Mini Review
Mini Review

Affiliation:
1FUCP, Foundation University Islamabad, Islamabad 46000, Pakistan
Email: ayesharwp@gmail.com
ORCID: https://orcid.org/0009-0004-2188-2783
Affiliation:
2Margalla Institute of Health Sciences, Rawalpindi 46000, Pakistan
ORCID: https://orcid.org/0009-0000-7637-8139
Explor Neuroprot Ther. 2025;5:1004117 DOI: https://doi.org/10.37349/ent.2025.1004117
Received: June 14, 2025 Accepted: September 17, 2025 Published: October 16, 2025
Academic Editor: Noureddin Nakhostin Ansari, Tehran University of Medical Sciences (TUMS), Iran
Healthcare professionals, especially those in rehabilitation, are increasingly vulnerable to occupational burnout, particularly in the post-pandemic landscape. This review synthesizes existing literature on the prevalence of burnout, possible contributing factors, resilience mechanisms, and interventions tailored to physiotherapists and related disciplines. A narrative review was carried out by combing through databases including PubMed, Scopus, and Web of Science for literature published between 2020 and 2025. The studies focused on burnout, mental health, and resilience among rehabilitation professionals were included in the review. Burnout remains prevalent, with emotional exhaustion and reduced personal growth commonly reported. Risk factors include lack of support, excessive workload, and exposure to workplace bullying. Protective mechanisms entail individual resilience behaviors, social support, and institutional strategies such as regulated supervision and workload management. Addressing burnout in rehabilitation settings requires a dual approach—strengthening individual factors and directing systemic organizational reforms. Embedding resilience education into the training core curriculum and workplace code of conduct may boost mental well-being.
Burnout, exhaustion, and fatigue are terms that are often used interchangeably. These terms are interrelated but possess distinct psychological and physiological characteristics that continually coexist in health professionals, particularly those in rehabilitation roles. Rehabilitation professionals, also known as rehab workers, are healthcare providers who help individuals recover physical, cognitive, emotional, or social function after an injury, illness, or disability. This group commonly includes: physical therapists (PTs), occupational therapists (OTs), speech-language pathologists (SLPs), rehabilitation nurses, recreational therapists, rehabilitation counselors, and psychiatrists, along with Physical Medicine & Rehabilitation physicians. They collaborate in interdisciplinary teams to provide patient-centered care across a continuum of settings.
These professionals work in diverse settings, including but not limited to inpatient and outpatient rehab centers, nursing facilities, long-term and assisted living centers, community mental health or vocational rehab settings, and home health agencies. The setting influences the nature of the workload and risk of burnout based on the availability of resources such as staffing, caseload, and emotional labor. Rehab workers occupy a unique space in the health ecosystem due to the nature of their work, that is, their long-term engagement with the patients, with a heavy focus on goal-oriented treatment practice, making them vulnerable to exhaustion and emotional fatigue.
In order to manage these states, it is of foremost importance to have a clear understanding of these conditions. Burnout is a psychological syndrome brought on by chronic workplace stress and may be characterized by emotional exhaustion, depersonalization (cynicism), and a weakened sense of personal accomplishment [1]. It does not happen overnight but rather develops over time, consequently affecting an individual’s motivation levels, personal and social engagement, and long-term career satisfaction. Exhaustion, on the other hand, is a core constituent of burnout, but it can exist independently. It classically refers to a sense of being overwhelmingly tired—Be it mentally, emotionally, or physically, and sometimes all of these combined, caused by prolonged stress or exertion [2]. Fatigue is much more generalized and physiological in nature, often resulting from a lack of proper rest or energy drainage due to physical exertion or overextended mental workload. While exhaustion can recover with a sufficient amount of short-term rest, fatigue may persist a bit longer and compromise an individual’s cognitive and motor performance [3].
Recent studies have indicated that burnout is most alarming due to its long-term impact and association with mental disorders such as anxiety and depression [4]. However, the remedial measures differ: Fatigue necessitates proper sleep and nutrition regulation, exhaustion benefits from adjustments in workload, and burnout demands structural organizational modifications and psycho-social assistance. It is critical to understand these distinctions for early detection and specified interventions in rehabilitative settings (see Table 1).
Summary for burnout factors and protective mechanisms.
| Category | Description |
|---|---|
| Burnout prevalence | 30–60% health professionals report symptoms of exhaustion and low efficacy. |
| Risk factors | High caseloads, lack of support, workplace conflicts, exposure to bullying, and lack of job security. |
| Protective mechanisms | Resilience, social support, emotional regulation, and mindfulness. |
| Institutional strategies | Supervisor-led programs, workload distribution, and wellness programs. |
| Educational approaches | Mentorship, early exposure to mental health resources, and resilience education. |
Burnout among health-care providers has been acknowledged as a threat to service quality and professional well-being. For rehabilitation specialists, including PTs, SLPs, and OTs, unique stress factors such as limited recognition, emotionally exhaustive work, and administrative burdens raise the stakes. Post-pandemic changes in employment patterns and continuously growing demands for rehabilitation services further exacerbate this problem. This review explores the latest evidence on occupational burnout in this cohort, probes the role of resilience, and summarizes both individual-level and organizational intervention frameworks.
