











Aim:
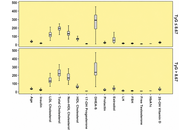
The aim of this study was to investigate the relationship between the triglyceride-glucose (TyG) index and hormonal, biochemical, and lipid parameters in patients with polycystic ovary syndrome (PCOS).
Methods:
In this retrospective single-center study, 2,243 outpatient records were reviewed. Among 696 patients diagnosed with PCOS between 2015 and 2022, 233 newly diagnosed and treatment-naive patients were included. TyG was calculated using fasting triglyceride and glucose values. Correlations between TyG and laboratory parameters were assessed. The optimal TyG cut-off for insulin resistance was evaluated using HOMA-IR and receiver operating characteristic analysis.
Results:
TyG was positively correlated with HbA1c, age, LDL cholesterol, total cholesterol, non-HDL cholesterol, insulin, and HOMA-IR, and negatively correlated with HDL cholesterol. The optimal TyG cut-off was 8.67, with an AUC of 0.709, sensitivity of 50.49%, and specificity of 85.38%. Patients with TyG values above the cut-off had higher age, insulin, LDL cholesterol, total cholesterol, non-HDL cholesterol, and HbA1c values, whereas HDL cholesterol and estradiol levels were lower.
Conclusions:
TyG was associated with insulin resistance markers and dyslipidemic parameters in patients with PCOS. These findings support the potential clinical utility of TyG as a simple surrogate marker for metabolic risk assessment in PCOS.
Aim:
The aim of this study was to investigate the relationship between the triglyceride-glucose (TyG) index and hormonal, biochemical, and lipid parameters in patients with polycystic ovary syndrome (PCOS).
Methods:
In this retrospective single-center study, 2,243 outpatient records were reviewed. Among 696 patients diagnosed with PCOS between 2015 and 2022, 233 newly diagnosed and treatment-naive patients were included. TyG was calculated using fasting triglyceride and glucose values. Correlations between TyG and laboratory parameters were assessed. The optimal TyG cut-off for insulin resistance was evaluated using HOMA-IR and receiver operating characteristic analysis.
Results:
TyG was positively correlated with HbA1c, age, LDL cholesterol, total cholesterol, non-HDL cholesterol, insulin, and HOMA-IR, and negatively correlated with HDL cholesterol. The optimal TyG cut-off was 8.67, with an AUC of 0.709, sensitivity of 50.49%, and specificity of 85.38%. Patients with TyG values above the cut-off had higher age, insulin, LDL cholesterol, total cholesterol, non-HDL cholesterol, and HbA1c values, whereas HDL cholesterol and estradiol levels were lower.
Conclusions:
TyG was associated with insulin resistance markers and dyslipidemic parameters in patients with PCOS. These findings support the potential clinical utility of TyG as a simple surrogate marker for metabolic risk assessment in PCOS.
DOI: https://doi.org/10.37349/eemd.2026.101479
Aim:
Assess the benefits of using a diabetes app and connected blood glucose (BG) meter in people with type 2 diabetes (PwT2D) with higher-than-recommended mean BG. It is well understood that sustained higher levels of glycemia are linked to diabetes related complications and that early intervention to reduce hyperglycemia is an important clinical goal.
Methods:
We sourced server data from a total population of 22,696 PwT2D using the OneTouch Reveal diabetes app in conjunction with a OneTouch Verio Flex or Reflect BG meter. We identified three groups (mean BG > 180, > 155, and between > 155 and < 180 mg/dL) at higher risk for diabetes-associated complications based on their hyperglycemia. Data from their first 14 days using the app was compared with the last 14 days at the end of each timeframe, using paired within-subject differences.
Results:
At 1 year in PwT2D with baseline mean BG > 155 mg/dL, readings in range (RIR) improved by 24.0%, and mean BG decreased by 35.9 mg/dL, from 196.4 mg/dL to 160.5 mg/dL. These improvements were due to reductions in hyperglycemic readings. Subjects with the highest baseline mean BG of > 180 mg/dL had the greatest reduction (–54.3 mg/dL) in mean BG after experiencing the new app and meter for 1 year. Those engaging more often with the app had greater improvements in glycemia.
Conclusions:
In PwT2D with higher-than-recommended mean BG, substantial improvements in glycemia were associated with subjects using a diabetes app with a connected blood glucose meter at 3 months, and these improvements were sustained out to 1-year.
Aim:
Assess the benefits of using a diabetes app and connected blood glucose (BG) meter in people with type 2 diabetes (PwT2D) with higher-than-recommended mean BG. It is well understood that sustained higher levels of glycemia are linked to diabetes related complications and that early intervention to reduce hyperglycemia is an important clinical goal.
Methods:
We sourced server data from a total population of 22,696 PwT2D using the OneTouch Reveal diabetes app in conjunction with a OneTouch Verio Flex or Reflect BG meter. We identified three groups (mean BG > 180, > 155, and between > 155 and < 180 mg/dL) at higher risk for diabetes-associated complications based on their hyperglycemia. Data from their first 14 days using the app was compared with the last 14 days at the end of each timeframe, using paired within-subject differences.
Results:
At 1 year in PwT2D with baseline mean BG > 155 mg/dL, readings in range (RIR) improved by 24.0%, and mean BG decreased by 35.9 mg/dL, from 196.4 mg/dL to 160.5 mg/dL. These improvements were due to reductions in hyperglycemic readings. Subjects with the highest baseline mean BG of > 180 mg/dL had the greatest reduction (–54.3 mg/dL) in mean BG after experiencing the new app and meter for 1 year. Those engaging more often with the app had greater improvements in glycemia.
Conclusions:
In PwT2D with higher-than-recommended mean BG, substantial improvements in glycemia were associated with subjects using a diabetes app with a connected blood glucose meter at 3 months, and these improvements were sustained out to 1-year.
DOI: https://doi.org/10.37349/eemd.2026.101478
Background:
Type 2 diabetes (T2D) is a chronic metabolic condition requiring sustained pharmacological and behavioural management. Suboptimal medication adherence remains a major barrier to achieving adequate glycaemic control and is associated with increased morbidity, mortality, and healthcare costs. Patient-centred care (PCC) has been widely recommended as an approach to enhance patient engagement, adherence, and clinical outcomes; however, evidence regarding its effectiveness remains inconsistent. This systematic review aimed to synthesise evidence from primary studies evaluating PCC interventions on medication adherence, glycaemic control, and psychosocial outcomes in adults with T2D.
Methods:
This review followed PRISMA 2020 guidelines and was prospectively registered in PROSPERO (CRD420251115067). A comprehensive search of MEDLINE, Embase, EMCare, CINAHL, PsycINFO, and the Cochrane Library was conducted for studies published between 2005 and 2025. Eligible studies included primary research evaluating PCC interventions in adults with T2D and reporting adherence or clinical outcomes. Data were synthesised narratively due to heterogeneity, and vote counting based on direction of effect was applied. Risk of bias was assessed using RoB 2.0, ROBINS-I, and CASP tools, and overall certainty of evidence was evaluated using the GRADE framework.
Results:
Eighteen studies were included, comprising seven randomised controlled trials, eight observational studies, and three qualitative studies. PCC interventions consistently improved medication adherence and psychosocial outcomes, including patient empowerment and engagement. In contrast, effects on glycaemic control were variable, with four studies reporting improvement, seven showing no effect, and three demonstrating mixed findings. Overall, the evidence suggests a predominantly positive but inconsistent effect on HbA1c.
Discussion:
PCC interventions appear effective in improving behavioural and psychosocial outcomes but demonstrate inconsistent impact on glycaemic control. These findings suggest that PCC should be considered a supportive strategy to enhance engagement and adherence rather than a standalone intervention for improved clinical outcomes. Further research is required to identify optimal intervention components that can improve clinical outcomes.
