










Aim:
Artificial intelligence may support syncope evaluation, but reliability of language models in structured syncope care remains uncertain. We evaluated diagnostic performance, safety, and within-case consistency of Generative Pre-trained Transformer-5 (GPT-5) in patients with transient loss of consciousness (T-LOC).
Methods:
This prospective cohort study included 55 patients evaluated in syncope units. GPT-5 and a syncope-expert assessed identical case information after core evaluation (CE: history-taking, physical examination, active standing test, and 12-lead electrocardiogram) and extended evaluation (EE: CE plus additional testing when indicated). An expert panel adjudicated the final diagnosis after 18 months. Outcomes were diagnostic yield, final-diagnosis inclusion rate, diagnostic precision score (DPS), cardiac diagnostic safety, and within-case consistency across five repeated GPT-5 runs.
Results:
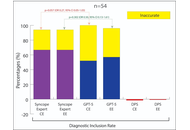
Of 55 patients, 54 had complete follow-up for performance analyses. Diagnostic yield was 94% for the syncope-expert at CE and EE, and 100% and 96% for GPT-5 at CE and EE, respectively. GPT-5 included the final diagnosis in 52% (CE) and 57% (EE) of cases, versus 67% for the syncope-expert. DPS remained negative for GPT-5 at CE (mean −0.03, SD 0.54) and EE (mean −0.01, SD 0.49). Among four final cardiac syncope cases, GPT-5 selected the final diagnosis in one case and the syncope-expert in three. First-diagnosis consistency across five GPT-5 runs was 69% after CE and 74% after EE.
Conclusions:
GPT-5 generated diagnostic outputs frequently but showed limited precision, cardiac safety concerns, and within-case variability. Its role in syncope evaluation should remain supportive within clinician-led pathways rather than autonomous.
Aim:
Artificial intelligence may support syncope evaluation, but reliability of language models in structured syncope care remains uncertain. We evaluated diagnostic performance, safety, and within-case consistency of Generative Pre-trained Transformer-5 (GPT-5) in patients with transient loss of consciousness (T-LOC).
Methods:
This prospective cohort study included 55 patients evaluated in syncope units. GPT-5 and a syncope-expert assessed identical case information after core evaluation (CE: history-taking, physical examination, active standing test, and 12-lead electrocardiogram) and extended evaluation (EE: CE plus additional testing when indicated). An expert panel adjudicated the final diagnosis after 18 months. Outcomes were diagnostic yield, final-diagnosis inclusion rate, diagnostic precision score (DPS), cardiac diagnostic safety, and within-case consistency across five repeated GPT-5 runs.
Results:
Of 55 patients, 54 had complete follow-up for performance analyses. Diagnostic yield was 94% for the syncope-expert at CE and EE, and 100% and 96% for GPT-5 at CE and EE, respectively. GPT-5 included the final diagnosis in 52% (CE) and 57% (EE) of cases, versus 67% for the syncope-expert. DPS remained negative for GPT-5 at CE (mean −0.03, SD 0.54) and EE (mean −0.01, SD 0.49). Among four final cardiac syncope cases, GPT-5 selected the final diagnosis in one case and the syncope-expert in three. First-diagnosis consistency across five GPT-5 runs was 69% after CE and 74% after EE.
Conclusions:
GPT-5 generated diagnostic outputs frequently but showed limited precision, cardiac safety concerns, and within-case variability. Its role in syncope evaluation should remain supportive within clinician-led pathways rather than autonomous.
DOI: https://doi.org/10.37349/ec.2026.1012114
Aim:
Maternal nutritional insufficiency during pregnancy is a major public health concern associated with adverse neurodevelopmental outcomes in offspring. This study investigated the effects of global maternal nutrient restriction before and/or during gestation on cognitive and behavioral performance in rat offspring and evaluated the potential for recovery following postnatal dietary normalization.
Methods:
Female Wistar rats were assigned to either a control diet (AIN-93G) or a 50% global nutrient-restricted diet. Nutrient-restricted groups received dietary restriction before pregnancy alone (RD-P) or before and throughout gestation (RD-W), followed by a standard diet after birth or weaning. Offspring were assessed at postnatal days 35–40 using the Y-maze spontaneous alternation test for working memory, the Open Field Test for locomotor activity, and the Elevated Plus Maze (EPM) for anxiety-like behavior. Data were analyzed using one-way ANOVA with Dunnett’s post hoc test (p < 0.05).
Results:
Maternal nutrient restriction did not significantly affect Y-maze spontaneous alternation performance (p > 0.05), indicating preserved working memory. However, offspring from restricted groups exhibited significantly greater time spent in EPM open arms (p < 0.001), suggesting reduced anxiety-like behavior, with the strongest effect observed in the RD-W group. Increased locomotor activity was also detected in nutrient-restricted offspring during the Open Field Test (p = 0.0118). Gestational maternal food intake showed weak negative correlations with EPM open-arm duration (r = −0.34, p = 0.06) and locomotor activity (r = −0.28, p = 0.12).
Conclusions:
Maternal global nutrient restriction induces persistent, domain-specific behavioral alterations in offspring. While postnatal dietary normalization may partially ameliorate deficits in activity-related behaviors, reduced anxiety-like behavior persists into adolescence. These findings emphasize the critical role of adequate maternal nutrition in shaping offspring neurodevelopment and behavioral health, highlighting the importance of nutritional interventions during the preconceptional and gestational periods.
Aim:
Maternal nutritional insufficiency during pregnancy is a major public health concern associated with adverse neurodevelopmental outcomes in offspring. This study investigated the effects of global maternal nutrient restriction before and/or during gestation on cognitive and behavioral performance in rat offspring and evaluated the potential for recovery following postnatal dietary normalization.
Methods:
Female Wistar rats were assigned to either a control diet (AIN-93G) or a 50% global nutrient-restricted diet. Nutrient-restricted groups received dietary restriction before pregnancy alone (RD-P) or before and throughout gestation (RD-W), followed by a standard diet after birth or weaning. Offspring were assessed at postnatal days 35–40 using the Y-maze spontaneous alternation test for working memory, the Open Field Test for locomotor activity, and the Elevated Plus Maze (EPM) for anxiety-like behavior. Data were analyzed using one-way ANOVA with Dunnett’s post hoc test (p < 0.05).
Results:
Maternal nutrient restriction did not significantly affect Y-maze spontaneous alternation performance (p > 0.05), indicating preserved working memory. However, offspring from restricted groups exhibited significantly greater time spent in EPM open arms (p < 0.001), suggesting reduced anxiety-like behavior, with the strongest effect observed in the RD-W group. Increased locomotor activity was also detected in nutrient-restricted offspring during the Open Field Test (p = 0.0118). Gestational maternal food intake showed weak negative correlations with EPM open-arm duration (r = −0.34, p = 0.06) and locomotor activity (r = −0.28, p = 0.12).
Conclusions:
Maternal global nutrient restriction induces persistent, domain-specific behavioral alterations in offspring. While postnatal dietary normalization may partially ameliorate deficits in activity-related behaviors, reduced anxiety-like behavior persists into adolescence. These findings emphasize the critical role of adequate maternal nutrition in shaping offspring neurodevelopment and behavioral health, highlighting the importance of nutritional interventions during the preconceptional and gestational periods.
DOI: https://doi.org/10.37349/eff.2026.1010177
Gastric mucosa-associated lymphoid tissue (MALT) lymphoma represents a distinctive low-grade non-Hodgkin B-cell malignancy and one of the clearest examples of infection-associated carcinogenesis. Accounting for 7–9% of all B-cell lymphomas, this disease demonstrates a unique therapeutic paradigm, as early-stage gastric MALT lymphoma achieves complete remission in approximately 60–90% of patients following Helicobacter pylori eradication alone. This response reflects the tumor’s dependence on chronic antigenic stimulation, though disease progression and treatment resistance are driven by genetic alterations, such as the t(11;18) translocation, that confer antigen-independent growth. This review synthesizes current knowledge on clinical presentation, diagnostic evaluation, immunopathogenesis, prognostic factors, and evidence-based management of gastric MALT lymphoma. This review discusses the molecular mechanisms underlying the transition from antigen-dependent to antigen-independent disease, emerging therapeutic strategies, including targeted molecular therapies and BTK inhibitors, and addresses ongoing challenges in diagnosis, treatment resistance, and surveillance. Additionally, the broader implications of gastric MALT lymphoma to better understand how chronic infection drives lymphomagenesis and how pathogen eradication can lead to regression of antigen-dependent lymphoma, with the aim of providing insights for other microbe-associated malignancies, have been discussed.
