
















Aim:
Tremor is one of the most common neurological movement disorders, arising from dysfunction in the neuromuscular system. However, comprehensive analyses of peripheral blood elements, red blood cells (RBC) and white blood cells (WBC) counts, as well as liver and kidney function in patients with tremor remain limited. This cross-sectional study investigated alterations in serum elements, complete blood counts, and liver function in patients with tremor. The study sought to identify independent risk factors and evaluate their diagnostic performance.
Methods:
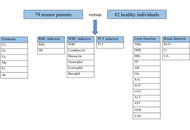
Blood samples from 79 patients with tremor and 82 healthy controls were analyzed. Serum elements, RBC, WBC, platelet (PLT), liver function, and renal function were measured using the QL8000 element analyzer, XN 2800 automated hematology analyzer, and Roche Cobas 8000 system.
Results:
Serum copper (Cu) and lead (Pb) levels were significantly elevated in tremor patients. These patients also showed increased monocytes, decreased eosinophils, and impaired liver function, including elevated aspartate aminotransferase and globulin with reduced albumin.
Conclusions:
Tremor patients show distinct alterations in Cu, Pb, monocyte counts, eosinophil counts, and liver function markers. These findings suggest that these parameters may serve as potential diagnostic indicators and therapeutic targets. Cu and Pb were identified as independent risk factors, and their combination significantly improved diagnostic efficiency.
Aim:
Tremor is one of the most common neurological movement disorders, arising from dysfunction in the neuromuscular system. However, comprehensive analyses of peripheral blood elements, red blood cells (RBC) and white blood cells (WBC) counts, as well as liver and kidney function in patients with tremor remain limited. This cross-sectional study investigated alterations in serum elements, complete blood counts, and liver function in patients with tremor. The study sought to identify independent risk factors and evaluate their diagnostic performance.
Methods:
Blood samples from 79 patients with tremor and 82 healthy controls were analyzed. Serum elements, RBC, WBC, platelet (PLT), liver function, and renal function were measured using the QL8000 element analyzer, XN 2800 automated hematology analyzer, and Roche Cobas 8000 system.
Results:
Serum copper (Cu) and lead (Pb) levels were significantly elevated in tremor patients. These patients also showed increased monocytes, decreased eosinophils, and impaired liver function, including elevated aspartate aminotransferase and globulin with reduced albumin.
Conclusions:
Tremor patients show distinct alterations in Cu, Pb, monocyte counts, eosinophil counts, and liver function markers. These findings suggest that these parameters may serve as potential diagnostic indicators and therapeutic targets. Cu and Pb were identified as independent risk factors, and their combination significantly improved diagnostic efficiency.
DOI: https://doi.org/10.37349/emed.2026.1001414
Artificial intelligence (AI) has rapidly advanced in radiology, demonstrating high performance across a wide range of diagnostic tasks. However, clinical adoption remains slower and more uneven than anticipated. This discrepancy reflects a fundamental gap between algorithm validation and clinical implementation. Current validation strategies primarily rely on controlled datasets and performance metrics such as accuracy and area under the curve, which often fail to capture the complexity of clinical environments. This article examines the nature of this “validation gap” and argues that it reflects a broader structural mismatch between how AI systems are evaluated and how clinical care operates. We propose a conceptual framework comprising three levels of validation: technical validity, workflow validity, and clinical validity. While most studies focus on technical performance, limited attention is given to integration into clinical workflows and impact on patient outcomes. Key factors contributing to this gap include limited generalizability across diverse populations and imaging protocols, poor alignment with clinical workflows, and the underrepresentation of uncertainty in model outputs. These limitations hinder effective implementation and may reduce trust in AI systems. Bridging this gap requires a shift toward more comprehensive validation strategies, including multicenter and prospective studies, improved workflow integration, and explicit incorporation of uncertainty and human–AI interaction. Ultimately, the clinical value of AI in radiology should be assessed not only by its performance in controlled settings but also by its ability to support decision-making and improve patient outcomes in real-world practice.
Artificial intelligence (AI) has rapidly advanced in radiology, demonstrating high performance across a wide range of diagnostic tasks. However, clinical adoption remains slower and more uneven than anticipated. This discrepancy reflects a fundamental gap between algorithm validation and clinical implementation. Current validation strategies primarily rely on controlled datasets and performance metrics such as accuracy and area under the curve, which often fail to capture the complexity of clinical environments. This article examines the nature of this “validation gap” and argues that it reflects a broader structural mismatch between how AI systems are evaluated and how clinical care operates. We propose a conceptual framework comprising three levels of validation: technical validity, workflow validity, and clinical validity. While most studies focus on technical performance, limited attention is given to integration into clinical workflows and impact on patient outcomes. Key factors contributing to this gap include limited generalizability across diverse populations and imaging protocols, poor alignment with clinical workflows, and the underrepresentation of uncertainty in model outputs. These limitations hinder effective implementation and may reduce trust in AI systems. Bridging this gap requires a shift toward more comprehensive validation strategies, including multicenter and prospective studies, improved workflow integration, and explicit incorporation of uncertainty and human–AI interaction. Ultimately, the clinical value of AI in radiology should be assessed not only by its performance in controlled settings but also by its ability to support decision-making and improve patient outcomes in real-world practice.
DOI: https://doi.org/10.37349/emed.2026.1001412
This article belongs to the special issue Artificial Intelligence in Precision Imaging: Innovations Shaping the Future of Clinical Diagnostics
Artificial intelligence (AI) is transforming clinical decision-making across cranio-maxillofacial trauma, oral health, and systemic disease. These domains are increasingly recognised as biologically and clinically interconnected, yet they are often studied and managed independently. This perspective introduces the concept of an integrative triangle linking facial trauma, oral health, and systemic disease, with AI serving as the computational bridge that enables cross-domain modelling and coordinated care. AI applications within this framework include imaging-based fracture detection, patient-specific implant design, automated oral disease diagnosis, multimodal risk prediction, and longitudinal outcome modelling. By integrating imaging, clinical, laboratory, and behavioural data, AI can identify shared inflammatory and metabolic pathways influencing trauma recovery and chronic disease progression. This closed-loop paradigm supports continuous learning, allowing outcomes in one domain to inform prediction and intervention in the others. The integrative triangle provides a translational roadmap for precision medicine, moving from isolated prediction toward coordinated prevention and intervention. Future development will require multimodal data integration, prospective validation, and responsible governance to ensure explainable and equitable AI deployment. This framework positions facial trauma and oral health as central components of systemic precision medicine and highlights AI as a catalyst for integrated, patient-centred care.
Artificial intelligence (AI) is transforming clinical decision-making across cranio-maxillofacial trauma, oral health, and systemic disease. These domains are increasingly recognised as biologically and clinically interconnected, yet they are often studied and managed independently. This perspective introduces the concept of an integrative triangle linking facial trauma, oral health, and systemic disease, with AI serving as the computational bridge that enables cross-domain modelling and coordinated care. AI applications within this framework include imaging-based fracture detection, patient-specific implant design, automated oral disease diagnosis, multimodal risk prediction, and longitudinal outcome modelling. By integrating imaging, clinical, laboratory, and behavioural data, AI can identify shared inflammatory and metabolic pathways influencing trauma recovery and chronic disease progression. This closed-loop paradigm supports continuous learning, allowing outcomes in one domain to inform prediction and intervention in the others. The integrative triangle provides a translational roadmap for precision medicine, moving from isolated prediction toward coordinated prevention and intervention. Future development will require multimodal data integration, prospective validation, and responsible governance to ensure explainable and equitable AI deployment. This framework positions facial trauma and oral health as central components of systemic precision medicine and highlights AI as a catalyst for integrated, patient-centred care.