Background:
Type 2 diabetes (T2D) is a chronic metabolic condition requiring sustained pharmacological and behavioural management. Suboptimal medication adherence remains a major barrier to achieving adequate glycaemic control and is associated with increased morbidity, mortality, and healthcare costs. Patient-centred care (PCC) has been widely recommended as an approach to enhance patient engagement, adherence, and clinical outcomes; however, evidence regarding its effectiveness remains inconsistent. This systematic review aimed to synthesise evidence from primary studies evaluating PCC interventions on medication adherence, glycaemic control, and psychosocial outcomes in adults with T2D.
Methods:
This review followed PRISMA 2020 guidelines and was prospectively registered in PROSPERO (CRD420251115067). A comprehensive search of MEDLINE, Embase, EMCare, CINAHL, PsycINFO, and the Cochrane Library was conducted for studies published between 2005 and 2025. Eligible studies included primary research evaluating PCC interventions in adults with T2D and reporting adherence or clinical outcomes. Data were synthesised narratively due to heterogeneity, and vote counting based on direction of effect was applied. Risk of bias was assessed using RoB 2.0, ROBINS-I, and CASP tools, and overall certainty of evidence was evaluated using the GRADE framework.
Results:
Eighteen studies were included, comprising seven randomised controlled trials, eight observational studies, and three qualitative studies. PCC interventions consistently improved medication adherence and psychosocial outcomes, including patient empowerment and engagement. In contrast, effects on glycaemic control were variable, with four studies reporting improvement, seven showing no effect, and three demonstrating mixed findings. Overall, the evidence suggests a predominantly positive but inconsistent effect on HbA1c.
Discussion:
PCC interventions appear effective in improving behavioural and psychosocial outcomes but demonstrate inconsistent impact on glycaemic control. These findings suggest that PCC should be considered a supportive strategy to enhance engagement and adherence rather than a standalone intervention for improved clinical outcomes. Further research is required to identify optimal intervention components that can improve clinical outcomes.
DOI: https://doi.org/10.37349/eemd.2026.101477
This article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Aim:
Diabetic neuropathy is the most prevalent diabetic complication, impacting up to 60% of people with diabetes. It is characterized by distal symmetrical loss of sensory function in the lower extremities, presenting with spontaneous excruciating neuropathic pain, hyperalgesia, and allodynia that impairs quality of life. The current work aims to evaluate the neuroprotective potential of naringin (a citrus flavonoid) and examine its ability to improve Streptozotocin (STZ)-induced diabetic neuropathic pain by investigating its hypoglycemic, lipid-lowering, anti-inflammatory, and antioxidant effects.
Methods:
Diabetes was induced in 30 of 40 male Sprague-Dawley rats via a single STZ injection (45 mg/kg). Rats were divided into four groups: normal control, diabetic control, naringin-treated, and glimepiride-treated (positive control). After treatment, serum and brain tissues were collected to assess biochemical parameters. Pain-related behaviors were evaluated using hot plate, tail immersion, and von Frey filament tests.
Results:
A significant increase in the serum levels of glucose, triglyceride, total cholesterol, low-density lipoprotein-cholesterol, and nitric oxide, with a concomitant decrease in body weight, plasma insulin, and high-density lipoprotein-cholesterol, was observed in diabetic rats. Also, the brain level of malondialdehyde was increased, while that of reduced glutathione, glutathione peroxidase, catalase, and superoxide dismutase were markedly decreased. Furthermore, diabetic rats showed a marked increase in plasma levels of inflammatory cytokines including interleukin-6 and tumor necrosis factor-α. Moreover, hot plate, tail immersion, and von Frey tests revealed hyperalgesia in diabetic rats. Treatment with naringin and glimepiride reduced pain hypersensitivity, restored body weight, and nearly normalized the altered biochemical parameters, more significantly with naringin than with glimepiride.
Conclusions:
These results may highlight the potential effects of naringin as a therapeutic strategy for diabetes and its complications, including peripheral neuropathy.
Aim:
Diabetic neuropathy is the most prevalent diabetic complication, impacting up to 60% of people with diabetes. It is characterized by distal symmetrical loss of sensory function in the lower extremities, presenting with spontaneous excruciating neuropathic pain, hyperalgesia, and allodynia that impairs quality of life. The current work aims to evaluate the neuroprotective potential of naringin (a citrus flavonoid) and examine its ability to improve Streptozotocin (STZ)-induced diabetic neuropathic pain by investigating its hypoglycemic, lipid-lowering, anti-inflammatory, and antioxidant effects.
Methods:
Diabetes was induced in 30 of 40 male Sprague-Dawley rats via a single STZ injection (45 mg/kg). Rats were divided into four groups: normal control, diabetic control, naringin-treated, and glimepiride-treated (positive control). After treatment, serum and brain tissues were collected to assess biochemical parameters. Pain-related behaviors were evaluated using hot plate, tail immersion, and von Frey filament tests.
Results:
A significant increase in the serum levels of glucose, triglyceride, total cholesterol, low-density lipoprotein-cholesterol, and nitric oxide, with a concomitant decrease in body weight, plasma insulin, and high-density lipoprotein-cholesterol, was observed in diabetic rats. Also, the brain level of malondialdehyde was increased, while that of reduced glutathione, glutathione peroxidase, catalase, and superoxide dismutase were markedly decreased. Furthermore, diabetic rats showed a marked increase in plasma levels of inflammatory cytokines including interleukin-6 and tumor necrosis factor-α. Moreover, hot plate, tail immersion, and von Frey tests revealed hyperalgesia in diabetic rats. Treatment with naringin and glimepiride reduced pain hypersensitivity, restored body weight, and nearly normalized the altered biochemical parameters, more significantly with naringin than with glimepiride.
Conclusions:
These results may highlight the potential effects of naringin as a therapeutic strategy for diabetes and its complications, including peripheral neuropathy.
DOI: https://doi.org/10.37349/eemd.2026.101476
This article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Aim:
Estrogens regulate energy balance and glucose homeostasis, but whether they coordinate endocrine changes across the gut–pancreas axis in obesity remains unclear. This study examined whether ethinyl estradiol (EE2) improves metabolic control in obese diabetic mice through combined effects on pancreatic islets and intestinal enteroendocrine cells.
Methods:
Female ob/ob mice received EE2 (4,000 ng/mL) or vehicle in drinking water for 21 days. Body weight, food intake, glucose levels, glucose tolerance, pancreatic islet composition, and ileal enteroendocrine cell populations were assessed using biochemical assays and immunohistochemistry.
Results:
EE2 significantly reduced body weight and energy intake and produced sustained lowering of blood glucose with markedly improved glucose tolerance and reduced terminal insulin levels. EE2 increased islet density and beta-cell proliferation and shifted islet size distribution toward larger islets, consistent with enhanced islet growth. Alpha-cell area was significantly reduced, indicating improved insulin–glucagon balance. Peptide YY (PYY)-positive cells within pancreatic islets were markedly increased, whereas somatostatin (SST)-positive cells were unchanged. In the ileum, EE2 significantly reduced crypt depth and increased the number of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP)-positive enteroendocrine cells, particularly within crypt regions, indicating enhanced incretin cell abundance. These coordinated changes across the gut and pancreas were associated with improved glucose control and reduced hyperinsulinaemia.
Conclusions:
EE2 improves metabolic control in obese diabetic mice through linked changes in pancreatic islet cell composition and intestinal incretin-producing cells. By increasing beta-cell renewal, reducing alpha-cell area, and enhancing GLP-1, GIP, and PYY expression, estrogen establishes a gut–pancreas endocrine environment that supports glucose homeostasis in obesity.
