 Original Article
Original Article

Affiliation:
1Department of Physiology, Faculty of Medicine, Al-Azhar University, Damietta 34517, Egypt
2Department of Physiology, Faculty of Medicine, Horus University, Damietta 34517, Egypt
Email: OsamaMahmoud.2220@azhar.edu.eg; omahmoud@horus.edu.eg
ORCID: https://orcid.org/0000-0002-3076-5130
Affiliation:
3Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, Taif University, Taif 21944, Saudi Arabia
Affiliation:
4Department of Pathology, College of Medicine, Taif University, Taif 21944, Saudi Arabia
Affiliation:
1Department of Physiology, Faculty of Medicine, Al-Azhar University, Damietta 34517, Egypt
2Department of Physiology, Faculty of Medicine, Horus University, Damietta 34517, Egypt
Affiliation:
1Department of Physiology, Faculty of Medicine, Al-Azhar University, Damietta 34517, Egypt
Affiliation:
1Department of Physiology, Faculty of Medicine, Al-Azhar University, Damietta 34517, Egypt
2Department of Physiology, Faculty of Medicine, Horus University, Damietta 34517, Egypt
Affiliation:
5Medical Biochemistry and Molecular Biology Department, Faculty of Medicine, Al-Azhar University, Damietta 34517, Egypt
Affiliation:
6Physiology Department, Faculty of Medicine, Tanta University, Tanta 31527, Egypt
Affiliation:
7Forensic Toxicology Unit, Najran Forensic Medical Services Center, Ministry of Health, Najran 66241, Saudi Arabia
Affiliation:
1Department of Physiology, Faculty of Medicine, Al-Azhar University, Damietta 34517, Egypt
8Department of Anatomy and Physiology, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh 13317, Saudi Arabia.
Explor Endocr Metab Dis. 2026;3:101476 DOI: https://doi.org/10.37349/eemd.2026.101476
Received: March 31, 2026 Accepted: June 03, 2026 Published: July 08, 2026
Academic Editor: Gulali Aktas, Abant Izzet Baysal University Hospital, Turkey
The article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Aim: Diabetic neuropathy is the most prevalent diabetic complication, impacting up to 60% of people with diabetes. It is characterized by distal symmetrical loss of sensory function in the lower extremities, presenting with spontaneous excruciating neuropathic pain, hyperalgesia, and allodynia that impairs quality of life. The current work aims to evaluate the neuroprotective potential of naringin (a citrus flavonoid) and examine its ability to improve Streptozotocin (STZ)-induced diabetic neuropathic pain by investigating its hypoglycemic, lipid-lowering, anti-inflammatory, and antioxidant effects.
Methods: Diabetes was induced in 30 of 40 male Sprague-Dawley rats via a single STZ injection (45 mg/kg). Rats were divided into four groups: normal control, diabetic control, naringin-treated, and glimepiride-treated (positive control). After treatment, serum and brain tissues were collected to assess biochemical parameters. Pain-related behaviors were evaluated using hot plate, tail immersion, and von Frey filament tests.
Results: A significant increase in the serum levels of glucose, triglyceride, total cholesterol, low-density lipoprotein-cholesterol, and nitric oxide, with a concomitant decrease in body weight, plasma insulin, and high-density lipoprotein-cholesterol, was observed in diabetic rats. Also, the brain level of malondialdehyde was increased, while that of reduced glutathione, glutathione peroxidase, catalase, and superoxide dismutase were markedly decreased. Furthermore, diabetic rats showed a marked increase in plasma levels of inflammatory cytokines including interleukin-6 and tumor necrosis factor-α. Moreover, hot plate, tail immersion, and von Frey tests revealed hyperalgesia in diabetic rats. Treatment with naringin and glimepiride reduced pain hypersensitivity, restored body weight, and nearly normalized the altered biochemical parameters, more significantly with naringin than with glimepiride.
Conclusions: These results may highlight the potential effects of naringin as a therapeutic strategy for diabetes and its complications, including peripheral neuropathy.
Diabetes mellitus (DM) is a chronic condition marked by high blood sugar levels due to the inability of the body to produce or use insulin effectively. This condition disrupts the metabolism of carbohydrates, fats, and proteins, leading to various health complications. Diabetes is primarily classified into three types: type 1, an autoimmune disorder where the immune system destroys insulin-producing pancreatic β-cells; type 2, characterized by insulin resistance or insufficient insulin production; and gestational diabetes, which develops or is first diagnosed during pregnancy [1].