Gastric mucosa-associated lymphoid tissue (MALT) lymphoma represents a distinctive low-grade non-Hodgkin B-cell malignancy and one of the clearest examples of infection-associated carcinogenesis. Accounting for 7–9% of all B-cell lymphomas, this disease demonstrates a unique therapeutic paradigm, as early-stage gastric MALT lymphoma achieves complete remission in approximately 60–90% of patients following Helicobacter pylori eradication alone. This response reflects the tumor’s dependence on chronic antigenic stimulation, though disease progression and treatment resistance are driven by genetic alterations, such as the t(11;18) translocation, that confer antigen-independent growth. This review synthesizes current knowledge on clinical presentation, diagnostic evaluation, immunopathogenesis, prognostic factors, and evidence-based management of gastric MALT lymphoma. This review discusses the molecular mechanisms underlying the transition from antigen-dependent to antigen-independent disease, emerging therapeutic strategies, including targeted molecular therapies and BTK inhibitors, and addresses ongoing challenges in diagnosis, treatment resistance, and surveillance. Additionally, the broader implications of gastric MALT lymphoma to better understand how chronic infection drives lymphomagenesis and how pathogen eradication can lead to regression of antigen-dependent lymphoma, with the aim of providing insights for other microbe-associated malignancies, have been discussed.
DOI: https://doi.org/10.37349/edd.2026.1005128
This article belongs to the special issue Helicobacter Pylori and Infection: Genomics, Diagnosis, Pathogenesis, Antibiotic Resistance, Microbiota, Cancer, Prevention and Therapeutics
Lignin, the second most abundant natural polymer after cellulose, has emerged as a promising renewable resource for developing functional biomaterials. Due to its aromatic structure and abundance of phenolic, hydroxyl, and methoxy groups, lignin exhibits intrinsic antioxidant, UV-blocking, antimicrobial, and biocompatible properties, making it an attractive candidate for hydrogel fabrication. This review provides a comprehensive overview of lignin-based hydrogel, focusing on their structural characteristics, extraction methods, and strategies used for hydrogel preparation, including crosslinking copolymerization, graft polymerization, interpenetrating polymer networks, and controlled polymerization techniques such as ATRP and RAFT. Particular emphasis is placed on recent advances in the application of lignin-based hydrogels in biosensing and biomedical fields, including wearable strain and pressure sensors, drug delivery systems, wound healing, and tissue engineering. The multifunctional properties of lignin contribute to enhanced mechanical strength, electrical conductivity, UV protection, and controlled drug release, enabling the design of smart and sustainable hydrogel systems. Despite these advantages, several challenges remain that limit large-scale translation, including lignin heterogeneity, limited solubility, variability in hydrogel performance, and potential impurities from industrial extraction processes. Addressing this limitation through improved lignin purification, chemical modification, and standardized synthesis approaches will be essential for advancing lignin-based hydrogels towards practical biomedical and sensing applications.
Lignin, the second most abundant natural polymer after cellulose, has emerged as a promising renewable resource for developing functional biomaterials. Due to its aromatic structure and abundance of phenolic, hydroxyl, and methoxy groups, lignin exhibits intrinsic antioxidant, UV-blocking, antimicrobial, and biocompatible properties, making it an attractive candidate for hydrogel fabrication. This review provides a comprehensive overview of lignin-based hydrogel, focusing on their structural characteristics, extraction methods, and strategies used for hydrogel preparation, including crosslinking copolymerization, graft polymerization, interpenetrating polymer networks, and controlled polymerization techniques such as ATRP and RAFT. Particular emphasis is placed on recent advances in the application of lignin-based hydrogels in biosensing and biomedical fields, including wearable strain and pressure sensors, drug delivery systems, wound healing, and tissue engineering. The multifunctional properties of lignin contribute to enhanced mechanical strength, electrical conductivity, UV protection, and controlled drug release, enabling the design of smart and sustainable hydrogel systems. Despite these advantages, several challenges remain that limit large-scale translation, including lignin heterogeneity, limited solubility, variability in hydrogel performance, and potential impurities from industrial extraction processes. Addressing this limitation through improved lignin purification, chemical modification, and standardized synthesis approaches will be essential for advancing lignin-based hydrogels towards practical biomedical and sensing applications.
DOI: https://doi.org/10.37349/ebmx.2026.101369
This article belongs to the special issue Lignin-based Hydrogels for Energy, Sensing and Medical Applications
Aim:
To examine whether heart rate variability (HRV) parameters predict work-related musculoskeletal disorder (WMSD) risk profiles in Hong Kong (China) professionals and provide incremental predictive validity beyond self-reported perceived stress.
Methods:
A cross-sectional study recruited 105 full-time office workers from Hong Kong’s financial, legal, healthcare, technology sectors, and other professionals across five corporate sites between December 2025 and February 2026. Participants completed HRV assessment using a photoplethysmography device (5-minute resting protocol plus 1-minute deep breathing protocol), the Perceived Stress Scale-14 (PSS-14), a musculoskeletal pain questionnaire, postural assessment (forward head posture index, thoracic kyphosis angle), and a sedentary behavior inventory. Pearson correlation, hierarchical multiple regression, mediation analysis (PROCESS Model 4), and moderation analysis (PROCESS Model 1) examined associations between HRV parameters, perceived stress, postural variables, and pain outcomes. Statistical significance was set at p < 0.05.
Results:
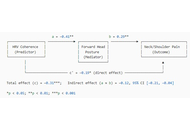
HRV parameters were significantly negatively correlated with pain intensity (r = –0.31, p < 0.001) and multi-site pain burden (r = –0.38, p < 0.001). Normalized coherence emerged as the strongest HRV predictor of pain severity (β = –0.29, p < 0.001), explaining 11.4% additional variance beyond PSS-14 alone. Forward head posture and thoracic kyphosis statistically mediated the coherence–neck/shoulder pain association. Daily sedentary hours moderated the HRV-pain association, with workers exceeding 8 hours of seated work showing the strongest autonomic–musculoskeletal risk profiles.
Conclusions:
HRV parameters, particularly normalized coherence, are associated with WMSD-relevant pain outcomes in Hong Kong office workers and capture variance not explained by self-reported stress alone. These findings support HRV as a potentially useful objective complement to existing WMSD risk-screening approaches in sedentary professional populations, although longitudinal validation is required before clinical application.
Aim:
To examine whether heart rate variability (HRV) parameters predict work-related musculoskeletal disorder (WMSD) risk profiles in Hong Kong (China) professionals and provide incremental predictive validity beyond self-reported perceived stress.
Methods:
A cross-sectional study recruited 105 full-time office workers from Hong Kong’s financial, legal, healthcare, technology sectors, and other professionals across five corporate sites between December 2025 and February 2026. Participants completed HRV assessment using a photoplethysmography device (5-minute resting protocol plus 1-minute deep breathing protocol), the Perceived Stress Scale-14 (PSS-14), a musculoskeletal pain questionnaire, postural assessment (forward head posture index, thoracic kyphosis angle), and a sedentary behavior inventory. Pearson correlation, hierarchical multiple regression, mediation analysis (PROCESS Model 4), and moderation analysis (PROCESS Model 1) examined associations between HRV parameters, perceived stress, postural variables, and pain outcomes. Statistical significance was set at p < 0.05.
Results:
HRV parameters were significantly negatively correlated with pain intensity (r = –0.31, p < 0.001) and multi-site pain burden (r = –0.38, p < 0.001). Normalized coherence emerged as the strongest HRV predictor of pain severity (β = –0.29, p < 0.001), explaining 11.4% additional variance beyond PSS-14 alone. Forward head posture and thoracic kyphosis statistically mediated the coherence–neck/shoulder pain association. Daily sedentary hours moderated the HRV-pain association, with workers exceeding 8 hours of seated work showing the strongest autonomic–musculoskeletal risk profiles.
Conclusions:
HRV parameters, particularly normalized coherence, are associated with WMSD-relevant pain outcomes in Hong Kong office workers and capture variance not explained by self-reported stress alone. These findings support HRV as a potentially useful objective complement to existing WMSD risk-screening approaches in sedentary professional populations, although longitudinal validation is required before clinical application.