DOI: https://doi.org/10.37349/emed.2026.1001413
Recent studies argue that other physiological solutions are superior to normal saline, which is due to their physiological features, better outcomes in critical care, and lower risk of hyperchloremia and acidosis; nonetheless, it is still a mystery how normal saline has dominated the field of fluid therapy worldwide. Moreover, there is an ongoing debate on whether harm to human health may limit its spread in the future. Additionally, new evidence revealed some of the deleterious effects of normal saline, including coagulopathy, metabolic acidosis, acute kidney injury (AKI), and higher mortality in ICU. The predominant cause for these outcomes appears to be the excess chloride concentration of normal saline relative to plasma. Therefore, it appears relevant to suggest that a normal saline solution should be normalized to that of human serum to overcome these pitfalls. An ideal normal saline solution shall be similar to human serum in its pH, osmolarity, and content of sodium, chloride, and essential minerals.
Recent studies argue that other physiological solutions are superior to normal saline, which is due to their physiological features, better outcomes in critical care, and lower risk of hyperchloremia and acidosis; nonetheless, it is still a mystery how normal saline has dominated the field of fluid therapy worldwide. Moreover, there is an ongoing debate on whether harm to human health may limit its spread in the future. Additionally, new evidence revealed some of the deleterious effects of normal saline, including coagulopathy, metabolic acidosis, acute kidney injury (AKI), and higher mortality in ICU. The predominant cause for these outcomes appears to be the excess chloride concentration of normal saline relative to plasma. Therefore, it appears relevant to suggest that a normal saline solution should be normalized to that of human serum to overcome these pitfalls. An ideal normal saline solution shall be similar to human serum in its pH, osmolarity, and content of sodium, chloride, and essential minerals.
DOI: https://doi.org/10.37349/emed.2026.1001411
Aim:
To evaluate ultrasound-derived congestion phenotypes in acute decompensated heart failure with preserved ejection fraction (HFpEF) and their association with cardiac remodeling and in-hospital outcomes.
Methods:
This prospective study included 235 patients (median age 77.0 years, 75.3% women) with acute decompensated HFpEF. Within 2 hours of admission, all patients underwent echocardiography, lung ultrasound (B-lines), venous excess ultrasound score (VExUS) assessment, and bioimpedance analysis. Patients were classified into three phenotypes based on pulmonary (B-lines > 3) and systemic venous congestion (VExUS): low-low (no significant pulmonary or systemic congestion), pulmonary-dominant, and mixed severe. The primary endpoint was in-hospital mortality.
Results:
Moderate-to-severe venous congestion (VExUS grade 2–3) was present in 60.8% of patients. The mixed severe phenotype predominated (60.9%) and was associated with higher body mass index (BMI) and waist (p < 0.001). This group demonstrated more advanced cardiac dysfunction, including higher E/e’ (14.9 vs. 11.9; p < 0.001), greater left atrial remodeling (left atrial volume index 45.0 vs. 39.0 mL/m2; p < 0.001), and increased left ventricular mass index (p = 0.010). Right ventricular (RV) involvement was more pronounced, with lower TAPSE (18.0 vs. 20.0 mm; p < 0.001) and higher tricuspid regurgitation velocity (p < 0.001). Markers of congestion showed a gradient, with higher NT-proBNP (3,072.5 vs. 1,197.0 pg/mL; p < 0.001), increased extracellular water (129% vs. 101%; p < 0.001), and lower phase angle (4.9 vs. 5.5; p < 0.001). In-hospital mortality was highest in the mixed severe phenotype [11.2% vs. 3.0% and 1.7%; p = 0.039; odds ratio (OR) 5.67]. B-lines correlated with tricuspid regurgitation velocity, E/e’, and extracellular water (all r ≥ 0.50).
Conclusions:
Ultrasound-derived congestion phenotyping in HFpEF identifies distinct profiles associated with atrial and ventricular remodeling and worse in-hospital outcomes. Future studies are required to determine whether phenotype-guided decongestive strategies can improve outcomes beyond risk stratification.
Aim:
To evaluate ultrasound-derived congestion phenotypes in acute decompensated heart failure with preserved ejection fraction (HFpEF) and their association with cardiac remodeling and in-hospital outcomes.
Methods:
This prospective study included 235 patients (median age 77.0 years, 75.3% women) with acute decompensated HFpEF. Within 2 hours of admission, all patients underwent echocardiography, lung ultrasound (B-lines), venous excess ultrasound score (VExUS) assessment, and bioimpedance analysis. Patients were classified into three phenotypes based on pulmonary (B-lines > 3) and systemic venous congestion (VExUS): low-low (no significant pulmonary or systemic congestion), pulmonary-dominant, and mixed severe. The primary endpoint was in-hospital mortality.
Results:
Moderate-to-severe venous congestion (VExUS grade 2–3) was present in 60.8% of patients. The mixed severe phenotype predominated (60.9%) and was associated with higher body mass index (BMI) and waist (p < 0.001). This group demonstrated more advanced cardiac dysfunction, including higher E/e’ (14.9 vs. 11.9; p < 0.001), greater left atrial remodeling (left atrial volume index 45.0 vs. 39.0 mL/m2; p < 0.001), and increased left ventricular mass index (p = 0.010). Right ventricular (RV) involvement was more pronounced, with lower TAPSE (18.0 vs. 20.0 mm; p < 0.001) and higher tricuspid regurgitation velocity (p < 0.001). Markers of congestion showed a gradient, with higher NT-proBNP (3,072.5 vs. 1,197.0 pg/mL; p < 0.001), increased extracellular water (129% vs. 101%; p < 0.001), and lower phase angle (4.9 vs. 5.5; p < 0.001). In-hospital mortality was highest in the mixed severe phenotype [11.2% vs. 3.0% and 1.7%; p = 0.039; odds ratio (OR) 5.67]. B-lines correlated with tricuspid regurgitation velocity, E/e’, and extracellular water (all r ≥ 0.50).
Conclusions:
Ultrasound-derived congestion phenotyping in HFpEF identifies distinct profiles associated with atrial and ventricular remodeling and worse in-hospital outcomes. Future studies are required to determine whether phenotype-guided decongestive strategies can improve outcomes beyond risk stratification.