Aim:
Estrogens regulate energy balance and glucose homeostasis, but whether they coordinate endocrine changes across the gut–pancreas axis in obesity remains unclear. This study examined whether ethinyl estradiol (EE2) improves metabolic control in obese diabetic mice through combined effects on pancreatic islets and intestinal enteroendocrine cells.
Methods:
Female ob/ob mice received EE2 (4,000 ng/mL) or vehicle in drinking water for 21 days. Body weight, food intake, glucose levels, glucose tolerance, pancreatic islet composition, and ileal enteroendocrine cell populations were assessed using biochemical assays and immunohistochemistry.
Results:
EE2 significantly reduced body weight and energy intake and produced sustained lowering of blood glucose with markedly improved glucose tolerance and reduced terminal insulin levels. EE2 increased islet density and beta-cell proliferation and shifted islet size distribution toward larger islets, consistent with enhanced islet growth. Alpha-cell area was significantly reduced, indicating improved insulin–glucagon balance. Peptide YY (PYY)-positive cells within pancreatic islets were markedly increased, whereas somatostatin (SST)-positive cells were unchanged. In the ileum, EE2 significantly reduced crypt depth and increased the number of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP)-positive enteroendocrine cells, particularly within crypt regions, indicating enhanced incretin cell abundance. These coordinated changes across the gut and pancreas were associated with improved glucose control and reduced hyperinsulinaemia.
Conclusions:
EE2 improves metabolic control in obese diabetic mice through linked changes in pancreatic islet cell composition and intestinal incretin-producing cells. By increasing beta-cell renewal, reducing alpha-cell area, and enhancing GLP-1, GIP, and PYY expression, estrogen establishes a gut–pancreas endocrine environment that supports glucose homeostasis in obesity.
DOI: https://doi.org/10.37349/eemd.2026.101475
This article belongs to the special issue Innovative Strategies for Diabetes and Metabolic Disorders: Current and Future Directions
Background:
Diabetes mellitus (DM) refers to a group of metabolic diseases characterized by reduced insulin synthesis and release, leading to hyperglycemia, oxidative stress, and inflammation. The prevalence of DM continues to increase worldwide, primarily driven by type 2 DM (T2DM). While numerous prescription drugs are widely available for the management of T2DM, these treatments must be coupled with significant changes in diet and lifestyle to have long-term effects. This comparative review aims to summarize and critically evaluate some of the dietary antioxidant and anti-inflammatory functional foods (FFs), including bioactive compounds on glycemic regulation, oxidative stress, inflammatory markers, and other outcomes in T2DM patients.
Methods:
A comprehensive literature search was performed from June 2014 to December 2025 in Cochrane Library, Embase, Google Scholar, PubMed/Medline, and Scopus databases.
Results:
Thirty-one meta-analyses describing the effects of specific FFs on glycemic outcomes, including fasting blood glucose, HbA1c, insulin levels, insulin resistance, oxidative or inflammatory stress, and/or the doses needed to achieve these endpoints, in T2DM patients were included. Comparative analyses of the data for green tea in T2DM showed significant antioxidant effects, but conflicting data for glycemic regulation, and no significant effect on inflammatory markers. Flaxseed products significantly reduced oxidative stress and HbA1c but had no anti-inflammatory effects. Both anthocyanins and resveratrol from fruits and vegetables significantly reduced fasting blood glucose, HbA1c, as well as oxidative and inflammatory markers. Turmeric and curcumin significantly reduced fasting blood glucose, but the data for ginger were conflicted. In T2DM patients, turmeric and ginger significantly reduced markers of oxidation and inflammation.
Discussion:
Overall, improvements in diet, including the incorporation of specific FFs and exercise, along with standard treatments, may be cost-effective methods to reduce the public health impact of T2DM. Limitations included the significant heterogeneity, high risk of bias, and low to moderate quality of the randomized controlled trial (RCT).
Background:
Diabetes mellitus (DM) refers to a group of metabolic diseases characterized by reduced insulin synthesis and release, leading to hyperglycemia, oxidative stress, and inflammation. The prevalence of DM continues to increase worldwide, primarily driven by type 2 DM (T2DM). While numerous prescription drugs are widely available for the management of T2DM, these treatments must be coupled with significant changes in diet and lifestyle to have long-term effects. This comparative review aims to summarize and critically evaluate some of the dietary antioxidant and anti-inflammatory functional foods (FFs), including bioactive compounds on glycemic regulation, oxidative stress, inflammatory markers, and other outcomes in T2DM patients.
Methods:
A comprehensive literature search was performed from June 2014 to December 2025 in Cochrane Library, Embase, Google Scholar, PubMed/Medline, and Scopus databases.
Results:
Thirty-one meta-analyses describing the effects of specific FFs on glycemic outcomes, including fasting blood glucose, HbA1c, insulin levels, insulin resistance, oxidative or inflammatory stress, and/or the doses needed to achieve these endpoints, in T2DM patients were included. Comparative analyses of the data for green tea in T2DM showed significant antioxidant effects, but conflicting data for glycemic regulation, and no significant effect on inflammatory markers. Flaxseed products significantly reduced oxidative stress and HbA1c but had no anti-inflammatory effects. Both anthocyanins and resveratrol from fruits and vegetables significantly reduced fasting blood glucose, HbA1c, as well as oxidative and inflammatory markers. Turmeric and curcumin significantly reduced fasting blood glucose, but the data for ginger were conflicted. In T2DM patients, turmeric and ginger significantly reduced markers of oxidation and inflammation.
Discussion:
Overall, improvements in diet, including the incorporation of specific FFs and exercise, along with standard treatments, may be cost-effective methods to reduce the public health impact of T2DM. Limitations included the significant heterogeneity, high risk of bias, and low to moderate quality of the randomized controlled trial (RCT).
DOI: https://doi.org/10.37349/eemd.2026.101474
Establishing remission as a clinical goal for carefully selected patients with Type 2 Diabetes Mellitus (T2DM) represents a fundamental shift from the traditional paradigm of lifelong disease management. Short disease duration, preserved C-peptide levels, and overweight or obesity are the central criteria for T2DM remission. T2DM remission may help reduce the psychological burden on patients, improve quality of life, delay disease progression, and reduce the risk of long-term complications. This consensus aims to help physicians establish standardized clinical diagnosis and treatment protocols for T2DM remission in overweight or obese patients with T2DM, and support related research to develop safer and more effective interventions. Notably, T2DM remission is conditional, reversible and population-selective, which is not universally applicable to all T2DM patients across different disease stages and healthcare settings.
Establishing remission as a clinical goal for carefully selected patients with Type 2 Diabetes Mellitus (T2DM) represents a fundamental shift from the traditional paradigm of lifelong disease management. Short disease duration, preserved C-peptide levels, and overweight or obesity are the central criteria for T2DM remission. T2DM remission may help reduce the psychological burden on patients, improve quality of life, delay disease progression, and reduce the risk of long-term complications. This consensus aims to help physicians establish standardized clinical diagnosis and treatment protocols for T2DM remission in overweight or obese patients with T2DM, and support related research to develop safer and more effective interventions. Notably, T2DM remission is conditional, reversible and population-selective, which is not universally applicable to all T2DM patients across different disease stages and healthcare settings.
