









Aim:
Attention deficit hyperactivity disorder (ADHD) is a common condition impacting approximately 5% of children and 3–4% of adults in the United Kingdom (UK). While it cannot be cured, treatment has been shown to positively impact the difficulties associated with ADHD. However, ADHD is widely underdiagnosed and undertreated in the UK. This paper reports the results of a model developed to estimate pharmacological treatment rates by area across National Health Service (NHS) integrated care systems (ICSs) in England, health boards in Scotland and Wales, and health & social care trusts (HSCTs) in Northern Ireland.
Methods:
The model used the UK general population and ADHD prevalence data to estimate the number of patients with ADHD in each area. Prescription data for medicines licensed for the treatment of ADHD were then used to estimate the number of patients who are untreated and treated, and the percentage treatment rates by area. The analysis was descriptive, focusing on quantifying geographic variation in treatment rates.
Results:
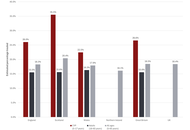
Nationally, the estimated proportions of children and young people (CYP; 5–17 years) and adults (18–65 years) treated were 26.6% and 15.6%, respectively, of the expected ADHD populations. Treatment rates by ICS or health board in England, Scotland, and Wales ranged from 11.7% to 60.6% for the CYP population and 8.6% to 24.8% for the adult population (data for Northern Ireland were not available by age group). Overall treatment rates (ages 5–65 years) in Northern Ireland ranged from 6.7% in the lowest-ranking HSCT to 31.1% in the highest-ranking HSCT.
Conclusions:
In the UK, there is currently a high degree of geographic variation across all NHS systems and a generally low level of treatment of ADHD, especially in adults. Up to a 4.6-fold difference in pharmacological treatment rates was observed between NHS service provider areas.
Aim:
Attention deficit hyperactivity disorder (ADHD) is a common condition impacting approximately 5% of children and 3–4% of adults in the United Kingdom (UK). While it cannot be cured, treatment has been shown to positively impact the difficulties associated with ADHD. However, ADHD is widely underdiagnosed and undertreated in the UK. This paper reports the results of a model developed to estimate pharmacological treatment rates by area across National Health Service (NHS) integrated care systems (ICSs) in England, health boards in Scotland and Wales, and health & social care trusts (HSCTs) in Northern Ireland.
Methods:
The model used the UK general population and ADHD prevalence data to estimate the number of patients with ADHD in each area. Prescription data for medicines licensed for the treatment of ADHD were then used to estimate the number of patients who are untreated and treated, and the percentage treatment rates by area. The analysis was descriptive, focusing on quantifying geographic variation in treatment rates.
Results:
Nationally, the estimated proportions of children and young people (CYP; 5–17 years) and adults (18–65 years) treated were 26.6% and 15.6%, respectively, of the expected ADHD populations. Treatment rates by ICS or health board in England, Scotland, and Wales ranged from 11.7% to 60.6% for the CYP population and 8.6% to 24.8% for the adult population (data for Northern Ireland were not available by age group). Overall treatment rates (ages 5–65 years) in Northern Ireland ranged from 6.7% in the lowest-ranking HSCT to 31.1% in the highest-ranking HSCT.
Conclusions:
In the UK, there is currently a high degree of geographic variation across all NHS systems and a generally low level of treatment of ADHD, especially in adults. Up to a 4.6-fold difference in pharmacological treatment rates was observed between NHS service provider areas.
DOI: https://doi.org/10.37349/ent.2026.1004163
This article belongs to the special issue Advances in the Pathogenesis, Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder
Neurodegenerative and neurodevelopmental neurological disorders represent a growing global health burden, characterized by progressive neuronal dysfunction, cognitive decline, and impaired functional outcomes. Increasing evidence highlights neuroinflammation as a central pathophysiological mechanism linking mitochondrial dysfunction, oxidative stress, microbiota dysbiosis, and synaptic impairment across diverse neurological conditions. This narrative review was conducted using a structured literature search approach, incorporating major biomedical databases to enhance transparency and reproducibility. This review synthesizes contemporary evidence on mechanistic pathways underlying neuroinflammation-mediated neurodegeneration and critically evaluates emerging neuroprotective therapeutic strategies. Particular emphasis is placed on mitochondrial transfer approaches, novel circulating and imaging biomarkers, and integrative neurotechnological innovations such as artificial intelligence-driven neuroimaging analytics. While several therapeutic approaches demonstrate promise in preclinical models, most remain at early experimental or translational stages, with limited validation in large-scale human studies. Current findings suggest that targeting neuroimmune signaling cascades, restoring mitochondrial bioenergetics, and modulating gut-brain axis interactions may provide synergistic neuroprotective benefits. The review proposes a multidimensional precision-medicine framework incorporating biomarker-guided therapeutic selection and interdisciplinary care models. Future research priorities include longitudinal biomarker validation, randomized clinical trials of mitochondrial-based therapies, and integration of digital neurodiagnostic platforms to enhance early disease detection. Despite these advances, significant gaps remain in clinical translation, standardization of biomarkers, and long-term therapeutic safety, necessitating cautious interpretation of emerging evidence.
Neurodegenerative and neurodevelopmental neurological disorders represent a growing global health burden, characterized by progressive neuronal dysfunction, cognitive decline, and impaired functional outcomes. Increasing evidence highlights neuroinflammation as a central pathophysiological mechanism linking mitochondrial dysfunction, oxidative stress, microbiota dysbiosis, and synaptic impairment across diverse neurological conditions. This narrative review was conducted using a structured literature search approach, incorporating major biomedical databases to enhance transparency and reproducibility. This review synthesizes contemporary evidence on mechanistic pathways underlying neuroinflammation-mediated neurodegeneration and critically evaluates emerging neuroprotective therapeutic strategies. Particular emphasis is placed on mitochondrial transfer approaches, novel circulating and imaging biomarkers, and integrative neurotechnological innovations such as artificial intelligence-driven neuroimaging analytics. While several therapeutic approaches demonstrate promise in preclinical models, most remain at early experimental or translational stages, with limited validation in large-scale human studies. Current findings suggest that targeting neuroimmune signaling cascades, restoring mitochondrial bioenergetics, and modulating gut-brain axis interactions may provide synergistic neuroprotective benefits. The review proposes a multidimensional precision-medicine framework incorporating biomarker-guided therapeutic selection and interdisciplinary care models. Future research priorities include longitudinal biomarker validation, randomized clinical trials of mitochondrial-based therapies, and integration of digital neurodiagnostic platforms to enhance early disease detection. Despite these advances, significant gaps remain in clinical translation, standardization of biomarkers, and long-term therapeutic safety, necessitating cautious interpretation of emerging evidence.
DOI: https://doi.org/10.37349/ent.2026.1004162
This article belongs to the special issue Neuro-Inflammation as a Target in the Design of Multifunctional Drug Candidates for Neurodegenerative Diseases
Aim:
Identify new genetic variants linked to neurodevelopmental disorders to be used in routine genetic diagnostics.
Methods:
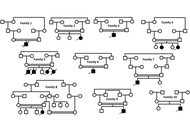
Whole exome sequencing (WES) was used for ten unrelated families from Jordan characterized by one or two affected members with neurodevelopmental disorders (NDDs), in which the parents are consanguineous in nine families.
Results:
Ten variants are identified in this study; one variant per family. Eight variants are identified by cross-link with the pathogenic variants in ClinVar and in our in-house database, and two variants are identified for the first time. Nine of the total identified variants are homozygous in the nine consanguineous families and one variant is heterozygous in the non-consanguineous family. Three of the identified variants were previously reported in unrelated Jordanian families compared to the families in this study. These three variants are NM_018359.5:c.344T>A;p.Val115Glu in the gene UFSP2, NM_000487.6:c.256C>G;p.Arg86Gly in the gene ARSA and NM_017882.3:c.144G>A;p.Trp48* in the gene CLN6. The variants that are identified for the first time are splicing variants; splice donor variant NM_000433.4:c.366+1G>C in the gene NCF2 and splice acceptor variant NM_000191.3:c.498-1G>A in the gene HMGCL.
Conclusions:
The results of this study stress the importance of continuous research using WES for NDDs in Jordan to identify new variants.
Aim:
Identify new genetic variants linked to neurodevelopmental disorders to be used in routine genetic diagnostics.
