




Editor's Picks
Open Access
Review
Advancing our understanding of schizophrenia: insights from recent research, emerging therapies, and future directions
Schizophrenia (SZ) is a complex psychiatric disorder characterized by disruptions in cognition, perception, and behavior, contributing significantly to the global burden of psychiatric disorders and necessitating ongoing research into its pathophysiology, diagnosis, and treatment. This narrative review explores recent insights into SZ research, highlighting the genetic, neurochemical, and neurodevelopmental factors that contribute to the disorder. Emerging evidence underscores the dynamic interplay between neurotransmitter imbalances, particularly involving dopamine, glutamate, and gamma-aminobutyric acid (GABA), and neuroinflammation, oxidative stress, and immune dysregulation in the pathophysiology of SZ. Neuroimaging, clinical staging models, and multi-omics technologies have deepened our understanding of structural and functional brain abnormalities, identifying potential biomarkers for early detection and subtyping. This has refined diagnostic frameworks and informed precision psychiatry approaches. Advances in pharmacological treatments, including trace amine-associated receptor 1 agonists, glutamatergic modulators, psychedelics, and anti-inflammatory agents, offer new therapeutic possibilities beyond conventional dopamine antagonists. Novel targets, such as N-methyl-D-aspartate (NMDA) receptor modulation and neuroprotective strategies, are also being explored to address negative and cognitive symptoms. Additionally, non-pharmacological interventions, such as neuromodulation techniques, digital therapeutics, and psychosocial interventions, are promising complementary strategies. Digital phenotyping, machine learning (ML), and artificial intelligence (AI)-driven tools enable real-time symptom tracking, early risk prediction, and personalized care delivery. Despite these advancements, challenges remain in early diagnosis, treatment adherence, and equitable access to mental health care, particularly in low-resource settings. Therefore, addressing these barriers requires interdisciplinary collaboration, public health education, and the integration of scalable, culturally sensitive, and AI-based mental health innovations. Future research should prioritize multi-omics integration, longitudinal and transdiagnostic studies, biomarker validation, and the real-world implementation of personalized interventions to improve outcomes and quality of life for individuals living with SZ.

Open Access
Review
Neuropathic pain: proposal of a mechanism-based treatment
Neuropathic pain, defined by the International Association for the Study of Pain as “pain caused by a lesion or disease of the somatosensory system”, has an estimated prevalence of 7–9.2% in the general population and is associated with poorer health-related quality of life than other types of pain. Diagnosis can be improved by the use of diagnostic algorithms, but treatment remains rather unsatisfactory, with only 30–40% of patients achieving an acceptable response. Some authors have suggested that the poor results in the treatment of neuropathic pain may be related to the different mechanisms present in each patient and have tried to correlate them with clinical characteristics in order to evaluate possible targeted treatments. This approach has been used in some studies evaluating the response to specific pharmacotherapies in clusters of patients, with encouraging results but still limited applicability to clinical practice. In this narrative review, we attempt to analyse the literature suggesting possible pathogenetic mechanisms manifested along the nociceptive pathway due to a lesion or disease of the nervous system; aware of the limitations of exploring such a wide field, we look for conditions that could be targeted by the available pharmacological or interventional treatment options. Functional changes may occur in the nociceptive system from the periphery to the cerebral cortex, in particular in the nociceptive terminals, along the first-order neuron and the dorsal root ganglion, at the first synapses, or at supraspinal levels. Clinical assessment is the first step in the study of anatomical and functional changes; the diagnostic hypothesis should be confirmed, if possible, by instrumental studies or diagnostic blocks or procedures to guide an individualised therapeutic algorithm from less to more invasive treatments.