DOI: https://doi.org/10.37349/eemd.2026.101473
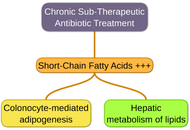
The emerging field of immunometabolism has established that the metabolic pathways governing immune cell function—glycolysis, oxidative phosphorylation, fatty acid oxidation, and amino acid metabolism—are fundamental determinants of immune responses in health and disease. This review synthesizes current evidence on how dietary inputs serve as primary environmental modulators of this immunometabolism programming. We detail the mechanisms by which macronutrients (carbohydrates, lipids, proteins), micronutrients, and specific dietary patterns (e.g., Western, Mediterranean, ketogenic) engage key nutrient-sensing pathways (mechanistic target of rapamycin [mTOR], AMP-activated protein kinase [AMPK], hypoxia-inducible factor-1α [HIF-1α], peroxisome proliferator-activated receptor [PPARs]) to rewire immune cell metabolism and influence functional phenotypes. A central role is afforded to the gut microbiota as a critical intermediary, translating diet into immunoregulatory signals, such as short-chain fatty acids. We further explore how obesogenic diets disrupt this network to fuel chronic low-grade inflammation (metaflammation), driving the pathophysiology of common metabolic diseases, including obesity, type 2 diabetes, non-alcoholic fatty liver disease (NAFLD), and atherosclerosis. Finally, we evaluate therapeutic nutritional strategies—from nutraceuticals and probiotics to the promise of precision nutrition—designed to recalibrate immunometabolism. This review underscores that diet is a powerful, modifiable lever of immunity, positioning targeted nutritional intervention as a pivotal strategy for preventing and managing metabolic disease.
The emerging field of immunometabolism has established that the metabolic pathways governing immune cell function—glycolysis, oxidative phosphorylation, fatty acid oxidation, and amino acid metabolism—are fundamental determinants of immune responses in health and disease. This review synthesizes current evidence on how dietary inputs serve as primary environmental modulators of this immunometabolism programming. We detail the mechanisms by which macronutrients (carbohydrates, lipids, proteins), micronutrients, and specific dietary patterns (e.g., Western, Mediterranean, ketogenic) engage key nutrient-sensing pathways (mechanistic target of rapamycin [mTOR], AMP-activated protein kinase [AMPK], hypoxia-inducible factor-1α [HIF-1α], peroxisome proliferator-activated receptor [PPARs]) to rewire immune cell metabolism and influence functional phenotypes. A central role is afforded to the gut microbiota as a critical intermediary, translating diet into immunoregulatory signals, such as short-chain fatty acids. We further explore how obesogenic diets disrupt this network to fuel chronic low-grade inflammation (metaflammation), driving the pathophysiology of common metabolic diseases, including obesity, type 2 diabetes, non-alcoholic fatty liver disease (NAFLD), and atherosclerosis. Finally, we evaluate therapeutic nutritional strategies—from nutraceuticals and probiotics to the promise of precision nutrition—designed to recalibrate immunometabolism. This review underscores that diet is a powerful, modifiable lever of immunity, positioning targeted nutritional intervention as a pivotal strategy for preventing and managing metabolic disease.
DOI: https://doi.org/10.37349/eemd.2026.101472
Metabolic diseases, including obesity, insulin resistance, and type 2 diabetes mellitus, are increasingly recognized as conditions characterized by chronic low-grade inflammation driven by dysregulated cytokine signaling. Persistent elevation of pro-inflammatory mediators disrupts insulin signaling and contributes to metabolic dysfunction. Nutritional interventions capable of restoring cytokine balance are emerging as promising adjunct strategies for metabolic disease management. Chickpea (Cicer arietinum L.), a widely consumed legume, is rich in polyphenols, saponins, dietary fiber, and bioactive peptides with potential immunometabolic benefits. This review critically summarizes the role of chickpea bioactives in modulating cytokine signaling networks, with particular emphasis on the IL-6-JAK-STAT3-SOCS3 axis and NF-κB pathway. Chickpea components exert antioxidant and anti-inflammatory effects, suppress pro-inflammatory cytokine production, and may improve insulin sensitivity. Additionally, their potential chemoprotective effects in obesity-associated metabolic disorders are discussed. Furthermore, this review highlights key gaps in mechanistic and translational research and proposes future directions for pathway-oriented investigations. Although current evidence supports the therapeutic potential of chickpea, further mechanistic and clinical validation is required.
Metabolic diseases, including obesity, insulin resistance, and type 2 diabetes mellitus, are increasingly recognized as conditions characterized by chronic low-grade inflammation driven by dysregulated cytokine signaling. Persistent elevation of pro-inflammatory mediators disrupts insulin signaling and contributes to metabolic dysfunction. Nutritional interventions capable of restoring cytokine balance are emerging as promising adjunct strategies for metabolic disease management. Chickpea (Cicer arietinum L.), a widely consumed legume, is rich in polyphenols, saponins, dietary fiber, and bioactive peptides with potential immunometabolic benefits. This review critically summarizes the role of chickpea bioactives in modulating cytokine signaling networks, with particular emphasis on the IL-6-JAK-STAT3-SOCS3 axis and NF-κB pathway. Chickpea components exert antioxidant and anti-inflammatory effects, suppress pro-inflammatory cytokine production, and may improve insulin sensitivity. Additionally, their potential chemoprotective effects in obesity-associated metabolic disorders are discussed. Furthermore, this review highlights key gaps in mechanistic and translational research and proposes future directions for pathway-oriented investigations. Although current evidence supports the therapeutic potential of chickpea, further mechanistic and clinical validation is required.
DOI: https://doi.org/10.37349/eemd.2026.101471
This article belongs to the special issue Role of Dysregulated Cytokine Signaling Pathways in Metabolic Disease
Obesity, diabetes mellitus (DM), metabolic dysfunction-associated steatotic liver disease (MASLD), and cardiovascular diseases (CVDs) share pathogenic mechanisms like oxidative stress and inflammation. Resveratrol (RSV) offers therapeutic potential by activating the sirtuin (SIRT) signaling network. This review synthesizes RSV’s pharmacological impacts on adipose, pancreatic, hepatic, and cardiovascular tissues, focusing on the AMPK/SIRT1/PGC-1α axis, PI3K/AKT pathways, and epigenetic modulations. Despite robust preclinical data, a significant translational gap exists. Clinical evidence is heterogeneous, often contradicting animal studies due to varying dosages, durations, and population characteristics. RSV acts as a pan-SIRT activator, though its precise SIRT1 activation mechanism, direct or via NAD+ modulation, remains debated. In obesity, RSV promotes adipose beiging and thermogenesis, yet clinical weight loss is modest. For DM, it preserves β-cell function and improves insulin sensitivity, primarily benefiting diabetic populations with variable glycemic outcomes. In MASLD, RSV ameliorates steatosis and fibrosis in models, but large-scale human trials confirming histological benefits are lacking. Regarding CVDs, RSV protects against endothelial dysfunction and inflammation, showing minor improvements in biomarkers like blood pressure, though hard endpoints need validation. Major limitations hinder clinical efficacy, such as poor oral bioavailability, rapid metabolism, and significant interindividual pharmacokinetic variability. The lack of standardized formulations further complicates systemic exposure. Nevertheless, the RSV-SIRT axis remains a unified metabolic and epigenetic modulator, stabilizing cellular microenvironments across organ systems. It represents a promising target for complex metabolic syndromes. Future research should prioritize overcoming bioavailability challenges through novel delivery systems and investigating synergistic combinatorial therapies to bridge the gap between preclinical promise and clinical reality.