Methods:
Whole exome sequencing (WES) was used for ten unrelated families from Jordan characterized by one or two affected members with neurodevelopmental disorders (NDDs), in which the parents are consanguineous in nine families.
Results:
Ten variants are identified in this study; one variant per family. Eight variants are identified by cross-link with the pathogenic variants in ClinVar and in our in-house database, and two variants are identified for the first time. Nine of the total identified variants are homozygous in the nine consanguineous families and one variant is heterozygous in the non-consanguineous family. Three of the identified variants were previously reported in unrelated Jordanian families compared to the families in this study. These three variants are NM_018359.5:c.344T>A;p.Val115Glu in the gene UFSP2, NM_000487.6:c.256C>G;p.Arg86Gly in the gene ARSA and NM_017882.3:c.144G>A;p.Trp48* in the gene CLN6. The variants that are identified for the first time are splicing variants; splice donor variant NM_000433.4:c.366+1G>C in the gene NCF2 and splice acceptor variant NM_000191.3:c.498-1G>A in the gene HMGCL.
Conclusions:
The results of this study stress the importance of continuous research using WES for NDDs in Jordan to identify new variants.
DOI: https://doi.org/10.37349/ent.2026.1004161
This article belongs to the special issue Advances in the Pathogenesis, Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder
Aim:
This study aimed to redefine post-stress depressive pathogenesis through a novel five-disease multimorbidity trajectory model (brain1-coronary-brain2-gastro-enteric; B1CB2GE) and to evaluate the multifunctional anchoring effects of Bupleurum chinense Shugan-San (BSS) and its absorbed compounds (ACs), including meranzin hydrate (MH), in AFS (acute forced swimming) male Sprague-Dawley rats.
Methods:
Temporal multimorbidity trajectories of B1CB2GE clusters were established in AFS rats and compared with single-disease models using 10 integrative analytic methods, including dynamic cluster trajectory modeling, biochemical profiling, and pharmacokinetic-pharmacodynamic (PK-PD) correlation analyses. A multi-cell experiment was used as a proxy for the in vivo system, whereas H-ECs (H2O2-treated endothelial cells) were used as a proxy for the multicellular system. Circulatory biomarkers related to oxidative, endothelial, and inflammatory (OEI) impairment, brain-derived neurotrophic factor (BDNF) levels, and cecal butyrate contents were measured. The role of the ghrelin (Ghr) receptor was examined using the antagonist D-Lys3-GHRP-6 (D-Lys). Forced-swim test, gastric emptying, enteric transit, and coronary flow were used to characterize post-AFS multimorbidity trajectory phenotypes in animals.
Results:
Fifteen minutes after AFS, distinct temporal B1CB2GE multimorbidity clusters emerged with normalized ranking values: G 15.31 > B2 1.17 > B1 0.85 > C 0.49 > E 0.32. These clusters were accurately anchored by BSS and its five tailored sets of 1–10 ACs, demonstrating multifunctional modulation ranging from 53.23% to 156.32%, with optimal anchoring efficiency of 96.37–104.14%. MH, a representative multifunctional compound, exhibited the strongest prokinetic and OEI-restorative effects, elevating BDNF and cecal butyrate levels. These therapeutic effects were abolished by D-Lys, confirming a Ghr-dependent mechanism.
Conclusions:
This study introduces a multimorbidity trajectory framework (B1CB2GE) for modeling post-stress depression and demonstrates that Shugan-like herbal formulas such as BSS effectively anchor dynamic multimorbidity progression via multifunctional compounds like MH. These findings provide a systems-pharmacology basis for understanding and treating complex comorbid depressive disorders through multifunctional anchoring herbal therapeutics.
Aim:
This study aimed to redefine post-stress depressive pathogenesis through a novel five-disease multimorbidity trajectory model (brain1-coronary-brain2-gastro-enteric; B1CB2GE) and to evaluate the multifunctional anchoring effects of Bupleurum chinense Shugan-San (BSS) and its absorbed compounds (ACs), including meranzin hydrate (MH), in AFS (acute forced swimming) male Sprague-Dawley rats.
Methods:
Temporal multimorbidity trajectories of B1CB2GE clusters were established in AFS rats and compared with single-disease models using 10 integrative analytic methods, including dynamic cluster trajectory modeling, biochemical profiling, and pharmacokinetic-pharmacodynamic (PK-PD) correlation analyses. A multi-cell experiment was used as a proxy for the in vivo system, whereas H-ECs (H2O2-treated endothelial cells) were used as a proxy for the multicellular system. Circulatory biomarkers related to oxidative, endothelial, and inflammatory (OEI) impairment, brain-derived neurotrophic factor (BDNF) levels, and cecal butyrate contents were measured. The role of the ghrelin (Ghr) receptor was examined using the antagonist D-Lys3-GHRP-6 (D-Lys). Forced-swim test, gastric emptying, enteric transit, and coronary flow were used to characterize post-AFS multimorbidity trajectory phenotypes in animals.
Results:
Fifteen minutes after AFS, distinct temporal B1CB2GE multimorbidity clusters emerged with normalized ranking values: G 15.31 > B2 1.17 > B1 0.85 > C 0.49 > E 0.32. These clusters were accurately anchored by BSS and its five tailored sets of 1–10 ACs, demonstrating multifunctional modulation ranging from 53.23% to 156.32%, with optimal anchoring efficiency of 96.37–104.14%. MH, a representative multifunctional compound, exhibited the strongest prokinetic and OEI-restorative effects, elevating BDNF and cecal butyrate levels. These therapeutic effects were abolished by D-Lys, confirming a Ghr-dependent mechanism.
Conclusions:
This study introduces a multimorbidity trajectory framework (B1CB2GE) for modeling post-stress depression and demonstrates that Shugan-like herbal formulas such as BSS effectively anchor dynamic multimorbidity progression via multifunctional compounds like MH. These findings provide a systems-pharmacology basis for understanding and treating complex comorbid depressive disorders through multifunctional anchoring herbal therapeutics.
DOI: https://doi.org/10.37349/ent.2026.1004159
Aim:
Spinal cord injury (SCI) disrupts autonomic regulation of the gastrointestinal tract, resulting in altered motility, microbial dysbiosis, and decreased production of short-chain fatty acids such as butyrate, a metabolite with neuroprotective properties. This study aimed to evaluate the effects of SCI level and severity on gut microbiota composition and butyrate concentration, and to determine the impact of symbiotic supplementation with Enterococcus faecium and agave inulin on microbial and metabolic recovery.
Methods:
Twenty female Sprague Dawley rats were randomized into five groups: Sham, thoracic five moderate (T5M), thoracic five severe (T5S), thoracic nine moderate (T9M), and thoracic nine severe (T9S). Fecal samples were collected four weeks post-injury and again after four weeks of daily symbiotic administration. Butyrate levels were quantified by gas chromatography, and microbial composition was analyzed by 16S ribosomal RNA (16S rRNA) sequencing (V3–V4 region). Locomotor recovery was assessed weekly using the Basso, Beattie, and Bresnahan (BBB) scale.
Results:
All SCI groups displayed significant dysbiosis compared with Sham, characterized by decreased relative abundance of butyrate-producing genera such as Clostridium at week four, as confirmed in the main dataset. Following symbiotic supplementation, Bifidobacterium, Lactobacillus, and Clostridium levels showed partial restoration, although responses varied by injury site and severity. The T9M group demonstrated the most consistent recovery of butyrate-producing taxa; however, butyrate concentration decreased after treatment, while T9S showed a significant increase in butyrate concentration, and T5S exhibited minimal change. Motor recovery was greatest in T9M, followed by T9S and T5M, with no significant improvement in T5S.
Conclusions:
SCI level and severity strongly influenced microbial dysbiosis, butyrate metabolism, and motor recovery. Symbiotic supplementation partially restored butyrate-producing bacterial taxa, with the most pronounced metabolic and functional benefits observed in the T9M group. These findings support a level-dependent role of gut-brain axis modulation as a potential therapeutic strategy after SCI.
Aim:
Spinal cord injury (SCI) disrupts autonomic regulation of the gastrointestinal tract, resulting in altered motility, microbial dysbiosis, and decreased production of short-chain fatty acids such as butyrate, a metabolite with neuroprotective properties. This study aimed to evaluate the effects of SCI level and severity on gut microbiota composition and butyrate concentration, and to determine the impact of symbiotic supplementation with Enterococcus faecium and agave inulin on microbial and metabolic recovery.