DOI: https://doi.org/10.37349/emed.2026.1001410
This article belongs to the special issue Assessment of Atrial and Ventricular Volumes and Functional Properties: Novel Insights
Obesity during the menopausal transition accelerates vascular aging through systemic inflammation, insulin resistance, and estrogen loss. These pathological processes impair endothelial function and arterial compliance, thereby increasing cardiovascular risk while simultaneously disrupting cerebral circulation, neurovascular regulation, and neuroendocrine stability that contribute to cognitive decline and psychological vulnerability. Regular exercise has emerged as an important non-pharmacological strategy to counteract these multidimensional impairments. Particular attention has been given to the modifying role of hormonal status and the differential adaptations observed between premenopausal and postmenopausal states. Evidence indicates that aerobic and multimodal programs enhance nitric oxide bioavailability, vascular elasticity, and cerebral perfusion, whereas resistance training contributes to musculoskeletal strength, metabolic regulation, and psychological resilience. Novel approaches such as interval-based or hypoxic exercise may provide additional benefits for postmenopausal women but require individualized supervision. Importantly, exercise-induced vascular improvements extend beyond cardiovascular protection, restoring cerebral blood flow, promoting hippocampal plasticity, and stabilizing hypothalamic–pituitary–adrenal axis function. These adaptations mediate enhancements in memory, executive performance, mood regulation, and stress resilience. This review synthesizes current findings across aerobic training, resistance training, combined training, high-intensity interval training, and hypoxic conditioning, and proposes an integrative vascular–cognitive–mental health framework that unifies these domains into a coherent model, with vascular function as a central mechanistic pathway linking exercise to cognitive and psychological outcomes, while underscoring the need for precision exercise prescriptions tailored to hormonal status, vascular risk, and functional capacity in obese women.
Obesity during the menopausal transition accelerates vascular aging through systemic inflammation, insulin resistance, and estrogen loss. These pathological processes impair endothelial function and arterial compliance, thereby increasing cardiovascular risk while simultaneously disrupting cerebral circulation, neurovascular regulation, and neuroendocrine stability that contribute to cognitive decline and psychological vulnerability. Regular exercise has emerged as an important non-pharmacological strategy to counteract these multidimensional impairments. Particular attention has been given to the modifying role of hormonal status and the differential adaptations observed between premenopausal and postmenopausal states. Evidence indicates that aerobic and multimodal programs enhance nitric oxide bioavailability, vascular elasticity, and cerebral perfusion, whereas resistance training contributes to musculoskeletal strength, metabolic regulation, and psychological resilience. Novel approaches such as interval-based or hypoxic exercise may provide additional benefits for postmenopausal women but require individualized supervision. Importantly, exercise-induced vascular improvements extend beyond cardiovascular protection, restoring cerebral blood flow, promoting hippocampal plasticity, and stabilizing hypothalamic–pituitary–adrenal axis function. These adaptations mediate enhancements in memory, executive performance, mood regulation, and stress resilience. This review synthesizes current findings across aerobic training, resistance training, combined training, high-intensity interval training, and hypoxic conditioning, and proposes an integrative vascular–cognitive–mental health framework that unifies these domains into a coherent model, with vascular function as a central mechanistic pathway linking exercise to cognitive and psychological outcomes, while underscoring the need for precision exercise prescriptions tailored to hormonal status, vascular risk, and functional capacity in obese women.
DOI: https://doi.org/10.37349/emed.2026.1001409
The increasing survival rates among paediatric and adolescent cancer patients has increased attention on long-term consequences of chemotherapy, particularly male fertility. This review addresses age- and dose-dependent gonadotoxicity and drug type on reproductive potential. It further investigates the damage, including disruption of the hypothalamic-pituitary-gonadal axis and epigenetic alterations that may pose transgenerational risks. A systematic search of PubMed, Scopus, Web of Science, and Google Scholar was conducted for studies from database inception to April 2025. Inclusion criteria included paediatric and adolescent male cancer patients or adult survivors of childhood cancer and reported chemotherapy-related effects on fertility. Preclinical animal models were included to elucidate epigenetic changes. Due to heterogeneity of study designs, a narrative synthesis was performed to categorize findings into hormonal, cellular, and clinical outcomes. Chemotherapy-induced infertility is highly dependent on the developmental stage and specific regimen. Alkylating agents and platinum-based therapies were consistently associated with impaired spermatogenesis, hormonal disruption, and azoospermia or oligospermia. Chemotherapy and cranial irradiation were altered hormonal system that regulates male reproduction and persists epigenetic changes in germ cells. Fertility preservation for postpubertal males is through sperm cryopreservation, while prepubertal boys relied on experimental strategies such as testicular tissue cryopreservation and in vitro spermatogenesis. Chemotherapy induces epigenetic after-effects, including altered DNA methylation patterns that persist even after spermatogenesis recovers. Chemotherapy compromises male fertility through cytotoxic damage and potential long-term genomic instability. The findings highlight that reproductive recovery does not guarantee genomic recovery (epigenetically intact sperm). Consequently, oncofertility care must adapt a reproductive health model that prioritizes early, customized counselling and use of biomarkers to better predict and preserve fertility in young survivors. Although sperm banking remains a standard approach for postpubertal, promising experimental may expand fertility options for prepubertal boys in future.
The increasing survival rates among paediatric and adolescent cancer patients has increased attention on long-term consequences of chemotherapy, particularly male fertility. This review addresses age- and dose-dependent gonadotoxicity and drug type on reproductive potential. It further investigates the damage, including disruption of the hypothalamic-pituitary-gonadal axis and epigenetic alterations that may pose transgenerational risks. A systematic search of PubMed, Scopus, Web of Science, and Google Scholar was conducted for studies from database inception to April 2025. Inclusion criteria included paediatric and adolescent male cancer patients or adult survivors of childhood cancer and reported chemotherapy-related effects on fertility. Preclinical animal models were included to elucidate epigenetic changes. Due to heterogeneity of study designs, a narrative synthesis was performed to categorize findings into hormonal, cellular, and clinical outcomes. Chemotherapy-induced infertility is highly dependent on the developmental stage and specific regimen. Alkylating agents and platinum-based therapies were consistently associated with impaired spermatogenesis, hormonal disruption, and azoospermia or oligospermia. Chemotherapy and cranial irradiation were altered hormonal system that regulates male reproduction and persists epigenetic changes in germ cells. Fertility preservation for postpubertal males is through sperm cryopreservation, while prepubertal boys relied on experimental strategies such as testicular tissue cryopreservation and in vitro spermatogenesis. Chemotherapy induces epigenetic after-effects, including altered DNA methylation patterns that persist even after spermatogenesis recovers. Chemotherapy compromises male fertility through cytotoxic damage and potential long-term genomic instability. The findings highlight that reproductive recovery does not guarantee genomic recovery (epigenetically intact sperm). Consequently, oncofertility care must adapt a reproductive health model that prioritizes early, customized counselling and use of biomarkers to better predict and preserve fertility in young survivors. Although sperm banking remains a standard approach for postpubertal, promising experimental may expand fertility options for prepubertal boys in future.
DOI: https://doi.org/10.37349/emed.2026.1001408
Aim:
Adult-onset Still’s disease (AOSD) is a rare systemic inflammatory disorder marked by fever, rash, joint pain, and hyperferritinemia. While immune dysregulation is implicated in AOSD, the exact causal mechanisms remain unclear. This study aimed to investigate the genetic causal relationship between 731 immune cell phenotypes and AOSD, and to identify protective or risk-associated profiles.
