 Systematic Review
Systematic Review

Affiliation:
1Chelsea and Westminster NHS Foundation Trust, West Middlesex University Hospital, TW7 6AF London, UK
Email: t.leka@nhs.net
ORCID: https://orcid.org/0009-0009-9237-8476
Affiliation:
2Faculty of Science and Technology, Middlesex University, NW4 4BT, London, UK
ORCID: https://orcid.org/0000-0003-4568-2300
Explor Endocr Metab Dis. 2026;3:101477 DOI: https://doi.org/10.37349/eemd.2026.101477
Received: April 14, 2026 Accepted: June 15, 2026 Published: July 16, 2026
Academic Editor: Gulali Aktas, Abant Izzet Baysal University Hospital, Turkey
The article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Background: Type 2 diabetes (T2D) is a chronic metabolic condition requiring sustained pharmacological and behavioural management. Suboptimal medication adherence remains a major barrier to achieving adequate glycaemic control and is associated with increased morbidity, mortality, and healthcare costs. Patient-centred care (PCC) has been widely recommended as an approach to enhance patient engagement, adherence, and clinical outcomes; however, evidence regarding its effectiveness remains inconsistent. This systematic review aimed to synthesise evidence from primary studies evaluating PCC interventions on medication adherence, glycaemic control, and psychosocial outcomes in adults with T2D.
Methods: This review followed PRISMA 2020 guidelines and was prospectively registered in PROSPERO (CRD420251115067). A comprehensive search of MEDLINE, Embase, EMCare, CINAHL, PsycINFO, and the Cochrane Library was conducted for studies published between 2005 and 2025. Eligible studies included primary research evaluating PCC interventions in adults with T2D and reporting adherence or clinical outcomes. Data were synthesised narratively due to heterogeneity, and vote counting based on direction of effect was applied. Risk of bias was assessed using RoB 2.0, ROBINS-I, and CASP tools, and overall certainty of evidence was evaluated using the GRADE framework.
Results: Eighteen studies were included, comprising seven randomised controlled trials, eight observational studies, and three qualitative studies. PCC interventions consistently improved medication adherence and psychosocial outcomes, including patient empowerment and engagement. In contrast, effects on glycaemic control were variable, with four studies reporting improvement, seven showing no effect, and three demonstrating mixed findings. Overall, the evidence suggests a predominantly positive but inconsistent effect on HbA1c.
Discussion: PCC interventions appear effective in improving behavioural and psychosocial outcomes but demonstrate inconsistent impact on glycaemic control. These findings suggest that PCC should be considered a supportive strategy to enhance engagement and adherence rather than a standalone intervention for improved clinical outcomes. Further research is required to identify optimal intervention components that can improve clinical outcomes.
Type 2 diabetes (T2D) is a chronic metabolic disorder affecting millions of individuals worldwide and requiring sustained pharmacological and behavioural management. Effective diabetes management requires healthcare providers to implement patient-centred strategies that explicitly account for ethnic diversity, enabling the delivery of culturally tailored self-management support that optimises engagement and clinical outcomes. Suboptimal medication adherence remains a significant barrier to achieving adequate glycaemic control and is associated with increased morbidity, mortality, and healthcare costs [1, 2].
Patient-centred care (PCC) has been increasingly advocated by leading organisations, including the American Diabetes Association (ADA), the European Association for the Study of Diabetes (EASD), and the National Institute for Health and Care Excellence (NICE), as an approach to improving patient engagement and adherence. This model emphasises shared decision-making, the establishment of individualised treatment goals, and alignment of care with patients’ preferences, needs, and values [3–5]. Despite the growing emphasis on PCC, evidence regarding its effectiveness in improving medication adherence and clinical outcomes in T2D remains inconsistent. Reported effects vary across intervention types, populations, and study designs, and these inconsistencies have not yet been comprehensively synthesised using structured methodological approaches. Therefore, the objective of this systematic review is to synthesise evidence from primary studies evaluating PCC interventions on medication adherence and clinical outcomes, including glycated haemoglobin (HbA1c), in adults with T2D, while critically assessing heterogeneity and the strength of the available evidence.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251115067) prior to data extraction to ensure methodological transparency and adherence to international reporting standards.