Methods:
Twenty female Sprague Dawley rats were randomized into five groups: Sham, thoracic five moderate (T5M), thoracic five severe (T5S), thoracic nine moderate (T9M), and thoracic nine severe (T9S). Fecal samples were collected four weeks post-injury and again after four weeks of daily symbiotic administration. Butyrate levels were quantified by gas chromatography, and microbial composition was analyzed by 16S ribosomal RNA (16S rRNA) sequencing (V3–V4 region). Locomotor recovery was assessed weekly using the Basso, Beattie, and Bresnahan (BBB) scale.
Results:
All SCI groups displayed significant dysbiosis compared with Sham, characterized by decreased relative abundance of butyrate-producing genera such as Clostridium at week four, as confirmed in the main dataset. Following symbiotic supplementation, Bifidobacterium, Lactobacillus, and Clostridium levels showed partial restoration, although responses varied by injury site and severity. The T9M group demonstrated the most consistent recovery of butyrate-producing taxa; however, butyrate concentration decreased after treatment, while T9S showed a significant increase in butyrate concentration, and T5S exhibited minimal change. Motor recovery was greatest in T9M, followed by T9S and T5M, with no significant improvement in T5S.
Conclusions:
SCI level and severity strongly influenced microbial dysbiosis, butyrate metabolism, and motor recovery. Symbiotic supplementation partially restored butyrate-producing bacterial taxa, with the most pronounced metabolic and functional benefits observed in the T9M group. These findings support a level-dependent role of gut-brain axis modulation as a potential therapeutic strategy after SCI.
DOI: https://doi.org/10.37349/ent.2026.1004160
This article belongs to the special issue Role of Microbiota in Neurological Diseases
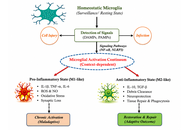
Microglia, the resident immune cells of the central nervous system, are increasingly recognized as key regulators of neural development, synaptic plasticity, and behavior. In addition to their classical role in immune surveillance, microglia actively shape neuronal circuits and influence cognitive and emotional functions across the life span. Accumulating evidence now implicates aberrant or chronic microglial activation as a central mechanism underlying neuroinflammation-associated behavioral and cognitive disturbances in a wide range of neuropsychiatric disorders, including major depressive disorder, schizophrenia, autism spectrum disorder, posttraumatic stress disorder, and attention-deficit/hyperactivity disorder. This narrative review synthesizes preclinical and clinical findings linking dysregulated microglial activation to brain pathology of neuropsychiatric disorders, with particular emphasis on cytokine signaling, oxidative stress, synaptic remodeling, and gut–brain–microglia interactions. This review discusses how sustained microglial priming and excessive inflammatory responses disrupt neurotransmitter systems, impair synaptic integrity, and alter neural network connectivity in brain regions critical for emotion regulation, cognition, and social behavior. Advances in neuroimaging, including TSPO-PET and multimodal approaches, have enabled in vivo assessment of microglial activation in humans, strengthening translational relevance. Furthermore, this review evaluates emerging therapeutic strategies aimed at modulating microglial function, including pharmacological immunomodulators, CSF1R-based depletion and repopulation approaches, lifestyle interventions, and novel cell-based and vesicle-based therapies. Finally, this review highlights key translational challenges, particularly species-specific differences between mouse and human microglia, and proposes future directions for precision neuroimmune interventions. Collectively, the evidence reviewed here positions microglia as both mechanistic drivers and therapeutic targets in neuropsychiatric disorders rooted in chronic neuroinflammation.
Microglia, the resident immune cells of the central nervous system, are increasingly recognized as key regulators of neural development, synaptic plasticity, and behavior. In addition to their classical role in immune surveillance, microglia actively shape neuronal circuits and influence cognitive and emotional functions across the life span. Accumulating evidence now implicates aberrant or chronic microglial activation as a central mechanism underlying neuroinflammation-associated behavioral and cognitive disturbances in a wide range of neuropsychiatric disorders, including major depressive disorder, schizophrenia, autism spectrum disorder, posttraumatic stress disorder, and attention-deficit/hyperactivity disorder. This narrative review synthesizes preclinical and clinical findings linking dysregulated microglial activation to brain pathology of neuropsychiatric disorders, with particular emphasis on cytokine signaling, oxidative stress, synaptic remodeling, and gut–brain–microglia interactions. This review discusses how sustained microglial priming and excessive inflammatory responses disrupt neurotransmitter systems, impair synaptic integrity, and alter neural network connectivity in brain regions critical for emotion regulation, cognition, and social behavior. Advances in neuroimaging, including TSPO-PET and multimodal approaches, have enabled in vivo assessment of microglial activation in humans, strengthening translational relevance. Furthermore, this review evaluates emerging therapeutic strategies aimed at modulating microglial function, including pharmacological immunomodulators, CSF1R-based depletion and repopulation approaches, lifestyle interventions, and novel cell-based and vesicle-based therapies. Finally, this review highlights key translational challenges, particularly species-specific differences between mouse and human microglia, and proposes future directions for precision neuroimmune interventions. Collectively, the evidence reviewed here positions microglia as both mechanistic drivers and therapeutic targets in neuropsychiatric disorders rooted in chronic neuroinflammation.
DOI: https://doi.org/10.37349/ent.2026.1004158
This article belongs to the special issue Defending the Brain and the Mind: Exploring Neuroprotective Therapies for Mental Health Disorders
This Perspective explores why hyperbaric oxygen therapy (HBOT) deserves closer clinical and scientific attention as a possible treatment for ischemic stroke and a potential neuroprotective strategy in chronic central nervous system disorders, especially multiple sclerosis and other progressive or age-related neurological conditions. While HBOT is not yet widely accepted for these indications, three factors justify reconsideration: its strong safety profile, a biologically plausible mechanistic rationale, and recurrent signals of benefit from selected neurological studies. We review HBOT’s historical development, current accepted indications, and evidence that adverse effects are generally mild, uncommon, and reversible under modern protocols. In neurology, efficacy remains unproven, yet interest persists due to preliminary findings and repeated patient-reported improvements. A central argument is that the main barrier to progress is not safety, but evidence generation. Conventional randomized controlled trials face major challenges: difficult blinding, wide variation in dosing protocols, and uncertainty about meaningful outcomes in chronic neurological disease. Moreover, HBOT is non-patentable, which limits commercial investment and leaves a potentially valuable intervention underexplored. Mechanistically, we move beyond explanations centred solely on oxygen delivery or oxidative stress. As a working hypothesis, neurological benefits may partly arise from cumulative adaptive responses—including a rebound hormesis following repeated hyperoxic exposure. We conclude with a pragmatic research agenda: continuous, low-cost physiological monitoring in patients already receiving HBOT, coupled with a medium-term goal of adequately powered efficacy trials.
This Perspective explores why hyperbaric oxygen therapy (HBOT) deserves closer clinical and scientific attention as a possible treatment for ischemic stroke and a potential neuroprotective strategy in chronic central nervous system disorders, especially multiple sclerosis and other progressive or age-related neurological conditions. While HBOT is not yet widely accepted for these indications, three factors justify reconsideration: its strong safety profile, a biologically plausible mechanistic rationale, and recurrent signals of benefit from selected neurological studies. We review HBOT’s historical development, current accepted indications, and evidence that adverse effects are generally mild, uncommon, and reversible under modern protocols. In neurology, efficacy remains unproven, yet interest persists due to preliminary findings and repeated patient-reported improvements. A central argument is that the main barrier to progress is not safety, but evidence generation. Conventional randomized controlled trials face major challenges: difficult blinding, wide variation in dosing protocols, and uncertainty about meaningful outcomes in chronic neurological disease. Moreover, HBOT is non-patentable, which limits commercial investment and leaves a potentially valuable intervention underexplored. Mechanistically, we move beyond explanations centred solely on oxygen delivery or oxidative stress. As a working hypothesis, neurological benefits may partly arise from cumulative adaptive responses—including a rebound hormesis following repeated hyperoxic exposure. We conclude with a pragmatic research agenda: continuous, low-cost physiological monitoring in patients already receiving HBOT, coupled with a medium-term goal of adequately powered efficacy trials.
DOI: https://doi.org/10.37349/ent.2026.1004157
Aim:
To assess the effect of a synbiotic supplement composed of Enterococcus faecium and agave inulin on cognitive function in older adults with mild cognitive impairment (MCI).
