Systematic Review
Systematic Review

Affiliation:
1Unit of Pediatric Pulmonology, Clínica MEDS, Santiago 7690000, Chile
2Centro del Desarrollo MEDICOP, Santiago 7591047, Chile
Email: alberto.vidal@meds.cl
ORCID: https://orcid.org/0000-0002-8819-9127
Affiliation:
2Centro del Desarrollo MEDICOP, Santiago 7591047, Chile
3Unit of Child and Adolescent Psychiatry Clínica MEDS, Santiago 7690000, Chile
ORCID: https://orcid.org/0009-0000-3608-067X
Explor Asthma Allergy. 2026;4:1009115 DOI: https://doi.org/10.37349/eaa.2026.1009115
Received: November 30, 2025 Accepted: February 11, 2026 Published: March 09, 2026
Academic Editor: Pasquale Caponnetto, University of Catania, Italy
The article belongs to the special issue Asthma and its Relationship with Psychological and Psychopathological Factors
Background: Adolescence is a vulnerable and constantly changing stage of life. Experiencing chronic illnesses such as bronchial asthma during this period can lead to heightened physical, psychological, and social problems in addition to the wide scope of challenges that coincide with the stage. The objective of this research was to identify risk and protective factors for mental health disorders, as well as the preventive and treatment strategies recommended to preserve mental health in adolescents with asthma (AA).
Methods: A search was conducted in Medline, Web of Science, EBSCO Host, PsycINFO, ScienceDirect, and Scopus for articles published in English between 2020 and 2025 using the following search terms: i) asthma in adolescents and ii) psychosocial or emotional problems. The items were checked using the PRISMA checklist.
Results: Thirty-eight articles were found: eight on mental health problems, fourteen on biopsychosocial risk factors, ten on biopsychosocial protection factors, and six on biopsychosocial interventions in AA.
Discussion: Internalizing problems such as anxiety and depression, or externalizing problems such as attention deficit hyperactivity disorder (ADHD) or conduct disorders, are prevalent in AA. Several biopsychosocial risk factors, both individual and familial, have been identified as being related to mental health problems in AA. Protective biopsychosocial factors have also been found in AA, such as certain personal characteristics, family types or structures, friends, or schoolmates. Prevention or treatment strategies for mental health problems in AA should consider a personalized approach, taking into account the family system, friendships, and the school environment.
The WHO defines adolescence as the stage of life between 10 and 19 years of age, during which young people experience significant physical, cognitive, and psychosocial changes [1]. Currently, the adolescent population consists of 1.3 billion, representing 16% of the world’s populace [2]. Chronic diseases or conditions are present in 10% to 30% of adolescents, and their treatment requires multidisciplinary interventions addressing biological, psychological, and sociocultural aspects [3]. Bronchial asthma is one of the most common chronic diseases in adolescence, reaching a global prevalence of 7.9% among 13- and 14-year-olds [4]. Additionally, one in seven adolescents suffers from mental health problems [5]. The most common being anxiety and depressive disorders (up to 40%), followed by behavioral disorders (20.1%) and attention deficit hyperactivity disorder (ADHD) (19.5%) [6]. Further, young people with chronic diseases that affect physical health, such as asthma or others, suffer more frequently from anxious-depressive symptoms in early and middle adolescence than those without these comorbidities [7, 8]. It has also been shown that adolescents with chronic conditions experience a cumulative risk of mood, anxiety, and behavioral disorders due to the physical limitations caused by the disease [9]. In pediatric asthma, mental health comorbidities such as anxiety, depression, or ADHD have been associated with low levels of treatment adherence, more medical consultations, poor disease control, and alterations in quality of life [10, 11]. Furthermore, it has been shown that the COVID-19 pandemic caused greater psychological stress and alterations in the quality of life in AA compared to their healthy peers [12, 13]. Despite the great advances in pediatric and adolescent respiratory medicine, it is still quite common for specialists to treat adolescent asthma with an eminently biomedical approach, focusing more on the disease than on the patient and relegating psychosocial aspects to the background, which is perceived by patients and their families as dehumanized medicine [14]. Considering the aforementioned, it is necessary to identify the biopsychosocial risk, protective factors, and the recommended preventive strategies to preserve the mental health of adolescents with asthma (AA).