Methods:
Using a two-sample Mendelian randomization (TSMR) approach, we applied inverse variance weighted (IVW) as the primary method, supplemented by MR-Egger, weighted median, simple mode, and weighted mode methods for robustness. Genetic instrumental variables for immune traits were sourced from recent genome-wide association studies (GWAS), and AOSD genetic predispositions were derived from the finn-b-STILL_ADULT cohort, comprising 201,947 individuals of European ancestry (3,403 AOSD cases and 198,544 controls).
Results:
We identified 49 immune cell-related traits showing nominally significant associations with AOSD (all adjusted P > 0.05 after FDR correction). Among these, 34 traits showed nominally protective trends, while 15 showed nominally risk-associated trends. Reciprocally, AOSD showed nominally suggestive effects on 40 immune cell traits, with 25 exhibiting a trend toward decreased levels and 15 toward increased levels. Additionally, we conducted multiple sensitivity analyses to explore potential heterogeneity and pleiotropy, though the primary findings did not survive FDR correction.
Conclusions:
These nominally significant associations between immune cell traits and AOSD, though not surviving FDR correction, may offer hypothesis-generating insights for future therapeutic research. The observed directional trends—with certain traits showing nominally protective or risk-associated patterns—suggest potential avenues for further exploration in the development of targeted treatment approaches for AOSD.
Aim:
Adult-onset Still’s disease (AOSD) is a rare systemic inflammatory disorder marked by fever, rash, joint pain, and hyperferritinemia. While immune dysregulation is implicated in AOSD, the exact causal mechanisms remain unclear. This study aimed to investigate the genetic causal relationship between 731 immune cell phenotypes and AOSD, and to identify protective or risk-associated profiles.
Methods:
Using a two-sample Mendelian randomization (TSMR) approach, we applied inverse variance weighted (IVW) as the primary method, supplemented by MR-Egger, weighted median, simple mode, and weighted mode methods for robustness. Genetic instrumental variables for immune traits were sourced from recent genome-wide association studies (GWAS), and AOSD genetic predispositions were derived from the finn-b-STILL_ADULT cohort, comprising 201,947 individuals of European ancestry (3,403 AOSD cases and 198,544 controls).
Results:
We identified 49 immune cell-related traits showing nominally significant associations with AOSD (all adjusted P > 0.05 after FDR correction). Among these, 34 traits showed nominally protective trends, while 15 showed nominally risk-associated trends. Reciprocally, AOSD showed nominally suggestive effects on 40 immune cell traits, with 25 exhibiting a trend toward decreased levels and 15 toward increased levels. Additionally, we conducted multiple sensitivity analyses to explore potential heterogeneity and pleiotropy, though the primary findings did not survive FDR correction.
Conclusions:
These nominally significant associations between immune cell traits and AOSD, though not surviving FDR correction, may offer hypothesis-generating insights for future therapeutic research. The observed directional trends—with certain traits showing nominally protective or risk-associated patterns—suggest potential avenues for further exploration in the development of targeted treatment approaches for AOSD.
DOI: https://doi.org/10.37349/emed.2026.1001406
Tricuspid valve endocarditis has potential associations with various conditions, but it is commonly related to intravenous drug abuse. Often, its eradication can become very challenging due to high post-operative mortality and high rate of recurrence due to persistence of drug abuse habits. The bidirectional Glenn shunt (BGS), typically employed in congenital heart surgery, combined with tricuspid valvectomy, has occasionally been used for recurrent endocarditis. Herein, we present a 31-year-old woman with drug addiction scheduled for her fourth reintervention due to the early degeneration and infection of a previous pulmonary homograft used for recurring tricuspid valve endocarditis. The final surgical strategy was valvectomy and BGS, aimed at eliminating all potential sources of infection and providing more time for the patient to overcome drug addiction, enabling further treatment if necessary.
Tricuspid valve endocarditis has potential associations with various conditions, but it is commonly related to intravenous drug abuse. Often, its eradication can become very challenging due to high post-operative mortality and high rate of recurrence due to persistence of drug abuse habits. The bidirectional Glenn shunt (BGS), typically employed in congenital heart surgery, combined with tricuspid valvectomy, has occasionally been used for recurrent endocarditis. Herein, we present a 31-year-old woman with drug addiction scheduled for her fourth reintervention due to the early degeneration and infection of a previous pulmonary homograft used for recurring tricuspid valve endocarditis. The final surgical strategy was valvectomy and BGS, aimed at eliminating all potential sources of infection and providing more time for the patient to overcome drug addiction, enabling further treatment if necessary.
DOI: https://doi.org/10.37349/emed.2026.1001407
The recent improvements of the ultrasounds technology and the probes have led the dental community to start to apply this technology at macrovascular and microvascular level. This scoping review aims to investigate the diagnostic and research applications of ultrasonography in periodontics. A comprehensive literature search was conducted in PubMed, Scopus, and Web of Science, to identify relevant studies in periodontology: The search strategy included the following terms: “ultrasonography”, “echography”, “ultrasound”, “dentistry”. The review was conducted in accordance with the PRISMA-ScR guidelines. In addition, a manual search was conducted through the following journals from the last 10 years: Journal of Clinical Periodontology, the Journal of Dental Research and Oral Surgery, and Oral Medicine, Oral Pathology and Oral Radiology. Ten studies were included, covering different applications of ultrasonography in periodontology. Ultrasonography was employed in peri-implant and periodontal diagnosis, assessment of soft tissue thickness and vascularization, palatal wound and bone healing. This review highlights the effectiveness of ultrasonography in diagnosis and surgical evaluation. Further research, standardized protocols, and randomized clinical trials are needed, expanding the investigation to more fields relevant to the maxillofacial district.
The recent improvements of the ultrasounds technology and the probes have led the dental community to start to apply this technology at macrovascular and microvascular level. This scoping review aims to investigate the diagnostic and research applications of ultrasonography in periodontics. A comprehensive literature search was conducted in PubMed, Scopus, and Web of Science, to identify relevant studies in periodontology: The search strategy included the following terms: “ultrasonography”, “echography”, “ultrasound”, “dentistry”. The review was conducted in accordance with the PRISMA-ScR guidelines. In addition, a manual search was conducted through the following journals from the last 10 years: Journal of Clinical Periodontology, the Journal of Dental Research and Oral Surgery, and Oral Medicine, Oral Pathology and Oral Radiology. Ten studies were included, covering different applications of ultrasonography in periodontology. Ultrasonography was employed in peri-implant and periodontal diagnosis, assessment of soft tissue thickness and vascularization, palatal wound and bone healing. This review highlights the effectiveness of ultrasonography in diagnosis and surgical evaluation. Further research, standardized protocols, and randomized clinical trials are needed, expanding the investigation to more fields relevant to the maxillofacial district.