Open Access
Review
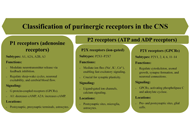
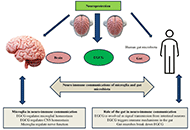
Mechanisms of astrocytic and microglial purinergic signaling in homeostatic regulation and implications for neurological disease
Purinergic signaling, mediated by ATP and adenosine receptors, plays a crucial role in cellular communication and homeostasis within the central nervous system (CNS), particularly by regulating synaptic activity, glial cell functions, and neuroplasticity. Glial cells, including astrocytes and microglia, contribute to both short-term processes, such as neurotransmission and neuroinflammation, and long-term functions, including synaptic remodeling, tissue repair, and behavioral adaptation. Dysregulation of purinergic signaling in these cells has been implicated in the pathogenesis of various neurodegenerative and neuropsychiatric disorders. This article explores the evolving concept of the synapse, highlighting the active role of glial cells in synaptic modulation and emphasizing the significance of purinergic signaling in synaptic function and responses to conditions such as injury and neurotoxicity. Specifically, it examines the roles of ATP and adenosine receptors—such as P2X4, P2X7, P2Y1, and P2Y12—in mediating key astrocytic and microglial functions, including neuroinflammation, phagocytosis, synaptic plasticity, and neuronal damage. Furthermore, the article discusses the involvement of purinergic receptors in neurological disorders such as epilepsy, Alzheimer’s disease, Parkinson’s disease, multiple sclerosis, ischemic stroke, Rett syndrome, and autism spectrum disorder, as well as potential therapeutic strategies targeting these receptors to mitigate inflammation, promote tissue repair, and improve clinical outcomes.
Articles
Latest
Most Viewed
Most Downloaded
Most Cited
Open Access
Review
Cognitive impairment after traumatic brain injury: mechanisms, clinical profiles, and implications for cognitive remediation and functional recovery
Giulio Verrienti ... Dario Tedesco
Published: August 04, 2026 Explor Neurosci. 2026;5:1006143

Open Access
Review
The “lactate window” hypothesis: exercise-induced lactate dynamics in neurometabolic remodeling and symptom-dimensional exercise prescription for depression
Jianda Kong
Published: August 03, 2026 Explor Neurosci. 2026;5:1006142
This article belongs to the special issue Depression: From Pathophysiology to Treatment Innovation

Open Access
Review
Exercise and brain health in long COVID: mechanisms and therapeutic implications for neuropsychiatric disorders
Giulio Verrienti
Published: July 28, 2026 Explor Neurosci. 2026;5:1006141

Open Access
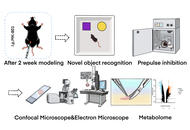
Original Article
MK-801-induced cognitive dysfunction in a schizophrenia model: mechanistic links between interstitial fluid drainage impairment and neural metabolic disturbances
Xin Mao ... Ren Long
Published: July 02, 2026 Explor Neurosci. 2026;5:1006140
Open Access
Review
Type 2 diabetes in dementia and Alzheimer’s disease: Intertwined global health issues brewing on the horizon
Zsolt G. Venkei, Masha G. Savelieff
Published: July 01, 2026 Explor Neurosci. 2026;5:1006139