A review of the scientific evidence on psychosocial problems in adolescent asthma was conducted between October and November 2025. Studies published in English within the last five years (2020–2025) were collected from various scientific databases (PubMed, Medline, Web of Science, EBSCO Host, PsycINFO, ScienceDirect, Scopus, and Google Scholar). Two phrases were used for the search: i) asthma in adolescents and ii) psychosocial or emotional problems. Controlled studies, follow-up cohorts, intervention studies, and systematic reviews were included. The items were checked using the PRISMA checklist. Each study was assessed by the two authors of this review. Duplicate studies, studies with patients under 10 years of age or over 21 years of age, or studies that did not clearly show their results were excluded.
Of the 285 records reviewed, 38 were ultimately included in the review (Figure 1). The retrieved articles were divided into four topics: eight in mental health problems, fourteen in psychosocial risk factors, ten in protective psychosocial factors, and six in preventive and treatment strategies.
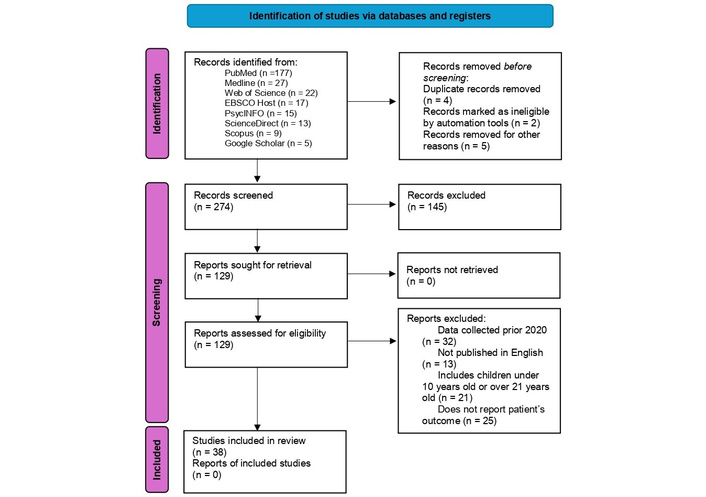
Flow diagram of the screening process. Adapted from [94]. © 2021 The Author(s). Licensed under CC BY 4.0.
Mental health problems in adolescents can be divided into two groups: internalizing, which have to do with symptoms that occur in the inner world of the person, often silent, that do not disturb the environment, and externalizing, which are disruptive, maladaptive, or even violent behaviors that frequently disturb or alter their family, school, and social environment [15, 16]. It has been shown that, in adolescence, internalizing problems are more common in women and externalizing problems in men, with different trajectories according to gender and neurodevelopment [17]. A study conducted on AA and their parents reported a significant association with internalizing problems and peer relationship difficulties [18]. Moreover, a study conducted in South America with a large number of patients showed that AA had common mental disorders (anxiety or depression) comorbidities at a higher frequency than those without asthma [19]. Anxiety can increase with the severity of asthma in adolescents, with prevalences of up to 60% reported in severe asthma [20]. AA may have more panic attacks than those without asthma, a risk that increases to almost five times if smoking is added as a comorbidity [21]. Furthermore, it has been reported that AA have worse scores on self-esteem scales than healthy controls [22]. It has also been documented that AA exposed to high levels of stress may experience more depression than those not exposed to stress [23]. A recent study conducted in Asia reported that adolescents with current or previous asthma have up to twice the risk of suicide compared to controls without asthma [24]. Externalizing problems frequently found in AA include attention problems and behavioral problems [25]. Table 1 summarizes the most frequent mental health problems in AA, and Table 2 shows characteristics of the main studies on internalizing and externalizing problems.
Mental health problems in adolescents with asthma.
| Internalizing | Externalizing |
|---|---|
| Anxiety | Behavioral disorders |
| Depression | ADHD |
| Panic attack | Peer relationship problems |
| Specific phobia | |
| Low self-esteem | |
| Somatic complaints |
ADHD: attention-deficit hyperactivity disorder.
