79 results in Exploration of Endocrine and Metabolic Diseases
Most Downloaded
Sort by :
- Latest
- Most Viewed
- Most Downloaded
- Most Cited
Open Access
Review
Recent advances in artificial intelligence-assisted endocrinology and diabetes
Ioannis T. Oikonomakos ... Stefan R. Bornstein
Published: April 01, 2024 Explor Endocr Metab Dis. 2024;1:16–26

Open Access
Commentary
Updates from the 2025 American Diabetes Association guidelines on standards of medical care in diabetes
Dipti Tiwari ... Tar Choon Aw
Published: April 15, 2025 Explor Endocr Metab Dis. 2025;2:101428
Open Access
Consensus Statement
Expert Consensus on Type 2 Diabetes Remission
Endocrinology and Metabolism Physician Branch of Chinese Medical Doctor Association
Published: May 20, 2026 Explor Endocr Metab Dis. 2026;3:101473
Open Access
Commentary
The 2024 American Diabetes Association guidelines on Standards of Medical Care in Diabetes: key takeaways for laboratory
Dipti Tiwari, Tar Choon Aw
Published: July 23, 2024 Explor Endocr Metab Dis. 2024;1:158–166

Open Access
Original Article
Comparative pharmacodynamic analysis of resmetirom, semaglutide and obeticholic acid in translational mouse models of MASH
Rufeng Zhang ... Chunli Sun
Published: June 24, 2025 Explor Endocr Metab Dis. 2025;2:101433

Open Access
Review
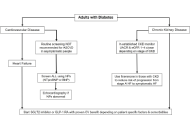
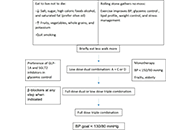
A brief approach to hypertension in type 2 diabetes mellitus
Yilmaz Gunes
Published: February 04, 2025 Explor Endocr Metab Dis. 2025;2:101422
This article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Open Access
Case Report
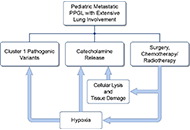
A case series of three patients with extensive lung metastatic pheochromocytoma/paraganglioma: evaluation, treatment challenges, and outcomes
Kailah M. Charles ... Karel Pacak
Published: November 15, 2024 Explor Endocr Metab Dis. 2024;1:218–233
Open Access
Review
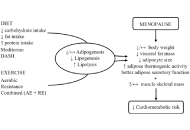
Healthy adipose tissue after menopause: contribution of balanced diet and physical exercise
Bruno Vecchiatto ... Fabiana S. Evangelista
Published: March 13, 2025 Explor Endocr Metab Dis. 2025;2:101424
This article belongs to the special issue Metabolic Syndrome in Menopause
Open Access
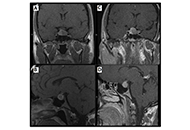
Case Report
Patient diagnosed with acromegaly and pituitary apoplexy after breast carcinoma treatment: challenges in diagnosis and management
Ignacio Jiménez Hernando, Laura González Fernández
Published: November 26, 2024 Explor Endocr Metab Dis. 2024;1:234–243
Open Access
Review
Optimizing hormone replacement therapy for postmenopausal women with type 2 diabetes: a review
Butheinah A. Al-Sharafi, Samih A. Odhaib
Published: April 28, 2025 Explor Endocr Metab Dis. 2025;2:101430
This article belongs to the special issue Metabolic Syndrome in Menopause

Open Access
Review
Hormonal changes during aging and their effects on quality of life
Carter Coggins ... Vikrant Rai
Published: November 10, 2025 Explor Endocr Metab Dis. 2025;2:101447
This article belongs to the special issue The Fountain of Youth: Decoding the Hormonal Regulation of Aging

Open Access
Review
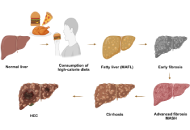
Significance of FXR agonists in MASLD treatment: a deep dive into lipid alteration by analytical techniques
Pirangi Srikanth ... Sukhendu Nandi
Published: March 25, 2025 Explor Endocr Metab Dis. 2025;2:101425
This article belongs to the special issue Regulators of Glucose Homeostasis, Lipid Metabolism and Energy Balance
Open Access
Review
Glucocorticoid receptor alpha: origins and functions of the master regulator of homeostatic corrections in health and critical illness
Gianfranco Umberto Meduri
Published: March 28, 2025 Explor Endocr Metab Dis. 2025;2:101426

Open Access
Review
Synergistic glucocorticoids, vitamins, and microbiome strategies for gut protection in critical illness
Gianfranco Umberto Meduri
Published: May 14, 2025 Explor Endocr Metab Dis. 2025;2:101432

Open Access
Review
Glucocorticoid signalling coordinating circadian rhythms between the glymphatic system and sleep contributes to brain health
Laura C. A. van der Zwet ... Tom Deboer
Published: July 15, 2025 Explor Endocr Metab Dis. 2025;2:101437
This article belongs to the special issue The HPA Axis in Health and Disease

Open Access
Review
Endogenous glucocorticoids during skeletal ageing
Eugenie Macfarlane ... Markus Joachim Seibel
Published: August 16, 2024 Explor Endocr Metab Dis. 2024;1:191–212
This article belongs to the special issue The Fountain of Youth: Decoding the Hormonal Regulation of Aging

Open Access
Review
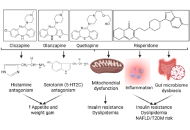
Psychotropic medications and metabolic side effects
Michael Natalizio ... Vikrant Rai
Published: November 24, 2025 Explor Endocr Metab Dis. 2025;2:101450
This article belongs to the special issue Regulators of Glucose Homeostasis, Lipid Metabolism and Energy Balance
Open Access
Review
Circulating endocannabinoids and brain anatomy: unraveling the weight loss connection through lifestyle and surgery approaches
Gabrielle St-Arnaud ... Vincenzo Di Marzo
Published: April 07, 2025 Explor Endocr Metab Dis. 2025;2:101427
This article belongs to the special issue Regulators of Glucose Homeostasis, Lipid Metabolism and Energy Balance

Open Access
Original Article
Hormone oscillations in the HPA axis: dynamical diseases and beyond
John Milton, Alexander Churilov
Published: June 24, 2025 Explor Endocr Metab Dis. 2025;2:101434
This article belongs to the special issue The HPA Axis in Health and Disease
Open Access
Case Report
Intravenous calcitriol: a critical intervention for severe postoperative hypoparathyroidism when oral administration is not feasible
Ignacio Jiménez Hernando ... Marta Pérez Noguero
Published: May 08, 2025 Explor Endocr Metab Dis. 2025;2:101431

Journal Information