Obesity, diabetes mellitus (DM), metabolic dysfunction-associated steatotic liver disease (MASLD), and cardiovascular diseases (CVDs) share pathogenic mechanisms like oxidative stress and inflammation. Resveratrol (RSV) offers therapeutic potential by activating the sirtuin (SIRT) signaling network. This review synthesizes RSV’s pharmacological impacts on adipose, pancreatic, hepatic, and cardiovascular tissues, focusing on the AMPK/SIRT1/PGC-1α axis, PI3K/AKT pathways, and epigenetic modulations. Despite robust preclinical data, a significant translational gap exists. Clinical evidence is heterogeneous, often contradicting animal studies due to varying dosages, durations, and population characteristics. RSV acts as a pan-SIRT activator, though its precise SIRT1 activation mechanism, direct or via NAD+ modulation, remains debated. In obesity, RSV promotes adipose beiging and thermogenesis, yet clinical weight loss is modest. For DM, it preserves β-cell function and improves insulin sensitivity, primarily benefiting diabetic populations with variable glycemic outcomes. In MASLD, RSV ameliorates steatosis and fibrosis in models, but large-scale human trials confirming histological benefits are lacking. Regarding CVDs, RSV protects against endothelial dysfunction and inflammation, showing minor improvements in biomarkers like blood pressure, though hard endpoints need validation. Major limitations hinder clinical efficacy, such as poor oral bioavailability, rapid metabolism, and significant interindividual pharmacokinetic variability. The lack of standardized formulations further complicates systemic exposure. Nevertheless, the RSV-SIRT axis remains a unified metabolic and epigenetic modulator, stabilizing cellular microenvironments across organ systems. It represents a promising target for complex metabolic syndromes. Future research should prioritize overcoming bioavailability challenges through novel delivery systems and investigating synergistic combinatorial therapies to bridge the gap between preclinical promise and clinical reality.
DOI: https://doi.org/10.37349/eemd.2026.101470
Aim:
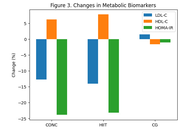
The aim of this study was to compare the effects of high-intensity interval training (HIIT) and concurrent training (CONC) on body composition and metabolic profile in postmenopausal women.
Methods:
Forty-five postmenopausal women with overweight or obesity (50–65 years) were randomly assigned to one of three groups: HIIT group, CONC group, or control group (CG). All groups underwent a 12-week intervention, consisting of three training sessions per week, scheduled on alternate days. All dependent variables (body composition, lipid, or glycemic markers) were assessed before and after a 12-week intervention period.
Results:
The CONC and HIIT groups showed anthropometric improvements compared to the CG. In this regard, CONC and HIIT significantly (P < 0.05) reduced their body weight and body mass index (BMI) compared with the CG. This reduction was due to a decrease in fat mass, mainly in the abdominal area, as reflected by the reduction in the waist-to-hip ratio. Participants in the CONC group showed greater reductions in body weight, BMI, and body fat percentage compared with the HIIT group, while both exercise interventions produced similar improvements in metabolic biomarkers. Regarding circulating parameters, CONC and HIIT significantly (P < 0.05) reduced circulating triglycerides, total cholesterol, and LDL-cholesterol, which resulted in a decrease in the atherogenic index of plasma (AIP, calculated as log[TG/HDL-C]) compared with CG. Blood glucose and insulin levels also decreased significantly (P < 0.05) in CONC and HIIT compared with CG, with a consequent reduction in the homeostatic model assessment-insulin resistance (HOMA-IR).
Conclusions:
A 12-week program of HIIT or CONC training represents an effective strategy for improving body fat reduction and metabolic profile in sedentary postmenopausal women with overweight or obesity [ClinicalTrials.gov, identifier (ID NCT07302191)].
Aim:
The aim of this study was to compare the effects of high-intensity interval training (HIIT) and concurrent training (CONC) on body composition and metabolic profile in postmenopausal women.
Methods:
Forty-five postmenopausal women with overweight or obesity (50–65 years) were randomly assigned to one of three groups: HIIT group, CONC group, or control group (CG). All groups underwent a 12-week intervention, consisting of three training sessions per week, scheduled on alternate days. All dependent variables (body composition, lipid, or glycemic markers) were assessed before and after a 12-week intervention period.
Results:
The CONC and HIIT groups showed anthropometric improvements compared to the CG. In this regard, CONC and HIIT significantly (P < 0.05) reduced their body weight and body mass index (BMI) compared with the CG. This reduction was due to a decrease in fat mass, mainly in the abdominal area, as reflected by the reduction in the waist-to-hip ratio. Participants in the CONC group showed greater reductions in body weight, BMI, and body fat percentage compared with the HIIT group, while both exercise interventions produced similar improvements in metabolic biomarkers. Regarding circulating parameters, CONC and HIIT significantly (P < 0.05) reduced circulating triglycerides, total cholesterol, and LDL-cholesterol, which resulted in a decrease in the atherogenic index of plasma (AIP, calculated as log[TG/HDL-C]) compared with CG. Blood glucose and insulin levels also decreased significantly (P < 0.05) in CONC and HIIT compared with CG, with a consequent reduction in the homeostatic model assessment-insulin resistance (HOMA-IR).
Conclusions:
A 12-week program of HIIT or CONC training represents an effective strategy for improving body fat reduction and metabolic profile in sedentary postmenopausal women with overweight or obesity [ClinicalTrials.gov, identifier (ID NCT07302191)].
DOI: https://doi.org/10.37349/eemd.2026.101469
This article belongs to the special issue Metabolic Syndrome in Menopause
The global rise in consumption of added sugars and confectionery parallels the increasing prevalence of obesity, metabolic dysfunction, and male hypogonadism. Testosterone is essential for male reproductive, metabolic, and cardiovascular health, and growing evidence indicates that excessive sugar intake may disrupt hormonal regulation. This narrative review synthesizes data from human observational and interventional studies and experimental animal models to evaluate the effects of sugar consumption on testosterone homeostasis and male reproductive outcomes. Acute glucose ingestion is associated with hyperinsulinemia and inflammatory cytokine release, which may contribute to transient reductions in circulating testosterone of approximately 20–30%, although findings vary across populations and study designs. Chronic high-sugar intake, particularly from sugar-sweetened beverages, promotes oxidative stress, adiposity, insulin resistance, and leptin dysregulation, which may collectively impair Leydig cell steroidogenesis and contribute to testosterone suppression. Animal studies consistently demonstrate testicular structural damage, downregulation of steroidogenic enzymes, and impaired spermatogenesis under high-sugar dietary conditions. Epidemiological studies associate frequent intake of sugar-sweetened beverages and confectionery with lower testosterone levels and poorer semen parameters. Emerging evidence suggests partial reversibility with dietary interventions emphasizing reduced sugar intake and increased antioxidant consumption. Overall, current data support a biologically plausible link between excessive sugar intake and impaired testosterone regulation, underscoring the need for longitudinal studies and public health strategies targeting added sugar reduction.
The global rise in consumption of added sugars and confectionery parallels the increasing prevalence of obesity, metabolic dysfunction, and male hypogonadism. Testosterone is essential for male reproductive, metabolic, and cardiovascular health, and growing evidence indicates that excessive sugar intake may disrupt hormonal regulation. This narrative review synthesizes data from human observational and interventional studies and experimental animal models to evaluate the effects of sugar consumption on testosterone homeostasis and male reproductive outcomes. Acute glucose ingestion is associated with hyperinsulinemia and inflammatory cytokine release, which may contribute to transient reductions in circulating testosterone of approximately 20–30%, although findings vary across populations and study designs. Chronic high-sugar intake, particularly from sugar-sweetened beverages, promotes oxidative stress, adiposity, insulin resistance, and leptin dysregulation, which may collectively impair Leydig cell steroidogenesis and contribute to testosterone suppression. Animal studies consistently demonstrate testicular structural damage, downregulation of steroidogenic enzymes, and impaired spermatogenesis under high-sugar dietary conditions. Epidemiological studies associate frequent intake of sugar-sweetened beverages and confectionery with lower testosterone levels and poorer semen parameters. Emerging evidence suggests partial reversibility with dietary interventions emphasizing reduced sugar intake and increased antioxidant consumption. Overall, current data support a biologically plausible link between excessive sugar intake and impaired testosterone regulation, underscoring the need for longitudinal studies and public health strategies targeting added sugar reduction.