Characteristics of the main studies on internalizing and externalizing problems.
| First author [reference] | Participants (n/age range) | Main findings |
|---|---|---|
| Keller et al. [18] | 937 adolescents between 11 and 18 years old | Parents of AA reported a significantly higher percentage of internalizing problems and peer relationship problems (p = 0.022 and 0.001, respectively), while the AA self-report was only significant in peer relationship difficulties (p = 0.004). |
| Felix et al. [19] | 66,567 students between 12 and 17 years old | AA had a significantly higher prevalence of common mental disorders (anxiety or depression) than those without asthma (p < 0.00001). |
| Licari et al. [20] | 40 AA aged 12 to 17 years | Anxiety rates sustained at 60% within a group of adolescents with severe asthma. Furthermore, depression was only found in adolescents who had both asthma and comorbid anxiety. |
| Wu et al. [21] | 162,766 adolescents between 11 and 16 years old | Patients with asthma had a higher risk of panic disorder than those without asthma (aHR: 1.70), a risk that increased in those who started smoking early (aHR: 4.95). Patients who were hospitalized or visited in the emergency department also had a higher risk of panic disorder (aHR: 2.07). |
| Valero-Moreno et al. [22] | 450 adolescents between 12 and 16 years old | AA had lower averages on the self-esteem scale than their healthy peers (p ≤ 0.001). |
| Park et al. [23] | 57,303 students aged 12 to 18 | AAs who experienced a significant degree of stress were 9 times more likely to have depression (p < 0.001) than adolescents not exposed to stress. |
| Chen et al. [24] | 153,526 adolescents between 11 and 16 years old | The suicide HR was higher in adolescents with current or previous asthma than in those without asthma (HR = 1.95 and 2.01, respectively). |
| Azzi et al. [25] | 604 teenagers between 12 and 18 years old | AA had more somatic complaints (p < 0.001), attention problems (p = 0.032), and behavioral problems (p = 0.025) than those who were not asthmatic. |
AA: adolescents with asthma; aHR: adjusted hazard ratio; HR: hazard ratio.
Resilience can be affected in adolescent asthma regardless of its degree of control [26]. Asthmatic adolescents with anxiety have been shown to be up to twice as likely to be hospitalized in an intensive care unit compared to those without anxiety [27]. It has also been reported that AA and anxiety have worse health status and lower levels of family resilience than only AA [28]. Anxiety and depression have both been shown to be related to poor asthma control in adolescents [29, 30]. In addition, asthmatic adolescents with poor adherence to controller treatment have up to nine times the risk of depression when compared to those with good adherence [31]. In AA, concern about their symptoms and the degree of emotional distress caused by such are correlated with worse outcomes in their quality of life [32]. It has also been shown that adolescent girls with more severe asthma and who are overweight have fewer skills in making and maintaining friendships than boys with mild asthma and who are not overweight [33]. Moreover, ADHD symptoms in AA have been associated with underperception of respiratory symptoms, maladaptive beliefs about asthma, and loss of treatment adherence, leading to higher emergency room visits due to asthma attacks [34, 35]. Furthermore, it has been reported that AA has a higher prevalence of short nighttime sleep (less than 7 hours) than healthy controls [36]. Sleep disturbances in adolescents are related to uncontrolled asthma, drowsiness, fatigue, and problems in self-management of their asthma that influence adherence to treatment and self-perception of symptoms [37]. Rurality, water pipe smoking, somatic complaints, and behavioral problems have been linked to poor asthma control in adolescents [38]. Parents who have problems coping with parenting or managing the stress caused by their adolescent children's asthma may negatively influence the development of the skills their children need to establish friendships with their peers [33]. Parents of AA who express discouragement, depression, or negative thoughts regarding the treatment and evolution of their children’s asthma negatively influence their health status [39]. Table 3 shows the main characteristics of studies on biopsychosocial risk factors, and Figure 2 shows the impact of biopsychosocial risk factors (individual and family) on AA.