DOI: https://doi.org/10.37349/emd.2026.1007128
This article belongs to the special issue Prevalence and Risk Factors of Work-related Musculoskeletal Disorders
Paediatric orthopaedics is currently witnessing a profound evolution, transitioning from traditional mechanical fixation toward a future defined by biological restoration and digital precision. The dynamic nature of the growing skeleton necessitates a “growth-aware” surgical philosophy to mitigate the lifelong burden on the child. This narrative review synthesises advancements across pivotal domains: advanced 3D imaging, virtual surgical planning, regenerative biotechnology (the “Diamond Concept”), and smart implant design, based on a rigorous analysis of 76 contemporary sources verified against Medline/PubMed databases. Innovations such as the EOS imaging system and AI-driven diagnostics have significantly reduced cumulative radiation exposure and inter-observer variability. The integration of 3D-printed patient-specific instrumentation and robotic assistance has elevated surgical fidelity in complex spinal and pelvic reconstructions. In the biological realm, the synergy of mesenchymal stem cells, BMPs, and bioactive scaffolds is providing solutions for recalcitrant defects. Furthermore, the advent of bioabsorbable magnesium alloys and internal motorized lengthening nails is effectively eliminating the need for secondary surgeries. The convergence of the “Digital Twin” paradigm with regenerative medicine offers a personalised trajectory for paediatric care. By embracing these advancements, clinicians can restore function while rigorously minimising the physical and psychological burden on the developing child.
Paediatric orthopaedics is currently witnessing a profound evolution, transitioning from traditional mechanical fixation toward a future defined by biological restoration and digital precision. The dynamic nature of the growing skeleton necessitates a “growth-aware” surgical philosophy to mitigate the lifelong burden on the child. This narrative review synthesises advancements across pivotal domains: advanced 3D imaging, virtual surgical planning, regenerative biotechnology (the “Diamond Concept”), and smart implant design, based on a rigorous analysis of 76 contemporary sources verified against Medline/PubMed databases. Innovations such as the EOS imaging system and AI-driven diagnostics have significantly reduced cumulative radiation exposure and inter-observer variability. The integration of 3D-printed patient-specific instrumentation and robotic assistance has elevated surgical fidelity in complex spinal and pelvic reconstructions. In the biological realm, the synergy of mesenchymal stem cells, BMPs, and bioactive scaffolds is providing solutions for recalcitrant defects. Furthermore, the advent of bioabsorbable magnesium alloys and internal motorized lengthening nails is effectively eliminating the need for secondary surgeries. The convergence of the “Digital Twin” paradigm with regenerative medicine offers a personalised trajectory for paediatric care. By embracing these advancements, clinicians can restore function while rigorously minimising the physical and psychological burden on the developing child.
DOI: https://doi.org/10.37349/emd.2026.1007129
This article belongs to the special issue Innovation in Orthopedics
Aim:
Evaluate the associations between usage of the standalone SmartMoms Canada mHealth intervention, and gestational weight gain (GWG) guideline adherence and lifestyle improvements in pregnant individuals in the context of a pragmatic study.
Methods:
Participants (18–40 years, BMI 18.5–39.9 kg/m2) were recruited into a single-arm trial conducted in Winnipeg and Ottawa, Canada. All participants were provided with the app, a Fitbit® tracker, and a smart scale. Participants were assessed in early, mid-, and late pregnancy. Physical activity was measured with the Godin Leisure Time Exercise score, and the Fitbit® tracker (steps and time in physical activity). Fitbit® app was used to measure dietary intake. App usage and GWG were monitored. GWG guideline adherence was compared with data from the Statistics Canada Maternal Experiences Survey (MES). GWG adherence and lifestyle changes were compared between app usage groups (≥ median weekly app usage vs. < median) with multinomial logistic regressions or t tests. Trajectories in lifestyle changes were compared between groups with repeated measure analyses.
Results:
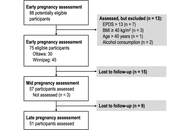
Of the 75 participants recruited in early pregnancy, 51 were followed through pregnancy (32% drop out). Overall app usage was low (median 1.30 min/wk). Adequate GWG was achieved by 35.7% (95% CI: 23.2–48.2) of participants vs. 32.6% in the MES; while excessive GWG occurred in 50.0% (95% CI: 36.9–63.1) vs. 48.7%. GWG adherence was not different between usage groups (P = 0.399), but a higher mean weekly app usage (continuous) was associated with lower odds of insufficient GWG (OR = 0.01, P = 0.035). There were no significant associations between app usage and changes in physical activity, but a lower increase in carbohydrate intake was observed in the higher usage group.
Conclusions:
Few associations were found between app usage and GWG or lifestyle outcomes. Lack of significant results could relate to low protocol and intervention adherence (Trial registration: http://www.isrctn.com/ISRCTN16254958).
Aim:
Evaluate the associations between usage of the standalone SmartMoms Canada mHealth intervention, and gestational weight gain (GWG) guideline adherence and lifestyle improvements in pregnant individuals in the context of a pragmatic study.
Methods:
Participants (18–40 years, BMI 18.5–39.9 kg/m2) were recruited into a single-arm trial conducted in Winnipeg and Ottawa, Canada. All participants were provided with the app, a Fitbit® tracker, and a smart scale. Participants were assessed in early, mid-, and late pregnancy. Physical activity was measured with the Godin Leisure Time Exercise score, and the Fitbit® tracker (steps and time in physical activity). Fitbit® app was used to measure dietary intake. App usage and GWG were monitored. GWG guideline adherence was compared with data from the Statistics Canada Maternal Experiences Survey (MES). GWG adherence and lifestyle changes were compared between app usage groups (≥ median weekly app usage vs. < median) with multinomial logistic regressions or t tests. Trajectories in lifestyle changes were compared between groups with repeated measure analyses.
Results:
Of the 75 participants recruited in early pregnancy, 51 were followed through pregnancy (32% drop out). Overall app usage was low (median 1.30 min/wk). Adequate GWG was achieved by 35.7% (95% CI: 23.2–48.2) of participants vs. 32.6% in the MES; while excessive GWG occurred in 50.0% (95% CI: 36.9–63.1) vs. 48.7%. GWG adherence was not different between usage groups (P = 0.399), but a higher mean weekly app usage (continuous) was associated with lower odds of insufficient GWG (OR = 0.01, P = 0.035). There were no significant associations between app usage and changes in physical activity, but a lower increase in carbohydrate intake was observed in the higher usage group.
Conclusions:
Few associations were found between app usage and GWG or lifestyle outcomes. Lack of significant results could relate to low protocol and intervention adherence (Trial registration: http://www.isrctn.com/ISRCTN16254958).
DOI: https://doi.org/10.37349/edht.2026.101197
Aim:
Attention deficit hyperactivity disorder (ADHD) is a common condition impacting approximately 5% of children and 3–4% of adults in the United Kingdom (UK). While it cannot be cured, treatment has been shown to positively impact the difficulties associated with ADHD. However, ADHD is widely underdiagnosed and undertreated in the UK. This paper reports the results of a model developed to estimate pharmacological treatment rates by area across National Health Service (NHS) integrated care systems (ICSs) in England, health boards in Scotland and Wales, and health & social care trusts (HSCTs) in Northern Ireland.
Methods:
The model used the UK general population and ADHD prevalence data to estimate the number of patients with ADHD in each area. Prescription data for medicines licensed for the treatment of ADHD were then used to estimate the number of patients who are untreated and treated, and the percentage treatment rates by area. The analysis was descriptive, focusing on quantifying geographic variation in treatment rates.
Results:
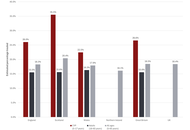
Nationally, the estimated proportions of children and young people (CYP; 5–17 years) and adults (18–65 years) treated were 26.6% and 15.6%, respectively, of the expected ADHD populations. Treatment rates by ICS or health board in England, Scotland, and Wales ranged from 11.7% to 60.6% for the CYP population and 8.6% to 24.8% for the adult population (data for Northern Ireland were not available by age group). Overall treatment rates (ages 5–65 years) in Northern Ireland ranged from 6.7% in the lowest-ranking HSCT to 31.1% in the highest-ranking HSCT.
Conclusions:
In the UK, there is currently a high degree of geographic variation across all NHS systems and a generally low level of treatment of ADHD, especially in adults. Up to a 4.6-fold difference in pharmacological treatment rates was observed between NHS service provider areas.