Poorly controlled DM leads to a range of serious long-term complications affecting various parts of the body. Long-term hyperglycemia in most cases results in various microvascular, macrovascular, and neural complications leading to conditions such as stroke, heart, kidney, and eye problems [2]. Among these secondary manifestations, diabetic neuropathy (DN) represents the most prevalent and debilitating complication, affecting up to 50% of all diabetic individuals. This condition typically manifests as symmetrical sensory loss, burning pain, and hyperalgesia, thereby severely disrupting patients’ quality of life. Diabetic neuropathic pain has been linked to local neuroinflammation and the activation of glial cells, where astrocytes and microglia become activated and release inflammatory mediators, which contribute to the regulation of pain signal transmission [3].
Diabetic-induced hyperalgesia is a condition where individuals with DN experience an increased sensitivity to pain. This can manifest as spontaneous pain or heightened responses to normally non-painful stimuli. The mechanisms behind hyperalgesia are complex and involve factors such as the formation of advanced glycation end products (AGEs), pro-inflammatory cytokines, and oxidative stress [4].
Flavonoids are natural compounds with diverse phenolic structures, commonly found in fruits, vegetables, grains, roots, stems, bark, tea, and wine. These natural products have many health benefits as they contain biologically active phytochemical constituents [5].
Flavonoids have been used in cosmetics, anti-wrinkle skin care products [6], and in natural dyes [7]. However, the most notable applications of flavonoids are in the medical field. They have been extensively used as antioxidants, anticancer, antiangiogenic, neuroprotective, antimicrobial, antiviral, and antiproliferative agents [8]. They also prevent cardiometabolic disorders [9] and have been shown to maintain better cognitive performance during aging [10].
Over 6,000 different classes and subclasses of flavonoids have been identified to date and are primarily synthesized by a variety of plants. Structurally, flavonoids have a 15-carbon skeleton, featuring 2 benzene rings connected by a three-carbon chain, hence classified as C6-C3-C6 compounds [11]. Depending on the carbon of the C ring to which the B ring is attached, as well as the degree of oxidation and unsaturation of the C ring, flavonoids can be split into a variety of distinct subgroups: isoflavones, neo-flavonoids, typical flavonoids (including flavones, flavonols, flavanones, flavanonols, catechins, and anthocyanins), and chalcones [5].
Naringin is a flavanone glycoside, scientifically known as 4’,5,7-trihydroxyflavanone-7-rhamnoglucoside, found in grapes and citrus fruits (the major flavonoid of grapefruit). Many studies have reported several biological effects of naringin, such as anti-inflammatory, antioxidant, antiviral, antihypertensive, hepatoprotective, nephroprotective, immunomodulatory, and anticancer activities, but some studies have also shown naringin-related side effects and drug interactions [12–14].
In accordance with the above, the main objective of the present work was to evaluate the potential antidiabetic, lipid-lowering, anti-inflammatory, and antioxidant effects of naringin, which may alleviate diabetic peripheral sensory neuropathy in rats, and compare them with those of the standard drug glimepiride.
The animal experiments were conducted following the guidelines and recommendations of the Institutional Animal Care and Use Committee (IACUC), after being approved by the Ethical Review Committee of the Faculty of Medicine, Al-Azhar University, Damietta, Egypt (DFM-IRB 00012398-11-03-002).
Naringin (Cat. No. 71162) and Streptozotocin (STZ) (Cat. No. S0130) were obtained from Sigma-Aldrich Chemical Co. (Burlington, MA, USA). Glimepiride (Amaryl) was purchased from Sanofi-Aventis (Cairo, Egypt). All other chemicals and reagents used were of analytical grade and purchased from standard commercial sources at the highest purity available.
Adult male, healthy Sprague-Dawley rats (n = 40, aged 9–12 weeks, weighing 150–200 g) were purchased from the National Research Centre (NRC) in Giza, Egypt. The animals were maintained under standard laboratory conditions in clean polypropylene cages (5 rats/cage), with a temperature of 22 ± 2°C, humidity (30–50% RH), and a 12-hour light/dark cycle. They had free access to water and standard rat chow throughout the adaptation period. Experimental procedures were conducted in the animal house of Damietta Faculty of Medicine, Al-Azhar University, Egypt.