Characteristics of the main studies on biopsychosocial risk factors.
| First author [reference] | Participants (n/age range) | Main findings |
|---|---|---|
| Ciprandi et al. [26] | 87 AA between 12 and 18 years old | Low scores were found on the resilience scale: 61 in controlled AA, 62 in partially controlled AA, and 60 in uncontrolled AA (p = 0.97). |
| Castiblanco et al. [27] | 197 rural adolescents between 12 and 17 years old | AA suffering anxiety had a slightly more than double the risk of being hospitalized in an intensive care unit (OR = 2.09), and an increase of one point on the anxiety scale increased the risk of hospitalization in intensive care for asthma symptoms by 5%. |
| Nabors et al. [28] | 20,723 adolescents between 12 and 17 years old | Those with asthma and comorbid anxiety had a higher risk of having low family resilience scores (aOR 1.7 vs. 1.09) and worse health status (aOR 19.6 vs. 3.14) than those with asthma alone. |
| Licari et al. [29] | 87 AA between 12 and 18 years old | Compared to the controlled AA, the uncontrolled AA had a significantly higher percentage of elevated anxiety index (p = 0.043) and a higher depression score (p = 0.013). |
| Patel et al. [30] | 197 AA between 13 and 19 years old | Depressive symptoms as measured by scales were significantly associated with poor asthma control as measured by ACT (p = 0.001). |
| Naveen et al. [31] | 102 AA | AA have a higher risk of depression as their adherence to treatment worsened: intermediate adherence (aOR = 7.09, p = 0 0.01), poor adherence (aOR = 9, p = 0.01). |
| Kosse et al. [32] | 243 AA between 12 and 18 years old | The quality of life reported in AA had a good correlation with identity (r = –0.66; p < 0.001), with concern about the disease (r = –0.64; p < 0.001), and emotional representation (r = 0.63; p < 0.001). |
| Workman et al. [33] | 1,812 AA between 12 and 17 years old | AA and allergies, behavioral problems, BMI > 85, or moderate to severe asthma had a higher risk of making and maintaining friendships than those without these conditions (OR = 4.71, 4.65, 1.4, and 1.19, respectively). Adolescents whose parents had problems coping with parenting or were exposed to stress were also at greater risk of making and maintaining friendships (OR = 5.72 and 3.6, respectively). |
| Fruchter et al. [34] | 296 AA and their parents between 10 and 17 years old | AAs and their parents who reported ADHD symptoms had a greater underperception of asthma symptoms (p = 0.04 and p = 0.02, respectively), as well as maladaptive beliefs regarding asthma (p < 0.001 for both). |
| Silverstein et al. [35] | 302 AA between 10 and 17 years old | AA, who had more ADHD symptoms, showed worse adherence to control medication and indirectly had more emergency room visits (p = 0.002 and 0.02, respectively) |
| Estanislau et al. [36] | Data from 59,442 adolescents between 12 and 17 years old | The prevalence of asthma was higher in adolescents with short nighttime sleep (< 7 hours), common mental disorders, and excess weight (p = 0.03, p < 0.0001, and p = 0.03, respectively). |
| Evans et al. [37] | 33 with uncontrolled AA between 12 and 15 years old and their caregivers | 42% of AA and caregivers reported nighttime symptoms that caused awakenings. Asthma sufferers reported that sleep disturbances are a barrier to asthma self-management. 27% of caregivers reported distress due to their children’s nighttime asthma symptoms. |
| Azzi et al. [38] | 202 adolescents between 12 and 18 years old | Living in a rural area, smoking water pipes, somatic complaints, and behavioral problems were associated with asthma control problems in adolescents (p = 0.018, 0.017, 0.005, and 0.038, respectively). |
| Dut et al. [39] | 204 adolescents between 12 and 21 years old and their parents | Parental depression and somatization were associated with psychiatric problems in adolescents (p = 0.04 and 0.02, respectively). Parental anxiety, negative parental self-esteem, and parental somatization were associated with somatization in adolescents (p = 0.04, 0.03, and 0.003, respectively). |
AA: adolescents with asthma; ACT: asthma control test; ADHD: attention deficit hyperactivity disorder; BMI: body mass index; OR: odds ratio; r: correlation coefficient.