A narrative literature review was conducted to explore the current evidence on burnout and resilience among rehabilitation professionals. Electronic databases, including PubMed, Scopus, and Web of Science, were manually searched using a combination of keywords and Boolean operators: “burnout”, “resilience”, “rehabilitation professionals”, “physiotherapy”, and “mental well-being”. The search was limited to peer-reviewed articles published in English between January 2020 and May 2025, to capture the most recent and relevant literature, particularly in the context of evolving post-pandemic healthcare dynamics. A total of 18 studies, out of 30, were included based on the criteria mentioned below.
Inclusion criteria were:
Empirical studies focused on burnout and/or resilience among PTs or related allied health professionals (e.g., OTs, SLPs, rehabilitation counselors, etc.).
Studies with clearly defined healthcare professional samples working in rehabilitation contexts.
Exclusion criteria included:
Editorials, commentaries, or dissertations.
Studies that involved non-healthcare professionals as primary participants.
Articles not published in English or outside the defined time frame.
The global prevalence of burnout varies worldwide, but it has been reported in 30–50% of rehabilitation professionals [5, 6]. Symptoms for burnout include, but are not limited to, emotional exhaustion, detachment, cynicism, hopelessness, and a dwindling sense of personal competence [7]. Female professionals have been found to be more prone to burnout than their male counterparts, and those with less experience are particularly vulnerable [8]. Take, for example, an intern with little or no knowledge of the departmental operations may become overwhelmed by the sudden change of environment, the workload, and responsibility for patients’ care. Without proper guidance and support, they might end up with burnout sooner or later. The negative effects of burnout eventually affect every area of life, ultimately making all responsibilities of the individual no less than a burden.
Though the global prevalence of burnout is high, it is especially higher in Asian countries. A study in Switzerland concluded that the average prevalence of overall burnout and exhaustion is approximately 18%, with higher rates in health workers than non-medical professionals [9]. Considerably higher trends, much similar to those of Asia, can be seen in the US, where a study reported 35.8% of residents of physical medicine meeting the burnout criteria, with the main reason being having inadequate personal and family time [10]. This suggests that sociocultural and systemic factors may influence burnout levels. Dynamics such as cultural attitudes towards work-life balance and workload distribution based on the resources available may also contribute to the cause.
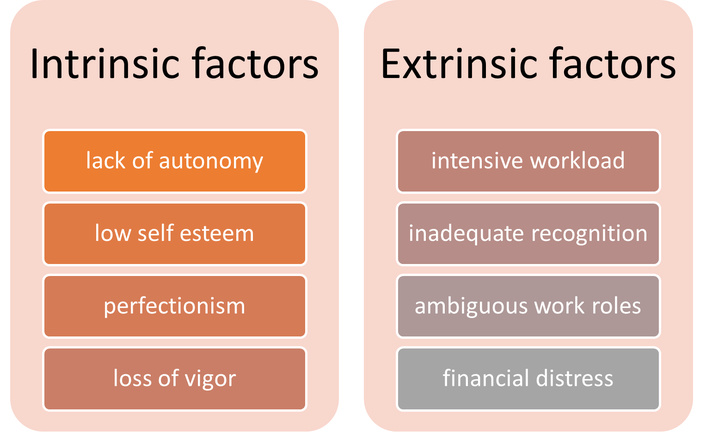
Key contributors include excessive caseloads, lack of administrative backing, and interpersonal conflict in workplaces [11]. Other factors may include peer neglect, worries about job security, money worries, and strained personal relationships (see Figure 1). A multicenter study in Korea highlighted that the physiotherapists experiencing workplace discrimination and/or inadequate supervision exhibited significantly higher burnout scores [12]. Similar trends were identified in Central Asian countries post-COVID, where institutional instability and volatility became the cause for further deterioration of work-related stresses [13]. While the Korean study emphasized inter-personal and supervisory issues, macro-level institutional instability was dominant in Central Asia. This contrast underscores how burnout drivers may shift depending on the scale of stressors. A cross-sectional study in Pakistan established that hectic routines and low salary cause high risks of developing burnout in fresh rehab workers [14]. Taken together, these findings reveal that while excessive demands and inadequate support are common determinants worldwide, the dominant drivers differ across settings.
