Mini Review
Mini Review

Affiliation:
Cardiology Department of Faulty of Medicine, Abant Izzet Baysal University, Golkoy 14030, Bolu, Turkey
Email: isasincer@yahoo.com
ORCID: https://orcid.org/0000-0003-2399-9585
Explor Endocr Metab Dis. 2025;2:101435 DOI: https://doi.org/10.37349/eemd.2025.101435
Received: January 12, 2025 Accepted: June 17, 2025 Published: June 30, 2025
Academic Editor: Jerzy Beltowski, Medical University of Lublin, Poland
The article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Diabetes affects approximately 463 million people worldwide, and this number is projected to reach 700 million by 2045. The most significant cause of increased mortality among diabetic patients is cardiovascular disease, with heart failure (HF) being one of the most commonly observed conditions within this group. Type 2 diabetes mellitus (T2DM), characterized by insulin resistance, accounts for more than 90% of all diabetes cases. Patients with T2DM have twice the risk of developing HF compared to non-diabetic individuals. The connection between diabetes mellitus (DM) and HF extends beyond the complications of ischemic heart disease, encompassing metabolic disturbances such as glucose toxicity and lipotoxicity resulting from insulin resistance, as well as vascular endothelial dysfunction, microcirculatory abnormalities, and capillary insufficiency. Lifestyle modifications for individuals with T2DM involve engaging in regular physical activity, maintaining a balanced diet, quitting smoking, and reducing alcohol consumption. For patients with reduced ejection fraction HF [heart failure with reduced ejection fraction (HFrEF)] and T2DM, guideline-recommended medical therapies [including ARNI, angiotensin converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARBs), beta-blockers, mineralocorticoid receptor antagonists (MRAs), and sodium glucose co-transporter-2 (SGLT2) inhibitors] should be considered. Recent large randomized controlled trials have demonstrated that SGLT2 inhibitors improve cardiovascular outcomes, including all-cause mortality, independent of diabetes status. This review will focus on the epidemiology, pathophysiology, risk factors for HF development, and treatment approaches in diabetic patients, particularly those with T2DM and systolic HF.
Diabetes affects approximately 463 million people worldwide, and this number is projected to reach 700 million by 2045 [1]. According to 2019 data, 1.5 million people globally died from diabetes and its complications [2]. The most significant cause of increased mortality among diabetic patients is cardiovascular disease, with heart failure (HF) being one of the most commonly observed conditions within this group [3–5].
Type 2 diabetes mellitus (T2DM), which is marked by insulin resistance, represents over 90% of all diabetes cases [6]. Patients with T2DM have twice the risk of developing HF compared to non-diabetic individuals [7]. Therefore, it is crucial for diabetic patients to manage traditional risk factors for HF—such as hypertension (HT), smoking, elevated blood glucose levels, and hyperlipidemia—at optimal levels.
Observational studies suggest that undiagnosed HF may be common in diabetic patients, with approximately 25% having heart failure with reduced ejection fraction (HFrEF) and 75% having heart failure with preserved ejection fraction (HFpEF) [8, 9].
Patients with HF and diabetes typically experience poorer clinical outcomes compared to those without diabetes, often presenting with higher rates of ischemic etiology, increased body mass index (BMI), elevated heart rate, systolic blood pressure, creatinine levels, and N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels [10]. Cardiovascular mortality, including deaths resulting from worsening HF, is 50–90% higher in patients who have both HF and diabetes, irrespective of the HF phenotype [11]. In patients with worsening HFrEF, newly diagnosed prediabetes has been independently linked to an increased long-term risk of all-cause mortality and cardiovascular death, highlighting the critical need for prediabetes screening in this group [12].
The main contributors to HF in individuals with diabetes include coronary artery disease (CAD), chronic kidney disease (CKD), HT, and the direct impact of insulin resistance and hyperglycemia on the myocardium [13]. CAD in diabetic patients is often accelerated, more severe, diffuse, and asymptomatic, which heightens the risk of myocardial infarction (MI) and ischemic myocardial dysfunction. Better blood pressure control is associated with a reduced risk of HF development. Observational data also identify longer diabetes duration, age, increased BMI, and CKD as predictors of HF in diabetic patients. Even in the absence of CAD or HT, complex pathophysiological mechanisms may contribute to myocardial dysfunction [8].
This review will focus on the epidemiology, pathophysiology, risk factors for HF development, and treatment approaches in diabetic patients, particularly those with T2DM and systolic HF.