Aim:
Attention deficit hyperactivity disorder (ADHD) is a common condition impacting approximately 5% of children and 3–4% of adults in the United Kingdom (UK). While it cannot be cured, treatment has been shown to positively impact the difficulties associated with ADHD. However, ADHD is widely underdiagnosed and undertreated in the UK. This paper reports the results of a model developed to estimate pharmacological treatment rates by area across National Health Service (NHS) integrated care systems (ICSs) in England, health boards in Scotland and Wales, and health & social care trusts (HSCTs) in Northern Ireland.
Methods:
The model used the UK general population and ADHD prevalence data to estimate the number of patients with ADHD in each area. Prescription data for medicines licensed for the treatment of ADHD were then used to estimate the number of patients who are untreated and treated, and the percentage treatment rates by area. The analysis was descriptive, focusing on quantifying geographic variation in treatment rates.
Results:
Nationally, the estimated proportions of children and young people (CYP; 5–17 years) and adults (18–65 years) treated were 26.6% and 15.6%, respectively, of the expected ADHD populations. Treatment rates by ICS or health board in England, Scotland, and Wales ranged from 11.7% to 60.6% for the CYP population and 8.6% to 24.8% for the adult population (data for Northern Ireland were not available by age group). Overall treatment rates (ages 5–65 years) in Northern Ireland ranged from 6.7% in the lowest-ranking HSCT to 31.1% in the highest-ranking HSCT.
Conclusions:
In the UK, there is currently a high degree of geographic variation across all NHS systems and a generally low level of treatment of ADHD, especially in adults. Up to a 4.6-fold difference in pharmacological treatment rates was observed between NHS service provider areas.
DOI: https://doi.org/10.37349/ent.2026.1004163
This article belongs to the special issue Advances in the Pathogenesis, Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder
Aim:
Diabetic neuropathy is the most prevalent diabetic complication, impacting up to 60% of people with diabetes. It is characterized by distal symmetrical loss of sensory function in the lower extremities, presenting with spontaneous excruciating neuropathic pain, hyperalgesia, and allodynia that impairs quality of life. The current work aims to evaluate the neuroprotective potential of naringin (a citrus flavonoid) and examine its ability to improve Streptozotocin (STZ)-induced diabetic neuropathic pain by investigating its hypoglycemic, lipid-lowering, anti-inflammatory, and antioxidant effects.
Methods:
Diabetes was induced in 30 of 40 male Sprague-Dawley rats via a single STZ injection (45 mg/kg). Rats were divided into four groups: normal control, diabetic control, naringin-treated, and glimepiride-treated (positive control). After treatment, serum and brain tissues were collected to assess biochemical parameters. Pain-related behaviors were evaluated using hot plate, tail immersion, and von Frey filament tests.
Results:
A significant increase in the serum levels of glucose, triglyceride, total cholesterol, low-density lipoprotein-cholesterol, and nitric oxide, with a concomitant decrease in body weight, plasma insulin, and high-density lipoprotein-cholesterol, was observed in diabetic rats. Also, the brain level of malondialdehyde was increased, while that of reduced glutathione, glutathione peroxidase, catalase, and superoxide dismutase were markedly decreased. Furthermore, diabetic rats showed a marked increase in plasma levels of inflammatory cytokines including interleukin-6 and tumor necrosis factor-α. Moreover, hot plate, tail immersion, and von Frey tests revealed hyperalgesia in diabetic rats. Treatment with naringin and glimepiride reduced pain hypersensitivity, restored body weight, and nearly normalized the altered biochemical parameters, more significantly with naringin than with glimepiride.
Conclusions:
These results may highlight the potential effects of naringin as a therapeutic strategy for diabetes and its complications, including peripheral neuropathy.
Aim:
Diabetic neuropathy is the most prevalent diabetic complication, impacting up to 60% of people with diabetes. It is characterized by distal symmetrical loss of sensory function in the lower extremities, presenting with spontaneous excruciating neuropathic pain, hyperalgesia, and allodynia that impairs quality of life. The current work aims to evaluate the neuroprotective potential of naringin (a citrus flavonoid) and examine its ability to improve Streptozotocin (STZ)-induced diabetic neuropathic pain by investigating its hypoglycemic, lipid-lowering, anti-inflammatory, and antioxidant effects.
Methods:
Diabetes was induced in 30 of 40 male Sprague-Dawley rats via a single STZ injection (45 mg/kg). Rats were divided into four groups: normal control, diabetic control, naringin-treated, and glimepiride-treated (positive control). After treatment, serum and brain tissues were collected to assess biochemical parameters. Pain-related behaviors were evaluated using hot plate, tail immersion, and von Frey filament tests.
Results:
A significant increase in the serum levels of glucose, triglyceride, total cholesterol, low-density lipoprotein-cholesterol, and nitric oxide, with a concomitant decrease in body weight, plasma insulin, and high-density lipoprotein-cholesterol, was observed in diabetic rats. Also, the brain level of malondialdehyde was increased, while that of reduced glutathione, glutathione peroxidase, catalase, and superoxide dismutase were markedly decreased. Furthermore, diabetic rats showed a marked increase in plasma levels of inflammatory cytokines including interleukin-6 and tumor necrosis factor-α. Moreover, hot plate, tail immersion, and von Frey tests revealed hyperalgesia in diabetic rats. Treatment with naringin and glimepiride reduced pain hypersensitivity, restored body weight, and nearly normalized the altered biochemical parameters, more significantly with naringin than with glimepiride.
Conclusions:
These results may highlight the potential effects of naringin as a therapeutic strategy for diabetes and its complications, including peripheral neuropathy.
DOI: https://doi.org/10.37349/eemd.2026.101476
This article belongs to the special issue Current Views on Pathogenesis, Diagnosis and Management of Type 2 Diabetes Mellitus and Its Complications and Related Conditions
Today, researchers have already made great progress in finding drug-based clinical solutions against microbial infections. It has become an essential part of a healthy human lifestyle. High antibiotic consumption has accelerated antibiotic resistance in microbial species (multi-drug-resistant microbial strains, like Staphylococcus aureus and Mycobacterium tuberculosis, have already been reported). Loss of microflora is also associated with the heavy and unnecessary use of drugs. This review presents bacteriophage as an alternative to antibiotics. The supporting bacteriophage characteristics include bacteriophage lytic mode of replication, specificity towards its host, bacteriophage mass production, and bacteriophage genetic modification (BRED and CRISPR) to make it capable of degrading microbial biofilm. The author has also tried to inculcate previous work that has already been done with bacteriophages for some clinical therapies. Potential administration routes (oral, intravenous, and intraoperative) used in clinical therapies are discussed.
Today, researchers have already made great progress in finding drug-based clinical solutions against microbial infections. It has become an essential part of a healthy human lifestyle. High antibiotic consumption has accelerated antibiotic resistance in microbial species (multi-drug-resistant microbial strains, like Staphylococcus aureus and Mycobacterium tuberculosis, have already been reported). Loss of microflora is also associated with the heavy and unnecessary use of drugs. This review presents bacteriophage as an alternative to antibiotics. The supporting bacteriophage characteristics include bacteriophage lytic mode of replication, specificity towards its host, bacteriophage mass production, and bacteriophage genetic modification (BRED and CRISPR) to make it capable of degrading microbial biofilm. The author has also tried to inculcate previous work that has already been done with bacteriophages for some clinical therapies. Potential administration routes (oral, intravenous, and intraoperative) used in clinical therapies are discussed.
DOI: https://doi.org/10.37349/eds.2026.1008166
Neurodegenerative and neurodevelopmental neurological disorders represent a growing global health burden, characterized by progressive neuronal dysfunction, cognitive decline, and impaired functional outcomes. Increasing evidence highlights neuroinflammation as a central pathophysiological mechanism linking mitochondrial dysfunction, oxidative stress, microbiota dysbiosis, and synaptic impairment across diverse neurological conditions. This narrative review was conducted using a structured literature search approach, incorporating major biomedical databases to enhance transparency and reproducibility. This review synthesizes contemporary evidence on mechanistic pathways underlying neuroinflammation-mediated neurodegeneration and critically evaluates emerging neuroprotective therapeutic strategies. Particular emphasis is placed on mitochondrial transfer approaches, novel circulating and imaging biomarkers, and integrative neurotechnological innovations such as artificial intelligence-driven neuroimaging analytics. While several therapeutic approaches demonstrate promise in preclinical models, most remain at early experimental or translational stages, with limited validation in large-scale human studies. Current findings suggest that targeting neuroimmune signaling cascades, restoring mitochondrial bioenergetics, and modulating gut-brain axis interactions may provide synergistic neuroprotective benefits. The review proposes a multidimensional precision-medicine framework incorporating biomarker-guided therapeutic selection and interdisciplinary care models. Future research priorities include longitudinal biomarker validation, randomized clinical trials of mitochondrial-based therapies, and integration of digital neurodiagnostic platforms to enhance early disease detection. Despite these advances, significant gaps remain in clinical translation, standardization of biomarkers, and long-term therapeutic safety, necessitating cautious interpretation of emerging evidence.