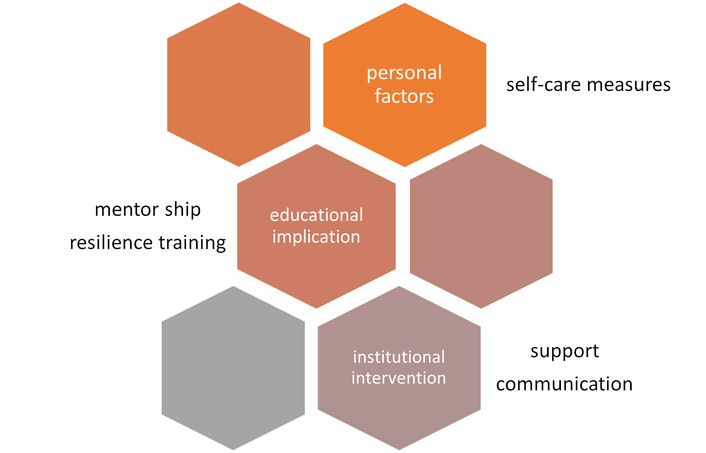
Personal resilience and tenacity present as a critical buffer. Defined as the capacity to recover in times of difficulty and to bounce back rather than breaking down, resilience relates well to improved coping and job satisfaction [15]. Active coping approaches such as cognitive behavioral strategies, emotional regulation training, and mindfulness have all been demonstrated to be effective (see Figure 2) [16]. Pulling away from patient care may even make a health worker feel guilty temporarily, but it is important to realize that an empty cup is of no use; only when a health provider is mentally well and grounded can they be more empathetic towards their patients.
To effectively manage burnout on an individual level, one must learn to prioritize oneself. The following are some tips on burnout recovery anyone can try [17, 18]:
Acceptance and compassion for oneself.
Aim for 7–9 hours of peaceful sleep.
A balanced, nutrient-rich diet.
Regular exercise to uplift mood and reduce sensory overload.
Setting boundaries and good time management.
Scheduling short breaks between work hours.
Adding mindfulness to daily routine, such as meditation, yoga, or as simple as deep breathing exercises.
Seeking support.
A supportive work environment can significantly reduce burnout incidence. Manageable workload distribution, transparent inter-personnel communication, and supervisor-led support programs enhance outcomes [19, 20]; changes integrated by the organizations are surprisingly more long-lasting. Institutions and administrative departments that incorporate clinicians’ wellness programs into the daily workflow show improved staff retention and self-esteem [21]. Many organizations already have policies to support their employees, but proper implementation is lacking.
Integrating resilience training into academic and clinical education can help prepare students to take occupational stress head-on [22]. Early exposure to mental health resources and mentorship builds up foundational coping skills [23]. Medical students would eventually benefit from such training not only in their future career but also in their time as students, improving their wellness and health, making them sound and grounded individuals early on (see Figure 2).
Burnout is multifactorial and complex, often rooted in systemic inefficiencies and organizational culture. While individual strength and adaptability offer a protective buffer, relying solely on self-regulation can lead to overexertion and suffering. Administrations must therefore share responsibility by creating an environment that promotes employees’ mental well-being. Integrating supportive policies, wellness curricula, and leadership training in resilience and emotional intelligence is crucial for long-term revolution. Stability among the workers not only improves employee well-being but also leads to high-quality patient care and increased overall competence.
However, the systemic and cultural contexts in which burnout occurs differ substantially between high-income countries (HICs) and low- and middle-income countries (LMICs). In HICs, well-structured healthcare systems often provide formal well-being programs, organizational backing, and sufficient staffing ratios, yet burnout remains prevalent, often driven by high-performance expectations and administrative obligations. In contrast, LMICs, including Pakistan, face additional challenges such as limited healthcare resources, high patient-to-provider ratios, lower salaries, and weaker institutional support systems. These systemic shortcomings magnify the burnout risk by placing heavier workloads on fewer staff members while offering minimal organizational protection. Cultural norms may further discourage healthcare workers from voicing distress or seeking professional help, perpetuating the cycle.
Recognizing these contextual differences is essential. Burnout awareness is vital for safeguarding the health, well-being, and long-term effectiveness of healthcare and rehabilitation professionals. These individuals function in environments that are often high-pressure, emotionally taxing, and physically demanding. Recognizing the early signs of burnout is critical in preventing the progression to more serious mental health issues, including anxiety, depression, and even substance use disorders. Timely identification allows for early intervention, whether through self-care strategies, peer support, professional counseling, or organizational changes. The impact of burnout extends well beyond the individual. When healthcare providers are burned out, patient care can suffer—manifesting in decreased empathy, increased medical errors, and reduced patient satisfaction. Future studies should move beyond cross-sectional prevalence studies and focus on longitudinal designs to better capture the progression and consequences of burnout. Specifically, more evaluation should be carried out for the longstanding changes of resilience training and institutional amendments to better inform policy and practice. Finally, mixed-methods research incorporating qualitative perspectives of the people involved could help uncover cultural barriers to help-seeking and inform more context-sensitive strategies.
Burnout in rehabilitation workers is both prevalent and preventable. Acute and chronic pressures linked to burnout and related illnesses are challenges faced by rehab workers in clinics, hospitals, or at the first point of care. As a result, prompt treatments that lessen the impact of challenging clinical circumstances on such employees are crucial and essential to their mental well-being. A bi-focal strategy, which would target personal uplifting and structural reforms, is direly required to address the mental health needs of this workforce.
HICs: high-income countries
LMICs: low- and middle-income countries
OTs: occupational therapists
PTs: physical therapists
SLPs: speech-language pathologists
AI: Conceptualization, Methodology, Investigation, Writing—original draft. MA: Investigation, Writing—review & editing. Both authors have read and approved the submitted version.
The authors declare that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 5686
Download: 28
Times Cited: 0