Open Access
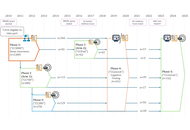
Protocol
The Cambridge Centre for Ageing and Neuroscience (Cam-CAN) longitudinal study protocol: Phase 4 (“Enrichment”) and Phase 5 (“Rescan”)
Ina Demetriou ... Richard Henson
Published: June 29, 2026 Explor Neurosci. 2026;5:1006138
Open Access
Review
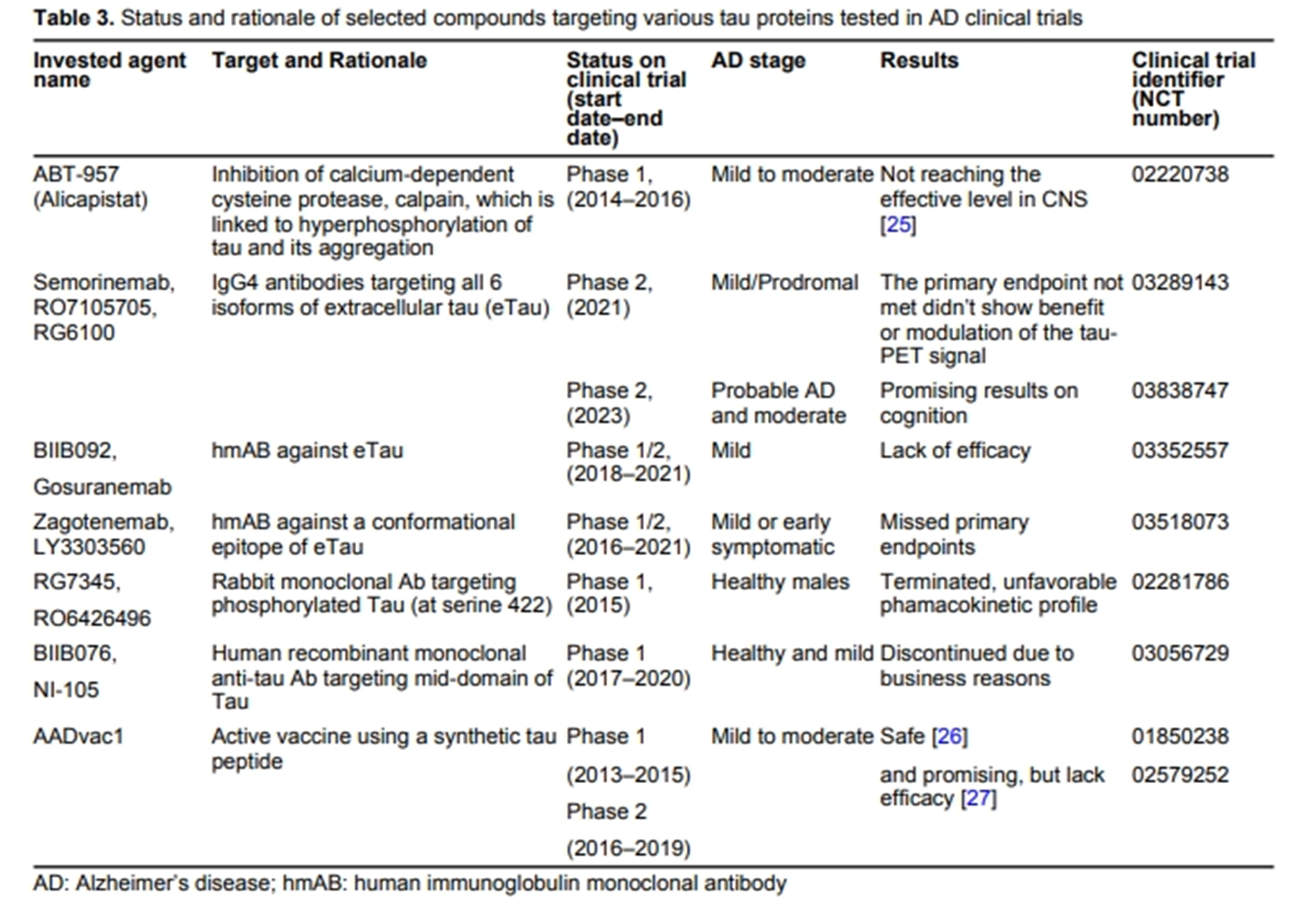
Current therapeutics for Alzheimer’s disease and clinical trials
Danqing Xiao, Chen Zhang
Published: June 27, 2024 Explor Neurosci. 2024;3:255–271
This article belongs to the special issue Alzheimer’s Disease
Open Access
Review
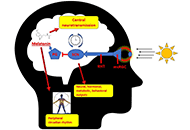
Effects mediated by melatonin and cortisol of artificial light and noise, alone and in combination, on sleep and health
Nahum M. Gabinet
Published: September 13, 2024 Explor Neurosci. 2024;3:382–417
This article belongs to the special issue Circadian Rhythm and Melatonin

Open Access
Review
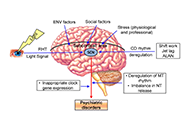
Impact of circadian clock dysfunction on human health
Saptadip Samanta, Sk Asif Ali
Published: September 29, 2022 Explor Neurosci. 2022;1:4–30
This article belongs to the special issue Circadian Rhythm and Melatonin

Open Access
Review
Neuropharmacologic modulation of the melatonergic system
Utku Aykan ... Canan Uluoglu
Published: December 22, 2023 Explor Neurosci. 2023;2:287–306
This article belongs to the special issue Circadian Rhythm and Melatonin
Open Access
Review
An intricate relationship between circadian rhythm dysfunction and psychiatric diseases
Saptadip Samanta, Debasis Bagchi
Published: August 23, 2024 Explor Neurosci. 2024;3:321–351
This article belongs to the special issue Circadian Rhythm and Melatonin
Open Access
Review
Negative environmental influences on the developing brain mediated by epigenetic modifications
Maya Komar-Fletcher ... Joanna Michalina Jurek
Published: September 28, 2023 Explor Neurosci. 2023;2:193–211
Open Access
Mini Review
Nutritional treatment with the ketogenic diet in children with refractory epilepsy: a narrative review
Srilaxmi Vityala ... Swathi Nenavath
Published: October 30, 2023 Explor Neurosci. 2023;2:245–250
This article belongs to the special issue Epilepsy
Open Access
Review
Current therapeutics for Alzheimer’s disease and clinical trials
Danqing Xiao, Chen Zhang
Published: June 27, 2024 Explor Neurosci. 2024;3:255–271
This article belongs to the special issue Alzheimer’s Disease
Open Access
Review
Stigma and psychosocial problems in patients with epilepsy
Kubra Yeni
Published: December 06, 2023 Explor Neurosci. 2023;2:251–263
This article belongs to the special issue Epilepsy