A comprehensive literature search was conducted across six electronic databases, namely MEDLINE, Embase, EMCare, CINAHL, PsycINFO, and the Cochrane Library. The search included studies published between January 2005 and December 2025. Both controlled vocabulary terms and free-text keywords related to PCC, T2D, and medication adherence were used in combination with Boolean operators (AND/OR). The detailed MEDLINE search strategy is presented in Tables 1 and 2. Additionally, the reference lists of relevant systematic reviews and eligible primary studies were manually screened to identify further relevant articles.
Partial sample search strategy used in MEDLINE search history.
| # | Database | Search term | Results |
|---|---|---|---|
| 1 | MEDLINE | exp “PATIENT-CENTERED CARE”/ | 18,424 |
| 2 | MEDLINE | (“patient centred” OR “patient centered” OR “patient orientated”).ti,ab | 18,728 |
| 3 | MEDLINE | (“person centred” OR “person centered”).ti,ab | 4,271 |
| 4 | MEDLINE | (“patient focused care” OR “shared decision making” OR “patient preference*”).ti,ab | 14,097 |
| 5 | MEDLINE | (“person focused care” OR “personalised approach” OR “personalized approach” OR “personalised care” OR “personalized care” OR “individualised care” OR “individualized care”).ti,ab | 3,526 |
| 6 | MEDLINE | (patient* ADJ2 preference*).ti,ab | 15,075 |
| 7 | MEDLINE | (patient* ADJ2 preference*).ti,ab | 15,075 |
| 8 | MEDLINE | (patient* ADJ2 choice*).ti,ab | 14,978 |
| 9 | MEDLINE | exp “PATIENT PREFERENCE”/ | 7,344 |
| 10 | MEDLINE | (“shared decision making”).ti,ab | 6,448 |
| 11 | MEDLINE | exp “DECISION MAKING”/ | 189,995 |
| 12 | MEDLINE | (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 8 OR 9 OR 10 OR 11) | 256,941 |
| 13 | MEDLINE | exp “DIABETES MELLITUS, TYPE 2”/ | 124,030 |
| 41 | MEDLINE | (28 AND 40) | 9 |
| 42 | MEDLINE | 41 [Languages English] | 8 |
Sample search strategy used in Cochrane Library search history.
| ID | Database | Search terms |
|---|---|---|
| #1 | Cochrane Library | MeSH descriptor: [Patient-Centered Care] explode all trees |
| #2 | Cochrane Library | “patient centred” OR “patient centered” OR “patient orientated” OR “person centered” OR “person centred” OR “patient focused care” OR “shared decision making” OR “personalised approach” OR “personalized approach” OR “personalised care” OR “personalized care” OR “individualised care” OR “individualized care” |
| #3 | Cochrane Library | patient near/2 preference* |
| #4 | Cochrane Library | MeSH descriptor: [Patient Preference] explode all trees |
| #5 | Cochrane Library | patient near/2 choice* |
| #6 | Cochrane Library | “shared decision making” |
| #7 | Cochrane Library | MeSH descriptor: [Decision Making] explode all trees |
Studies were considered eligible for inclusion if they were primary research studies, including randomised controlled trials, quasi-experimental studies, or observational studies, published in English between 2005 and 2025. Eligible studies included adult populations aged 18 years or older diagnosed with T2D and evaluated interventions explicitly incorporating PCC principles. Furthermore, studies were required to report outcomes related to medication adherence and/or clinical outcomes. Studies were excluded if they were systematic reviews, meta-analyses, clinical guidelines, editorials, commentaries, or expert opinions, or if they lacked primary data. Studies that did not explicitly evaluate PCC as a core component of the intervention or analytical framework were also excluded. In addition, studies were excluded if medication adherence outcomes were unclear or not reported, or if the publication lacked original data, such as conference abstracts. Research primarily focusing on mental health populations was excluded to maintain clinical specificity, as such studies often involve distinct determinants of adherence and intervention frameworks that differ from those used in general T2D management. This review therefore focuses exclusively on primary evidence to avoid duplication and inflation of effect estimates.
