Review
Review

Affiliation:
1Department of Radiology, University of Florida, Gainesville, FL 32608, USA
Email: kpierre150@gmail.com
ORCID: https://orcid.org/0000-0002-0083-9602
Affiliation:
2Department of Neurosurgery, Mayo Clinic, Jacksonville, FL 32224, USA
ORCID: https://orcid.org/0000-0003-4241-7368
Affiliation:
3College of Medicine, University of Florida, Gainesville, FL 32610, USA
ORCID: https://orcid.org/0000-0003-4245-8290
Affiliation:
3College of Medicine, University of Florida, Gainesville, FL 32610, USA
Affiliation:
3College of Medicine, University of Florida, Gainesville, FL 32610, USA
Affiliation:
4Department of Neurosurgery, University of Florida, Gainesville, FL 32608, USA
Affiliation:
5Biomolecular Sciences Graduate Program, Boise State University, Boise, ID 83725, USA
Affiliation:
4Department of Neurosurgery, University of Florida, Gainesville, FL 32608, USA
ORCID: https://orcid.org/0000-0001-6577-4080
Explor Neurosci. 2022;1:83–99 DOI: https://doi.org/10.37349/en.2022.00007
Received: August 29, 2022 Accepted: September 26, 2022 Published: December 30, 2022
Academic Editor: Dirk M. Hermann, University of Duisburg-Essen, Germany
Stroke is a leading cause of morbidity and mortality. The advent of mechanical thrombectomy has largely improved patient outcomes. This article reviews the features and outcomes associated with aspiration, stent retrievers, and combination catheters used in current practice. There is also a discussion on clinical considerations based on anatomical features and clot composition. The reperfusion grading scale and outcome metrics commonly used following thrombectomy when a patient is still in the hospital are reviewed. Lastly, there are proposed discharge and outpatient follow-up goals in caring for patients hospitalized for a stroke.
Strokes are the 5th leading cause of death in the United States, accounting for over 160,000 deaths in the nearly 800,000 annually affected individuals and resulting in significant long-term disability in many survivors [1, 2]. Though the incidence of stroke has decreased, increased longevity has resulted in elevated lifetime risk (24.9% in 2016 vs. 22.8% in 1990) [3]. As 87% of strokes are ischemic, intravenous (IV) thrombolysis using tissue plasminogen activator (tPA) can be used for patients presenting with stroke within 4.5 h [1]. However, mechanical thrombectomy (MT) is now the new standard of care in ischemic stroke in appropriate candidates [1, 4–7]. It has been proven more effective than thrombolysis alone in several randomized control trials [8, 9].
MT is used for stroke caused by large anterior circulation artery occlusions. Patients may be treated within 24 h of symptom onset regardless of prior tPA administration [10]. With modern techniques and technology, there is often recanalization of over 80% of the lumen diameter [11]. While MT may be used to treat patients with posterior circulation (PC) strokes, the benefits are not as well-established [10].
In MT, obstructed arteries are accessed via microcatheters, through which a thrombectomy device is passed [12]. Categories of MT devices include coil retrievers, stentrievers, aspiration catheters, and mechanical clot disruption apparatuses [12]. Coil retrievers are delivered to the clot via a microcatheter and deployed at a destination across the clot. Once the coil engages the clot, revascularization is achieved by pulling the coil-clot complex back into the catheter [13]. Like the coil retriever, the stentriever is delivered via a microcatheter. The self-expanding stent is positioned inside the thrombus, allowing its appendages to intertwine with the thrombus, and is subsequently drawn back into the catheter used for delivery [13]. Aspiration devices use vacuum suction to remove clots from occluded arteries [12, 13]. The addition of a separator wire with a bulbous tip that can be pushed and pulled to detach a clot from the lumen addresses aspiration device tip clogging or congestion [12]. There has also been an increasing use of combination catheters that employ the use of aspiration catheters with coil retrievers and stentrievers.
The type of MT device used to treat a patient with stroke is determined by the clinical scenario and judgment of the operating neuro-interventionalist.