HF is rapidly increasing in individuals with diabetes mellitus (DM) and is associated with high mortality and morbidity rates [14]. A recent study involving 3.25 million participants highlighted that the presence of DM is associated with a twofold higher incidence of HF. Factors such as longer DM duration and poor glycemic control have been identified as indicators of increased HF risk [15]. However, HF can also develop in young individuals with newly diagnosed DM [16]. Diabetic cardiomyopathy has been shown to be more common in diabetic women than in men, which may be attributed to estrogen’s functional role in regulating insulin sensitivity [14]. Studies have particularly observed higher prevalence rates of HF in women with T2DM [17, 18]. This gender disparity is explained by factors such as distinct hormonal profiles, increased BMI, blood pressure, and the timing of diabetes diagnosis in women [18, 19].
Racial disparities in the prevalence of DM among individuals with HF have been observed. Multiple studies report that the prevalence of DM in HF patients ranges from 47% to 56% among Black, Hispanic, and Native American populations [20, 21].
Since insulin resistance or the development of DM is prevalent among individuals with HF, the relationship between these two conditions is bidirectional. In a registry of 7,488 HF patients, a DM prevalence of 29% was reported [3]. However, the prevalence of DM among HF patients varies across studies. Over 20% of HF patients exhibit pathological glucose homeostasis, with clinical studies on acute HF reporting prevalence rates as high as 47% [9]. Data from various registries show that the prevalence of DM among patients with HF ranges from approximately 25% to 40%, depending on the specific population studied [22].
In T2DM, the primary factor directly and indirectly influencing HF development is hyperglycemia. Glycemic control is an independent predictor of HF in T2DM [23]. Additionally, the duration of diabetes increases the risk of HF by 17% every five years [24]. Furthermore, 70% of T2DM patients have HT [25]. Elevated blood pressure is associated with increased aortic stiffness, more severe cardiac structural and functional abnormalities, coronary microvascular dysfunction, and a higher risk of HF [26–28].
Approximately 60% of T2DM patients are obese, with central abdominal obesity and high fat mass index linked to an increased risk of HF in this population [29–31]. CKD is observed in 40% of T2DM patients and impaired kidney function along with albuminuria are strong independent predictors of HF in T2DM [31]. Dyslipidemia, characterized by elevated non-HDL cholesterol or decreased HDL levels, is also an independent risk factor for HF [32]. Other independent risk factors for HF development include poor glycemic control, hypoglycemia, and excessive variability in glycemic parameters [33, 34].
Reducing or managing these risk factors can lower the risk of HF in T2DM patients. While these risk factors are consistent for both HFrEF and HFpEF, certain characteristics differ between the two groups. Female gender, obesity, and physical inactivity are more common in the HFpEF group, whereas male gender and CAD are more frequently observed in HFrEF [35].
The relationship between DM and HF is not solely based on complications of ischemic heart disease but also involves metabolic disorders such as glucose toxicity and lipotoxicity due to insulin resistance, vascular endothelial dysfunction, microcirculation abnormalities, and capillary insufficiency. It has been suggested that cardiac dysfunction in the absence of significant CAD, HT, or valvular heart disease should be termed “diabetic cardiomyopathy” [36].
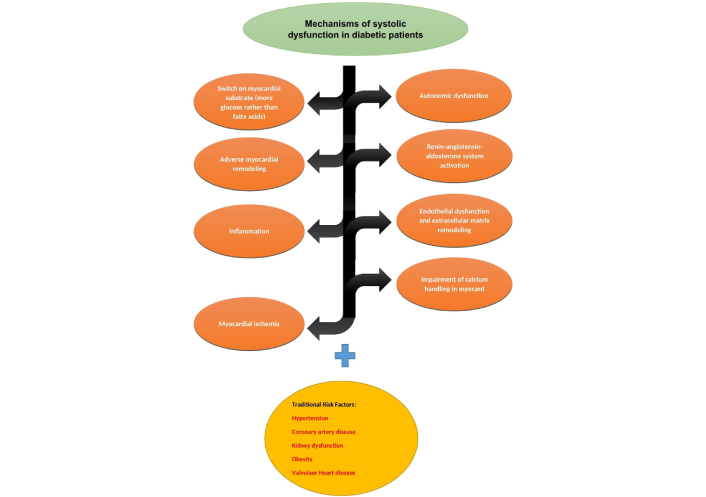
There are different types of HF associated with DM [37]. The development of HF and cardiac dysfunction in DM, along with associated risk factors, is summarized in Figure 1 [38].