DOI: https://doi.org/10.37349/eemd.2026.101468
Circadian rhythms are intrinsic 24-hour cycles that coordinate key metabolic processes, including glucose homeostasis, lipid metabolism, and energy expenditure. Disruption of these rhythms, due to sleep disturbances, shift work, or irregular feeding schedules, contributes to the development of obesity, insulin resistance, and dyslipidemia. Core clock genes, including circadian locomotor output cycles kaput (CLOCK), brain and muscle ARNT-like 1 (BMAL1), period gene (PER), and cryptochrome (CRY), play a central role in orchestrating these metabolic pathways. Chronotherapy, aligning lifestyle, behavioral, and pharmacologic interventions with circadian timing, represents a promising, yet underexplored, strategy for metabolic disease management. Evidence suggests that interventions such as time-restricted feeding, light therapy, pharmacologic modulators of clock gene expression, and wearable technology can improve glucose control, lipid profiles, and body weight. This review synthesizes current knowledge on the molecular regulation of metabolism by circadian clocks, elucidates mechanistic links between rhythm disruption and metabolic dysfunction, and explores translational strategies to restore circadian homeostasis. By targeting circadian rhythms, personalized and cost-effective interventions can be developed to mitigate the global burden of metabolic disorders. Future research should focus on large-scale clinical trials, precision chronotherapy, and integration of wearable devices to optimize the timing of interventions, ultimately enhancing treatment efficacy and long-term metabolic health.
Circadian rhythms are intrinsic 24-hour cycles that coordinate key metabolic processes, including glucose homeostasis, lipid metabolism, and energy expenditure. Disruption of these rhythms, due to sleep disturbances, shift work, or irregular feeding schedules, contributes to the development of obesity, insulin resistance, and dyslipidemia. Core clock genes, including circadian locomotor output cycles kaput (CLOCK), brain and muscle ARNT-like 1 (BMAL1), period gene (PER), and cryptochrome (CRY), play a central role in orchestrating these metabolic pathways. Chronotherapy, aligning lifestyle, behavioral, and pharmacologic interventions with circadian timing, represents a promising, yet underexplored, strategy for metabolic disease management. Evidence suggests that interventions such as time-restricted feeding, light therapy, pharmacologic modulators of clock gene expression, and wearable technology can improve glucose control, lipid profiles, and body weight. This review synthesizes current knowledge on the molecular regulation of metabolism by circadian clocks, elucidates mechanistic links between rhythm disruption and metabolic dysfunction, and explores translational strategies to restore circadian homeostasis. By targeting circadian rhythms, personalized and cost-effective interventions can be developed to mitigate the global burden of metabolic disorders. Future research should focus on large-scale clinical trials, precision chronotherapy, and integration of wearable devices to optimize the timing of interventions, ultimately enhancing treatment efficacy and long-term metabolic health.
DOI: https://doi.org/10.37349/eemd.2026.101467
Osteoarthritis (OA) is the most prevalent form of arthritis and a leading cause of disability worldwide. Epidemiological studies indicate that its global prevalence is rising, particularly among women, who often experience more severe disease than men. This sex disparity is most pronounced around menopause and is influenced by female-specific biological and hormonal factors, joint morphology, reproductive history, and sex-specific comorbidities that contribute to disease onset and progression. A mechanistic understanding of these factors is essential to identify individuals at risk, implement preventive strategies, enable early diagnosis, and mitigate complications, ultimately preserving function and quality of life. This review focuses on the determinants underlying the higher incidence and severity of OA in women, highlighting the interplay between hormonal changes, anatomy, and systemic factors.
Osteoarthritis (OA) is the most prevalent form of arthritis and a leading cause of disability worldwide. Epidemiological studies indicate that its global prevalence is rising, particularly among women, who often experience more severe disease than men. This sex disparity is most pronounced around menopause and is influenced by female-specific biological and hormonal factors, joint morphology, reproductive history, and sex-specific comorbidities that contribute to disease onset and progression. A mechanistic understanding of these factors is essential to identify individuals at risk, implement preventive strategies, enable early diagnosis, and mitigate complications, ultimately preserving function and quality of life. This review focuses on the determinants underlying the higher incidence and severity of OA in women, highlighting the interplay between hormonal changes, anatomy, and systemic factors.
DOI: https://doi.org/10.37349/eemd.2026.101466
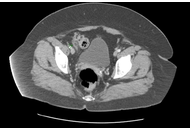
Epiploic appendagitis is a rare, self-limiting inflammatory condition of the colonic epiploic appendages. It commonly presents with acute focal lower quadrant abdominal pain and may mimic appendicitis, colitis, or diverticulitis. Rapid weight loss has been proposed as a potential predisposing factor, although clinical evidence remains limited. This report describes a case of epiploic appendagitis occurring in temporal association with substantial and relatively rapid weight reduction during treatment with tirzepatide, a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist. A 45-year-old individual with a history of obesity, prediabetes, hypertension, hypothyroidism, and inflammatory bowel syndrome presented to primary care with right lower quadrant abdominal pain. Initial evaluation attributed symptoms to constipation; however, pain progressed despite management. Computed tomography (CT) of the abdomen and pelvis with contrast was obtained due to concern for appendicitis and demonstrated imaging findings consistent with epiploic appendagitis localized to the cecum. The patient had experienced clinically significant and relatively rapid weight loss during tirzepatide dose escalation prior to presentation. Management was conservative with nonsteroidal anti-inflammatory drugs and supportive care, without surgical intervention. Symptoms resolved completely within two weeks, and tirzepatide therapy was continued without recurrence. Although epiploic appendagitis has not been identified as a safety signal in randomized trials, systematic reviews, or pharmacovigilance analyses of GLP-1/GIP receptor agonists, this case highlights epiploic appendagitis as an important diagnostic consideration in patients presenting with focal abdominal pain during periods of substantial weight loss. Awareness of this uncommon condition may help prevent misdiagnosis and unnecessary interventions as pharmacologic weight loss therapies become more widely used.
Epiploic appendagitis is a rare, self-limiting inflammatory condition of the colonic epiploic appendages. It commonly presents with acute focal lower quadrant abdominal pain and may mimic appendicitis, colitis, or diverticulitis. Rapid weight loss has been proposed as a potential predisposing factor, although clinical evidence remains limited. This report describes a case of epiploic appendagitis occurring in temporal association with substantial and relatively rapid weight reduction during treatment with tirzepatide, a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist. A 45-year-old individual with a history of obesity, prediabetes, hypertension, hypothyroidism, and inflammatory bowel syndrome presented to primary care with right lower quadrant abdominal pain. Initial evaluation attributed symptoms to constipation; however, pain progressed despite management. Computed tomography (CT) of the abdomen and pelvis with contrast was obtained due to concern for appendicitis and demonstrated imaging findings consistent with epiploic appendagitis localized to the cecum. The patient had experienced clinically significant and relatively rapid weight loss during tirzepatide dose escalation prior to presentation. Management was conservative with nonsteroidal anti-inflammatory drugs and supportive care, without surgical intervention. Symptoms resolved completely within two weeks, and tirzepatide therapy was continued without recurrence. Although epiploic appendagitis has not been identified as a safety signal in randomized trials, systematic reviews, or pharmacovigilance analyses of GLP-1/GIP receptor agonists, this case highlights epiploic appendagitis as an important diagnostic consideration in patients presenting with focal abdominal pain during periods of substantial weight loss. Awareness of this uncommon condition may help prevent misdiagnosis and unnecessary interventions as pharmacologic weight loss therapies become more widely used.