Methods:
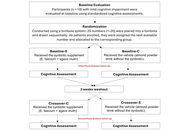
In a triple-blind randomized crossover trial, nineteen adults aged 64–85 years with MCI received either the synbiotic or an isocaloric vehicle for eight weeks, followed by a three-week washout and treatment crossover. Cognitive outcomes were assessed at baseline, after the first intervention, and after crossover using the Modified Mini-Mental State Examination (MMSE), Rey-Osterrieth Complex Figure Test (RCFT; copy and memory), and Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults (AERAC) self-efficacy scale. Paired and unpaired Student’s t-tests were used for statistical comparisons (p < 0.05).
Results:
The synbiotic group showed significant improvement relative to baseline across all domains: MMSE (p = 0.05), AERAC (p = 0.005), RCFT-copy (p = 0.03), and RCFT-memory (p = 0.03). Post-treatment comparisons between groups also favored the synbiotic, with significant differences in MMSE (p = 0.001), AERAC (p = 0.001), RCFT-copy (p = 0.0095), and RCFT-memory (p = 0.001). After crossover, cognitive gains were sustained and reproduced. MMSE scores reached 17.89 ± 1.45 in the synbiotic-first group versus 18.20 ± 0.63 in the control-first group (p < 0.001). RCFT-copy remained high (29.83 ± 4.18 vs. 29.52 ± 5.60, p = 0.0157), while RCFT-memory scores differed (17.56 ± 6.73 vs. 17.20 ± 3.29, p = 0.0005). AERAC scores continued to improve during crossover (82.60 ± 10.49 vs. 85.46 ± 8.28, p < 0.001). No adverse effects occurred.
Conclusions:
Synbiotic supplementation significantly improved global cognition, visuoconstructive ability, memory, and functional self-efficacy in older adults with MCI. Benefits persisted beyond the initial intervention and were replicated when the control group received the synbiotic, supporting its potential as a safe and effective strategy to mitigate age-related cognitive decline.
Aim:
To assess the effect of a synbiotic supplement composed of Enterococcus faecium and agave inulin on cognitive function in older adults with mild cognitive impairment (MCI).
Methods:
In a triple-blind randomized crossover trial, nineteen adults aged 64–85 years with MCI received either the synbiotic or an isocaloric vehicle for eight weeks, followed by a three-week washout and treatment crossover. Cognitive outcomes were assessed at baseline, after the first intervention, and after crossover using the Modified Mini-Mental State Examination (MMSE), Rey-Osterrieth Complex Figure Test (RCFT; copy and memory), and Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults (AERAC) self-efficacy scale. Paired and unpaired Student’s t-tests were used for statistical comparisons (p < 0.05).
Results:
The synbiotic group showed significant improvement relative to baseline across all domains: MMSE (p = 0.05), AERAC (p = 0.005), RCFT-copy (p = 0.03), and RCFT-memory (p = 0.03). Post-treatment comparisons between groups also favored the synbiotic, with significant differences in MMSE (p = 0.001), AERAC (p = 0.001), RCFT-copy (p = 0.0095), and RCFT-memory (p = 0.001). After crossover, cognitive gains were sustained and reproduced. MMSE scores reached 17.89 ± 1.45 in the synbiotic-first group versus 18.20 ± 0.63 in the control-first group (p < 0.001). RCFT-copy remained high (29.83 ± 4.18 vs. 29.52 ± 5.60, p = 0.0157), while RCFT-memory scores differed (17.56 ± 6.73 vs. 17.20 ± 3.29, p = 0.0005). AERAC scores continued to improve during crossover (82.60 ± 10.49 vs. 85.46 ± 8.28, p < 0.001). No adverse effects occurred.
Conclusions:
Synbiotic supplementation significantly improved global cognition, visuoconstructive ability, memory, and functional self-efficacy in older adults with MCI. Benefits persisted beyond the initial intervention and were replicated when the control group received the synbiotic, supporting its potential as a safe and effective strategy to mitigate age-related cognitive decline.
DOI: https://doi.org/10.37349/ent.2026.1004156
This article belongs to the special issue Role of Microbiota in Neurological Diseases
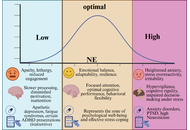
Norepinephrine (NE), a central catecholamine neurotransmitter synthesized primarily in the locus coeruleus (LC), plays a critical role in regulating arousal, attention, emotional processing, and stress responsiveness. While contemporary personality neuroscience has established the role of NE in acute psychological states, its contribution to stable personality traits remains underexplored. This review synthesizes neurobiological, psychological, genetic, and psychopharmacological evidence to propose a NE-personality continuum that links tonic and phasic dynamics of the LC-NE system to enduring individual differences in alertness, anxiety, and adaptability. Alertness is associated with optimal noradrenergic tone and efficient phasic signaling, which enhances the signal-to-noise ratio and attentional focus. Anxiety arises from chronic hyperactivation or dysregulated NE release, particularly involving excessive α1- and β-adrenergic receptor activity and impaired modulation from the prefrontal cortex. Adaptability denotes a harmonious interaction between the limbic system and prefrontal cortex, which facilitates cognitive flexibility and emotional regulation in response to changing environmental demands. The connection between NE activity and personality traits follows an inverted U-shaped pattern. Low tone leads to apathy and less engagement, moderate tone helps with resilience and optimal functioning, and high tone leads to hypervigilance and rigidity. This model combines findings from fundamental neuroscience and clinical research to provide a physiologically based framework for understanding how long-term variations in noradrenergic regulation affect personality traits, as described in established trait theories. The findings underline the feasibility of adding noradrenergic biomarkers and pharmaceutical therapies into clinical practice, as well as the importance of longitudinal and multimodal research to determine trait-level causality. This is especially important for understanding how to use these elements to improve treatment plans for personality disorders.
Norepinephrine (NE), a central catecholamine neurotransmitter synthesized primarily in the locus coeruleus (LC), plays a critical role in regulating arousal, attention, emotional processing, and stress responsiveness. While contemporary personality neuroscience has established the role of NE in acute psychological states, its contribution to stable personality traits remains underexplored. This review synthesizes neurobiological, psychological, genetic, and psychopharmacological evidence to propose a NE-personality continuum that links tonic and phasic dynamics of the LC-NE system to enduring individual differences in alertness, anxiety, and adaptability. Alertness is associated with optimal noradrenergic tone and efficient phasic signaling, which enhances the signal-to-noise ratio and attentional focus. Anxiety arises from chronic hyperactivation or dysregulated NE release, particularly involving excessive α1- and β-adrenergic receptor activity and impaired modulation from the prefrontal cortex. Adaptability denotes a harmonious interaction between the limbic system and prefrontal cortex, which facilitates cognitive flexibility and emotional regulation in response to changing environmental demands. The connection between NE activity and personality traits follows an inverted U-shaped pattern. Low tone leads to apathy and less engagement, moderate tone helps with resilience and optimal functioning, and high tone leads to hypervigilance and rigidity. This model combines findings from fundamental neuroscience and clinical research to provide a physiologically based framework for understanding how long-term variations in noradrenergic regulation affect personality traits, as described in established trait theories. The findings underline the feasibility of adding noradrenergic biomarkers and pharmaceutical therapies into clinical practice, as well as the importance of longitudinal and multimodal research to determine trait-level causality. This is especially important for understanding how to use these elements to improve treatment plans for personality disorders.
DOI: https://doi.org/10.37349/ent.2026.1004155
The NEUROD2 gene encodes a transcription factor essential for neuronal differentiation and cortical development. Pathogenic variants cause a rare autosomal dominant neurodevelopmental disorder with variable expressivity, typically presenting in early infancy with developmental delay, epilepsy, and behavioral abnormalities. We report a newborn girl carrying a de novo heterozygous missense variant NM_006160.4:c.790G>A, p.(Ala264Thr), located outside the canonical basic helix-loop-helix (bHLH) domain. Soon after birth, she presented respiratory depression, hypotonia, feeding difficulties, and electrographic seizures. Magnetic resonance imaging (MRI) showed subcortical white matter hyperintensity, and the electroencephalogram (EEG) revealed abnormal background activity. During follow-up, epilepsy was controlled, but neurodevelopmental delay with autistic features emerged. This case represents the earliest reported clinical onset associated with NEUROD2 variants and expands the phenotypic and mutational spectrum. It highlights that variants outside known hotspots can cause severe disease and supports including NEUROD2 in the differential diagnosis of neonatal neurological impairment.