Diabetes-induced hyperglycemia and hyperinsulinemia lead to capillary damage, myocardial fibrosis, and mitochondrial dysfunction, contributing to myocardial hypertrophy [39]. Hyperglycemia results in the formation of advanced glycation end products (AGEs), which are glycosylated proteins or lipids formed after prolonged glucose exposure. AGEs cross-link with extracellular matrix proteins, increase fibrosis, and impair myocardial relaxation. Additionally, AGEs promote an increase in cytosolic reactive oxygen species (ROS), inflammation, and intracellular damage [40]. Glycosylated molecules initiate inflammatory signaling, promote apoptosis, fibrotic remodeling, and immune cell infiltration. The accumulation of AGEs is a driving factor for microvascular damage in diabetes.
Chronic activation of the renin-angiotensin-aldosterone system (RAAS) is observed in diabetic patients. Elevated angiotensin II (AT-II) levels cause vasoconstriction, increase afterload, and promote left ventricular (LV) hypertrophy. AT-II also supports collagen production and extracellular matrix protein accumulation, leading to myocardial contractile dysfunction [36]. This condition is associated with cardiomyocyte stiffness and myocardial collagen deposition [37]. Consequently, increased myocardial stiffness results in systolic/diastolic dysfunction, reduced myocardial strain, atrial enlargement, and higher atrial fibrillation prevalence in diabetic patients [41].
Excess free fatty acids, due to DM and obesity, primarily accumulate as triglycerides in adipose tissue. Ectopic fat deposits in non-adipose organs, such as the myocardium, liver, and skeletal muscle, disrupt mitochondrial function and lead to organ dysfunction [42]. Lipotoxicity in cardiomyocytes manifests as fat accumulation and lipid droplets. Increased oxidative stress and inflammation result in cardiac fibrosis and hypertrophy [42].
In the liver and skeletal muscle, fat deposition induces chronic inflammation and insulin resistance, leading to impaired glucose tolerance, dyslipidemia, and HT. Excess fatty acids accumulate as lipid droplets and triglycerides in cells while increasing diacylglycerol and ceramide levels [36]. Diacylglycerol exacerbates insulin resistance and oxidative stress through protein kinase C activation. Ceramide induces mitochondrial dysfunction and oxidative stress, contributing to LV hypertrophy and cardiac dysfunction [43]. Glucagon-like peptide-1 receptor agonists (GLP-1RAs), such as semaglutide, have demonstrated significant benefits in managing HFpEF, particularly in patients with obesity and type 2 diabetes. The STEP-HFpEF trial, a randomized controlled study published in the New England Journal of Medicine, evaluated the effects of semaglutide in this patient population. Participants receiving semaglutide experienced notable improvements in HF symptoms, physical function, and quality of life compared to those on placebo. Additionally, semaglutide led to substantial weight loss and reductions in inflammatory markers, suggesting a multifaceted mechanism of action. These findings highlight the potential of GLP-1RAs as a therapeutic option for HFpEF, addressing both metabolic and cardiovascular aspects of the disease [44].
In diabetes, progressive mitochondrial dysfunction in cardiomyocytes leads to lipid accumulation, increased ROS production, and exacerbation of diabetic cardiomyopathy. Mitochondrial bioenergetic impairment disrupts intracellular calcium handling, causing abnormalities in myocardial contraction and relaxation [44]. Dysfunctional mitochondria undergo mitophagy, a protective autophagic process that clears abnormal mitochondria and reduces myocardial apoptosis. However, excessive mitophagy can exacerbate myocardial damage in diabetic cardiomyopathy [36, 44].
Cardiac autonomic neuropathy involves abnormalities in heart rate control, vascular hemodynamics, and cardiac structure and function. Hyperglycemia triggers oxidative stress and the accumulation of toxic glycosylation products, leading to neuronal dysfunction and death [44].
In murine models of T2DM, increased intracellular resting Ca2+, delayed Ca2+ transitions, reduced sarcoplasmic reticulum Ca2+ pumping, and impaired Ca2+ reuptake result in contractile and relaxation abnormalities [45].
Prolonged hyperglycemia leads to vasculopathy, with a linear relationship between glucose levels and adverse effects. Both microvascular and macrovascular complications are major contributors to morbidity and mortality in diabetic patients. Changes in endothelial and vascular smooth muscle cells play a key role in vasculopathy. Regarding myocardial perfusion, DM induces both macrovascular and microvascular ischemia, contributing to myocardial dysfunction [44].