After a two-week adaptation period, DM was induced via a single intraperitoneal injection of STZ (45 mg/kg body weight [BW]) dissolved in 0.1 M citrate buffer (pH 4.5) [15], whereas control animals received an equal volume of the vehicle alone. Fasting blood glucose (FBG) levels were assessed 72 hours post-injection using a glucometer (Easy Gluco, Infopia, Korea); subsequently, only animals exhibiting concentrations exceeding 250 mg/dL were included in the diabetic cohorts for subsequent pharmacological evaluation.
Immediately following the confirmation of diabetes, the standard rat chow was replaced with a high-fat diet (HFD). This dietary regimen was maintained for a duration of four weeks to facilitate the development of diabetic complications, specifically peripheral neuropathy. The HFD consisted of 60% of total kcal (daily energy intake) from fat, 20% of total kcal from carbohydrates, and 20% of total kcal from protein (comprising lard, cholesterol, and standard nutrients) [16].
The rats were then divided into four groups as follows: Group 1, normal control (NC): 10 non-diabetic rats received citrate buffer (pH 4.5) and normal drinking water. Group 2, diabetic control (DC): 10 diabetic rats received normal drinking water. Group 3, naringin-treated diabetic rats (NGN-D): 10 diabetic rats, treated with naringin (100 mg/kg BW/day) by intragastric gavage for 4 weeks [17]. Group 4, glimepiride-treated diabetic rats (GD-D): 10 diabetic rats received glimepiride (0.5 mg/kg BW/day) orally for 4 weeks [18].
Initial BW was measured at the beginning of the experiment, and final BW was recorded at the end of the experiment. The next day after treatment, hyperalgesia was assessed by several behavioral tests, blood samples were collected from retro-orbital veins, and the rats were then anesthetized via i.p. injection of a mixture of 50 mg/kg ketamine hydrochloride and 5 mg/kg xylazine [19] and killed by decapitation. The animals’ brains were removed, washed with ice-cold saline after removing the adhering tissue, and stored on ice. The animal experiments were approved by the Ethical Review Committee of the Faculty of Medicine, Al-Azhar University, Damietta, Egypt (DFM-IRB 00012398-11-03-002).
A comprehensive visual timeline detailing the spanning adaptation, DN confirmation, treatment, and assessment phases is illustrated in Figure 1.
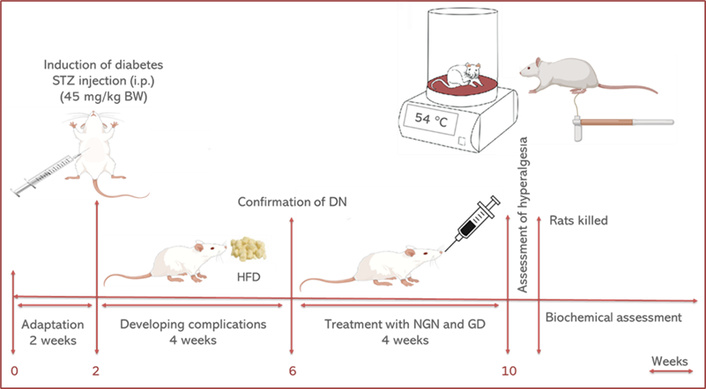
Graphical experimental design. BW: body weight; DN: diabetic neuropathy; HFD: high-fat diet; STZ: Streptozotocin; GD: glimepiride; NGN: naringin.
For measurement of insulin, interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α), plasma was separated by collecting a portion of the blood into heparinized tubes and centrifuging it at 600 × g for 15 min. Another portion of the blood was centrifuged at 3,000 × g for 15 min to separate the serum for determination of glucose, triglyceride (TG), total cholesterol (TC), high-density lipoprotein-cholesterol (HDL-C), low-density lipoprotein-cholesterol (LDL-C), and nitric oxide (NO).
On the other hand, the stored brain tissues were rinsed with ice-cold saline, dried, sectioned into small pieces, and then homogenized in ice-cold buffer (10 mM KH2PO4; 20 mM EDTA; 30 mM KCl). The resulting homogenate was centrifuged at 4°C (1,000 × g for 10 min), and the isolated supernatant was used to determine brain oxidants and antioxidant defense markers.
Serum glucose, TG, TC, LDL-C, HDL-C, proinflammatory cytokines including TNF-α, and IL-6 were measured by enzymatic methods using commercially available kits (RayBiotech), following the manufacturer’s recommendations.