The NEUROD2 gene encodes a transcription factor essential for neuronal differentiation and cortical development. Pathogenic variants cause a rare autosomal dominant neurodevelopmental disorder with variable expressivity, typically presenting in early infancy with developmental delay, epilepsy, and behavioral abnormalities. We report a newborn girl carrying a de novo heterozygous missense variant NM_006160.4:c.790G>A, p.(Ala264Thr), located outside the canonical basic helix-loop-helix (bHLH) domain. Soon after birth, she presented respiratory depression, hypotonia, feeding difficulties, and electrographic seizures. Magnetic resonance imaging (MRI) showed subcortical white matter hyperintensity, and the electroencephalogram (EEG) revealed abnormal background activity. During follow-up, epilepsy was controlled, but neurodevelopmental delay with autistic features emerged. This case represents the earliest reported clinical onset associated with NEUROD2 variants and expands the phenotypic and mutational spectrum. It highlights that variants outside known hotspots can cause severe disease and supports including NEUROD2 in the differential diagnosis of neonatal neurological impairment.
DOI: https://doi.org/10.37349/ent.2026.1004154
This article belongs to the special issue Neuroprotection in Pediatric Neurological Disorders: from Rare Diseases to Perinatal Brain Injury
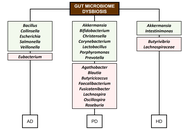
By individual examination, the present review provides an overview of the potential involvement of various human microbiomes, including the gut, oral, skin, and nasal, in the pathophysiology of neurodegenerative diseases. Research has demonstrated that gut microbiome dysbiosis is linked to the pathogenesis of neurodegenerative conditions, including Alzheimer’s, Parkinson’s, and Huntington’s diseases, through mechanisms involving microbial metabolites, neuroinflammation, amyloid aggregation, and altered neurotransmission. Emerging evidence suggests that the oral, skin, and nasal microbiomes may also influence neurodegenerative diseases through mechanisms such as microbial translocation, immune modulation, metabolite production, and interactions with the gut-brain axis. Although the potential of microbiome-based interventions for neurodegenerative diseases has been highlighted, several gaps remain, such as variability between human and animal models, a lack of standardized multi-omics approaches, and a limited understanding of individual microbial roles. Future studies should focus on clarifying the mechanisms by which dysbiosis in human host microbiomes impacts the pathophysiology of neurodegenerative diseases, identifying reliable biomarkers, and developing safe and effective microbiome-based therapies.
By individual examination, the present review provides an overview of the potential involvement of various human microbiomes, including the gut, oral, skin, and nasal, in the pathophysiology of neurodegenerative diseases. Research has demonstrated that gut microbiome dysbiosis is linked to the pathogenesis of neurodegenerative conditions, including Alzheimer’s, Parkinson’s, and Huntington’s diseases, through mechanisms involving microbial metabolites, neuroinflammation, amyloid aggregation, and altered neurotransmission. Emerging evidence suggests that the oral, skin, and nasal microbiomes may also influence neurodegenerative diseases through mechanisms such as microbial translocation, immune modulation, metabolite production, and interactions with the gut-brain axis. Although the potential of microbiome-based interventions for neurodegenerative diseases has been highlighted, several gaps remain, such as variability between human and animal models, a lack of standardized multi-omics approaches, and a limited understanding of individual microbial roles. Future studies should focus on clarifying the mechanisms by which dysbiosis in human host microbiomes impacts the pathophysiology of neurodegenerative diseases, identifying reliable biomarkers, and developing safe and effective microbiome-based therapies.
DOI: https://doi.org/10.37349/ent.2026.1004153
This article belongs to the special issue Role of Microbiota in Neurological Diseases
Short-chain fatty acids (SCFAs) are microbial-derived metabolites produced primarily through the fermentation of dietary fibre by the intestinal microbiota. Current evidence indicates that they play a key role in modulating nociception and pain processing across immune, metabolic, and neural pathways. The prevailing view that SCFAs suppress pain has been challenged by emerging evidence demonstrating that these same metabolites can also drive hyperalgesia. This apparent “SCFA paradox” persists because most studies have examined individual metabolites in isolation rather than considering them within their broader biological context. Here, we propose an integrative framework in which SCFAs function within a competitive receptor triad, and pain outcomes are dictated by the balance among three signalling axes: a pro-inflammatory immune axis driven by acetate acting through G protein-coupled receptor 43 (GPR43), a pro-resolutive metabolic axis mediated by butyrate via histone deacetylase (HDAC) inhibition and activation of GPR109A, and a direct neural sensing axis triggered by propionate through olfactory receptor 78 (OLFR78). Chronic pain, therefore, does not arise simply from the presence or absence of SCFAs, but from the pathological dominance of one of these axes shaped by specific dysbiosis profiles. This framework moves beyond correlation by providing a mechanistic basis for precision interventions designed to rebalance SCFA signalling, offering novel therapeutic opportunities for neuropathic and inflammatory pain conditions.
Short-chain fatty acids (SCFAs) are microbial-derived metabolites produced primarily through the fermentation of dietary fibre by the intestinal microbiota. Current evidence indicates that they play a key role in modulating nociception and pain processing across immune, metabolic, and neural pathways. The prevailing view that SCFAs suppress pain has been challenged by emerging evidence demonstrating that these same metabolites can also drive hyperalgesia. This apparent “SCFA paradox” persists because most studies have examined individual metabolites in isolation rather than considering them within their broader biological context. Here, we propose an integrative framework in which SCFAs function within a competitive receptor triad, and pain outcomes are dictated by the balance among three signalling axes: a pro-inflammatory immune axis driven by acetate acting through G protein-coupled receptor 43 (GPR43), a pro-resolutive metabolic axis mediated by butyrate via histone deacetylase (HDAC) inhibition and activation of GPR109A, and a direct neural sensing axis triggered by propionate through olfactory receptor 78 (OLFR78). Chronic pain, therefore, does not arise simply from the presence or absence of SCFAs, but from the pathological dominance of one of these axes shaped by specific dysbiosis profiles. This framework moves beyond correlation by providing a mechanistic basis for precision interventions designed to rebalance SCFA signalling, offering novel therapeutic opportunities for neuropathic and inflammatory pain conditions.
DOI: https://doi.org/10.37349/ent.2026.1004151
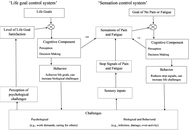
Explanations and treatment of fibromyalgia syndrome (FMS) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are controversial, and outcomes are poor. This paper describes sensation-suppression theory, a theory modelled on self-organizing control systems that are capable of adaptation in response to inputs and used in applications of artificial intelligence. The theory shows how the need to suppress inflammatory and other causes of pain or fatigue due to challenging circumstances sensitizes the neurological processing of pain and fatigue, thereby creating the amplified sensations and abnormal cognitions of central sensitivity syndromes. These syndromes are caused by errors in an evolutionarily early behavior-control mechanism of animals that comes into conflict with the later cognitive behavior-control mechanism of humans. Unlike the cognitive and current biological theories, the sensation-suppression theory explains both the personality and biological risk factors for central sensitivity syndromes and why onset is sometimes gradual and sometimes sudden. A specific form of autonomic dysregulation that could act as a new empirical test of the theory is suggested. Recovery is achieved by reversing the biological homeostatic dysregulation through a specific form of pacing where the person changes from one short, non-stressful activity to another, and where activity is calibrated to the level of illness and the patient’s current biological state. Recovery is hampered or prevented by systemic inflammation and lifestyle obligations. The theory provides a sympathetic narrative for the cause and treatment of FMS and ME/CFS and promotes a recovery lifestyle that prioritizes the needs of the patient. Prevention requires hearing what the body is saying.