Neurodegenerative and neurodevelopmental neurological disorders represent a growing global health burden, characterized by progressive neuronal dysfunction, cognitive decline, and impaired functional outcomes. Increasing evidence highlights neuroinflammation as a central pathophysiological mechanism linking mitochondrial dysfunction, oxidative stress, microbiota dysbiosis, and synaptic impairment across diverse neurological conditions. This narrative review was conducted using a structured literature search approach, incorporating major biomedical databases to enhance transparency and reproducibility. This review synthesizes contemporary evidence on mechanistic pathways underlying neuroinflammation-mediated neurodegeneration and critically evaluates emerging neuroprotective therapeutic strategies. Particular emphasis is placed on mitochondrial transfer approaches, novel circulating and imaging biomarkers, and integrative neurotechnological innovations such as artificial intelligence-driven neuroimaging analytics. While several therapeutic approaches demonstrate promise in preclinical models, most remain at early experimental or translational stages, with limited validation in large-scale human studies. Current findings suggest that targeting neuroimmune signaling cascades, restoring mitochondrial bioenergetics, and modulating gut-brain axis interactions may provide synergistic neuroprotective benefits. The review proposes a multidimensional precision-medicine framework incorporating biomarker-guided therapeutic selection and interdisciplinary care models. Future research priorities include longitudinal biomarker validation, randomized clinical trials of mitochondrial-based therapies, and integration of digital neurodiagnostic platforms to enhance early disease detection. Despite these advances, significant gaps remain in clinical translation, standardization of biomarkers, and long-term therapeutic safety, necessitating cautious interpretation of emerging evidence.
DOI: https://doi.org/10.37349/ent.2026.1004162
This article belongs to the special issue Neuro-Inflammation as a Target in the Design of Multifunctional Drug Candidates for Neurodegenerative Diseases
Aim:
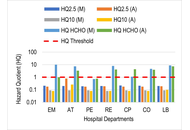
Indoor air quality (IAQ) is a critical component of occupational health in hospitals, where healthcare workers face exposure to particulates and clinical chemical vapours. Prolonged exposure to these environments is linked to an increased incidence of chronic respiratory conditions. This study aimed to quantify the indoor concentrations of particulate matter (PM2.5 and PM10), formaldehyde (HCHO), and total volatile organic compounds (TVOCs) in public and private tertiary healthcare facilities in Benin City, Nigeria, and to evaluate the associated non−carcinogenic and carcinogenic health risks for personnel.
Methods:
IAQ was monitored in triplicate at high-occupancy sampling points over an eight-week period using handheld digital monitors. Health risks were assessed using hazard quotient (HQ) and incremental lifetime cancer risk (ILCR) models. Additionally, a structured questionnaire was administered to 152 hospital workers to correlate environmental data with self-reported respiratory symptoms.
Results:
The PM2.5 and TVOC levels frequently exceeded the WHO guidelines in both facilities. The private facility exhibited alarming HCHO concentrations, particularly in the emergency (HQ = 10.04) and laboratory (HQ = 8.86) units, indicating risks up to ten times the safety threshold. Similarly, the ILCR exceeded the 1.0 × 10−4 threshold at the highest exposure site, reaching a peak of 1.49 × 10−4. Coughing (78.3%) was the most prevalent symptom. Notably, compared with workers in the private sector, workers in public hospitals faced significantly greater respiratory burdens, with an adjusted odds ratio (AOR) of 3.009 (95% CI: 1.277–7.088) for persistent cough and an AOR of 2.681 (95% CI: 1.093–6.578) for chest pain.
Conclusions:
Hospital indoor air poses severe toxicological and carcinogenic risks. Immediate implementation of advanced mechanical ventilation and specialized filtration is needed to safeguard healthcare personnel.
Aim:
Indoor air quality (IAQ) is a critical component of occupational health in hospitals, where healthcare workers face exposure to particulates and clinical chemical vapours. Prolonged exposure to these environments is linked to an increased incidence of chronic respiratory conditions. This study aimed to quantify the indoor concentrations of particulate matter (PM2.5 and PM10), formaldehyde (HCHO), and total volatile organic compounds (TVOCs) in public and private tertiary healthcare facilities in Benin City, Nigeria, and to evaluate the associated non−carcinogenic and carcinogenic health risks for personnel.
Methods:
IAQ was monitored in triplicate at high-occupancy sampling points over an eight-week period using handheld digital monitors. Health risks were assessed using hazard quotient (HQ) and incremental lifetime cancer risk (ILCR) models. Additionally, a structured questionnaire was administered to 152 hospital workers to correlate environmental data with self-reported respiratory symptoms.
Results:
The PM2.5 and TVOC levels frequently exceeded the WHO guidelines in both facilities. The private facility exhibited alarming HCHO concentrations, particularly in the emergency (HQ = 10.04) and laboratory (HQ = 8.86) units, indicating risks up to ten times the safety threshold. Similarly, the ILCR exceeded the 1.0 × 10−4 threshold at the highest exposure site, reaching a peak of 1.49 × 10−4. Coughing (78.3%) was the most prevalent symptom. Notably, compared with workers in the private sector, workers in public hospitals faced significantly greater respiratory burdens, with an adjusted odds ratio (AOR) of 3.009 (95% CI: 1.277–7.088) for persistent cough and an AOR of 2.681 (95% CI: 1.093–6.578) for chest pain.
Conclusions:
Hospital indoor air poses severe toxicological and carcinogenic risks. Immediate implementation of advanced mechanical ventilation and specialized filtration is needed to safeguard healthcare personnel.
DOI: https://doi.org/10.37349/eaa.2026.1009129
This article belongs to the special issue Environment, Infectious Diseases, and Allergy
Beyond the importance of organic seeds as key inputs in sustainable food production systems, when assessing the scientific evidence supporting their agronomic performance, commercialization, and quality/compositional characterization, several critical gaps remain. Aspects such as defining organic, agroecological and conventional seeds, regulatory frameworks, and compositional characteristics are frequently addressed in a fragmented manner in the literature. Discussing the implications of organic seed production, together with clarifying terms that are often used indiscriminately, is essential to ensure appropriate standards and product quality. At the same time, research-driven methodologies for control and data generation play a crucial role in overcoming challenges related to certification and traceability, particularly in the seed sector. Nevertheless, current evidence on organic seeds remains limited and largely exploratory, with variable results across studies and a strong influence of confounding factors (genetic, regional, climate). This situation complicates the identification of universal markers and the development of robust classification models. To address these limitations, this review integrates and reflects on the state-of-the-art knowledge on organic seed production, including agronomic, regulatory, and market traits. In addition, we synthesize major analytical approaches to assess organic seed authentication, highlighting the potential of intrinsic compositional features through fingerprinting strategies using elemental, isotopic, and metabolomic profiles as complementary tools from the traditionally used techniques based on physicochemical and physiological parameters (e.g., vigour, germination, purity). The remaining challenge lies in connecting academic research and practical application. While holistic approaches, such as omics, provide insights into seed composition and marker discovery, their use is restricted to laboratory settings due to the need for costly instrumentation and complex data processing. Advancing this field requires translating these findings into accessible tools by using the identified markers that support regulatory frameworks, which finally promote agronomic practices and market expansion, also ensuring transparency in the organic seed sector.