DOI: https://doi.org/10.37349/emed.2026.1001405
Although emotions play a fundamental role in modulating pain perception, their objective assessment in clinical contexts remains challenging. Recent advances in artificial intelligence (AI) have opened new opportunities to measure emotional states through facial expression analysis, physiological signal modeling, natural language processing (NLP), and multimodal data integration. In affective computing, the field that focuses on technologies designed to recognize, interpret, process, and simulate human emotions, facial expression-based emotion recognition has progressed from traditional machine learning methods to advanced deep learning approaches, including convolutional neural networks (CNNs), attention-based hybrid models, and transformer architectures. Similarly, recurrent neural networks and self-supervised learning methods have been implemented for developing models from physiological signals such as electrocardiography, photoplethysmography, galvanic skin response, and related biosignals. Additionally, NLP systems can extract affective information from naturalistic text, using both lexicon-based and transformer-based models. Finally, multimodal fusion and alignment techniques allow the integration of heterogeneous data streams, providing richer and more ecologically valid emotion representations. Collectively, these strategies offer powerful tools for advancing automatic pain assessment (APA) in cancer care, with the potential to support personalized, emotion-aware therapeutic approaches. However, from an AI perspective, several open challenges remain, including multimodal representation learning under weak supervision, robustness to missing or degraded modalities, limited explainability of affective inference models, lack of standardized benchmarking protocols, and the presence of bias and domain shift in emotion datasets. Given the inherently subjective, context-dependent, and culturally mediated features of the emotional experience, further research is needed to address these technical limitations, integrating technological advances with the intrinsic complexity of emotion interpretation.
Although emotions play a fundamental role in modulating pain perception, their objective assessment in clinical contexts remains challenging. Recent advances in artificial intelligence (AI) have opened new opportunities to measure emotional states through facial expression analysis, physiological signal modeling, natural language processing (NLP), and multimodal data integration. In affective computing, the field that focuses on technologies designed to recognize, interpret, process, and simulate human emotions, facial expression-based emotion recognition has progressed from traditional machine learning methods to advanced deep learning approaches, including convolutional neural networks (CNNs), attention-based hybrid models, and transformer architectures. Similarly, recurrent neural networks and self-supervised learning methods have been implemented for developing models from physiological signals such as electrocardiography, photoplethysmography, galvanic skin response, and related biosignals. Additionally, NLP systems can extract affective information from naturalistic text, using both lexicon-based and transformer-based models. Finally, multimodal fusion and alignment techniques allow the integration of heterogeneous data streams, providing richer and more ecologically valid emotion representations. Collectively, these strategies offer powerful tools for advancing automatic pain assessment (APA) in cancer care, with the potential to support personalized, emotion-aware therapeutic approaches. However, from an AI perspective, several open challenges remain, including multimodal representation learning under weak supervision, robustness to missing or degraded modalities, limited explainability of affective inference models, lack of standardized benchmarking protocols, and the presence of bias and domain shift in emotion datasets. Given the inherently subjective, context-dependent, and culturally mediated features of the emotional experience, further research is needed to address these technical limitations, integrating technological advances with the intrinsic complexity of emotion interpretation.
DOI: https://doi.org/10.37349/emed.2026.1001404
This article belongs to the special issue Innovative Approaches to Chronic Pain Management: from Multidisciplinary Strategies to Artificial Intelligence Perspectives
Aim:
Myxofibrosarcoma (MFS) is characterized by high local recurrence and complex microenvironmental interactions. Although three-dimensional (3D) culture systems better mimic in vivo tumor architecture than conventional two-dimensional (2D) monolayer cultures, the global proteomic consequences of dimensionality in MFS remain incompletely defined.
Methods:
We performed quantitative mass spectrometry-based proteomic profiling of eight independently established patient-derived MFS cell lines cultured under 2D monolayer and 3D spheroid conditions. Differential protein expression and pathway enrichment analyses were conducted to delineate dimensionality-driven molecular programs.
Results:
Culture dimensionality emerged as the principal determinant of proteomic variation across all cell lines. Compared with monolayers, 3D spheroids exhibited significant enrichment of hypoxia response, autophagy-related processes, extracellular matrix organization, and PI3K-Akt signaling pathways. In contrast, 2D cultures preferentially upregulated DNA replication, RNA processing, and cell-cycle-associated pathways. These findings indicate that 3D architecture alone is sufficient to induce coordinated stress-adaptive and survival-oriented proteomic reprogramming in MFS cells.
Conclusions:
This study provides a comprehensive proteomic atlas defining dimensionality-dependent molecular states in MFS. While functional validation was beyond the scope of this work, the pathway rewiring identified here establishes a mechanistic framework for future hypothesis-driven investigations targeting autophagy- and PI3K-Akt-associated vulnerabilities in 3D MFS models.
Aim:
Myxofibrosarcoma (MFS) is characterized by high local recurrence and complex microenvironmental interactions. Although three-dimensional (3D) culture systems better mimic in vivo tumor architecture than conventional two-dimensional (2D) monolayer cultures, the global proteomic consequences of dimensionality in MFS remain incompletely defined.
Methods:
We performed quantitative mass spectrometry-based proteomic profiling of eight independently established patient-derived MFS cell lines cultured under 2D monolayer and 3D spheroid conditions. Differential protein expression and pathway enrichment analyses were conducted to delineate dimensionality-driven molecular programs.
Results:
Culture dimensionality emerged as the principal determinant of proteomic variation across all cell lines. Compared with monolayers, 3D spheroids exhibited significant enrichment of hypoxia response, autophagy-related processes, extracellular matrix organization, and PI3K-Akt signaling pathways. In contrast, 2D cultures preferentially upregulated DNA replication, RNA processing, and cell-cycle-associated pathways. These findings indicate that 3D architecture alone is sufficient to induce coordinated stress-adaptive and survival-oriented proteomic reprogramming in MFS cells.
Conclusions:
This study provides a comprehensive proteomic atlas defining dimensionality-dependent molecular states in MFS. While functional validation was beyond the scope of this work, the pathway rewiring identified here establishes a mechanistic framework for future hypothesis-driven investigations targeting autophagy- and PI3K-Akt-associated vulnerabilities in 3D MFS models.
DOI: https://doi.org/10.37349/emed.2026.1001403
Aim:
Adherence to antihypertensive medication is essential for positive outcomes among patients diagnosed with hypertension. Yet, up to 72% of individuals prescribed antihypertensives do not take medication as prescribed. Understanding mechanisms of behavior change (MoBCs) for antihypertensive adherence provides essential insight for how to change adherence behavior. This study examined the association between 4 potential MoBCs and self-reported antihypertensive adherence.
Methods:
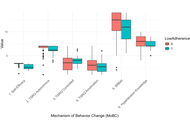
This exploratory, cross-sectional study recruited 101 patients prescribed antihypertensive medications to complete self-report questionnaires on adherence and potential mechanisms of nonadherence. Antihypertensive adherence was assessed using the Hill-Bone Compliance to High Blood Pressure Therapy Scale (HB-HBP). The 4 putative MoBCs for nonadherence included self-efficacy, self-regulation, behavioral automaticity, and hypertension knowledge. Associations between self-reported antihypertensive adherence and MoBCs were examined using independent samples t-tests and multivariate median regression with covariate adjustment for participant characteristics.
Results:
The sample had a mean age of 61.7 years (SD = 13.1 years), was 59.4% female (n = 60), 66.3% White (n = 67), and 7.9% Hispanic (n = 8). Low adherence was reported by 16.8% of the study sample. Participants who reported low adherence to antihypertensive medications had lower scores on the self-efficacy questionnaire (p < 0.001) and hypertension knowledge (p = 0.045). Self-efficacy and hypertension knowledge remained significantly associated with self-reported adherence in multivariate regression with covariate adjustment.