The database search yielded a total of 68,564 records. After screening, 131 articles were assessed at full-text level. Following the application of eligibility criteria, 113 studies were excluded, primarily due to inclusion of non-primary evidence, absence of PCC interventions, or failure to report adherence or relevant clinical outcomes. Ultimately, 18 studies were included in the final synthesis, consisting of 7 randomised controlled or interventional studies, 8 observational studies, and 3 qualitative studies. The study selection process is illustrated in Figure 1.
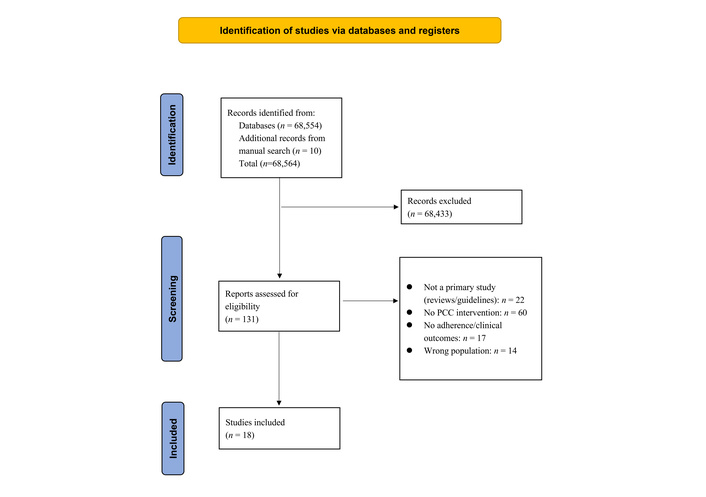
PRISMA 2020 flowchart for systematic reviews. PCC: patient-centred care. Adapted from [27]. © Author(s) 2021. Distributed under a Creative Commons Attribution (CC BY 4.0) license.
Data were extracted using a standardised data extraction form, including information on study design, population characteristics, intervention details, PCC components, measures of medication adherence, and reported clinical and psychosocial outcomes (Table S1). The included studies were subsequently categorised according to study design into randomised controlled or interventional studies, observational studies, and qualitative or mixed-methods studies.
Given the heterogeneity in study designs, interventions, and outcome measures, quantitative meta-analysis was not considered appropriate. A structured narrative synthesis was therefore undertaken, supplemented by vote counting based on the direction of effect [6].
Three primary outcome domains were assessed: glycaemic control, measured by HbA1c; medication adherence; and psychosocial outcomes, including patient empowerment, satisfaction, and engagement. Study results were categorised based on direction of effect as demonstrating improvement, no effect, or mixed or inconclusive findings.
Quality appraisal was conducted using validated, design-specific tools. Randomised controlled trials were assessed using the Cochrane Risk of Bias (RoB 2.0) tool, while non-randomised and observational studies were evaluated using the ROBINS-I tool. Qualitative studies were appraised using the Critical Appraisal Skills Programme (CASP) checklists. Each study was independently assessed by two reviewers [7–9].
The overall certainty of evidence for each outcome was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework [10]. This assessment considered risk of bias, inconsistency, indirectness, imprecision, and potential publication bias. Evidence was categorised as high, moderate, low, or very low certainty. High-certainty evidence was generally derived from well-conducted randomised controlled trials with adequate sample sizes and clearly defined outcomes. Moderate-certainty evidence reflected studies with minor methodological limitations, whereas low and very low certainty ratings were primarily associated with methodological weaknesses, including small sample sizes, inadequate reporting, lack of randomisation, or high risk of bias. Quality assessment informed the interpretation of findings but did not involve quantitative scoring or weighting due to the heterogeneity of study designs and methodologies.
Microsoft Copilot was used to assist with language editing of the manuscript. All content was reviewed and verified by the authors.
The final sample comprised 18 studies, including seven randomised controlled trials, eight observational studies, and three qualitative investigations, as depicted in the PRISMA 2020 flow diagram for systematic reviews. The interventions evaluated across these studies encompassed shared decision-making models, patient empowerment strategies, pharmacist-led medication management, and culturally tailored programmes. Outcomes assessed were multidimensional, incorporating clinical indicators such as HbA1c, behavioural measures including medication adherence, and psychosocial outcomes such as patient engagement and satisfaction. Notably, substantial heterogeneity was observed across the included studies with respect to intervention design, duration, and outcome measurement approaches, limiting direct comparability between findings.