Brain level of malondialdehyde (MDA) was measured following the method described by Ohkawa et al. [20]. Superoxide dismutase (SOD) activity was measured by the conventional technique of Marklund S and Marklund G [21]. NO and catalase (CAT) enzyme activity were calorimetrically assessed according to Montgomery and Dymock [22] and Aebi [23], respectively. Glutathione peroxidase (GPx) enzyme activity was assessed following the method of Paglia and Valentine [24] and Factor et al. [25] by measuring NADPH oxidation at 340 nm in the presence of glutathione.
Primary and secondary antibodies were utilized in accordance with validated manufacturer protocols. Astrocytic activation was quantified in brain tissue sections using a rabbit polyclonal anti-Glial Fibrillary Acidic Protein (GFAP) primary antibody (Cat. No. ab7260, Abcam, Cambridge, UK; dilution 1:1000). Microglial profiling was conducted using a rabbit polyclonal anti-ionized calcium-binding adapter molecule 1 (Iba1) antibody (Cat. No. 019-19741, Wako Pure Chemical Industries, Osaka, Japan; dilution 1:500). Tissue sections were subsequently incubated with a horseradish peroxidase (HRP)-conjugated goat anti-rabbit IgG secondary antibody (Cat. No. sc-2004, Santa Cruz Biotechnology, Dallas, TX, USA; dilution 1:2000). Visualizations and cellular quantification were performed via light microscopy, with negative control sections processed omitting the primary antibodies to confirm staining specificity.
Diabetes-induced hyperalgesia was evaluated in the diabetic rats by observing pain thresholds and pain perception using behavioral tests including hot plate, tail immersion, and mechanical sensitivity (von Frey) tests [26].
In the hot plate test, rats were placed individually on a hot plate (54 ± 0.1°C), and the latency to front and hind paw licking, rubbing, or jumping to avoid the heat was determined. To prevent thermal injury to the paw tissue, a maximum cut-off time of 30 s was strictly enforced, adapting safety parameters established in previous literature [27].
The tail immersion test was conducted by immersing the distal portion of the rat’s tail into a hot water bath maintained at 55 ± 0.5°C. The latency period before the tail withdrawal reflex was recorded; a shorter latency indicates thermal hyperalgesia. To ensure optimal ethical care and prevent thermal tissue damage, a maximum cut-off time of 15 seconds was strictly enforced to terminate stimulus exposure in the absence of a spontaneous reflex [28].
In the mechanical sensitivity (von Frey) test, rats were placed individually in mesh-floored boxes and allowed to adapt for 20 min. Calibrated von Frey filaments were pressed perpendicularly on the plantar surface of the hind paw with a sufficient force to bend the filament for 6 s. With animals that did not give a response, filaments of the next-greater force were applied, while in the presence of a response, filaments of the next-lower force were used. Each animal underwent 4 to 5 trials separated by 5-min intervals. The mean threshold force, expressed in grams, required to trigger a paw withdrawal reflex was calculated and used for statistical analysis [29].
Data were analyzed using SPSS software (version 22.0; IBM Corp., Armonk, NY, USA). The normality of data distribution and homogeneity of variance were assessed using the Shapiro-Wilk and Levene’s tests, respectively. Quantitative variables are expressed as mean ± standard error of the mean for n = 10 animals per group. Significant differences between multiple groups were determined using one-way analysis of variance (ANOVA), followed by Tukey’s post-hoc test for pairwise multiple comparisons. Statistical significance was defined as p < 0.05. Results were further categorized as highly significant at p < 0.001, while values of p > 0.05 were considered statistically non-significant.
As shown in Table 1, there were no significant differences (p > 0.05) in the BW between the studied groups at the beginning of the experiment. At the end of the experiment, diabetic rats showed a decrease in the final BW, with a significantly reduced weight gain (p < 0.01) compared to the NC rats. Treatment with naringin or glimepiride resulted in significant weight gain and recovery of the reduced BW compared with the DC rats (p < 0.01). Table 1 also shows that naringin and glimepiride significantly modulate the glycemic status of diabetic rats by decreasing plasma glucose and increasing insulin levels compared with DC rats (p < 0.01).