Conclusions:
The current study supports the hypothesis that self-efficacy for adherence and additionally hypertension knowledge are the MoBCs most strongly associated with self-reported adherence behavior. Behavioral interventions to improve medication adherence should consider focusing on self-efficacy and hypertension knowledge as potentially important target MoBCs. The authors recommend that future research should consider tailored intervention approaches that target specific mechanisms of adherence and specific self-reported reasons for nonadherence.
Aim:
Adherence to antihypertensive medication is essential for positive outcomes among patients diagnosed with hypertension. Yet, up to 72% of individuals prescribed antihypertensives do not take medication as prescribed. Understanding mechanisms of behavior change (MoBCs) for antihypertensive adherence provides essential insight for how to change adherence behavior. This study examined the association between 4 potential MoBCs and self-reported antihypertensive adherence.
Methods:
This exploratory, cross-sectional study recruited 101 patients prescribed antihypertensive medications to complete self-report questionnaires on adherence and potential mechanisms of nonadherence. Antihypertensive adherence was assessed using the Hill-Bone Compliance to High Blood Pressure Therapy Scale (HB-HBP). The 4 putative MoBCs for nonadherence included self-efficacy, self-regulation, behavioral automaticity, and hypertension knowledge. Associations between self-reported antihypertensive adherence and MoBCs were examined using independent samples t-tests and multivariate median regression with covariate adjustment for participant characteristics.
Results:
The sample had a mean age of 61.7 years (SD = 13.1 years), was 59.4% female (n = 60), 66.3% White (n = 67), and 7.9% Hispanic (n = 8). Low adherence was reported by 16.8% of the study sample. Participants who reported low adherence to antihypertensive medications had lower scores on the self-efficacy questionnaire (p < 0.001) and hypertension knowledge (p = 0.045). Self-efficacy and hypertension knowledge remained significantly associated with self-reported adherence in multivariate regression with covariate adjustment.
Conclusions:
The current study supports the hypothesis that self-efficacy for adherence and additionally hypertension knowledge are the MoBCs most strongly associated with self-reported adherence behavior. Behavioral interventions to improve medication adherence should consider focusing on self-efficacy and hypertension knowledge as potentially important target MoBCs. The authors recommend that future research should consider tailored intervention approaches that target specific mechanisms of adherence and specific self-reported reasons for nonadherence.
DOI: https://doi.org/10.37349/emed.2026.1001402
This article belongs to the special issue Drug Adherence in Hypertension
Hepatocellular carcinoma (HCC) is an aggressive primary liver malignancy with a high propensity for extrahepatic spread, most commonly to the lungs, lymph nodes, and bones. Metastases to atypical sites like the orbital and oral cavity are uncommon and often underrecognized. We report the case of a 74-year-old male with hepatitis C-related cirrhosis who was diagnosed with HCC and initially treated with locoregional therapies. Disease progression was marked by the development of biopsy-confirmed pulmonary metastases, followed by treatment with durvalumab plus tremelimumab immunotherapy and external beam radiation. Despite therapy, further progression occurred with mediastinal lymphadenopathy. The patient subsequently developed visual disturbances, and ophthalmologic evaluation identified a solitary choroidal mass consistent with metastatic HCC. Around the same time, he presented with recurrent oral bleeding, and a biopsy of a maxillary gingival lesion confirmed metastatic HCC. This case highlights the aggressive nature of advanced HCC and its potential for unusual metastatic spread. To our knowledge, this is among the few reported cases of HCC with orbital and oral metastases. Awareness of atypical metastatic presentations and a multidisciplinary approach are essential for timely diagnosis and optimal management.
Hepatocellular carcinoma (HCC) is an aggressive primary liver malignancy with a high propensity for extrahepatic spread, most commonly to the lungs, lymph nodes, and bones. Metastases to atypical sites like the orbital and oral cavity are uncommon and often underrecognized. We report the case of a 74-year-old male with hepatitis C-related cirrhosis who was diagnosed with HCC and initially treated with locoregional therapies. Disease progression was marked by the development of biopsy-confirmed pulmonary metastases, followed by treatment with durvalumab plus tremelimumab immunotherapy and external beam radiation. Despite therapy, further progression occurred with mediastinal lymphadenopathy. The patient subsequently developed visual disturbances, and ophthalmologic evaluation identified a solitary choroidal mass consistent with metastatic HCC. Around the same time, he presented with recurrent oral bleeding, and a biopsy of a maxillary gingival lesion confirmed metastatic HCC. This case highlights the aggressive nature of advanced HCC and its potential for unusual metastatic spread. To our knowledge, this is among the few reported cases of HCC with orbital and oral metastases. Awareness of atypical metastatic presentations and a multidisciplinary approach are essential for timely diagnosis and optimal management.
DOI: https://doi.org/10.37349/emed.2026.1001401
Background:
Sickle cell disease (SCD) is a group of heritable conditions with significant morbidity, burden of disease management and healthcare delivery issues. Medical mistrust (MM) is a psychological outcome of healthcare delivery issues. The purpose of this review was to assess the concept of MM in the literature on SCD, summarize the findings and gaps, and was guided by three questions: 1) How has MM been measured and/or described in patients with SCD? 2) What factors have been described in the literature that predispose patients with SCD to develop MM? 3) What consequences or outcomes have been described because of MM in patients with SCD?
Methods:
The methodological framework of Arksey and O’Malley was used to review articles from PubMed, Scopus, Web of Science, CINAHL, PsycInfo, and EMBASE. Inclusion criteria were quantitative, qualitative, and mixed methods peer-reviewed studies published in English between 1994 and 2025; articles focused on patients with SCD and those that described concepts found in the existing MM instruments.
Results:
Forty-two studies were included; 26 were strictly qualitative, 11 were mixed methods, and 5 were strictly quantitative. No study used an existing MM measure; yet concepts from MM measures were described: group disparities and suspicion. Negative healthcare staff communication, poor pain control, transition of care, and lack of provider transparency predisposed patients toward MM. Outcomes of MM included avoidance of care, nonadherence, psychological distress, and maladaptive coping.
Discussion:
This review highlights the predictors and outcomes of MM in patients with SCD and identifies the notable gaps in the state of the SCD MM literature. More studies are needed to assess the development and consequences of MM in patients with SCD. The findings highlight the experiences of patients with SCD and offer researchers insights into possible interventions to decrease MM and improve outcomes.
Background:
Sickle cell disease (SCD) is a group of heritable conditions with significant morbidity, burden of disease management and healthcare delivery issues. Medical mistrust (MM) is a psychological outcome of healthcare delivery issues. The purpose of this review was to assess the concept of MM in the literature on SCD, summarize the findings and gaps, and was guided by three questions: 1) How has MM been measured and/or described in patients with SCD? 2) What factors have been described in the literature that predispose patients with SCD to develop MM? 3) What consequences or outcomes have been described because of MM in patients with SCD?
Methods:
The methodological framework of Arksey and O’Malley was used to review articles from PubMed, Scopus, Web of Science, CINAHL, PsycInfo, and EMBASE. Inclusion criteria were quantitative, qualitative, and mixed methods peer-reviewed studies published in English between 1994 and 2025; articles focused on patients with SCD and those that described concepts found in the existing MM instruments.