Open Access
Review
Impact of circadian clock dysfunction on human health
Saptadip Samanta, Sk Asif Ali
Published: September 29, 2022 Explor Neurosci. 2022;1:4–30
This article belongs to the special issue Circadian Rhythm and Melatonin
Open Access
Review
Negative environmental influences on the developing brain mediated by epigenetic modifications
Maya Komar-Fletcher ... Joanna Michalina Jurek
Published: September 28, 2023 Explor Neurosci. 2023;2:193–211
Open Access
Mini Review
Neuroprotective compounds from three common medicinal plants of West Bengal, India: a mini review
Suvendu Ghosh ... Debosree Ghosh
Published: December 26, 2023 Explor Neurosci. 2023;2:307–317
This article belongs to the special issue Medicinal Plants and Bioactive Phytochemicals in Neuroprotection

Open Access
Review
Current therapeutics for Alzheimer’s disease and clinical trials
Danqing Xiao, Chen Zhang
Published: June 27, 2024 Explor Neurosci. 2024;3:255–271
This article belongs to the special issue Alzheimer’s Disease
Open Access
Review
Stigma and psychosocial problems in patients with epilepsy
Kubra Yeni
Published: December 06, 2023 Explor Neurosci. 2023;2:251–263
This article belongs to the special issue Epilepsy
Open Access
Review
Impact of circadian clock dysfunction on human health
Saptadip Samanta, Sk Asif Ali
Published: September 29, 2022 Explor Neurosci. 2022;1:4–30
This article belongs to the special issue Circadian Rhythm and Melatonin
Open Access
Review
Connecting the ends: signaling via receptor tyrosine kinases and cytoskeletal degradation in neurodegeneration
Priyanka Sengupta ... Debashis Mukhopadhyay
Published: February 20, 2024 Explor Neurosci. 2024;3:1–26
This article belongs to the special issue Alzheimer’s Disease

Open Access
Review
Neuroprotective insights into epigallocatechin gallate (EGCG) for neurodegenerative disorders
Neha Kamboj ... Rahul Kumar
Published: February 24, 2025 Explor Neurosci. 2025;4:100673
This article belongs to the special issue Medicinal Plants and Bioactive Phytochemicals in Neuroprotection
Open Access
Review
Neuropharmacologic modulation of the melatonergic system
Utku Aykan ... Canan Uluoglu
Published: December 22, 2023 Explor Neurosci. 2023;2:287–306
This article belongs to the special issue Circadian Rhythm and Melatonin
Special Issues
Ongoing Special lssues
Completed Special lssues
Medicinal Plants and Bioactive Phytochemicals in Neuroprotection (Vol II)
Guest Editor: Prof. Marcello Iriti
Submission Deadline: July 31, 2026
Published Articles: 2
Depression: From Pathophysiology to Treatment Innovation
Guest Editors: Prof. Dirk M. Hermann; Dr. Ayan Mohamud Yusuf
Submission Deadline: December 31, 2026
Published Articles: 2
The Science of Ischemic Stroke
Guest Editor: Sheng-Tao Hou
Submission Deadline: July 31, 2026
Published Articles: 1
Advances in Parkinson's Disease Research: From Underlying Mechanisms to Novel Therapeutic Targets and Biodiagnostics
Guest Editor: Prof. Ludmilla A. Morozova-Roche
Submission Deadline: July 31, 2026
Published Articles: 0
Progress in Alzheimer's disease research: etiology, molecular mechanisms involved in disease progression, and advances in therapies aimed at slowing or reversing neurodegeneration
Guest Editor: Prof. Ryszard Pluta
Submission Deadline: December 31, 2026
Published Articles: 4
Advances in Epilepsy Research
Guest Editor: Prof. Jinwei Zhang
Submission Deadline: October 31, 2026
Published Articles: 7


Membership




Journal Information
Journal Indexing
Journal Metrics
Speed


From Submission to First Decision: 4 days
From First Decision to Acceptance: 83 days
From Acceptance to Publication: 30 days
Article Usage (total)
Views: 1,271,030
Downloads: 11,626
Acceptance Rate
34%; 2025
44%; 2024
41%; 2023

 Title: Unravelling the interplaybetween #Harmattan wind andbaroreflex functions: implicationon environmental health andcardiovascular #pathophys
Title: Unravelling the interplaybetween #Harmattan wind andbaroreflex functions: implicationon environmental health andcardiovascular #pathophysFollow the Journal