Complications, such as hemorrhage and successive embolization by thrombus fragmentation, may be seen in MT with all devices. Complications appear to be more frequent with the use of coil retrieval and aspiration (10%) when compared to stentriever (2–4%) [13].
Patient factors also influence response to MT therapy. Area of ischemia may influence patient recovery following stroke as treatment of white matter infarcts shows better recovery than that of gray matter infarcts [14]. Good collateral circulation has also been associated with improved outcomes and decreased rates of complication following stroke [15]. In addition, hyperglycemia and the amount of time between the onset of symptoms and achievement of reperfusion have been shown to have a significant impact of patient outcome [16, 17].
Detachable stents are widely used to assist the revascularization of vascular stenosis or to support the coiling of intracranial aneurysms. Non-detachable stents showed promising in vitro and in vivo outcomes for clot and foreign body removal and introduced a second generation of clot retrievers for patients with acute ischemic stroke [18, 19]. Non-detachable stents (stent retrievers) are temporarily placed in the cerebral vasculature and restore blood flow by the expansion of the stent within the occluded vessel. The stent retriever mesh then embeds into the clot and allows for clot retrieval when removing the stent [20]. This type of device improved previous MT techniques by providing immediate blood flow restoration and more effective target thrombus retrieval. Stent retrievers are often combined with a balloon guide catheter (BGC) that may be inflated to arrest anterograde flow and allow aspiration [21]. Based on the SWIFT randomized trial, the first stent retriever approved by the Food and Drug Administration (FDA) in 2012 was the Solitaire FR [22]. A number of different devices have also surfaced in the last few years including Trevo XP, Merci, EmboTrap, Versi, Embolus Retriever with Interlinked Cages (ERIC), Tigertriever, among others. An overview of the different stent retrievers currently available in the market can be found in Table 1.
Stent retrievers
| Stent retriever | Company | FDA approval | Design/Shape | Study | Outcomes |
|---|---|---|---|---|---|
| Solitaire FR | Medtronic | 2012 | Self-expanding stent cut into a nitinol plate with a honeycomb pattern | SWIFT-PRIME [19]SWIFT-DIRECT [23]REVASCAT [24]EXTEND-IA [25]ESCAPE [26] | Successful revascularization achieved in 91% (thrombectomy alone; up to 96% with alteplase) |
| Trevo XP | Stryker | 2012 | Self-expanding stent with a unique distal shaped section for clot retrieval; its platinum marker allows fluoroscopic control of the distal portion | DAWN [27]TREVO 2 [28] | Successful revascularization achieved in 86% |
| Merci | UCLA Health | 2004 | Stent formed of nitinol with a characteristic helical shape that traps the clot once deployed. Often combined with BGC to prevent anterograde flow | MERCI [29]SWIFT [22]TREVO 2 [28] | Successful revascularization achieved in 60%; 19% device-related subarachnoid hemorrhage |
| EmboTrap | Johnson and Johnson | 2018 | Dual-layer construct to improve clot engagement and distal mesh to reduce emboli | ARISE [30] | Successful revascularization achieved in 80.2%; 67% with functional independence at 90 days |
| Versi | NeuroVasc | Stent formed with nitinol that has three articulated stent segments that facilitate opening during retrieval | Sakai et al. [31] | Successful revascularization achieved in 100% (11 patients); 72.7% favorable functional outcomes (mRS 0–2) at 90 days | |
| ERIC | MicroVention Terumo | Three to five interlinked cages preventing the clot from shearing off during retraction | ETIS [32] | Successful revascularization achieved in 82%; 40% favorable outcome (mRS ≤ 2) | |
| Tigertriever | Rapid Medical | Device with handle that allows physician to expand or contract the mesh | Kara et al. [33] | Successful revascularization achieved in 75.4%; 27.9% with favorable clinical outcomes |
mRS: modified Rankin scale; UCLA: University of California, Los Angeles