Effect of treatment on body weight and the glycemic status of diabetic rats.
| Item | Groups | ||||
|---|---|---|---|---|---|
| NC | DC | NGN-D | GD-D | p-value | |
| Initial BW (g) | 161.07 ± 1.89 | 169.15 ± 1.33 | 165.36 ± 1.81 | 167.17 ± 1.48 | p > 0.05 |
| Final BW (g) | 200.15 ± 2.29 | 146.41 ± 2.45a | 209.4 ± 2.31b | 206.94 ± 3.84b | p < 0.01 |
| Weight gain | 41.08 ± 0.41 | –23.74 ± 2.12a | 44.04 ± 0. 5b | 39.77 ± 2.36b | p < 0.01 |
| Glucose (mg/dL) | 68.47 ± 5.12 | 229.17 ± 8.13a | 72.08 ± 4.13b | 74.91 ± 4.41b | p < 0.01 |
| Insulin (μU/mL) | 17.44 ± 2.19 | 7.17 ± 0.81a | 19.08 ± 1.54b | 21.11 ± 2.53b | p < 0.01 |
Data are expressed as means ± SEM of 10 rats/group. Initial and final body weight (BW) were measured, and weight gain was calculated. a Significantly different from the NC group (p < 0.01); b Significantly different from the DC group (p < 0.01). DC: diabetic control; GD-D: glimepiride-treated diabetic rats; NC: normal control; NGN-D: naringin-treated diabetic rats.
The results of hot-plate and tail-immersion tests revealed a significantly decreased pain threshold in DC rats compared to the NC rats (p < 0.01). Both tests revealed a significant increase in nociceptive threshold in both naringin-treated and GD-D rats as compared to DC rats (p < 0.01), with a more pronounced response in the tail-immersion test to naringin compared to glimepiride (p < 0.05) (Figure 2). Also, the results of the mechanical sensitivity (von Frey) test revealed a significant reduction in the tactile withdrawal threshold in DC rats compared with the NCs (p < 0.01), which was significantly corrected when diabetic rats were treated with either naringin or glimepiride (Figure 2).
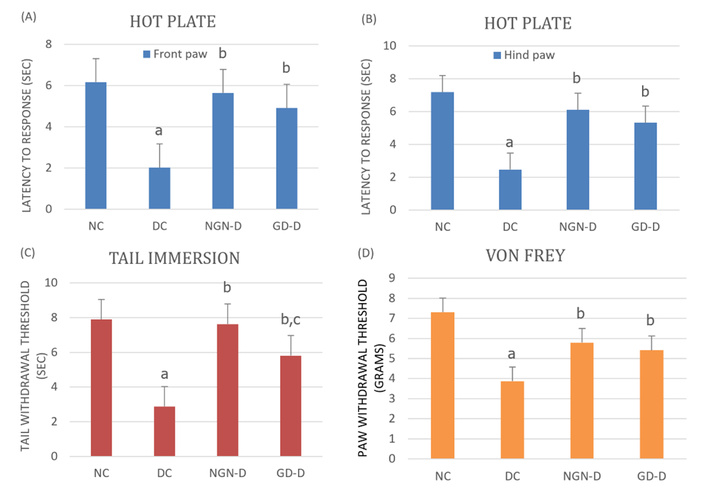
Effect of naringin or glimepiride on pain threshold in the (A) hot plate (front paw), (B) hot plate (hind paw), (C) tail immersion, and (D) von Frey tests in diabetic rats. Naringin or glimepiride significantly increased response latency in the hot plate and tail immersion tests, and tactile withdrawal threshold in the von Frey test, with a more pronounced response in the tail-immersion test to naringin compared to glimepiride. Data are expressed as means ± SEM of 10 rats/group. a Significantly different from the NC group (p < 0.01); b Significantly different from the DC group (p < 0.01); c Significantly different from the NGN-D group (p < 0.05). DC: diabetic control; GD-D: glimepiride-treated diabetic rats; NC: normal control; NGN-D: naringin-treated diabetic rats.
As shown in Table 2, diabetic rats reported significantly higher levels of TG, TC, LDL-C, TNF-α, and IL-6, with a significant reduction in HDL-C compared with the NC rats. Interestingly, the naringin and glimepiride-treated diabetic groups experienced ameliorated alterations in NO, serum lipids, as well as plasma IL-6 and TNF-α, with almost the same degree of efficacy for all observed parameters except for the proinflammatory cytokines, where the anti-inflammatory effect of naringin was more pronounced than that of glimepiride (p < 0.05).