Explanations and treatment of fibromyalgia syndrome (FMS) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are controversial, and outcomes are poor. This paper describes sensation-suppression theory, a theory modelled on self-organizing control systems that are capable of adaptation in response to inputs and used in applications of artificial intelligence. The theory shows how the need to suppress inflammatory and other causes of pain or fatigue due to challenging circumstances sensitizes the neurological processing of pain and fatigue, thereby creating the amplified sensations and abnormal cognitions of central sensitivity syndromes. These syndromes are caused by errors in an evolutionarily early behavior-control mechanism of animals that comes into conflict with the later cognitive behavior-control mechanism of humans. Unlike the cognitive and current biological theories, the sensation-suppression theory explains both the personality and biological risk factors for central sensitivity syndromes and why onset is sometimes gradual and sometimes sudden. A specific form of autonomic dysregulation that could act as a new empirical test of the theory is suggested. Recovery is achieved by reversing the biological homeostatic dysregulation through a specific form of pacing where the person changes from one short, non-stressful activity to another, and where activity is calibrated to the level of illness and the patient’s current biological state. Recovery is hampered or prevented by systemic inflammation and lifestyle obligations. The theory provides a sympathetic narrative for the cause and treatment of FMS and ME/CFS and promotes a recovery lifestyle that prioritizes the needs of the patient. Prevention requires hearing what the body is saying.
DOI: https://doi.org/10.37349/ent.2026.1004152
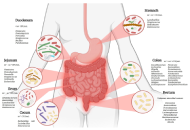
Growing evidence has directly linked the gastrointestinal tract, gut microbiota, and central nervous system, forming the gut-brain axis, a process that has been described as a key mechanism in regulating neurological processes. However, the presence of alterations in the composition of microorganisms in the digestive tract and dysbiosis has been linked to the activation of microglia, increased oxidative stress, alterations in the production of neurotransmitters, and exacerbation of neuroinflammation. These mechanisms have been associated with multiple pathologies and neurological conditions, and regulating them is key to the control of these diseases. In this context, various bacterial species play a neuroprotective role by promoting the integrity of the intestinal barrier, stimulating the synthesis of beneficial metabolites such as short-chain fatty acids (SCFAs), neurotransmitters, and modulating the inflammatory response. In addition, the characterization of these microbial profiles provides a broad perspective on understanding how changes in the microbiota contribute to the progression of neurological diseases. On the other hand, these new updates open up the possibility of designing personalised targeted therapeutic interventions that can regulate the gut microbiota and promote a neuroprotective and neuroregenerative environment. Another key point is that greater emphasis is placed on the need for more controlled clinical studies to validate efficacy and safety in humans, as well as knowledge of the mechanisms of action that make them possible. Finally, the modulation of the gut microbiota using probiotics, prebiotics, and postbiotics represents an innovative and effective opportunity to intervene in neuroimmune processes such as microglial activation, regulation of synaptic pruning, and neuroinflammatory pathways—processes implicated in various neurological diseases. In this context, this review integrates and analyzes the available evidence, highlighting potential interventions as treatments for these pathologies, as well as current limitations, to provide an updated framework to guide future research.
Growing evidence has directly linked the gastrointestinal tract, gut microbiota, and central nervous system, forming the gut-brain axis, a process that has been described as a key mechanism in regulating neurological processes. However, the presence of alterations in the composition of microorganisms in the digestive tract and dysbiosis has been linked to the activation of microglia, increased oxidative stress, alterations in the production of neurotransmitters, and exacerbation of neuroinflammation. These mechanisms have been associated with multiple pathologies and neurological conditions, and regulating them is key to the control of these diseases. In this context, various bacterial species play a neuroprotective role by promoting the integrity of the intestinal barrier, stimulating the synthesis of beneficial metabolites such as short-chain fatty acids (SCFAs), neurotransmitters, and modulating the inflammatory response. In addition, the characterization of these microbial profiles provides a broad perspective on understanding how changes in the microbiota contribute to the progression of neurological diseases. On the other hand, these new updates open up the possibility of designing personalised targeted therapeutic interventions that can regulate the gut microbiota and promote a neuroprotective and neuroregenerative environment. Another key point is that greater emphasis is placed on the need for more controlled clinical studies to validate efficacy and safety in humans, as well as knowledge of the mechanisms of action that make them possible. Finally, the modulation of the gut microbiota using probiotics, prebiotics, and postbiotics represents an innovative and effective opportunity to intervene in neuroimmune processes such as microglial activation, regulation of synaptic pruning, and neuroinflammatory pathways—processes implicated in various neurological diseases. In this context, this review integrates and analyzes the available evidence, highlighting potential interventions as treatments for these pathologies, as well as current limitations, to provide an updated framework to guide future research.
DOI: https://doi.org/10.37349/ent.2026.1004150
This article belongs to the special issue Role of Microbiota in Neurological Diseases
Neurodegenerative disorders represent a major and growing global health challenge, characterized by progressive neuronal loss, multifactorial pathophysiology, and limited disease-modifying pharmacological options. Increasing attention has therefore been directed toward non-pharmacological and integrative interventions as complementary strategies for neuroprotection and symptom management. These approaches target key mechanisms implicated in neurodegeneration, including oxidative stress, neuroinflammation, mitochondrial dysfunction, synaptic impairment, and dysregulated neuroplasticity. This narrative integrative review synthesizes current preclinical and clinical evidence on non-pharmacological interventions with demonstrated or emerging neuroprotective potential across major neurodegenerative disorders, including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and related conditions. The review focuses on four principal domains: physical activity and exercise, nutritional and dietary strategies, mind–body and psychosocial interventions, and sensory or neuromodulatory therapies. Collectively, these interventions influence convergent neurobiological pathways, including neurotrophic signaling, immune modulation, autonomic regulation, and gut–brain communication. Studies indicate that structured physical exercise enhances neurotrophic factor expression and mitochondrial resilience; dietary patterns rich in antioxidants and anti-inflammatory components mitigate oxidative damage and neuroinflammation; mind–body practices modulate stress-related neuroendocrine pathways and promote functional connectivity; and sensory or neuromodulatory interventions engage limbic and cortical networks relevant to cognition, mood, and motor control. Importantly, multimodal and integrative approaches appear to exert synergistic effects, aligning with the complex and systemic nature of neurodegenerative processes. Despite promising findings, challenges related to methodological heterogeneity, biomarker validation, and translational implementation persist. Future research should prioritize standardized protocols, objective neuroprotective endpoints, and personalized intervention frameworks supported by digital health technologies. Overall, non-pharmacological and integrative therapies represent a valuable, increasingly evidence-based component of comprehensive neuroprotective strategies, with significant potential to enhance quality of life and complement pharmacological treatments in the care of neurodegenerative diseases.
Neurodegenerative disorders represent a major and growing global health challenge, characterized by progressive neuronal loss, multifactorial pathophysiology, and limited disease-modifying pharmacological options. Increasing attention has therefore been directed toward non-pharmacological and integrative interventions as complementary strategies for neuroprotection and symptom management. These approaches target key mechanisms implicated in neurodegeneration, including oxidative stress, neuroinflammation, mitochondrial dysfunction, synaptic impairment, and dysregulated neuroplasticity. This narrative integrative review synthesizes current preclinical and clinical evidence on non-pharmacological interventions with demonstrated or emerging neuroprotective potential across major neurodegenerative disorders, including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and related conditions. The review focuses on four principal domains: physical activity and exercise, nutritional and dietary strategies, mind–body and psychosocial interventions, and sensory or neuromodulatory therapies. Collectively, these interventions influence convergent neurobiological pathways, including neurotrophic signaling, immune modulation, autonomic regulation, and gut–brain communication. Studies indicate that structured physical exercise enhances neurotrophic factor expression and mitochondrial resilience; dietary patterns rich in antioxidants and anti-inflammatory components mitigate oxidative damage and neuroinflammation; mind–body practices modulate stress-related neuroendocrine pathways and promote functional connectivity; and sensory or neuromodulatory interventions engage limbic and cortical networks relevant to cognition, mood, and motor control. Importantly, multimodal and integrative approaches appear to exert synergistic effects, aligning with the complex and systemic nature of neurodegenerative processes. Despite promising findings, challenges related to methodological heterogeneity, biomarker validation, and translational implementation persist. Future research should prioritize standardized protocols, objective neuroprotective endpoints, and personalized intervention frameworks supported by digital health technologies. Overall, non-pharmacological and integrative therapies represent a valuable, increasingly evidence-based component of comprehensive neuroprotective strategies, with significant potential to enhance quality of life and complement pharmacological treatments in the care of neurodegenerative diseases.