DOI: https://doi.org/10.37349/eemd.2026.101465
The hypothesis that early-life antibiotic exposure predisposes to obesity has, over the past decade, gained substantial traction across both biomedical literature and public discourse. Its appeal lies in a seemingly coherent mechanistic framework: disruption of the developing intestinal microbiota is presumed to induce long-lasting alterations in metabolic homeostasis, thereby promoting increased adiposity. However, reported effect sizes are consistently modest, with odds ratios typically ranging from 1.1 to 1.3, values that approach the limits of residual confounding and statistical imprecision. Studies incorporating rigorous adjustment for familial environment, socioeconomic status, and dietary patterns observe a complete loss of the association, underscoring the dominant influence of these confounders. This review revisits the conceptual emergence and sustained prominence of the antibiotic-obesity paradigm, positioning it as a case study in the amplification of weak epidemiological signals through mechanistic plausibility. Notwithstanding its methodological limitations, the hypothesis has exerted a constructive influence by fostering more judicious antibiotic use and stimulating renewed investigation into host-microbiota interactions within the context of metabolic disease.
The hypothesis that early-life antibiotic exposure predisposes to obesity has, over the past decade, gained substantial traction across both biomedical literature and public discourse. Its appeal lies in a seemingly coherent mechanistic framework: disruption of the developing intestinal microbiota is presumed to induce long-lasting alterations in metabolic homeostasis, thereby promoting increased adiposity. However, reported effect sizes are consistently modest, with odds ratios typically ranging from 1.1 to 1.3, values that approach the limits of residual confounding and statistical imprecision. Studies incorporating rigorous adjustment for familial environment, socioeconomic status, and dietary patterns observe a complete loss of the association, underscoring the dominant influence of these confounders. This review revisits the conceptual emergence and sustained prominence of the antibiotic-obesity paradigm, positioning it as a case study in the amplification of weak epidemiological signals through mechanistic plausibility. Notwithstanding its methodological limitations, the hypothesis has exerted a constructive influence by fostering more judicious antibiotic use and stimulating renewed investigation into host-microbiota interactions within the context of metabolic disease.
DOI: https://doi.org/10.37349/eemd.2026.101464
Aim:
Necrotizing fasciitis (NF) is a severe and early challenging-to-identify complication of diabetic foot (DF). This study aimed to develop and validate a novel risk assessment model for NF with DF patients utilizing conventional clinical indicators.
Methods:
A retrospective analysis was conducted on 815 DF patients admitted to the First Affiliated Hospital of Chongqing Medical University between October 2018 and April 2022. Based on the presence of NF, patients were stratified into a DF group (n = 703) and a DF complicated with NF (DNF) group (n = 112). Clinically and statistically significant variables were converted into categorical form. A new risk assessment for DNF (NRADNF) nomogram was developed via multivariable stepwise logistic regression. Model performance was evaluated using the area under the receiver operating characteristic curve (AUC) for discriminative ability, the Hosmer-Lemeshow goodness-of-fit test for calibration, decision curve analysis (DCA) for clinical utility, and bootstrap resampling for stability.
Results:
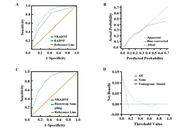
The final NRADNF model incorporated six indicators: age < 60 years, body temperature ≥ 38°C, foot skin necrosis, neutrophil-to-lymphocyte ratio (NLR) ≥ 8.5, hypersensitive C-reactive protein > 20 mg/L, and hemoglobin ≤ 100 g/L. The model demonstrated favorable predictive performance with an AUC of 0.815 (95% CI: 0.773, 0.857), and it was significantly superior to the RADNF model by our team (P = 0.027). Calibration curves and the Hosmer-Lemeshow test indicated good accuracy. DCA confirmed the model’s clinical net benefit, and internal validation via bootstrap resampling supported its stability.
Conclusions:
Based on its favorable predictive performance and accessible indicators, the NRADNF model is suitable for preliminary screening of DNF in clinical practice.
Aim:
Necrotizing fasciitis (NF) is a severe and early challenging-to-identify complication of diabetic foot (DF). This study aimed to develop and validate a novel risk assessment model for NF with DF patients utilizing conventional clinical indicators.
Methods:
A retrospective analysis was conducted on 815 DF patients admitted to the First Affiliated Hospital of Chongqing Medical University between October 2018 and April 2022. Based on the presence of NF, patients were stratified into a DF group (n = 703) and a DF complicated with NF (DNF) group (n = 112). Clinically and statistically significant variables were converted into categorical form. A new risk assessment for DNF (NRADNF) nomogram was developed via multivariable stepwise logistic regression. Model performance was evaluated using the area under the receiver operating characteristic curve (AUC) for discriminative ability, the Hosmer-Lemeshow goodness-of-fit test for calibration, decision curve analysis (DCA) for clinical utility, and bootstrap resampling for stability.
Results:
The final NRADNF model incorporated six indicators: age < 60 years, body temperature ≥ 38°C, foot skin necrosis, neutrophil-to-lymphocyte ratio (NLR) ≥ 8.5, hypersensitive C-reactive protein > 20 mg/L, and hemoglobin ≤ 100 g/L. The model demonstrated favorable predictive performance with an AUC of 0.815 (95% CI: 0.773, 0.857), and it was significantly superior to the RADNF model by our team (P = 0.027). Calibration curves and the Hosmer-Lemeshow test indicated good accuracy. DCA confirmed the model’s clinical net benefit, and internal validation via bootstrap resampling supported its stability.
Conclusions:
Based on its favorable predictive performance and accessible indicators, the NRADNF model is suitable for preliminary screening of DNF in clinical practice.
DOI: https://doi.org/10.37349/eemd.2026.101463
Aim:
In Mexico, 18.3% of patients over 20 years of age suffer from type 2 diabetes mellitus (T2DM). Visceral fat has been identified as a risk factor for developing T2DM, considering that its effect depends mainly on the amount, it has been proposed that its location also participates in the genesis of T2DM. This paper aims to analyze whether the location of fatty depots participates in the appearance of T2DM in patients with metabolic syndrome.
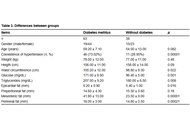
Methods:
A total of 101 patients with metabolic syndrome according to the criteria of the International Diabetes Federation were included. In all of them, epicardial fat (EF) was measured by echocardiography, according to the Iacobelis criteria. Preperitoneal fat (PreF), mesenteric fat (MF), and perirenal fat (PF) were also measured by ultrasound. The statistical methods used were the odds ratio (OR) and Fisher’s exact test.
Results:
We found a significant association between EF thickness (OR 8.28, 95% CI 2.16–31.70, p = 0.001) and MF (OR 4.27, 95% CI 1.63–11.13, p = 0.0037) with T2DM, 60% of patients with increased PF presented T2DM. Interestingly, no patient with a PF less than 10 mm presented with T2DM. We found no association between PreF and T2DM (OR 0.88, 95% CI 0.32–2.40).
Conclusions:
The results suggest that the location of adipose tissue plays an important role in the development of T2DM. This may be due to the type of adipocytokines secreted by the various fat deposits and their metabolic effects.
Aim:
In Mexico, 18.3% of patients over 20 years of age suffer from type 2 diabetes mellitus (T2DM). Visceral fat has been identified as a risk factor for developing T2DM, considering that its effect depends mainly on the amount, it has been proposed that its location also participates in the genesis of T2DM. This paper aims to analyze whether the location of fatty depots participates in the appearance of T2DM in patients with metabolic syndrome.