Although these stent retrievers operate by the same principle of retrieving a clot and restoring blood flow, differences in design and shape have resulted in variable revascularization rates. The Solitaire FR stent retriever is the most widely studied device with multiple clinical trials already completed; it is a self-expanding stent cut into a nitinol plate with a honeycomb pattern, showing a 91% reperfusion rate in the recent SWIFT-DIRECT study [23], supporting the use of alteplase before thrombectomy in eligible patients (96% reperfusion). Trevo XP is another widely used self-expanding stent retriever with a unique distal shaped section for clot retrieval; its platinum marker allows fluoroscopic control of the distal portion. In the TREVO 2 trial, this stent retriever showed 86% successful revascularization, which was significantly higher when compared to the Merci stent retriever (60%) [28]; the latter is also formed of nitinol but has a characteristic helical shape that traps the clot once deployed [34]. Other stent retrievers including EmboTrap (dual-layer construct to improve clot engagement and distal mesh to reduce emboli) [35], Versi (three articulated stent segments that facilitate opening during retrieval) [31], ERIC (three to five interlinked cages preventing the clot from shearing off during retraction) [36], and Tigertriever (a device with handle that allows physician to expand or contract the mesh) [33] have been studied less extensively. The SWIFT-DIRECT study demonstrated increased revascularization in patients administered IV thrombolytics prior to MT using the Solitaire FR stent retriever [23], while stent retrievers other than Solitaire FR are often combined with thrombolytic therapy or administered following unsuccessful thrombolysis with tPA, the literature is relatively limited, suggesting the need for further research in this area.
Multiple studies have analyzed and compared stent retrievers for revascularization rate differences and potential complications. Solitaire FR is often analyzed against Trevo XP. Though many studies report non-significant differences in revascularization and complication rates [37, 38], Trevo XP usually has shorter procedural time, decreased number of stent passages, and higher successful recanalization than Solitaire FR in studies showing statistically significant differences [39, 40].
Intermediate or distal access catheters are used for direct contact aspiration using negative pressure with an aspiration pump or syringe to dislodge the clot [41]. In addition to aspiration ability, the performance of these catheters is often judged by the ease of navigation, a feature of malleability depending on the catheter components. The device liner is made from a malleable substance such as polytetrafluoroethylene that ensures proper advancement through tortuous vasculature [42]. The aspiration capacity of the catheter is directly proportional to the inner diameter and the negative pressure magnitude [43]. It is proposed that higher catheter to vessel diameters achieve better perfusion because of increased force acting on the clot [44].
The Penumbra aspiration device was FDA-approved in 2008 [29]. This device allows the operator to perform clot fragmentation and aspiration by moving the catheter in and out [45]. The penumbra pivotal stroke trial demonstrated safe use up to 8 h from stroke onset and an 82% recanalization rate in 125 patients [45]. This aspiration device shows similar clinical outcomes to the Solitaire FR stent retriever in a retrospective review of 76 patients [46]. However, it demonstrated higher rates of complete recanalization with lower device passage count, shorter procedure times, and shorter recanalization times [46–50].
Other catheters are less well-studied. Those that are studied generally prove to be safe and effective [43, 51–54]. For example, REACT catheters achieved recanalization in 89–96% of cases and resulted in a rate of 24–36% of functional independence in 299 patients across three studies [43, 51, 55, 56]. Selected catheters currently available on the market are listed (Table 2) [53, 57–61].
It is important to note that various combined techniques with stent retrievers, distal aspiration catheters, and BGCs are used in many centers with good outcomes [62]. A recent meta-analysis demonstrated that the combined use of the aspiration catheter and stent retriever result in a superior first pass effect (40.8%) compared to stent retrievers alone (32.6%; P < 0.0001). However, they did not result in statistically significant improvements in functional independence and reperfusion [63]. Examples of combination techniques include the BAlloon guide with large bore Distal access catheter with Dual Aspiration with Stent retriever as Standard approach (BADDASS) technique [64], the REACT catheter combined with a stent retriever [56], aspiration-retriever technique for stroke (ARTS) [65], a stent retrieving into an aspiration catheter with proximal balloon (ASAP) technique [66], the stent retriever-assisted vacuum-locked extraction (SAVE) approach [67], and PRoximal balloon Occlusion TogEther with direCt Thrombus aspiration during stent retriever thrombectomy (PROTECTPLUS) [68]. Clinical experience with these techniques suggests they are safe and effective [64, 65, 67–69].