DOI: https://doi.org/10.37349/ent.2026.1004149
This article belongs to the special issue Breakthroughs in Mechanisms and Treatments for Neurodegenerative Diseases
Background:
Atrial fibrillation (AF) substantially increases the risk of ischemic stroke (IS), underscoring the need for effective anticoagulation strategies. Direct oral anticoagulants (DOACs) have largely supplanted vitamin K antagonists (VKAs) due to their favorable safety profile and ease of use. Factor XI (FXI) inhibitors, which target the intrinsic coagulation pathway, are emerging as potential alternatives that may offer reduced bleeding risk. This systematic review evaluates the efficacy and safety of FXI inhibitors compared with DOACs for stroke prevention in AF.
Methods:
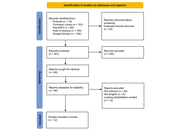
A total of 20 studies fulfilled the inclusion criteria, comprising 11 randomized controlled trials (RCTs), five systematic reviews or meta-analyses, and four narrative, cohort, or modeling studies. Eligible investigations compared FXI inhibitors with DOACs in patients diagnosed with AF. The primary outcomes assessed were stroke or systemic embolism, major bleeding, and all-cause mortality. Methodological quality was evaluated according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework, the revised Cochrane Risk of Bias 2 (RoB 2) tool for RCTs, and the Newcastle-Ottawa Scale (NOS).
Results:
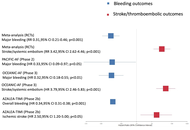
FXI inhibitors were associated with a significant reduction in major bleeding [relative risk (RR) 0.31; 95% confidence interval (CI) 0.21–0.46] and clinically relevant non-major bleeding (RR 0.66; 95% CI 0.47–0.93) compared with DOACs. Conversely, FXI inhibitors demonstrated an increased risk of stroke or systemic embolism (RR 3.17; 95% CI 2.18–4.62), as observed in the OCEANIC-AF trial [hazard ratio (HR) 3.79; 95% CI 2.46–5.83]. No significant difference was noted in all-cause mortality (RR 0.85; 95% CI 0.67–1.08). Limited evidence suggests that FXI inhibitors may also reduce bleeding-related hospitalizations.
Discussion:
FXI inhibitors provide a favorable bleeding profile but are less effective than DOACs for stroke prevention in patients with AF. Further long-term RCTs are warranted to delineate their role, particularly in populations at high risk of bleeding.
Background:
Atrial fibrillation (AF) substantially increases the risk of ischemic stroke (IS), underscoring the need for effective anticoagulation strategies. Direct oral anticoagulants (DOACs) have largely supplanted vitamin K antagonists (VKAs) due to their favorable safety profile and ease of use. Factor XI (FXI) inhibitors, which target the intrinsic coagulation pathway, are emerging as potential alternatives that may offer reduced bleeding risk. This systematic review evaluates the efficacy and safety of FXI inhibitors compared with DOACs for stroke prevention in AF.
Methods:
A total of 20 studies fulfilled the inclusion criteria, comprising 11 randomized controlled trials (RCTs), five systematic reviews or meta-analyses, and four narrative, cohort, or modeling studies. Eligible investigations compared FXI inhibitors with DOACs in patients diagnosed with AF. The primary outcomes assessed were stroke or systemic embolism, major bleeding, and all-cause mortality. Methodological quality was evaluated according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework, the revised Cochrane Risk of Bias 2 (RoB 2) tool for RCTs, and the Newcastle-Ottawa Scale (NOS).
Results:
FXI inhibitors were associated with a significant reduction in major bleeding [relative risk (RR) 0.31; 95% confidence interval (CI) 0.21–0.46] and clinically relevant non-major bleeding (RR 0.66; 95% CI 0.47–0.93) compared with DOACs. Conversely, FXI inhibitors demonstrated an increased risk of stroke or systemic embolism (RR 3.17; 95% CI 2.18–4.62), as observed in the OCEANIC-AF trial [hazard ratio (HR) 3.79; 95% CI 2.46–5.83]. No significant difference was noted in all-cause mortality (RR 0.85; 95% CI 0.67–1.08). Limited evidence suggests that FXI inhibitors may also reduce bleeding-related hospitalizations.
Discussion:
FXI inhibitors provide a favorable bleeding profile but are less effective than DOACs for stroke prevention in patients with AF. Further long-term RCTs are warranted to delineate their role, particularly in populations at high risk of bleeding.
DOI: https://doi.org/10.37349/ent.2026.1004148
This article belongs to the special issue Interdisciplinary Approach to Therapeutic Strategies of Neuroprotection in Present and Future
Background:
Multiple sclerosis (MS) is a chronic, autoimmune, inflammatory disease that affects the central nervous system. Although the true etiology of MS remains unknown, recent research suggests that it arises from a combination of genetic vulnerability and environmental factors. The human leukocyte antigen (HLA) region is a highly polymorphic locus on chromosome 6 encoding antigen-presenting molecules central to adaptive immunity. MS exhibits significant genetic and geographic heterogeneity, reflecting complex interactions between HLA polymorphisms and environmental influences. Risk and protective alleles differ across populations, reinforcing the importance of studying such variations to better understand the disease’s pathogenesis and guide therapeutic strategies.
Methods:
This systematic review followed the “Preferred Reporting Items for Systematic reviews and Meta-Analyses” (PRISMA) guidelines, and a bibliographic search was conducted in the Medline (PubMed) and Web of Science databases using the keywords “Multiple Sclerosis”, “Genetic Polymorphisms”, “SNPs”, and “Human Leukocyte Antigen”.
Results:
Twenty-one studies were included, comprising a total of over 50,000 participants across diverse populations. The reviewed studies demonstrate that the alleles DRB1*15:01, DQB1*06:02, DRB1*03:01, DRB1*04:01, DRB1*15:03, DPB1*03:01, as well as the haplotypes DRB1*15:01~DQB1*06:02 and DRB1*15:01~DQA1*01:02~DQB1*06:02, show high expression and are strongly associated with MS susceptibility. In contrast, the alleles A*02:01 and DRB1*01:01 have shown a protective role.
Discussion:
The evidence confirms a central role of HLA class II alleles and conserved extended haplotypes, particularly DRB1*15:01-containing haplotypes, in MS susceptibility, while highlighting protective alleles and marked variability across ancestral backgrounds. These findings underscore the importance of high-resolution HLA typing, standardized haplotype definitions and inclusion of diverse populations to refine MS risk estimates.
Background:
Multiple sclerosis (MS) is a chronic, autoimmune, inflammatory disease that affects the central nervous system. Although the true etiology of MS remains unknown, recent research suggests that it arises from a combination of genetic vulnerability and environmental factors. The human leukocyte antigen (HLA) region is a highly polymorphic locus on chromosome 6 encoding antigen-presenting molecules central to adaptive immunity. MS exhibits significant genetic and geographic heterogeneity, reflecting complex interactions between HLA polymorphisms and environmental influences. Risk and protective alleles differ across populations, reinforcing the importance of studying such variations to better understand the disease’s pathogenesis and guide therapeutic strategies.
Methods:
This systematic review followed the “Preferred Reporting Items for Systematic reviews and Meta-Analyses” (PRISMA) guidelines, and a bibliographic search was conducted in the Medline (PubMed) and Web of Science databases using the keywords “Multiple Sclerosis”, “Genetic Polymorphisms”, “SNPs”, and “Human Leukocyte Antigen”.
Results:
Twenty-one studies were included, comprising a total of over 50,000 participants across diverse populations. The reviewed studies demonstrate that the alleles DRB1*15:01, DQB1*06:02, DRB1*03:01, DRB1*04:01, DRB1*15:03, DPB1*03:01, as well as the haplotypes DRB1*15:01~DQB1*06:02 and DRB1*15:01~DQA1*01:02~DQB1*06:02, show high expression and are strongly associated with MS susceptibility. In contrast, the alleles A*02:01 and DRB1*01:01 have shown a protective role.
Discussion:
The evidence confirms a central role of HLA class II alleles and conserved extended haplotypes, particularly DRB1*15:01-containing haplotypes, in MS susceptibility, while highlighting protective alleles and marked variability across ancestral backgrounds. These findings underscore the importance of high-resolution HLA typing, standardized haplotype definitions and inclusion of diverse populations to refine MS risk estimates.