Beyond the importance of organic seeds as key inputs in sustainable food production systems, when assessing the scientific evidence supporting their agronomic performance, commercialization, and quality/compositional characterization, several critical gaps remain. Aspects such as defining organic, agroecological and conventional seeds, regulatory frameworks, and compositional characteristics are frequently addressed in a fragmented manner in the literature. Discussing the implications of organic seed production, together with clarifying terms that are often used indiscriminately, is essential to ensure appropriate standards and product quality. At the same time, research-driven methodologies for control and data generation play a crucial role in overcoming challenges related to certification and traceability, particularly in the seed sector. Nevertheless, current evidence on organic seeds remains limited and largely exploratory, with variable results across studies and a strong influence of confounding factors (genetic, regional, climate). This situation complicates the identification of universal markers and the development of robust classification models. To address these limitations, this review integrates and reflects on the state-of-the-art knowledge on organic seed production, including agronomic, regulatory, and market traits. In addition, we synthesize major analytical approaches to assess organic seed authentication, highlighting the potential of intrinsic compositional features through fingerprinting strategies using elemental, isotopic, and metabolomic profiles as complementary tools from the traditionally used techniques based on physicochemical and physiological parameters (e.g., vigour, germination, purity). The remaining challenge lies in connecting academic research and practical application. While holistic approaches, such as omics, provide insights into seed composition and marker discovery, their use is restricted to laboratory settings due to the need for costly instrumentation and complex data processing. Advancing this field requires translating these findings into accessible tools by using the identified markers that support regulatory frameworks, which finally promote agronomic practices and market expansion, also ensuring transparency in the organic seed sector.
DOI: https://doi.org/10.37349/eff.2026.1010175
This article belongs to the special issue Food Authenticity and Emerging Challenges of Novel Food
Aim:
Mycotoxins are toxic secondary metabolites produced by various fungal species, commonly found as contaminants in food products and biological matrices. Due to their potential adverse effects on human health, reliable analytical methods for their detection are essential.
Methods:
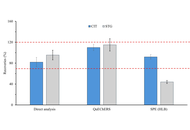
This study presents the development and validation of an analytical method based on ultra-high-performance liquid chromatography coupled with tandem mass spectrometry (UHPLC-MS/MS) for the simultaneous determination of the emerging mycotoxins citrinin (CIT) and sterigmatocystin (STG) in human urine. Sample preparation was optimized, performed using the QuEChERS (Quick, Easy, Cheap, Effective, Rugged, and Safe) extraction technique, selected for its high recovery rates and reproducibility.
Results:
The method demonstrated satisfactory linearity, precision, and sensitivity, with limits of quantification of 2.5 pg/mL and 0.75 pg/mL for CIT and STG, respectively. Analysis of twenty urine samples revealed the presence of CIT in six samples at trace concentrations, while STG was not detected above the quantification limit.
Conclusions:
A preliminary risk assessment of CIT indicated that the detected levels do not pose a significant toxicological risk. The validated method shows great potential for application in human biomonitoring studies aimed at assessing exposure to mycotoxins.
Aim:
Mycotoxins are toxic secondary metabolites produced by various fungal species, commonly found as contaminants in food products and biological matrices. Due to their potential adverse effects on human health, reliable analytical methods for their detection are essential.
Methods:
This study presents the development and validation of an analytical method based on ultra-high-performance liquid chromatography coupled with tandem mass spectrometry (UHPLC-MS/MS) for the simultaneous determination of the emerging mycotoxins citrinin (CIT) and sterigmatocystin (STG) in human urine. Sample preparation was optimized, performed using the QuEChERS (Quick, Easy, Cheap, Effective, Rugged, and Safe) extraction technique, selected for its high recovery rates and reproducibility.
Results:
The method demonstrated satisfactory linearity, precision, and sensitivity, with limits of quantification of 2.5 pg/mL and 0.75 pg/mL for CIT and STG, respectively. Analysis of twenty urine samples revealed the presence of CIT in six samples at trace concentrations, while STG was not detected above the quantification limit.
Conclusions:
A preliminary risk assessment of CIT indicated that the detected levels do not pose a significant toxicological risk. The validated method shows great potential for application in human biomonitoring studies aimed at assessing exposure to mycotoxins.
DOI: https://doi.org/10.37349/eff.2026.1010176
This article belongs to the special issue Food Contaminants: Analysis, Occurrence and Risk Assessment
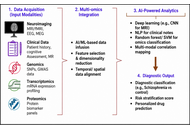
Schizophrenia affects approximately 24 million people worldwide, representing 0.3–0.7% of the global population, and remains a leading cause of years lived with disability. The disorder contributes to over 13 million disability-adjusted life years, underscoring its substantial global health and socioeconomic burden. This review critically examines the convergence of artificial intelligence (AI) and advanced oral drug delivery systems as an emerging strategy in schizophrenia management. Conventional diagnostic frameworks, reliant on subjective symptom assessment, often result in delayed or inaccurate diagnosis, while standard oral antipsychotics are limited by poor bioavailability, extensive first-pass metabolism, and inadequate brain targeting. Recent advances in AI, including natural language processing (NLP), neuroimaging analytics, electrophysiological modeling, and multi-omics integration, support diagnostic classification, risk prediction, symptom monitoring, and patient stratification. Simultaneously, nanotechnology-driven oral delivery platforms such as lipid nanoparticles, dendrimers, and proliposomes enhance pharmacokinetics, central nervous system targeting, and therapeutic adherence. The integration of AI with pharmacogenomics, wearable monitoring, and digital twin models further facilitates real-time dose optimization and personalized therapy. Despite promising preclinical and clinical outcomes, challenges related to data privacy, algorithmic bias, scalability, and regulatory translation persist. This review highlights a shift toward precision psychiatry, where AI-enabled diagnostics and smart oral therapeutics may support predictive, personalized, and adaptive care in schizophrenia.
Schizophrenia affects approximately 24 million people worldwide, representing 0.3–0.7% of the global population, and remains a leading cause of years lived with disability. The disorder contributes to over 13 million disability-adjusted life years, underscoring its substantial global health and socioeconomic burden. This review critically examines the convergence of artificial intelligence (AI) and advanced oral drug delivery systems as an emerging strategy in schizophrenia management. Conventional diagnostic frameworks, reliant on subjective symptom assessment, often result in delayed or inaccurate diagnosis, while standard oral antipsychotics are limited by poor bioavailability, extensive first-pass metabolism, and inadequate brain targeting. Recent advances in AI, including natural language processing (NLP), neuroimaging analytics, electrophysiological modeling, and multi-omics integration, support diagnostic classification, risk prediction, symptom monitoring, and patient stratification. Simultaneously, nanotechnology-driven oral delivery platforms such as lipid nanoparticles, dendrimers, and proliposomes enhance pharmacokinetics, central nervous system targeting, and therapeutic adherence. The integration of AI with pharmacogenomics, wearable monitoring, and digital twin models further facilitates real-time dose optimization and personalized therapy. Despite promising preclinical and clinical outcomes, challenges related to data privacy, algorithmic bias, scalability, and regulatory translation persist. This review highlights a shift toward precision psychiatry, where AI-enabled diagnostics and smart oral therapeutics may support predictive, personalized, and adaptive care in schizophrenia.
DOI: https://doi.org/10.37349/eds.2026.1008165
This article belongs to the special issue Nanoformulations for Non-Intravenous Drug Delivery
Sodium–glucose cotransporter 2 inhibitors (SGLT2i) were originally developed as glucose-lowering therapies for type 2 diabetes mellitus. However, robust clinical evidence has demonstrated substantial cardiovascular and renal protective effects that extend beyond glycemic control. Emerging data highlight their systemic influence across the cardiovascular–renal–metabolic (CRM) continuum, a conceptual framework describing the shared pathophysiological links between metabolic dysfunction, heart failure (HF), and chronic kidney disease (CKD). Despite the rapid expansion of clinical and mechanistic evidence, the integration of these insights into coordinated therapeutic implementation across cardiology, nephrology, and endocrinology remains incompletely synthesized. This structured narrative review synthesized evidence from PubMed/MEDLINE, Embase, and Google Scholar to identify relevant studies published between January 2016 and December 2025. Emphasis was placed on randomized controlled trials, meta-analyses, large observational cohorts, guideline documents, and translational mechanistic investigations evaluating pharmacologic mechanisms, clinical efficacy, and multidisciplinary applications of SGLT2i across CRM conditions. Cardiovascular and renal outcome trials consistently show that SGLT2i reduce hospitalization for heart failure, delay CKD progression, and improve major cardiovascular outcomes in both diabetic and non-diabetic populations. Mechanistically, these agents restore tubuloglomerular feedback, enhance cardiac energy efficiency through increased ketone utilization, attenuate inflammatory and profibrotic signaling pathways, and improve mitochondrial bioenergetics. These multisystem effects contribute to therapeutic benefits across HF phenotypes and CKD stages while also improving metabolic parameters such as adiposity, blood pressure, and hepatic steatosis. Collectively, current evidence supports SGLT2i as foundational disease-modifying therapies across the CRM spectrum. Future investigations should prioritize precision-based treatment approaches, biomarker-guided patient selection, and rational combination pharmacotherapy to further optimize outcomes across interconnected cardiovascular, renal, and metabolic diseases.