The presence of DM indicates that patients are at risk for HF and should be considered within the Stage A HF category, as well as at high risk for progression to subsequent stages of HF. At this stage, controlling blood glucose and other risk factors can alter the clinical risk of HF. According to ACC/AHA guidelines, Stage B HF, also referred to as “pre-HF”, is associated with an increased risk of cardiovascular and all-cause mortality, as well as progression to more advanced stages of overt HF. Many individuals with diabetes can be classified as Stage B [46].
Recommended laboratory evaluations for patients with HF include natriuretic peptides, complete blood count, urinalysis, serum electrolytes, blood urea nitrogen, serum creatinine, glucose, fasting lipid profile, liver function tests, and thyroid function tests. Chest X-rays and a 12-lead electrocardiogram are also advised. Imaging studies, such as transthoracic echocardiography, provide valuable information for evaluating patients with suspected or confirmed HF [46].
Additionally, in diabetic patients with suspected CAD, stress testing, myocardial perfusion scintigraphy, CT coronary angiography, and, if necessary, invasive coronary angiography should be performed.
Lifestyle changes for patients with T2DM include regular exercise, a balanced diet, smoking cessation, and minimizing alcohol intake. Epidemiological studies have shown that regular physical activity and a lower BMI are associated with reduced cardiovascular mortality [47, 48]. In a 4-year follow-up study, weight loss combined with appropriate exercise significantly reduced the risk of HF [47]. Reducing central obesity and fat mass index is particularly effective in lowering HF risk [29].
HT is a common and modifiable risk factor in T2DM. A 10 mmHg reduction in systolic blood pressure in the general population decreases HF risk by 28% [49]. HT control offers relatively greater risk reduction in T2DM patients than in non-diabetic individuals [relative risk (RR) 0.84, 95% CI 0.72–0.98 vs. RR 0.75, 95% CI 0.65–0.87]. The American Diabetes Association recommends maintaining blood pressure below 140/90 mmHg, which lowers the 10-year cardiovascular risk to less than 15%. In diabetic patients with albuminuria, angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) are preferred [50]. ACEi and thiazide diuretics have been shown to reduce HF risk more effectively than calcium channel blockers [51].
The treatment of HF in patients with and without diabetes is similar, but the effects of antidiabetic medications on HF vary. Safe therapies that also reduce HF-related events should be prioritized. ACEi and ARBs are recommended, particularly for Stage A or B HF patients with albuminuria and/or CAD. Combination therapy with a thiazide diuretic or ACEi is more effective than calcium channel blockers in preventing progression to symptomatic HF.
For patients with HFrEF and T2DM, guideline-recommended medical therapies [including ARNI, ACEi, ARBs, beta-blockers, mineralocorticoid receptor antagonists (MRAs) and sodium glucose co-transporter-2 (SGLT2) inhibitors] should be considered. ARNI is the first-line treatment and is preferred over ACEi or ARBs.
MRAs are used in both HT and HF. While steroidal MRAs reduce albuminuria, they may cause hyperkalemia, especially when combined with ACEi or ARBs [52]. Nonsteroidal MRAs, such as finerenone, are more potent and cause less hyperkalemia, reducing the risks of HF and kidney disease [38].
Recent large randomized controlled trials have demonstrated that SGLT2 inhibitors (SGLT2is) improve cardiovascular outcomes, including all-cause mortality, independent of diabetes status [53]. These inhibitors significantly reduce major adverse cardiovascular events and HF-related hospitalizations in diabetic patients [54].
SGLT inhibitors exert their antidiabetic effects by inhibiting glucose reabsorption in the proximal convoluted tubules of the kidney. This mechanism leads to glucosuria and, simultaneously, natriuresis. The resulting osmotic diuresis and natriuresis increase fluid excretion, contributing to reductions in blood pressure and body weight. These effects collectively result in positive cardiovascular and renal outcomes. Additionally, improved glycemic control promotes nitric oxide release, reducing oxidative stress. Furthermore, SGLT2is exhibit beneficial effects on atherosclerosis [55].
By reducing sodium reabsorption in the proximal tubule, SGLT2is increase the sodium concentration reaching the macula densa. This activates tubuloglomerular feedback, causing afferent arteriolar vasoconstriction and a subsequent decrease in intraglomerular pressure [56].