The randomised controlled trials were generally assessed as having low to moderate risk of bias, with limitations primarily related to blinding procedures and incomplete reporting. Observational studies demonstrated moderate to serious risk of bias, largely due to confounding factors and reliance on self-reported adherence measures. The qualitative studies were considered methodologically robust; however, their findings were limited in generalisability. Table 3 presents a structured summary of the risk of bias assessment conducted using RoB 2.0 for randomised trials, ROBINS-I for observational studies, and CASP for qualitative research. Overall, the evidence base was characterised by predominantly low-to-moderate risk among randomised trials, moderate-to-serious risk among observational studies, and strong methodological quality but limited external validity among qualitative studies.
Risk of bias assessment of included studies.
| Study | Study design | Tool used | Key bias domains | Overall risk |
|---|---|---|---|---|
| Adisa and Fakeye (2014) [15] | Observational (cross-sectional) | ROBINS-I | Self-reported adherence; selection bias; confounding | Moderate-Serious |
| Alatawi et al. (2016) [16] | Observational | ROBINS-I | Confounding; measurement bias; self-report | Moderate |
| Almutairi et al. (2023) [11] | RCT | RoB 2.0 | Small sample; possible attrition bias; reporting limitations | Moderate |
| Branda et al. (2013) [21] | RCT | RoB 2.0 | Lack of blinding; potential performance bias | Moderate |
| Brundisini et al. (2015) [24] | Qualitative meta-synthesis | CASP | Selection of studies; interpretive bias; transferability | Moderate |
| Cheng et al. (2018) [12] | RCT | RoB 2.0 | Limited sample size; imprecision; unclear allocation concealment | Moderate |
| Habte et al. (2017) [25] | Mixed-methods | CASP | Integration bias; sampling limitations | Moderate |
| Haque et al. (2014) [26] | Qualitative | CASP | Limited generalisability; recall bias | Moderate |
| Islam et al. (2018) [13] | RCT | RoB 2.0 | Performance bias; intervention fidelity concerns | Moderate |
| Lauffenburger et al. (2019) [17] | RCT | RoB 2.0 | Lack of blinding; outcome assessment bias | Moderate |
| Lee and Lin (2010) [18] | Observational | ROBINS-I | Confounding; selection bias | Moderate |
| Peyrot et al. (2018) [1] | Observational | ROBINS-I | Self-reported outcomes; residual confounding | Moderate |
| Rossi et al. (2015) [22] | Observational | ROBINS-I | Confounding; selection bias; missing data | Serious |
| Schoenthaler et al. (2012) [19] | Observational | ROBINS-I | Confounding; reporting bias; missing data | Serious |
| Schunk et al. (2015) [2] | Observational | ROBINS-I | Recall bias; self-reported adherence; confounding | Moderate-Serious |
| Skinner et al. (2015) [14] | RCT | RoB 2.0 | Allocation concealment unclear; performance bias | Moderate |
| Varming et al. (2019) [20] | RCT | RoB 2.0 | Lack of blinding; implementation variability | Moderate |
| Wang et al. (2019) [23] | Cross-sectional observational study | CASP | Selection bias, Measurement bias | Moderate-High |
A total of 18 studies were included in the vote counting synthesis, comprising seven randomised controlled trials, eight observational studies, and three qualitative studies. Vote counting based on direction of effect was applied to assess the consistency of findings across three key outcome domains: glycaemic control, medication adherence, and psychosocial outcomes (Table 4). In relation to glycaemic control, measured by HbA1c, four studies reported improvements [11–14]. Eight studies found no significant effect directly or indirectly when compared with usual care [1, 2, 15–20], and three studies reported mixed or unclear findings [21–23]. The remaining three studies [24–26] did not assess effects on HbA1c. Overall, this distribution indicates that although there is a tendency towards improvement in HbA1c, the evidence remains inconsistent, with a substantial proportion of studies demonstrating either no effect or variable outcomes. For medication adherence, the evidence demonstrated a much more consistent pattern of improvement. Ten studies reported significant improvements in adherence [2, 11–14, 16, 17, 19, 20, 22], while eight studies reported no significant effect or mixed/unclear findings [1, 15, 18, 21, 23–26]. This body of evidence suggests that PCC interventions are associated with improved medication adherence across a range of settings and study designs. Psychosocial outcomes, including measures of patient empowerment, satisfaction, and engagement, also showed a consistent positive trend. Ten studies reported improvements in these outcomes [1, 11–13, 16, 18, 20–23], while eight studies reported no significant or mixed/unclear effects [2, 14, 15, 17, 19, 24–26]. Taken together, the vote counting analysis indicates that while PCC interventions demonstrate consistent effectiveness in improving medication adherence and psychosocial outcomes, their impact on glycaemic control is more variable and context-dependent.