Sodium–glucose cotransporter 2 inhibitors (SGLT2i) were originally developed as glucose-lowering therapies for type 2 diabetes mellitus. However, robust clinical evidence has demonstrated substantial cardiovascular and renal protective effects that extend beyond glycemic control. Emerging data highlight their systemic influence across the cardiovascular–renal–metabolic (CRM) continuum, a conceptual framework describing the shared pathophysiological links between metabolic dysfunction, heart failure (HF), and chronic kidney disease (CKD). Despite the rapid expansion of clinical and mechanistic evidence, the integration of these insights into coordinated therapeutic implementation across cardiology, nephrology, and endocrinology remains incompletely synthesized. This structured narrative review synthesized evidence from PubMed/MEDLINE, Embase, and Google Scholar to identify relevant studies published between January 2016 and December 2025. Emphasis was placed on randomized controlled trials, meta-analyses, large observational cohorts, guideline documents, and translational mechanistic investigations evaluating pharmacologic mechanisms, clinical efficacy, and multidisciplinary applications of SGLT2i across CRM conditions. Cardiovascular and renal outcome trials consistently show that SGLT2i reduce hospitalization for heart failure, delay CKD progression, and improve major cardiovascular outcomes in both diabetic and non-diabetic populations. Mechanistically, these agents restore tubuloglomerular feedback, enhance cardiac energy efficiency through increased ketone utilization, attenuate inflammatory and profibrotic signaling pathways, and improve mitochondrial bioenergetics. These multisystem effects contribute to therapeutic benefits across HF phenotypes and CKD stages while also improving metabolic parameters such as adiposity, blood pressure, and hepatic steatosis. Collectively, current evidence supports SGLT2i as foundational disease-modifying therapies across the CRM spectrum. Future investigations should prioritize precision-based treatment approaches, biomarker-guided patient selection, and rational combination pharmacotherapy to further optimize outcomes across interconnected cardiovascular, renal, and metabolic diseases.
DOI: https://doi.org/10.37349/ec.2026.1012113
Aim:
The study aims to explore the relationship between TLR2 (rs3804100), TLR4 (rs1927914), and TLR7 (rs179008) gene polymorphisms and Human Cytomegalovirus (HCMV) serostatus in Iraqi women, and to assess the association between spontaneous abortion (SA) and these polymorphisms.
Methods:
A case-control study involving 200 women compared 100 who had SAs before 20 weeks of gestation with 100 healthy pregnant controls from Diyala and Babylon Governorates. The study utilised qualitative ELISA to detect HCMV IgG and IgM antibodies in serum and employed the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) technique for genotyping TLR2 (rs3804100 T>C), TLR4 (rs1927914 G>A), and TLR7 (rs179008 A>T) polymorphisms.
Results:
The study revealed that HCMV IgG and IgM antibodies were significantly elevated in women with SA compared to the control group (P < 0.001). No notable association was found between the TLR2 rs3804100 polymorphism and SA. Notably, there were marked differences in the genotype and allele distributions of TLR4 rs1927914 and TLR7 rs179008 observed between the cases and controls. Specific genotypes of TLR4 and TLR7 genes were associated with modified odds of SA. Furthermore, the high prevalence of HCMV IgG may be linked to genetic associations, particularly TLR genotypes, whereas analysis of HCMV IgM was constrained by the low prevalence observed in control subjects.
Conclusions:
Variations in the TLR4 and TLR7 genes may be associated with the risk of SA in women in this population. The influence of HCMV seropositivity on immune-related genetic associations should be approached with caution. Further studies with larger sample sizes and consideration of confounding variables are needed.
Aim:
The study aims to explore the relationship between TLR2 (rs3804100), TLR4 (rs1927914), and TLR7 (rs179008) gene polymorphisms and Human Cytomegalovirus (HCMV) serostatus in Iraqi women, and to assess the association between spontaneous abortion (SA) and these polymorphisms.
Methods:
A case-control study involving 200 women compared 100 who had SAs before 20 weeks of gestation with 100 healthy pregnant controls from Diyala and Babylon Governorates. The study utilised qualitative ELISA to detect HCMV IgG and IgM antibodies in serum and employed the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) technique for genotyping TLR2 (rs3804100 T>C), TLR4 (rs1927914 G>A), and TLR7 (rs179008 A>T) polymorphisms.
Results:
The study revealed that HCMV IgG and IgM antibodies were significantly elevated in women with SA compared to the control group (P < 0.001). No notable association was found between the TLR2 rs3804100 polymorphism and SA. Notably, there were marked differences in the genotype and allele distributions of TLR4 rs1927914 and TLR7 rs179008 observed between the cases and controls. Specific genotypes of TLR4 and TLR7 genes were associated with modified odds of SA. Furthermore, the high prevalence of HCMV IgG may be linked to genetic associations, particularly TLR genotypes, whereas analysis of HCMV IgM was constrained by the low prevalence observed in control subjects.
Conclusions:
Variations in the TLR4 and TLR7 genes may be associated with the risk of SA in women in this population. The influence of HCMV seropositivity on immune-related genetic associations should be approached with caution. Further studies with larger sample sizes and consideration of confounding variables are needed.
DOI: https://doi.org/10.37349/ei.2026.1003258
Breast cancer classification and therapeutic decision-making have traditionally relied on the evaluation of estrogen receptor alpha (ERα), PR, and HER2, yet this framework does not fully explain tumor heterogeneity, endocrine resistance, or estrogen responsiveness in ERα-negative contexts. Emerging evidence implicates non-genomic estrogen signaling mediated by membrane-associated receptors such as G protein-coupled estrogen receptor 1 (GPER-1) and ERα36. Acting as interconnected signaling nodes, these receptors activate MAPK/ERK and PI3K/AKT pathways and engage in crosstalk with receptors such as EGFR, promoting proliferation, cellular plasticity, and adaptive responses. Here, we propose an integrative framework based on three axes: endocrine resistance in ERα-positive tumors, estrogen responsiveness in ERα-negative subtypes, and environmental modulation of signaling. Within this model, GPER-1 and ERα36 form a coordinated network that extends beyond genomic mechanisms and converges on shared downstream effectors. These pathways also intersect with post-transcriptional regulation, tumor-microenvironment interactions, and extracellular vesicle-mediated communication, contributing to tumor progression and metastasis. Environmental ligands, such as bisphenol A, may further modulate signaling intensity, reinforcing plasticity and resistance phenotypes. Collectively, GPER-1 and ERα36 emerge as candidate biomarkers with diagnostic and therapeutic relevance. Their integration into multi-omics and functional classification strategies may refine breast cancer stratification and support more precise therapeutic approaches.
Breast cancer classification and therapeutic decision-making have traditionally relied on the evaluation of estrogen receptor alpha (ERα), PR, and HER2, yet this framework does not fully explain tumor heterogeneity, endocrine resistance, or estrogen responsiveness in ERα-negative contexts. Emerging evidence implicates non-genomic estrogen signaling mediated by membrane-associated receptors such as G protein-coupled estrogen receptor 1 (GPER-1) and ERα36. Acting as interconnected signaling nodes, these receptors activate MAPK/ERK and PI3K/AKT pathways and engage in crosstalk with receptors such as EGFR, promoting proliferation, cellular plasticity, and adaptive responses. Here, we propose an integrative framework based on three axes: endocrine resistance in ERα-positive tumors, estrogen responsiveness in ERα-negative subtypes, and environmental modulation of signaling. Within this model, GPER-1 and ERα36 form a coordinated network that extends beyond genomic mechanisms and converges on shared downstream effectors. These pathways also intersect with post-transcriptional regulation, tumor-microenvironment interactions, and extracellular vesicle-mediated communication, contributing to tumor progression and metastasis. Environmental ligands, such as bisphenol A, may further modulate signaling intensity, reinforcing plasticity and resistance phenotypes. Collectively, GPER-1 and ERα36 emerge as candidate biomarkers with diagnostic and therapeutic relevance. Their integration into multi-omics and functional classification strategies may refine breast cancer stratification and support more precise therapeutic approaches.