PC strokes are ischemic infarcts occurring in the vertebrobasilar arterial system [70]. They constitute approximately one-fifth of ischemic strokes and are managed differently from anterior circulation strokes [71].
Anatomical PC variants are relatively common in the PC and must be taken into account by the treating physician [70]. Roughly half the population has an incomplete circle of Willis. Another variation is the fetal posterior cerebral artery (FPCA), representing a posterior cerebral artery (PCA) arising from the internal carotid artery (ICA). Most are unilateral. When bilateral, they are often associated with a small caliber basilar artery. It is important to note that these FPCAs do not carry increased stroke risk [72, 73]. However, patients with hypoplastic vertebral arteries have increased PC stroke risk [74].
Thrombi at the terminal ICA, middle cerebral artery bifurcation, or trifurcations often prove difficult in attempting recanalization. In such cases, contact aspiration is often beneficial when recanalization with stent retrievers proves unsuccessful [75, 76]. Combination aspiration and stent retriever methods may also be beneficial in such situations [65, 77].
Like tPA administration, MT shows better outcomes when done in the first 3 h to 4.5 h following the initial stroke [78]. It is considered safe to recanalize PC 24 h prior to the ischemic event [76, 79, 80].
The histopathological clot composition determines recanalization difficulty. Clots are generally either rich in red blood cells (RBCs) or fibrin [81]. RBC-rich thrombi are generally more malleable and therefore more engageable. However, fibrin-rich thrombi are stiffer and therefore are less likely to fragment and theoretically should have lower embolization rates [82, 83]. Fibrin-rich thrombi generally require more recanalization attempts compared to thrombi rich with RBCs [83].
Studies suggest that computed tomography angiography (CTA) and magnetic resonance imaging (MRI) can determine clot composition. For example, clots with the hyperdense middle cerebral artery sign (HMCAS) and blooming artifact (BA) are more likely to be RBC-rich. Conversely, the absence of the HMCAS and BA likely indicated thrombi predominant in fibrin [84, 85]. An early study by Liebeskind et al. [84] demonstrated that HMCAS was seen in 100% of patients with RBC-dominant clot with a significant correlation between the degree of RBC composition and the presence of HMCAS. Similarly, BA was present in all patients with RBC-dominant clots [84]. A later systematic review reinforced these associations [86]. Therefore, it is important to consider the use of proximal balloon catheters in clots with HMCAS and BA to minimize embolization risk considering the clot is likely to be RBC-dominant [87, 88]. Furthermore, newer ex vivo studies are promising. Diffuse reflectance spectroscopy (DRS) detects RBC-rich clots with sensitivity and specificity of 0.722 and 0.846, respectively. DRS also discriminated between RBC- and fibrin-rich clots [89]. Another study showed that fibrin-rich have high penetrating homogeneous signals and RBC-rich clots have superficial low penetrating signals on optical coherence tomography (OCT) [90]. Lastly, an in vitro study revealed that Mono +50 keV dual energy computed tomography (CT) can successfully differentiate clot composition in an ex vivo model [91]. Recent in vivo studies incorporating machine learning in differentiating thrombus composition are also promising [92, 93].
Several clinical outcome metrics are commonly used post thrombectomy during hospitalization. Important metrics include reperfusion success, the mRS, the National Institutes of Health Stroke Scale (NIHSS), and the occurrence of symptomatic intracerebral hemorrhage (sICH) [94–97]. Patients who achieve successful reperfusion post thrombectomy experience better clinical outcomes than those who are unsuccessfully reperfused [98, 99]. The mRS is a valid and reliable clinician-reported measure of global disability in patients who have suffered a stroke [94]. It can be measured over time (at discharge, at 30 days, and at 90 days) to assess health outcomes. The mRS ranges from 0 (no disability) to 6 (death). A score of 0–3 at hospital discharge is an early favorable outcome for independent ambulation [100]. Additionally, providers widely use the NIHSS as an indicator for functional outcomes and early mortality. It is a 15-item neurological examination scale investigating the impact of cerebral infarction on the level of consciousness, visual fields, neglect, extraocular movements, strength, ataxia, sensation, and dysarthria. Patients with lower NIHSS had much better survival rates than those with significantly higher scores [101, 102]. sICH potentially increases the risk of functional dependence and was found to increase their ninety-day mortality [96, 97].