Effect direction summary (vote counting by outcome).
| Study | Glycaemic control (HbA1c) | Medication adherence | Psychosocial outcomes |
|---|---|---|---|
| Adisa and Fakeye (2014) [15] | ▶ | ◼ | ◼ |
| Alatawi et al. (2016) [16] | ▶ | ▲ | ▲ |
| Almutairi et al. (2023) [11] | ▲ | ▲ | ▲ |
| Branda et al. (2013) [21] | ◼ | ▶ | ▲ |
| Brundisini et al. (2015) [24] | NA | ◼ | ◼ |
| Cheng et al. (2018) [12] | ▲ | ▲ | ▲ |
| Habte et al. (2017) [25] | NA | ◼ | ◼ |
| Haque et al. (2014) [26] | NA | ◼ | ◼ |
| Islam et al. (2018) [13] | ▲ | ▲ | ▲ |
| Lauffenburger et al. (2019) [17] | ▶ | ▲ | ▶ |
| Lee and Lin (2010) [18] | ▶ | ◼ | ▲ |
| Peyrot et al. (2018) [1] | ▶ | ◼ | ▲ |
| Rossi et al. (2015) [22] | ◼ | ▲ | ▲ |
| Schoenthaler et al. (2012) [19] | ▶ | ▲ | ◼ |
| Schunk et al. (2015) [2] | ▶ | ▲ | ◼ |
| Skinner et al. (2015) [14] | ▲ | ▲ | ◼ |
| Varming et al. (2019) [20] | ▶ | ▲ | ▲ |
| Wang et al. (2019) [23] | ◼ | ◼ | ▲ |
▲: significant improvement; ▶: no significant effect; ◼: mixed/unclear; NA: not applicable.
This systematic review was conducted in accordance with the PRISMA guidelines and provides evidence that PCC interventions are associated with meaningful improvements in medication adherence and psychosocial outcomes among individuals with T2D [11–13, 16, 20, 22]. These findings were consistently observed across the included studies, suggesting that PCC plays an important role in enhancing patient engagement, self-management behaviours, and overall experience of care. In contrast, the effects of PCC interventions on glycaemic control, as measured by HbA1c, were less consistent. While some studies demonstrated statistically significant reductions in HbA1c, others reported no significant differences when compared with usual care. The overall pattern of results therefore indicates a modest and variable impact on glycaemic outcomes rather than a universally positive or clinically robust effect. This variability highlights the complexity of achieving sustained metabolic control in diabetes and suggests that PCC alone may not be sufficient to produce consistent clinical improvements across all populations and settings.
The findings of this review highlight several important considerations for interpreting the effectiveness of PCC interventions. First, the consistency of intervention effects differed markedly across outcome domains. Improvements in medication adherence and psychosocial outcomes, such as patient empowerment, engagement, and satisfaction, were consistently observed, suggesting that PCC interventions are particularly effective in influencing behavioural and experiential aspects of care. By contrast, glycaemic control outcomes demonstrated mixed results, indicating that improvements in clinical biomarkers may not directly or uniformly follow from enhanced patient engagement alone. Second, there was substantial heterogeneity in the design and implementation of the included interventions. Variations in duration, intensity, delivery method, and the components of PCC interventions likely contributed to the observed differences in outcomes. For example, interventions that incorporated structured support mechanisms, such as regular follow-up, multidisciplinary involvement, or behavioural coaching, may have been more effective than less intensive or shorter-duration approaches. This heterogeneity complicates direct comparison across studies and limits the ability to identify a single optimal intervention model. Third, the context in which interventions were delivered appears to influence their effectiveness. Stronger effects were often observed in populations with higher baseline risk, such as individuals with poorly controlled diabetes or those with limited health literacy [11–13, 17, 20]. These findings suggest that PCC interventions may yield the greatest benefit when targeted toward vulnerable or high-need populations, where barriers to adherence and engagement are more pronounced.