DOI: https://doi.org/10.37349/etat.2026.1002377
This article belongs to the special issue Breaking Boundaries in Breast Cancer Care: Emerging Controversies and Innovation in Surgical and Medical Approaches
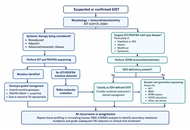
Gastrointestinal stromal tumours (GISTs) are the clearest solid-tumour model of precision oncology because diagnosis, prognosis, and treatment are strongly shaped by molecular genotype. The discovery of activating mutations in KIT proto-oncogene receptor tyrosine kinase (KIT) and platelet-derived growth factor receptor alpha (PDGFRA) transformed management by enabling genotype-directed use of tyrosine kinase inhibitors (TKIs) across localized and advanced disease. This review summarizes how molecular classification informs contemporary GIST care, from diagnostic work-up and risk stratification to neoadjuvant, adjuvant, and metastatic treatment planning. KIT exon 11 mutations generally predict sensitivity to standard-dose imatinib, whereas KIT exon 9 tumours may benefit from dose escalation. PDGFRA D842V confers primary resistance to imatinib but sensitivity to avapritinib, illustrating the clinical value of mutation-specific therapy. We also review KIT/PDGFRA-wild-type GISTs, including succinate dehydrogenase (SDH)-deficient, neurofibromin 1 (NF1)-associated, B-Raf proto-oncogene (BRAF)-mutant, and neurotrophic tyrosine receptor kinase (NTRK)-rearranged subtypes, where extended molecular testing is increasingly important. Surgery remains central in localized disease, but operative timing, extent of resection, and use of neoadjuvant therapy should be individualized according to tumour site, rupture risk, technical feasibility, and genotype. In advanced disease, sequential use of imatinib, sunitinib, regorafenib, ripretinib, and selected mutation-specific agents reflects evolving resistance biology and the need for ongoing molecular interpretation. Emerging tools such as broader genomic profiling and liquid biopsy may further refine treatment selection. GIST therefore demonstrates that precision oncology is most effective when molecular diagnostics, surgery, systemic therapy, and multidisciplinary decision-making are integrated across the full disease course.
Gastrointestinal stromal tumours (GISTs) are the clearest solid-tumour model of precision oncology because diagnosis, prognosis, and treatment are strongly shaped by molecular genotype. The discovery of activating mutations in KIT proto-oncogene receptor tyrosine kinase (KIT) and platelet-derived growth factor receptor alpha (PDGFRA) transformed management by enabling genotype-directed use of tyrosine kinase inhibitors (TKIs) across localized and advanced disease. This review summarizes how molecular classification informs contemporary GIST care, from diagnostic work-up and risk stratification to neoadjuvant, adjuvant, and metastatic treatment planning. KIT exon 11 mutations generally predict sensitivity to standard-dose imatinib, whereas KIT exon 9 tumours may benefit from dose escalation. PDGFRA D842V confers primary resistance to imatinib but sensitivity to avapritinib, illustrating the clinical value of mutation-specific therapy. We also review KIT/PDGFRA-wild-type GISTs, including succinate dehydrogenase (SDH)-deficient, neurofibromin 1 (NF1)-associated, B-Raf proto-oncogene (BRAF)-mutant, and neurotrophic tyrosine receptor kinase (NTRK)-rearranged subtypes, where extended molecular testing is increasingly important. Surgery remains central in localized disease, but operative timing, extent of resection, and use of neoadjuvant therapy should be individualized according to tumour site, rupture risk, technical feasibility, and genotype. In advanced disease, sequential use of imatinib, sunitinib, regorafenib, ripretinib, and selected mutation-specific agents reflects evolving resistance biology and the need for ongoing molecular interpretation. Emerging tools such as broader genomic profiling and liquid biopsy may further refine treatment selection. GIST therefore demonstrates that precision oncology is most effective when molecular diagnostics, surgery, systemic therapy, and multidisciplinary decision-making are integrated across the full disease course.
DOI: https://doi.org/10.37349/etat.2026.1002378
This article belongs to the special issue Precision Oncology: Molecular Classification, Efficacy Prediction, and Treatment Decision-Making
Aim:
The aim of this multicenter study was to assess patient characteristics and short-term survival outcomes of first-line (1L) enfortumab vedotin plus pembrolizumab (EVP) as compared with conventional chemotherapy in locally advanced or metastatic urothelial carcinoma (la/mUC).
Methods:
The database included 642 patients with la/mUC diagnosed between January 2008 and December 2025 at 12 collaborating hospitals. Baseline characteristics and follow-up data, including overall and organ-specific objective tumor response according to the RECIST v1.1, progression-free survival, and duration of response, were compared among the 1L regimens. Treatment-related adverse events (TRAEs) were graded according to the CTCAE v5.0 in patients treated with 1L EVP.
Results:
The objective response and disease control rate were higher with 1L EVP than with chemotherapy (66% vs. 42% and 83% vs. 68%, respectively). The organ-specific response rate for liver metastatic lesions was 85%. Median progression-free survival (95% confidence interval) for 1L EVP, gemcitabine plus cisplatin, and gemcitabine plus carboplatin was 14.5 months (10.5–not determined), 10.5 months (8.4–13.3), and 9.2 months (6.7–14.2), respectively. In the safety analysis set including 40 patients, all-grade TRAEs occurred in 36 (90%) patients, including grade 1–2 events in 30 (75%) and grade 3–4 toxicities in 6 (15%). Grade 3–4 TRAEs included skin toxicity (7.5%), anorexia (5.0%), anemia (5.0%), gastrointestinal disorders (2.5%), renal dysfunction (2.5%), and interstitial lung disease (2.5%). The median number of administered EV cycles was 4 (range, 1–13), 5 (2–13), and 10 (4–13) in the overall, responder, and complete-response populations, respectively. EV dose modifications and interruptions were frequent in the initial 2 months but rare thereafter.
Conclusions:
This multicenter study provides real-world evidence on short-term outcomes and safety with 1L EVP, highlighting its impact on the evolving treatment landscape for la/mUC.
Aim:
The aim of this multicenter study was to assess patient characteristics and short-term survival outcomes of first-line (1L) enfortumab vedotin plus pembrolizumab (EVP) as compared with conventional chemotherapy in locally advanced or metastatic urothelial carcinoma (la/mUC).
Methods:
The database included 642 patients with la/mUC diagnosed between January 2008 and December 2025 at 12 collaborating hospitals. Baseline characteristics and follow-up data, including overall and organ-specific objective tumor response according to the RECIST v1.1, progression-free survival, and duration of response, were compared among the 1L regimens. Treatment-related adverse events (TRAEs) were graded according to the CTCAE v5.0 in patients treated with 1L EVP.
Results:
The objective response and disease control rate were higher with 1L EVP than with chemotherapy (66% vs. 42% and 83% vs. 68%, respectively). The organ-specific response rate for liver metastatic lesions was 85%. Median progression-free survival (95% confidence interval) for 1L EVP, gemcitabine plus cisplatin, and gemcitabine plus carboplatin was 14.5 months (10.5–not determined), 10.5 months (8.4–13.3), and 9.2 months (6.7–14.2), respectively. In the safety analysis set including 40 patients, all-grade TRAEs occurred in 36 (90%) patients, including grade 1–2 events in 30 (75%) and grade 3–4 toxicities in 6 (15%). Grade 3–4 TRAEs included skin toxicity (7.5%), anorexia (5.0%), anemia (5.0%), gastrointestinal disorders (2.5%), renal dysfunction (2.5%), and interstitial lung disease (2.5%). The median number of administered EV cycles was 4 (range, 1–13), 5 (2–13), and 10 (4–13) in the overall, responder, and complete-response populations, respectively. EV dose modifications and interruptions were frequent in the initial 2 months but rare thereafter.
Conclusions:
This multicenter study provides real-world evidence on short-term outcomes and safety with 1L EVP, highlighting its impact on the evolving treatment landscape for la/mUC.
DOI: https://doi.org/10.37349/etat.2026.1002379
This article belongs to the special issue Emerging Innovation in Surgical and Medical Approaches on the Horizon for Urogenital Malignancies