Results:
Forty-two studies were included; 26 were strictly qualitative, 11 were mixed methods, and 5 were strictly quantitative. No study used an existing MM measure; yet concepts from MM measures were described: group disparities and suspicion. Negative healthcare staff communication, poor pain control, transition of care, and lack of provider transparency predisposed patients toward MM. Outcomes of MM included avoidance of care, nonadherence, psychological distress, and maladaptive coping.
Discussion:
This review highlights the predictors and outcomes of MM in patients with SCD and identifies the notable gaps in the state of the SCD MM literature. More studies are needed to assess the development and consequences of MM in patients with SCD. The findings highlight the experiences of patients with SCD and offer researchers insights into possible interventions to decrease MM and improve outcomes.
DOI: https://doi.org/10.37349/emed.2026.1001400
The involvement of the Internet of Things (IoT) technology and artificial intelligence (AI) in the matter of maternal healthcare has allowed monitoring pregnant women in real-time and predicting poor pregnancy outcomes, including stillbirth and premature birth. Nevertheless, to diminish the risks of devices, the introduction of such technologies has to be accompanied by harsh safety monitoring programs. Materiovigilance, as the systematic sensing and monitoring of adverse events associated with medical instruments, is also crucial to patient safety in high-risk obstetric environments. Wearable sensors, e.g., fetal Dopplers, smart fabrics, and adhesive patches, have enhanced the prediction of stillbirth by offering continuous acquisition of physiological data but presents a hazard of ill effects if not controlled adequately. The AI introduction into the sphere of Materiovigilance enhances regulatory conformity, real-time decision-making, and raises the possibility of risk identification. Despite the massive potential, issues such as inaccurate data, poor infrastructure, and underreporting persist, particularly in low- and middle-income countries. In such circumstances, the Materiovigilance Programme of India is another staged effort to enhance the device safety supervision and reporting systems. Engagement of different stakeholders such as clinicians, engineers, regulatory agencies, and technology developers provides an opportunity to secure the safety and efficacy of AI-equipped medical devices. Enhancement of Materiovigilance systems is required to preserve proper maternal-fetal health and sustain clinics in digital obstetrics, as any error in maternal-fetal monitoring may lead to preventable death.
The involvement of the Internet of Things (IoT) technology and artificial intelligence (AI) in the matter of maternal healthcare has allowed monitoring pregnant women in real-time and predicting poor pregnancy outcomes, including stillbirth and premature birth. Nevertheless, to diminish the risks of devices, the introduction of such technologies has to be accompanied by harsh safety monitoring programs. Materiovigilance, as the systematic sensing and monitoring of adverse events associated with medical instruments, is also crucial to patient safety in high-risk obstetric environments. Wearable sensors, e.g., fetal Dopplers, smart fabrics, and adhesive patches, have enhanced the prediction of stillbirth by offering continuous acquisition of physiological data but presents a hazard of ill effects if not controlled adequately. The AI introduction into the sphere of Materiovigilance enhances regulatory conformity, real-time decision-making, and raises the possibility of risk identification. Despite the massive potential, issues such as inaccurate data, poor infrastructure, and underreporting persist, particularly in low- and middle-income countries. In such circumstances, the Materiovigilance Programme of India is another staged effort to enhance the device safety supervision and reporting systems. Engagement of different stakeholders such as clinicians, engineers, regulatory agencies, and technology developers provides an opportunity to secure the safety and efficacy of AI-equipped medical devices. Enhancement of Materiovigilance systems is required to preserve proper maternal-fetal health and sustain clinics in digital obstetrics, as any error in maternal-fetal monitoring may lead to preventable death.
DOI: https://doi.org/10.37349/emed.2026.1001399
Idiopathic pulmonary fibrosis (IPF) is a progressive, fatal interstitial lung disease of undefined etiology. In recent years, its global incidence has shown an upward trend, with a median survival of approximately 3–5 years after diagnosis. Currently, clinical treatment outcomes for this disease remain limited. Approved therapeutic agents are nintedanib, pirfenidone, and nerandomilast, all of which are predominantly administered orally. The oral route renders drugs susceptible to degradation in the gastrointestinal tract, leading to reduced drug bioavailability and limited therapeutic efficacy. In this work, we believe that nanodelivery systems (NDSs) represent a promising approach to address the limitations of traditional therapies. Most importantly, we emphasized that inhalation NDSs should be prioritized to enhance the accumulation efficiency of targeted drugs at pulmonary lesion sites. Collectively, this study aims to provide insights into the developmental prospects of NDSs for IPF, paving the way for more efficient and personalized therapeutic approaches to enhance treatment efficacy while minimizing side effects.
Idiopathic pulmonary fibrosis (IPF) is a progressive, fatal interstitial lung disease of undefined etiology. In recent years, its global incidence has shown an upward trend, with a median survival of approximately 3–5 years after diagnosis. Currently, clinical treatment outcomes for this disease remain limited. Approved therapeutic agents are nintedanib, pirfenidone, and nerandomilast, all of which are predominantly administered orally. The oral route renders drugs susceptible to degradation in the gastrointestinal tract, leading to reduced drug bioavailability and limited therapeutic efficacy. In this work, we believe that nanodelivery systems (NDSs) represent a promising approach to address the limitations of traditional therapies. Most importantly, we emphasized that inhalation NDSs should be prioritized to enhance the accumulation efficiency of targeted drugs at pulmonary lesion sites. Collectively, this study aims to provide insights into the developmental prospects of NDSs for IPF, paving the way for more efficient and personalized therapeutic approaches to enhance treatment efficacy while minimizing side effects.
DOI: https://doi.org/10.37349/emed.2026.1001397
Aim:
Polypharmacy is increasingly prevalent among older adults and has been suggested as a potential risk factor for adverse health outcomes, including cognitive impairment and functional decline. Therefore, this study aimed to investigate the associations of polypharmacy with cognitive impairment and functional status among community-dwelling older adults using nationally representative data from the 2023 Korean Elderly Survey.
Methods:
A cross-sectional analysis was conducted using data from 9,898 community-dwelling older adults without a diagnosis of dementia. Polypharmacy was defined as the concurrent use of five or more physician-prescribed medications. Cognitive function was assessed using the Korean version of the Mini-Mental State Examination (K-MMSE), with cognitive impairment defined as a score ≤ 23. Functional status was evaluated using the Korean Activities of Daily Living (K-ADL) and Korean Instrumental Activities of Daily Living (K-IADL). Logistic regression was used to estimate odds ratios and 95% confidence intervals (CIs) for cognitive impairment, while multiple linear regression analyses examined associations with functional status. Models were sequentially adjusted for sociodemographic characteristics, health behaviors, and the number of chronic diseases.
Results:
Polypharmacy was associated with increased odds of cognitive impairment in the crude model (OR = 1.70, 95% CI: 1.40–2.05); however, this association was attenuated and became non-significant after adjustment for sociodemographic and health-related factors. In contrast, polypharmacy remained independently associated with poorer functional status in fully adjusted models, showing higher K-ADL scores (B = 0.14, p = 0.007) and K-IADL scores (B = 0.43, p < 0.001).
