1990–2021
Ahmed Abdulaziz Almohammadi
Published: April 27, 2026 Explor Neurosci. 2026;5:1006135
This article belongs to the special issue The Science of Ischemic Stroke
Open Access
Original Article
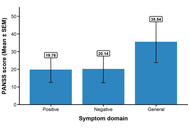
Redox-oxidative stress and micronutrients interplay in the clinical phenotype of schizophrenia in Nigerian subjects
Tolutope Adebimpe Oso ... Oluyemi Akinloye
Published: April 27, 2026 Explor Neurosci. 2026;5:1006134
Open Access
Review
Microbiota–mitochondria crosstalk in the gut–brain axis: a missing link in the etiology and treatment of major depressive disorder
Oluwagbenga Mayowa Adu ... Shukurat Joy Ajenikoko
Published: April 21, 2026 Explor Neurosci. 2026;5:1006133
This article belongs to the special issue Depression: From Pathophysiology to Treatment Innovation

Open Access
Review
Circadian astrocyte mitochondrial humanin regulates microglia and neuronal mitochondrial melatonergic pathway, with implications for aging and neurodegenerative conditions
George Anderson
Published: April 15, 2026 Explor Neurosci. 2026;5:1006132

Open Access
Review
Emerging insights in human brain and behavior from intracranial recordings
Ai Phuong S. Tong
Published: March 25, 2026 Explor Neurosci. 2026;5:1006131
This article belongs to the special issue Advances in Epilepsy Research
Open Access
Review
Fisetin in malignant nervous system tumors: molecular insights and translational advances
Ajay Kumar, Amita
Published: March 23, 2026 Explor Neurosci. 2026;5:1006130
This article belongs to the special issue Current Approaches to Malignant Tumors of the Nervous System

Open Access
Review
An exploratory narrative review of the symbiosis between intervention and patient education and how they improve pain-related disability
Kate Elizabeth Tordoff ... Mohamed Hassouna
Published: March 18, 2026 Explor Neurosci. 2026;5:1006129
Open Access
Review
Do new neurons grow in the adult human hippocampus? A review of the evidence
Maria Loumpourdi
Published: March 17, 2026 Explor Neurosci. 2026;5:1006128
Open Access
Review
BMAL1-PI3K/AKT crosstalk in ischemic injury and vascular repair: a circadian framework for neurovascular resilience
Mustafa C. Beker ... Ertugrul Kilic
Published: March 17, 2026 Explor Neurosci. 2026;5:1006127

Open Access
Review
Innovations in hydrocephalus modeling: bridging animal models, bioengineering platforms, and precision therapies
Ioannis Angelopoulos
Published: March 10, 2026 Explor Neurosci. 2026;5:1006126
Open Access
Retraction
Retraction: Extracellular vesicles in neurological disorders: emerging roles and underlying molecular mechanisms
Mst. Afsana Mimi, Md. Mahmudul Hasan
Published: February 08, 2026 Explor Neurosci. 2026;5:1006125
Open Access
Original Article
Tissue transglutaminase modulates pain but not neuronal survival after nerve injury
Gong-Wei Lyu ... Tie-Jun Sten Shi
Published: February 05, 2026 Explor Neurosci. 2026;5:1006124

Open Access
Original Article
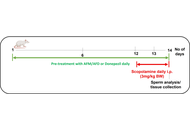
Restorative effects of Aframomum melegueta and Aframomum danielli-supplemented diets on sperm quality and testicular health following scopolamine-induced neurotoxicity in rats
Odunayo M. Agunloye ... Ganiyu Oboh
Published: February 01, 2026 Explor Neurosci. 2026;5:1006123
This article belongs to the special issue Medicinal Plants and Bioactive Phytochemicals in Neuroprotection (Vol II)
Open Access
Perspective
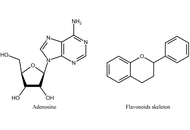
Perspectives on the use of flavonoids in glioblastoma treatment by targeting adenosine receptors
Katrin Sak
Published: January 22, 2026 Explor Neurosci. 2026;5:1006122
This article belongs to the special issue Current Approaches to Malignant Tumors of the Nervous System
Open Access
Review
Cerebral amyloid angiopathy: updates on pathophysiology, diagnosis, and management
Trinity Willsey ... Mo-Kyung Sin
Published: January 05, 2026 Explor Neurosci. 2026;5:1006121

Journal Information