Methods:
A total of 101 patients with metabolic syndrome according to the criteria of the International Diabetes Federation were included. In all of them, epicardial fat (EF) was measured by echocardiography, according to the Iacobelis criteria. Preperitoneal fat (PreF), mesenteric fat (MF), and perirenal fat (PF) were also measured by ultrasound. The statistical methods used were the odds ratio (OR) and Fisher’s exact test.
Results:
We found a significant association between EF thickness (OR 8.28, 95% CI 2.16–31.70, p = 0.001) and MF (OR 4.27, 95% CI 1.63–11.13, p = 0.0037) with T2DM, 60% of patients with increased PF presented T2DM. Interestingly, no patient with a PF less than 10 mm presented with T2DM. We found no association between PreF and T2DM (OR 0.88, 95% CI 0.32–2.40).
Conclusions:
The results suggest that the location of adipose tissue plays an important role in the development of T2DM. This may be due to the type of adipocytokines secreted by the various fat deposits and their metabolic effects.
DOI: https://doi.org/10.37349/eemd.2026.101462
This article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Diabetes and metabolic dysfunction represent growing global health challenges, and current therapies mitigate hyperglycemia without sufficiently altering the underlying disease processes. Rapid advances in regenerative medicine, gene editing, and nano-enabled drug delivery are reshaping therapeutic possibilities, offering the potential to restore β-cell function, enhance insulin sensitivity, and personalize care at an unprecedented scale. This review synthesizes emerging therapeutic strategies with the greatest translational promise, including stem cell-derived islet replacement, immune-evasive encapsulation devices, CRISPR-based gene correction, and targeted or glucose-responsive nanocarriers engineered for noninvasive insulin delivery. Complementary advances in multi-omics profiling, proteogenomics, microbiome science, and artificial intelligence are enabling stratification of patients based on molecular signatures, optimizing therapeutic selection, and predicting clinical outcomes. Despite remarkable breakthroughs—such as the early-phase clinical success of stem cell-derived β-cell replacement and organ-targeted lipid nanoparticles (LNPs)—significant barriers remain, including immunogenicity, off-target editing, scalability, ethical concerns, and long-term safety. By integrating mechanistic insights with translational developments, this review outlines a forward-looking perspective on next-generation treatments poised to shift diabetes care from glycemic management toward disease modification and personalized metabolic restoration.
Diabetes and metabolic dysfunction represent growing global health challenges, and current therapies mitigate hyperglycemia without sufficiently altering the underlying disease processes. Rapid advances in regenerative medicine, gene editing, and nano-enabled drug delivery are reshaping therapeutic possibilities, offering the potential to restore β-cell function, enhance insulin sensitivity, and personalize care at an unprecedented scale. This review synthesizes emerging therapeutic strategies with the greatest translational promise, including stem cell-derived islet replacement, immune-evasive encapsulation devices, CRISPR-based gene correction, and targeted or glucose-responsive nanocarriers engineered for noninvasive insulin delivery. Complementary advances in multi-omics profiling, proteogenomics, microbiome science, and artificial intelligence are enabling stratification of patients based on molecular signatures, optimizing therapeutic selection, and predicting clinical outcomes. Despite remarkable breakthroughs—such as the early-phase clinical success of stem cell-derived β-cell replacement and organ-targeted lipid nanoparticles (LNPs)—significant barriers remain, including immunogenicity, off-target editing, scalability, ethical concerns, and long-term safety. By integrating mechanistic insights with translational developments, this review outlines a forward-looking perspective on next-generation treatments poised to shift diabetes care from glycemic management toward disease modification and personalized metabolic restoration.
DOI: https://doi.org/10.37349/eemd.2026.101461
This article belongs to the special issue Innovative Strategies for Diabetes and Metabolic Disorders: Current and Future Directions
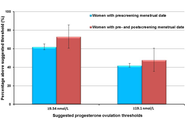
The dominant paradigm for healthy ageing in women+ (all genders) focuses on estrogen and sees the menopause, per se, as a major health problem (with low estrogen and progesterone levels). In reality, the risks for diseases that increase at older ages originate during the menstruating years. Rarely discussed evidence supports the central role of progesterone and normally ovulatory menstrual cycles in preventing early cardiovascular disease, fragility fractures, dementia, and cancers. Menstrual cycles with normal and predictable lengths but disturbed ovulation, including short luteal phases with lower progesterone production as well as anovulation without progesterone, likely occur in over 25% of all such cycles. These Subclinical Ovulatory Disturbances are usually an adaptive and protective response to physiological, sociocultural, or emotional stressors. Ovulatory disturbances and risks for health issues during ageing are intrinsically related to the social determinants of health—wholesome food, plentiful physical activity, strong communities, and access to timely and appropriate medical care. This review discusses the empirical evidence that normal ovulation and progesterone production during the premenopausal years lead to the prevention of early heart attacks and fragility fractures. Few studies document the effects of prevalent Subclinical Ovulatory Disturbances on brain issues (sleep, night sweats, ischemic strokes, pain, and addictions) and cancer risks. Serious gaps in women+’s fundamental reproductive physiology must be addressed with unbiased (population-based), rigorously collected longitudinal physiological, hormonal, and sociocultural data. Progesterone therapy during perimenopause and menopause also indirectly leads to healthy ageing through effective treatment of night sweats, hot flushes, and disturbed sleep, which are associated with cardiovascular problems and osteoporosis. Not only is progesterone effective for vasomotor symptoms in menopause, but also effective in perimenopause, a time of high and chaotic estrogen levels. In sum, strong summarized evidence suggests that progesterone and ovulation need further exploration for their important roles in promoting healthy ageing for women+.
The dominant paradigm for healthy ageing in women+ (all genders) focuses on estrogen and sees the menopause, per se, as a major health problem (with low estrogen and progesterone levels). In reality, the risks for diseases that increase at older ages originate during the menstruating years. Rarely discussed evidence supports the central role of progesterone and normally ovulatory menstrual cycles in preventing early cardiovascular disease, fragility fractures, dementia, and cancers. Menstrual cycles with normal and predictable lengths but disturbed ovulation, including short luteal phases with lower progesterone production as well as anovulation without progesterone, likely occur in over 25% of all such cycles. These Subclinical Ovulatory Disturbances are usually an adaptive and protective response to physiological, sociocultural, or emotional stressors. Ovulatory disturbances and risks for health issues during ageing are intrinsically related to the social determinants of health—wholesome food, plentiful physical activity, strong communities, and access to timely and appropriate medical care. This review discusses the empirical evidence that normal ovulation and progesterone production during the premenopausal years lead to the prevention of early heart attacks and fragility fractures. Few studies document the effects of prevalent Subclinical Ovulatory Disturbances on brain issues (sleep, night sweats, ischemic strokes, pain, and addictions) and cancer risks. Serious gaps in women+’s fundamental reproductive physiology must be addressed with unbiased (population-based), rigorously collected longitudinal physiological, hormonal, and sociocultural data. Progesterone therapy during perimenopause and menopause also indirectly leads to healthy ageing through effective treatment of night sweats, hot flushes, and disturbed sleep, which are associated with cardiovascular problems and osteoporosis. Not only is progesterone effective for vasomotor symptoms in menopause, but also effective in perimenopause, a time of high and chaotic estrogen levels. In sum, strong summarized evidence suggests that progesterone and ovulation need further exploration for their important roles in promoting healthy ageing for women+.
DOI: https://doi.org/10.37349/eemd.2026.101460
This article belongs to the special issue The Fountain of Youth: Decoding the Hormonal Regulation of Aging