Reperfusion success following MT has been measured and categorized into five different grades by the thrombolysis in cerebral infarction (TICI) scale, yet there is variability in definitions [98]. Reperfusion is graded by visually examining the extent of tissue reperfusion as depicted by the capillary blush on a digital subtraction angiography [103, 104]. The TICI scale spans from no perfusion (grade 0) to complete reperfusion (grade 3), with grade two subdivided into groups 2a and 2b (Table 3).
TICI scale [104]
| Category | Description |
|---|---|
| Grade 0 | No perfusion |
| Grade 1 | Minimal flow past the occlusion but no perfusion |
| Grade 2a | Minor partial reperfusion (< 50%) |
| Grade 2b | Major partial reperfusion (> 50%) |
| Grade 3 | Complete reperfusion with no flow defects |
Patients who undergo mechanical thrombectomies are closely monitored postoperatively in the neuro-intensive care unit (ICU). The first 24 h following intervention are the most crucial and require heightened awareness of complications. Potential complications include, but are not limited to, access site complications, vasospasms, iatrogenic arterial dissections, hemorrhagic complications, and embolic and ischemic events [105]. Thus, inpatient care includes continuous monitoring of vital signs and serial assessment of neurological and neurovascular status [106]. Suspected changes in the patient’s neurological assessment should be immediately reported to the team. Airway and oxygenation should be strictly monitored. Recommendations exist to maintain oxygen saturation above 94% in patients who have suffered from acute ischemic strokes [107]. Additionally, strict control of blood pressure management tends to lead to better outcomes; guidelines recommend always maintaining a systolic blood pressure of 140–180 mmHg with mean arterial pressure (MAP) greater than or equal to 70 mmHg [108]. Post-operative care also includes assessment of the groin site and distal extremities for infection, hematoma, or femoral nerve injuries.
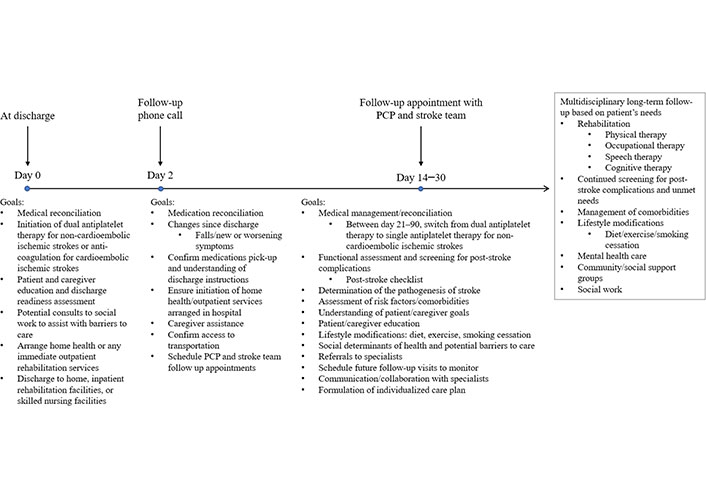
Research evaluating post-discharge care after stroke treated with MT is lacking. It is not yet known whether follow-up for MT should differ from more traditional treatment options. The optimal strategy for post-discharge care for stroke patients in general is still being elucidated as researchers and clinicians work to determine the most beneficial and feasible way to help patients transition from the hospital to long-term follow-up. Depending on their functional status and individual needs, after acute care in the hospital, patients can be discharged home with outpatient follow-up or home health care, to a skilled nursing facility, to a long-term acute care hospital, or to inpatient rehabilitation [109–111]. The transition from the hospital to home can be especially difficult and patients and their caregivers often feel overwhelmed and unprepared as transitional care remains fragmented between providers and varied between hospitals [112–117]. Current American Stroke Association/American Heart Association guidelines emphasize a structured, individualized, and interdisciplinary approach to post-acute care. Follow-up should be focused on patient and caregiver education and support, screening for post-stroke complications, management of comorbidities and modifiable risk factors, and referral to community support and local outpatient resources [109, 118–120]. A current model for transitional care between discharge and long-term follow-up integrating current guidelines and evidence-based approaches is proposed (Figure 1) [109, 110, 117, 119–135]. This model includes a follow-up telephone call two days post-discharge and early follow-up with both a primary care physician and the stroke team. Based on the patient’s individual deficits and needs, an individualized care plan should be designed, referrals should be sent to rehabilitation specialists, and long-term follow-up care should be initiated.