Randomized controlled trials, including EMPAREG, CANVAS, and DECLARE-TIMI, have demonstrated that different SGLT2is (empagliflozin in EMPAREG, canagliflozin in CANVAS, and dapagliflozin in DECLARE-TIMI) reduce glomerular hyperfiltration and albuminuria in patients with T2DM [57, 58].
Other studies have shown that while these agents initially cause a transient decline in glomerular filtration rate (GFR), they subsequently promote long-term stabilization and even recovery of GFR values [59]. This process, involving reduced intraglomerular pressure, is independent of blood pressure and plasma glucose levels. It is also associated with a reduction in albuminuria and slower GFR decline [60]. Unlike other antidiabetic agents, SGLT2is reduce hypoxia and oxidative stress in the proximal tubule and renal cortex. Due to these effects, they are referred to as the “beta-blockers of the kidney” [61].
In the DAPA-CKD trial, the dapagliflozin group demonstrated significant reductions in GFR decline, progression to kidney failure, and renal and cardiovascular mortality compared to placebo [62].
The cardioprotective effects of SGLT2is occur through natriuresis and diuresis. These effects lead to a reduction in plasma volume, as well as decreased ventricular preload and afterload. SGLT2is operate through several different mechanisms [63, 64], including:
Reduction in blood pressure.
Improvement in endothelial function.
Decrease in atherosclerosis.
Reduction in interstitial and intravascular volume.
Decrease in intraglomerular pressure.
Suppression of the renin-angiotensin system.
Increased insulin sensitivity in muscles, leading to enhanced glucose uptake.
Inhibition of gluconeogenesis and increased ketogenesis.
Regulation of cardiac energy metabolism.
Inhibition and reduction of myocardial Na+/H+ exchange.
Suppression of inflammation and myocardial oxidative stress, reducing hypertrophy and fibrosis.
Improvement in cardiac remodeling.
In primary prevention studies (EMPAREG OUTCOME, CANVAS, DECLARE TIMI-59), SGLT2is have shown positive results in preventing HF development, despite the ejection fraction (EF) data not being available for the participants [57, 65]. SGLT2is are thought to be effective in preventing both HFrEF and HFpEF.
The DAPA-HF study, which published findings on the effects of these medications in HFrEF patients, showed that SGLT2is reduced the primary endpoint by 26%, which included HF worsening and cardiovascular death. They reduced cardiovascular mortality by 18%, hospitalizations due to HF by 30%, and all-cause mortality by 17%.
As a result of these studies, it is expected that SGLT2is will solidify their role as the fourth line of treatment, following the core three drug classes for HF (ACEi, ARB, angiotensin receptor neprilysin inhibitors, beta-blockers, and MRAs).
DM is an important risk factor for HF. Especially in patients with T2DM, HF is one of the major cardiovascular events. To assess the risk of HF, clinical risk scores, echocardiography, and various biomarkers should be used. In addition to traditional treatments (beta-blockers, ACEi, or ARBs), newly developed drugs used in HF, such as SGLT2is, finerenone, GLP-1 receptor agonists, and ARNIs, should be considered. Moreover, in all patients with HF, regardless of whether they have DM, SGLT2is should be considered due to their clinical and mortality benefits.
ACEi: angiotensin converting enzyme inhibitors
AGEs: advanced glycation end products
ARBs: angiotensin receptor blockers
BMI: body mass index
CAD: coronary artery disease
CKD: chronic kidney disease
DM: diabetes mellitus
EF: ejection fraction
GFR: glomerular filtration rate
HF: heart failure
HFpEF: heart failure with preserved ejection fraction
HFrEF: heart failure with reduced ejection fraction
HT: hypertension
MRAs: mineralocorticoid receptor antagonists
ROS: reactive oxygen species
SGLT2: sodium glucose co-transporter-2
SGLT2is: sodium glucose co-transporter-2 inhibitors
T2DM: type 2 diabetes mellitus
IS: Conceptualization, Investigation, Writing—original draft, Writing—review & editing.
The author declares that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Elif Basaran, Gulali Aktas
Roanne Lecky ... Catriona Kelly
Mehmet Ali Kosekli
Maher Monir Akl, Amr Ahmed
Yutang Wang ... Guang Yang
Ivonne G. Narváez-Ortiz ... Alberto Maceda-Serrano
Osama Mahmoud Mehanna ... Ahmad Shaban Abd El Monsef
Thewodros Leka, Hemda Garelick
Halima Babikir Eltahir ... Abdelrahim Osman Mohamed