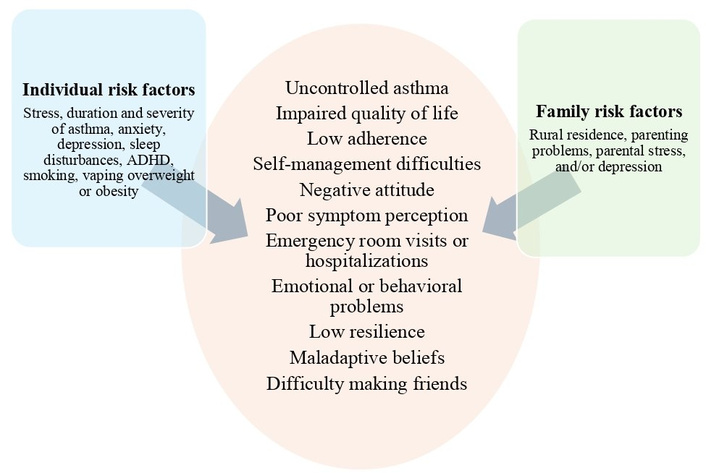
Biopsychosocial risk factors and their impact on adolescents with asthma. ADHD: attention deficit hyperactivity disorder.
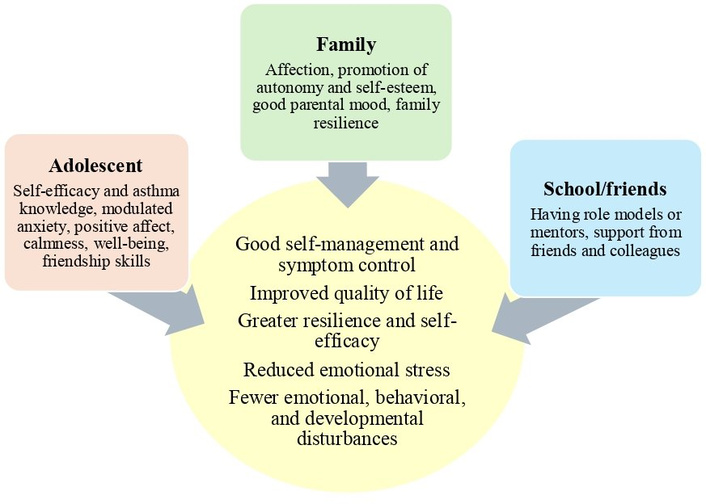
Knowledge and self-efficacy are considered protective factors in AA. Knowledge of the disease is useful and important in managing acute symptoms, which require a reactive approach (e.g., an asthma attack). However, self-efficacy is a more complex process that requires planning with an anticipatory focus and clear objectives, allowing the use of knowledge to prevent symptoms and support asthma self-control [40]. Both conditions have been linked to increased responsibility, better self-care, and quality of life in AA, and it is the duty of parents and health professionals to develop interventions to maintain and/or improve them [41]. Another factor that influences the care of AA is anxiety, which, at moderate levels, could be modulated by self-efficacy, to allow the adolescent to improve symptom prevention and self-care [42]. Positive affect in AA, and some of its components, such as vigor or vitality, well-being, happiness or satisfaction, and calmness, have been shown to reduce the psychological consequences of emotional stress [43]. Sleep hygiene is another factor that has been considered protective in adolescents, since those who have better sleep quality have better quality of life and attention at school [44]. Some family characteristics, such as the parents’ good mood or less psychological control, have been proposed as factors that favor the quality of life in AA [45, 46]. The ability to make and maintain friendships is associated with better personal development in the asthmatic adolescent, which in turn favors their resilience [47]. AAs who have mentors or who maintain good friendships with their peers have fewer emotional, behavioral, or developmental problems [48]. AAs who have peer support have better self-efficacy skills, which translates into better outcomes in their disease [49]. Table 4 shows the main characteristics of studies on protective biopsychosocial factors, and Figure 3 shows the benefit of biopsychosocial protective factors in AA.