Effect of treatment on lipid profile and proinflammatory cytokines in diabetic rats.
| Items | Groups | ||||
|---|---|---|---|---|---|
| NC | DC | NGN-D | GD-D | p-value | |
| TG (mg/dL) | 75.02 ± 1.4 | 131.17 ± 2.31a | 69.15 ± 4.42b | 71.66 ± 5.37b | p < 0.01 |
| TC (mg/dL) | 81.15 ± 4.72 | 125.42 ± 3.88a | 76.91 ± 3.21b | 79.77 ± 5.81b | p < 0.01 |
| LDL-C (mg/dL) | 34.62 ± 3.52 | 79.74 ± 2.52a | 32.71 ± 3.65b | 35.55 ± 3.67b | p < 0.01 |
| HDL-C (mg/dL) | 38.14 ± 3.49 | 16.32 ± 2.38a | 40.12 ± 3.71b | 37.28 ± 2.46b | p < 0.01 |
| TNF-α (ng/mL) | 0.74 ± 0.19 | 2.31 ± 0.08a | 0.76 ± 0.15b | 1.02 ± 0.14bc | p < 0.01 |
| IL-6 (pg/mL) | 311.4 ± 7.06 | 612.1 ± 27.18a | 309.2 ± 11.4b | 357.6 ± 32.2bc | p < 0.01 |
Data are expressed as means ± SEM of 10 rats/group. a Significantly different from the NC group (p < 0.01); b Significantly different from the DC group (p < 0.01); c Significantly different from the NGN-D group (p < 0.05). DC: diabetic control; GD-D: glimepiride-treated diabetic rats; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; NC: normal control; NGN-D: naringin-treated diabetic rats; TC: total cholesterol; TG: triglyceride; TNF-α: tumor necrosis factor-α.
Table 3 shows the effect of treatment with naringin and glimepiride on brain oxidants and antioxidant defense markers in diabetic rats, where the DC rats had a significant increase in plasma NO level and brain content of MDA, with a significant decrease in brain GSH, GPx, SOD, and CAT compared to the NC rats. In contrast, the naringin-treated and GD-D showed nearly normalized brain levels of MDA, GSH, GPx, SOD, and CAT, with no significant difference between the two drugs.
Effect of treatment on oxidative stress biomarkers in diabetic rats.
| Brain content (mg pr) | Groups | ||||
|---|---|---|---|---|---|
| NC | DC | NGN-D | GD-D | p-value | |
| NO (μmol/L) | 5.47 ± 1.23 | 19.18 ± 3.53a | 7.06 ± 2.62b | 7.97 ± 1.41b | p < 0.01 |
| MDA (nmol/mg pr) | 1.15 ± 0.29 | 5.42 ± 0.48a | 1.43 ± 0.31b | 1.81 ± 0.21b | p < 0.01 |
| GSH (μg/mg pr) | 7.17 ± 1.41 | 2.74 ± 0.12a | 6.14 ± 0.75b | 5.73 ± 1.06b | p < 0.01 |
| GPx (U/mg pr) | 28.14 ± 3.19 | 16.21 ± 2.13a | 25.12 ± 3.41b | 24.28 ± 2.34b | p < 0.01 |
| SOD (units/mg pr) | 5.41 ± 0.51 | 2.21 ± 1.48a | 4.72 ± 1.39b | 3.35 ± 1.15b | p < 0.01 |
| CAT (μmol of H2O2) | 5.53 ± 1.51 | 3.18 ± 0.46a | 5.62 ± 1.01b | 6.39 ± 1.33b | p < 0.01 |
Data are expressed as means ± SEM of 10 rats/group. a Significantly different from the NC group (p < 0.01); b Significantly different from the DC group (p < 0.01). CAT: catalase; DC: diabetic control; GD-D: glimepiride-treated diabetic rats. GPx: glutathione peroxidase; GSH: reduced glutathione; MDA: malondialdehyde; NC: normal control; NGN-D: naringin-treated diabetic rats; NO: nitric oxide; SOD: superoxide dismutase.
DN is exceptionally challenging to investigate due to the multifactorial nature of diabetic nerve injury. This process is primarily driven by chronic hyperglycemia, dyslipidemia, microvascular inflammation, and the progressive accumulation of AGEs [4, 30]. Mechanistically, STZ-induced neurodegeneration stems from a cascade where excessive intracellular glucose accelerates metabolic flux, yielding a profound overproduction of reactive oxygen species (ROS) and free radicals that overwhelm endogenous antioxidant defenses [29]. This persistent oxidative stress directly triggers endoplasmic reticulum (ER) stress, thereby initiating downstream neuronal apoptotic pathways within the peripheral nerve architecture [31].