DOI: https://doi.org/10.37349/ent.2026.1004147
The relationship between the gut microbiota and the central nervous system has gained attention as a biological axis that may influence the development of several neurological disorders. Recent evidence integrating genomic, neurobiological, and microbiota research shows how bacterial composition, host genetic variability, and the mechanisms of the microbiota-gut-brain axis interact in conditions such as autism spectrum disorder, epilepsy, and schizophrenia. These interactions function through neural, metabolic, and immunological related pathways involving intestinal and blood-brain barrier permeability. Genome-wide association studies (GWAS) and Mendelian randomization analyses highlight shared immunogenetic pathways that may shape both microbial profiles and neurological susceptibility. Consistent patterns of dysbiosis and alterations in neuroactive metabolites have also been reported, linking microbiota changes to neuroinflammation and disrupted neuronal signaling. This review synthesizes the current evidence supporting the integration of the microbiota-gut-brain axis and its underlying communication pathways. It also outlines the present therapeutic strategies for neurological disorders such as autism spectrum disorder, epilepsy, and schizophrenia, highlighting their potential to modulate neurological function. Additionally, it discusses the existing limitations in the field and offers insights into future research directions within this rapidly evolving area.
The relationship between the gut microbiota and the central nervous system has gained attention as a biological axis that may influence the development of several neurological disorders. Recent evidence integrating genomic, neurobiological, and microbiota research shows how bacterial composition, host genetic variability, and the mechanisms of the microbiota-gut-brain axis interact in conditions such as autism spectrum disorder, epilepsy, and schizophrenia. These interactions function through neural, metabolic, and immunological related pathways involving intestinal and blood-brain barrier permeability. Genome-wide association studies (GWAS) and Mendelian randomization analyses highlight shared immunogenetic pathways that may shape both microbial profiles and neurological susceptibility. Consistent patterns of dysbiosis and alterations in neuroactive metabolites have also been reported, linking microbiota changes to neuroinflammation and disrupted neuronal signaling. This review synthesizes the current evidence supporting the integration of the microbiota-gut-brain axis and its underlying communication pathways. It also outlines the present therapeutic strategies for neurological disorders such as autism spectrum disorder, epilepsy, and schizophrenia, highlighting their potential to modulate neurological function. Additionally, it discusses the existing limitations in the field and offers insights into future research directions within this rapidly evolving area.
DOI: https://doi.org/10.37349/ent.2026.1004146
This article belongs to the special issue Role of Microbiota in Neurological Diseases
Background:
Acquired brain injury (ABI) often causes long-lasting impairments in written language and handwriting that limit autonomy and daily functioning. Despite their relevance, these deficits have received limited research attention compared with spoken language disorders. The present work aims to systematically review interventions designed to improve reading, writing, and handwriting abilities in individuals with ABI.
Methods:
Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, PubMed, American Psychological Association (APA) PsycINFO, Cochrane Library, Web of Science, and Google Scholar were searched from inception to 1 November 2025. Eligible studies were randomized or non-randomized clinical trials (non-RCTs) involving adults or adolescents with ABI and documented written language impairments. Risk of bias was assessed using the Risk of Bias 2 tool (RCTs) and Risk of Bias in Non-randomized Studies—of Interventions tool (non-RCTs).
Results:
Twelve studies met inclusion criteria (2 RCTs, 10 non-RCTs), all conducted in post-stroke populations, highlighting the absence of evidence from other ABI aetiologies. Three main intervention categories emerged: (1) Behavioral treatments, which consistently improved trained spelling and functional writing, with some advantages for errorless learning in maintaining gains. (2) Technology-assisted approaches, including assistive software, digital spelling aids, and handwriting-focused programs, which showed feasibility, high usability, and improvements in accuracy, legibility, and motor fluency. (3) Neuromodulation, with one RCT showing that dual-site transcranial direct current stimulation can modestly enhance behavioral writing therapy. Most non-RCTs showed serious or critical risk of bias, and sample sizes were small, limiting generalizability.
Discussion:
Current evidence—although preliminary and restricted to post-stroke ABI—indicates that behavioral, technological, and neuromodulatory interventions can improve aspects of written language and handwriting after ABI. However, the available literature is characterized by small samples, substantial methodological variability, and a paucity of standardized and ecologically valid outcome measures. High-quality, adequately powered trials with standardized, functional outcomes are urgently needed, particularly in non-stroke ABI populations.
Background:
Acquired brain injury (ABI) often causes long-lasting impairments in written language and handwriting that limit autonomy and daily functioning. Despite their relevance, these deficits have received limited research attention compared with spoken language disorders. The present work aims to systematically review interventions designed to improve reading, writing, and handwriting abilities in individuals with ABI.
Methods:
Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, PubMed, American Psychological Association (APA) PsycINFO, Cochrane Library, Web of Science, and Google Scholar were searched from inception to 1 November 2025. Eligible studies were randomized or non-randomized clinical trials (non-RCTs) involving adults or adolescents with ABI and documented written language impairments. Risk of bias was assessed using the Risk of Bias 2 tool (RCTs) and Risk of Bias in Non-randomized Studies—of Interventions tool (non-RCTs).
Results:
Twelve studies met inclusion criteria (2 RCTs, 10 non-RCTs), all conducted in post-stroke populations, highlighting the absence of evidence from other ABI aetiologies. Three main intervention categories emerged: (1) Behavioral treatments, which consistently improved trained spelling and functional writing, with some advantages for errorless learning in maintaining gains. (2) Technology-assisted approaches, including assistive software, digital spelling aids, and handwriting-focused programs, which showed feasibility, high usability, and improvements in accuracy, legibility, and motor fluency. (3) Neuromodulation, with one RCT showing that dual-site transcranial direct current stimulation can modestly enhance behavioral writing therapy. Most non-RCTs showed serious or critical risk of bias, and sample sizes were small, limiting generalizability.
Discussion:
Current evidence—although preliminary and restricted to post-stroke ABI—indicates that behavioral, technological, and neuromodulatory interventions can improve aspects of written language and handwriting after ABI. However, the available literature is characterized by small samples, substantial methodological variability, and a paucity of standardized and ecologically valid outcome measures. High-quality, adequately powered trials with standardized, functional outcomes are urgently needed, particularly in non-stroke ABI populations.
DOI: https://doi.org/10.37349/ent.2026.1004145
This article belongs to the special issue Neuropsychology of Handwriting
Background:
Fully immersive virtual reality (IVR) is an emerging technology approach for cognitive training in individuals with mild cognitive impairment (MCI) and dementia. While interest in fully IVR continues to grow, it remains unclear the extent of effectiveness and the key components that contribute to successful implementation. This study aimed to explore the effectiveness of fully IVR cognitive training for individuals with MCI or dementia from previous research literature.
Methods:
A scoping review was conducted using a systematic search strategy based on the population, concept, and context framework.
Results:
Out of the 816 records identified, 123 full texts were screened, and eight studies were included in the review. The included studies all involved participants completing a cognitive training intervention using fully IVR headsets, with cognitive outcomes measured before and after the intervention. The most consistent improvements across the included studies were executive function, memory, and visuospatial abilities. Only two studies explicitly referenced a theoretical model.
Discussion:
Fully IVR cognitive training demonstrates promise for improving specific cognitive domains in individuals living with MCI or dementia. However, inconsistencies in outcomes and limited theoretical grounding highlight the need for further exploration. Broader considerations are discussed in the discussion section.
Background:
Fully immersive virtual reality (IVR) is an emerging technology approach for cognitive training in individuals with mild cognitive impairment (MCI) and dementia. While interest in fully IVR continues to grow, it remains unclear the extent of effectiveness and the key components that contribute to successful implementation. This study aimed to explore the effectiveness of fully IVR cognitive training for individuals with MCI or dementia from previous research literature.
Methods:
A scoping review was conducted using a systematic search strategy based on the population, concept, and context framework.
Results:
Out of the 816 records identified, 123 full texts were screened, and eight studies were included in the review. The included studies all involved participants completing a cognitive training intervention using fully IVR headsets, with cognitive outcomes measured before and after the intervention. The most consistent improvements across the included studies were executive function, memory, and visuospatial abilities. Only two studies explicitly referenced a theoretical model.
Discussion:
Fully IVR cognitive training demonstrates promise for improving specific cognitive domains in individuals living with MCI or dementia. However, inconsistencies in outcomes and limited theoretical grounding highlight the need for further exploration. Broader considerations are discussed in the discussion section.
DOI: https://doi.org/10.37349/ent.2026.1004144
This article belongs to the special issue Innovations in Neurotechnology: Integrating AI, Neuroimaging, and VR for the Assessment and Treatment of Neurological Conditions