Long-term follow-up focuses on continued rehabilitation, screening and treatment of post-stroke complications, and secondary prevention of stroke [109, 120, 127, 131]. Continued long-term follow-up visits and tools such as the post-stroke checklist can be used to routinely screen patients for post-stroke sequelae such as inability to perform activities of daily living, immobility, falls, swallowing dysfunction, spasticity, pain, incontinence, communication deficits, cognitive impairments, depression or anxiety, and social isolation [117]. Physical, speech, occupational, and cognitive therapy can help provide functional recovery and help patients adapt to continued deficits following a stroke [120, 131, 136]. Earlier rehabilitation is strongly associated with greater functional recovery [137–142]. Secondary prevention of stroke is accomplished through medications, management of comorbidities, and lifestyle changes. Patients with a non-cardioembolic ischemic stroke are prescribed dual antiplatelet therapy in the hospital which should be continued for 21–90 days [126, 143]. After 90 days, patients should be switched to single antiplatelet therapy such as low dose aspirin to prevent the recurrence of stroke [127]. Patients with a cardioembolic ischemic stroke should be started directly on anticoagulation such as warfarin, factor Xa inhibitors, and thrombin inhibitors [126, 127, 143]. Comorbidities such as hypertension, hyperlipidemia, and diabetes should be managed medically and through lifestyle modifications to prevent subsequent strokes [119, 126, 127, 143–149]. Smoking is a strong independent risk factor for stroke so patients should be counseled on smoking cessation and provided with appropriate resources [119, 127, 131].
Although there have been recent advances towards creating an organized, cohesive, and multidisciplinary plan of care for patients after discharge from the hospital, further work should be done to determine the barriers to incorporating these recommendations and guidelines into widespread clinical use. Additionally, research should be done to determine how post-stroke follow-up should be modified for patients receiving innovative treatments such as MT.
In conclusion, there have been significant advances and achievements in treating stroke using MT. We look forward to further research investigating the use of stent retriever, aspiration, and occlusive balloon devices alone and in combination in different clinical scenarios. We make recommendations for post-thrombectomy discharge care and also look forward to further research in this area. Particularly, systematic reviews and meta-analyses examining the efficacy of available devices will be beneficial. Further research examining the detection of thrombus composition using non-invasive imaging, evaluation of the impact of structured post-stroke objectives on outcomes, optimization of patient transfer networks, development of new MT devices, and use of neuroprotective drugs may help improve outcomes for patients with ischemic stroke.
BA: blooming artifact
BGC: balloon guide catheter
ERIC: Embolus Retriever with Interlinked Cages
FDA: Food and Drug Administration
HMCAS: hyperdense middle cerebral artery sign
mRS: modified Rankin scale
MT: mechanical thrombectomy
NIHSS: National Institutes of Health Stroke Scale
PC: posterior circulation
RBCs: red blood cells
TICI: thrombolysis in cerebral infarction
tPA: tissue plasminogen activator
BO wrote the original draft of the introduction. CPV wrote the original draft of the section on stent retrievers. ME wrote the original draft of the section on aspiration devices. ME wrote the original draft of the clinical considerations section. RH wrote the original draft of the section on short-term outcomes. AF wrote the original first draft of the section on long-term outcomes. As such, these individuals were responsible for data curation. KP and BLW contributed to the conceptualization and design of the study, provided guided supervision, and reviewed and edited the manuscript. All authors approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2022.
Copyright: © The Author(s) 2022. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.