The present study investigated the neuroprotective properties of naringin (a citrus flavonoid) on STZ-induced peripheral DN in rats by investigating its hypoglycemic, hypolipidemic, antioxidant, and anti-inflammatory effects and compared them with the effects of glimepiride (a standard antidiabetic drug). Crucially, our key findings demonstrate that naringin intervention successfully counteracted diabetic dyslipidemia, restored weight loss, and nearly normalized plasma glucose and insulin levels. At the neurobehavioral level, naringin significantly corrected altered pain thresholds in hot plate, tail immersion, and von Frey tests by suppressing systemic inflammatory cytokines (TNF-α and IL-6) and brain lipid peroxidation (MDA). While both therapeutic strategies yielded comparable improvements in lipid parameters and oxidative stress markers, naringin demonstrated a significantly superior capacity to attenuate neuroinflammation and thermal hyperalgesia compared to glimepiride. These pivotal results highlight naringin's promise as a targeted neuroprotective strategy that directly combats the multifactorial pathogenesis of diabetic nerve injury.
In this study, treatment of diabetic rats with naringin or glimepiride resulted in significant weight gain and nearly normalized plasma glucose and insulin levels. These results are consistent with previous studies showing that naringin can increase insulin secretion and reduce blood glucose levels by modulating key enzymes involved in glucose metabolism [32–34].
Our experimental data demonstrate that the administration of either naringin or the standard reference drug, glimepiride, significantly mitigates thermal hyperalgesia and mechanical tactile allodynia in STZ-treated rats, as evidenced by increased response latency in tail immersion and hot plate tests, and tactile withdrawal threshold in von Frey test, with naringin showing a more pronounced effect in the tail-immersion test suggesting its stronger anti-inflammatory and antioxidant properties [35]. These findings align with previous research suggesting that naringin reduces neuroinflammation and oxidative stress, both of which are key contributors to neuropathic pain [16]. These results are also similar to previous studies that observed a reduced pain threshold in animals following diabetes induction, as well as a dose-dependent improvement after treatment with naringin [36, 37].
Elevated levels of TG, TC, and LDL-C, along with reduced HDL-C, are common in diabetes and contribute to cardiovascular risk. Inflammatory cytokines are frequently linked to the induction of neuropathic pain, the hyperexcitability of afferent sensory nerves, and demyelination. Furthermore, they can alter the permeability of the blood-nerve barrier, ultimately leading to peripheral neuronal degeneration [38, 39]. This study showed that naringin or glimepiride significantly improved the lipid profile and reduced inflammatory cytokines in diabetic rats, with naringin showing a more pronounced anti-inflammatory effect. This highlights their role in alleviating diabetic dyslipidemia and inflammation, which are critical factors in the development of diabetic complications. These findings are consistent with the observation that naringin reduces hypercholesterolemia in rats fed a HFD by inhibiting 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reductase, resulting in lower plasma LDL-C and TG levels, without impacting HDL-C levels [40]. Consistently, in localized peripheral nerve injury and experimental inflammation models, Hu and Zhao [41], Tsai et al. [42], and Zeghichi-Hamri et al. [43] demonstrated that treatment with this citrus flavonoid significantly suppressed glial activation and inhibited the formation and release of these key pro-inflammatory mediators.
Oxidative stress plays a central role in the pathogenesis of diabetes and its complications. This study found that diabetic rats exhibited increased levels of MDA and decreased brain levels of GSH, GPx, SOD, and CAT. Treatment with naringin or glimepiride attenuated oxidative stress and improved antioxidant capacity in the brains of diabetic rats, indicating their potential to protect against oxidative damage. This is consistent with other studies showing that naringin has strong antioxidant properties via decreasing lipid peroxidation and buildup of ROS [44], thereby restoring and elevating SOD, GSH, GPx, and CAT activities [45].
While both naringin and glimepiride effectively managed hyperglycemia and improved the lipid profile, naringin demonstrated a significantly greater capacity to attenuate neuroinflammation and thermal hyperalgesia. Specifically, naringin outperformed glimepiride in reducing pro-inflammatory cytokines (TNF-α and IL-6) and increasing latency in the tail immersion test. In contrast, both treatments yielded comparable improvements in oxidative stress markers (MDA, GSH, GPx, SOD, and CAT) and lipid parameters (TG, TC, LDL-C, and HDL-C). These findings suggest that while both agents provide systemic benefits, naringin may offer superior targeted neuroprotective effects, making it a promising candidate for the management of DN [37]. A summary of the molecular pathways of diabetic nerve injury alongside the protective roles of naringin and glimepiride is illustrated in Figure 3.