This review has several notable strengths. By restricting inclusion to primary studies, it avoids duplication bias and ensures that findings are based on original data rather than secondary synthesis. The application of design-specific risk-of-bias tools, including RoB 2.0, ROBINS-I, and CASP, strengthens the methodological rigour of the assessment and allows for more nuanced evaluation of evidence quality across different study designs. Furthermore, the use of a structured narrative synthesis, incorporating direction-of-effect analysis, provides a transparent and systematic approach to summarising findings in the context of substantial heterogeneity. However, several limitations should be considered when interpreting the results. The heterogeneity across studies in terms of interventions, populations, and outcome measures precluded the use of meta-analysis, limiting the ability to generate pooled effect estimates. Variability in study quality and reporting standards also introduces uncertainty, particularly among observational studies, which were often subject to confounding and bias. In addition, the possibility of publication bias cannot be excluded, as studies reporting positive results may be more likely to be published. Finally, reliance on self-reported measures of medication adherence in some studies may have introduced reporting bias and overestimation of intervention effects.
The findings of this review suggest that PCC interventions are most effective when implemented as part of a comprehensive and structured care approach rather than as isolated strategies. Interventions that incorporate multidisciplinary support, particularly pharmacist-led medication management, appear to be associated with more consistent improvements in adherence. Tailoring interventions to the specific needs of patient populations, including cultural adaptation and consideration of health literacy, may further enhance their effectiveness. In addition, sufficient intensity and duration of intervention delivery appear to be critical factors in achieving meaningful outcomes. Given the inconsistent effects observed for glycaemic control, PCC should be conceptualised primarily as a supportive strategy that enhances patient engagement, adherence, and psychosocial well-being, rather than as a standalone intervention for achieving optimal metabolic control. Future research should focus on identifying the specific components of PCC interventions that are most effective, as well as evaluating their long-term impact on both behavioural and clinical outcomes. Greater standardisation in outcome measurement and reporting would also facilitate more robust comparisons across studies.
In summary, this systematic review demonstrates that PCC interventions are consistently associated with improvements in medication adherence and psychosocial outcomes as shown above among individuals with T2D. Evidence for improvements in glycaemic control is less consistent, with studies reporting a balanced distribution of positive, null, and mixed findings, indicating no uniform effect. Medication adherence outcomes showed the most consistent positive impact, particularly in interventions incorporating structured education, patient activation strategies, and pharmacist involvement. Similarly, psychosocial outcomes, including patient empowerment and satisfaction, improved across most studies, reinforcing the value of PCC in enhancing patient experience and engagement.
Overall, while variability in implementation and methodological quality persists, the evidence supports PCC as an effective component of diabetes management. Scaling up well-designed PCC interventions, particularly those that are pharmacist-led, culturally tailored, and empowerment-focused, has the potential to improve patient engagement and health outcomes and contribute to reducing the global burden of diabetes.
HbA1c: glycated haemoglobin
PCC: patient-centred care
T2D: type 2 diabetes
The supplementary table for this article is available at: https://www.explorationpub.com/uploads/Article/file/101477_sup_1.pdf.
TL: Conceptualization, Methodology, Writing—original draft. HG: Investigation, Data curation, Formal analysis, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
The primary data for this systematic review were sourced online from databases listed in the methods. Referenced articles are accessible on MEDLINE, Embase, EMCare, CINAHL, PsycINFO, and the Cochrane Library. Additional supporting data are available from the corresponding author upon request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 289
Download: 7
Times Cited: 0
Elif Basaran, Gulali Aktas
Roanne Lecky ... Catriona Kelly
Mehmet Ali Kosekli
Maher Monir Akl, Amr Ahmed
Yutang Wang ... Guang Yang
Ivonne G. Narváez-Ortiz ... Alberto Maceda-Serrano
Osama Mahmoud Mehanna ... Ahmad Shaban Abd El Monsef
Halima Babikir Eltahir ... Abdelrahim Osman Mohamed