Conclusions:
Polypharmacy was independently associated with functional impairment but not with cognitive impairment after comprehensive adjustment, suggesting that functional decline may represent a more sensitive and immediate consequence of complex medication use in older adults. These findings underscore the need for comprehensive geriatric assessment approaches that integrate medication review with functional evaluation.
Aim:
Polypharmacy is increasingly prevalent among older adults and has been suggested as a potential risk factor for adverse health outcomes, including cognitive impairment and functional decline. Therefore, this study aimed to investigate the associations of polypharmacy with cognitive impairment and functional status among community-dwelling older adults using nationally representative data from the 2023 Korean Elderly Survey.
Methods:
A cross-sectional analysis was conducted using data from 9,898 community-dwelling older adults without a diagnosis of dementia. Polypharmacy was defined as the concurrent use of five or more physician-prescribed medications. Cognitive function was assessed using the Korean version of the Mini-Mental State Examination (K-MMSE), with cognitive impairment defined as a score ≤ 23. Functional status was evaluated using the Korean Activities of Daily Living (K-ADL) and Korean Instrumental Activities of Daily Living (K-IADL). Logistic regression was used to estimate odds ratios and 95% confidence intervals (CIs) for cognitive impairment, while multiple linear regression analyses examined associations with functional status. Models were sequentially adjusted for sociodemographic characteristics, health behaviors, and the number of chronic diseases.
Results:
Polypharmacy was associated with increased odds of cognitive impairment in the crude model (OR = 1.70, 95% CI: 1.40–2.05); however, this association was attenuated and became non-significant after adjustment for sociodemographic and health-related factors. In contrast, polypharmacy remained independently associated with poorer functional status in fully adjusted models, showing higher K-ADL scores (B = 0.14, p = 0.007) and K-IADL scores (B = 0.43, p < 0.001).
Conclusions:
Polypharmacy was independently associated with functional impairment but not with cognitive impairment after comprehensive adjustment, suggesting that functional decline may represent a more sensitive and immediate consequence of complex medication use in older adults. These findings underscore the need for comprehensive geriatric assessment approaches that integrate medication review with functional evaluation.
DOI: https://doi.org/10.37349/emed.2026.1001398
Background:
Obstructive sleep apnea (OSA) is a syndrome characterized by episodes of complete cessation of breathing (apnea) or inadequate breathing (hypopnea) during sleep.
Methods:
A systematic search of PubMed, Cochrane Library, Embase, Scopus, Web of Science, and Lilacs databases was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We identified 1,532 records; after screening, 9 randomized controlled trials (RCTs), published between 2009 and 2020, met the inclusion criteria. These studies included 698 participants aged 5–75 years.
Results:
Nine randomized trials (n = 698; 2009–2020) showed that myofunctional therapy (MFT), alone or as an adjunct, for example, continuous positive airway pressure (CPAP) and nasal washing, reduced apnea-hypopnea index (AHI) versus control in adults and children. Snoring intensity improved in trials that measured it; several studies reported gains in oxygen saturation and mouth-breathing reduction. Protocols targeted the soft palate, tongue, and facial muscles with daily home exercises.
Discussion:
MFT appears to be a promising non-invasive treatment for reducing AHI, especially in pediatric patients. Its benefits extend beyond AHI reduction, supporting orofacial function and nasal breathing. However, its clinical integration remains limited due to a lack of standardized protocols and inconsistent reporting of patient adherence. Most studies also have short follow-up periods, which makes it difficult to assess long-term efficacy. To advance evidence-based use of MFT, future research should adopt standardized outcomes, monitor adherence systematically, and include long-term follow-up.
Background:
Obstructive sleep apnea (OSA) is a syndrome characterized by episodes of complete cessation of breathing (apnea) or inadequate breathing (hypopnea) during sleep.
Methods:
A systematic search of PubMed, Cochrane Library, Embase, Scopus, Web of Science, and Lilacs databases was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We identified 1,532 records; after screening, 9 randomized controlled trials (RCTs), published between 2009 and 2020, met the inclusion criteria. These studies included 698 participants aged 5–75 years.
Results:
Nine randomized trials (n = 698; 2009–2020) showed that myofunctional therapy (MFT), alone or as an adjunct, for example, continuous positive airway pressure (CPAP) and nasal washing, reduced apnea-hypopnea index (AHI) versus control in adults and children. Snoring intensity improved in trials that measured it; several studies reported gains in oxygen saturation and mouth-breathing reduction. Protocols targeted the soft palate, tongue, and facial muscles with daily home exercises.
Discussion:
MFT appears to be a promising non-invasive treatment for reducing AHI, especially in pediatric patients. Its benefits extend beyond AHI reduction, supporting orofacial function and nasal breathing. However, its clinical integration remains limited due to a lack of standardized protocols and inconsistent reporting of patient adherence. Most studies also have short follow-up periods, which makes it difficult to assess long-term efficacy. To advance evidence-based use of MFT, future research should adopt standardized outcomes, monitor adherence systematically, and include long-term follow-up.
DOI: https://doi.org/10.37349/emed.2026.1001396
The biopsychosocial model is the prevailing framework for chronic orofacial pain (COP). While COP is a heterogeneous clinical entity involving nociceptive and neuropathic components, it is increasingly defined by its nociplastic features—a systemic, non-nociceptive state in which psychological factors significantly influence symptoms. Current research frequently suffers from the conflation of constructs. Psychosocial predictors (e.g., self-efficacy) and outcome measures (e.g., pain interference) are often conceptually inseparable. To advance beyond this, we advocate for the integration of the brain-heart axis (BHA). The BHA provides objective, quantifiable markers of autonomic nervous system (ANS) dysregulation, the physical manifestation of chronic stress rooted in large-scale brain network imbalance. The present study proposes a theoretical framework in which psychological distress is reflected in corrected QT interval (QTc) changes, while low self-efficacy is mirrored by reduced heart rate variability (HRV). This integration is supported by the neurochemical roles of N-methyl-D-aspartate (NMDA) receptors in central sensitization and dopamine D2 receptor dysfunction in the basal ganglia. The present paper delineates a framework for research and clinical implementation within advanced dental training.
The biopsychosocial model is the prevailing framework for chronic orofacial pain (COP). While COP is a heterogeneous clinical entity involving nociceptive and neuropathic components, it is increasingly defined by its nociplastic features—a systemic, non-nociceptive state in which psychological factors significantly influence symptoms. Current research frequently suffers from the conflation of constructs. Psychosocial predictors (e.g., self-efficacy) and outcome measures (e.g., pain interference) are often conceptually inseparable. To advance beyond this, we advocate for the integration of the brain-heart axis (BHA). The BHA provides objective, quantifiable markers of autonomic nervous system (ANS) dysregulation, the physical manifestation of chronic stress rooted in large-scale brain network imbalance. The present study proposes a theoretical framework in which psychological distress is reflected in corrected QT interval (QTc) changes, while low self-efficacy is mirrored by reduced heart rate variability (HRV). This integration is supported by the neurochemical roles of N-methyl-D-aspartate (NMDA) receptors in central sensitization and dopamine D2 receptor dysfunction in the basal ganglia. The present paper delineates a framework for research and clinical implementation within advanced dental training.
DOI: https://doi.org/10.37349/emed.2026.1001395