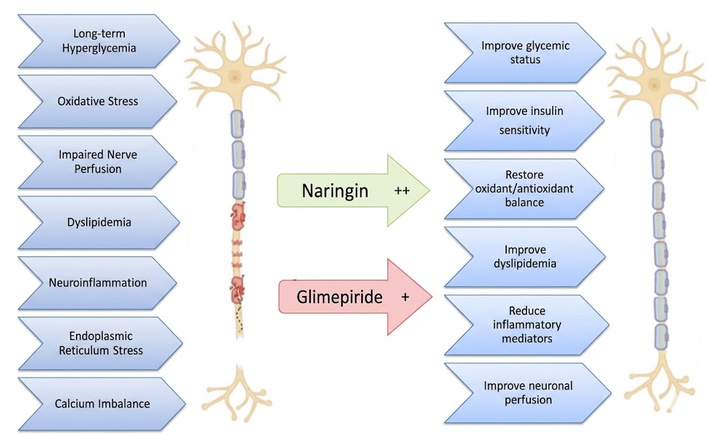
Scheme summarizing some of the molecular mechanisms of diabetes-induced neuronal damage, and how treatment with naringin or glimepiride improves it.
In summary, the study highlights the therapeutic potential of naringin in the management of diabetes and its complications, comparing it with glimepiride. Both compounds were effective in improving BW, glycemic status, pain sensitivity, lipid profile, neuroinflammation, and oxidative stress in diabetic rats. Notably, naringin exhibited more significant anti-inflammatory and antioxidant effects. These findings suggest that naringin could be a valuable addition to diabetes treatment, offering benefits beyond glycemic control, such as protection against neuropathy, dyslipidemia, and oxidative damage.
A limitation of this study is that it didn’t thoroughly investigate all the molecular mechanisms of naringin’s mitigating effects in DN; more in-depth research on its detailed mechanisms of action is needed. Also, further research utilizing nerve conduction velocity and molecular signaling assays is warranted to fully elucidate the underlying mechanisms of action. Furthermore, the present study utilized whole-brain homogenate for biochemical quantification. While this provides a global assessment of oxidative stress and inflammation, it may dilute region-specific variations. Since areas such as the hippocampus and cerebral cortex are known to be particularly vulnerable to diabetic metabolic insults, future studies should employ regional dissection to further refine our understanding of naringin’s site-specific neuroprotective mechanisms.
AGEs: advanced glycation end products
BW: body weight
CAT: catalase
DC: diabetic control
DM: diabetes mellitus
DN: diabetic neuropathy
GD-D: glimepiride-treated diabetic rats
GPx: glutathione peroxidase
HDL-C: high-density lipoprotein-cholesterol
HFD: high-fat diet
LDL-C: low-density lipoprotein-cholesterol
MDA: malondialdehyde
NC: normal control
NGN-D: naringin-treated diabetic rat
NO: nitric oxide
ROS: reactive oxygen species
SOD: superoxide dismutase
STZ: Streptozotocin
TC: total cholesterol
TG: triglyceride
TNF-α: tumor necrosis factor-α
OMM: Conceptualization, Methodology, Data curation, Formal analysis, Investigation, Writing—review & editing. AE: Conceptualization, Methodology, Data curation, Formal analysis, Writing—original draft, Writing—review & editing. BHE: Conceptualization, Data curation, Formal analysis, Writing—review & editing. MGMH: Methodology, Investigation. MAMA: Methodology, Writing—original draft. MRE: Methodology, Writing—original draft. AMH: Methodology, Investigation. NMG: Methodology, Investigation, Writing—original draft. AIS: Methodology, Writing—original draft. ASAEM: Methodology, Investigation. All authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
The animal study protocol has been approved by the Ethical Review Committee of the Faculty of Medicine, Al-Azhar University, Damietta, Egypt (DFM-IRB 00012398-11-03-002). All procedures were performed in strict accordance with international standards for the care and treatment of laboratory animals.
Not applicable.
Not applicable.
The datasets supporting the findings of this study are available from the corresponding author upon reasonable request.
The authors would like to acknowledge the Deanship of Graduate Studies and Scientific Research, Taif University, for funding this work. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 243
Download: 13
Times Cited: 0
Elif Basaran, Gulali Aktas
Roanne Lecky ... Catriona Kelly
Mehmet Ali Kosekli
Maher Monir Akl, Amr Ahmed
Yutang Wang ... Guang Yang
Ivonne G. Narváez-Ortiz ... Alberto Maceda-Serrano
Thewodros Leka, Hemda Garelick
Halima Babikir Eltahir ... Abdelrahim Osman Mohamed