Characteristics of the main studies on protective biopsychosocial factors.
| First author (reference) | Participants (n/age range) | Main findings |
|---|---|---|
| Leonard et al. [40] | 198 uncontrolled AA between 14 and 19 years old | In the AA, knowledge was significantly associated with disease prevention (p = 0.001) and self-efficacy (p < 0.001). |
| Sleath et al. [41] | 359 AA between 11 and 17 years old | The AAs with better levels of self-efficacy had higher levels of responsibility (p < 0.001), better control (p < 0.05), and better levels of quality of life (p < 0.001) related to the disease. |
| Turi et al. [42] | 197 AA between 13 and 19 years old | AA and anxiety were notably associated with the prevention of onset symptoms and mangagement the illness when presented, an effect which became less significant with higher levels of anxiety. AA with moderate generalized anxiety (not mild or severe) was associated with better management of existing symptoms, but not with better prevention of them. |
| Jenkins et al. [43] | 66 AA between 12 and 17 years old | In the AA, positive affection moderated the association between stress and asthma control (p = 0.009) and the association between psychological triggers and asthma control (p = 0.007). Calmness moderated symptom severity and stress (p = 0.036) and psychological triggers (p = 0.021). |
| Lawless et al. [44] | 41 AA between 13 and 17 years old | The AA with better sleep hygiene had better HRQL (p = 0.04) and attention for longer (p = 0.04) at school. |
| Valero-Moreno et al. [45] | 150 AA between 12 and 16 years old | The best parental mood had a positive effect on self-esteem (p < 0.01), a negative effect on the perception of threat to the disease (p < 0.05), and a positive effect on the quality of life (p < 0.01) of the AA. |
| Valero-Moreno et al. [46] | 150 AA between 12 and 16 years old | AAs who had parents with better moods or who were subjected to less psychological control had a better quality of life. |
| Nabors et al. [47] | 1,523 AA between 12 and 17 years old | AA with behavioral problems, anxiety, or depression, who reported fewer problems making and keeping friends, were more likely to have better personal development (p < 0.001 for all comparisons). |
| Nabors et al. [48] | 2,589 AA between 10 and 17 years old | AA members who had mentors and friendship skills had more family resilience (p < 0.01 for both variables). Young people with few or no problems making friends had fewer emotional and developmental problems and were less likely to seek emergency care (p < 0.01 for all variables). |
| Schacter et al. [49] | 440 AA between 14 and 21 years old | AA with better peer support had greater self-efficacy in managing their asthma, lower frequency of anxiety and depression (p < 0.00 for all comparisons). |
AA: adolescents with asthma; HRQL: health-related quality of life.
A study showed that AA who participated in 5 motivational interview sessions lasting 80 to 90 minutes had better levels of self-efficacy and treatment adherence than adolescents who were not interviewed [50]. AAs have been shown to perceive mobile action plans that provide real-time feedback to health professionals positively, because they allow them to improve their knowledge and self-management of asthma [51]. Face-to-face and online education through short videos has been well evaluated by asthmatic adolescents, their caregivers, and schoolmates [52]. Vigorous physical activity of at least 20 minutes three times a week has been shown to significantly decrease stress in AA [53]. The preparation stage for the transition of asthma from adolescence to adulthood is a multidimensional, frequently asynchronous process that depends heavily on gender, the degree of self-management of asthma, communication with health professionals, and access to health [54]. In asthmatic adolescents, hybrid educational interventions (face-to-face/online) have been shown to improve their readiness and self-efficacy for the transition [55]. Table 5 shows the characteristics of the main studies on biopsychosocial interventions, and Table 6 shows a summary of the biopsychosocial aspects that should be considered in the management of AA.
Characteristics of the main studies on biopsychosocial interventions.
| First author (reference) | Participants (n/age range) | Main findings |
|---|---|---|
| Taheri et al. [50] | 72 AA between 10 and 15 years old | The AA group that participated in the interviews recorded better levels of self-efficacy at two weeks and three months (p < 0.001 in both periods), and also better adherence at two weeks and three months (p = 0.006 and 0.04, respectively), than the control group. |
| He et al. [51] | 13 AA between 12 and 20 years old | The mobile application on the AA’s smart phones was measured by the average usability score, which reached 83 out of a total of 100 for the whole group, especially the older ones (12 to 16 years = 77.5 and ≥ 17 years = 87.5 points). |
| Gardiner et al. [52] | 151 adolescents between 13 and 15 years old | After watching the short three-minute educational video, the young people significantly improved their asthma knowledge in at least four of the six questions asked (question 1, p < 0.01; question 2, p = 0.02; questions 5 and 6, both with p < 0.01). |
| Kong et al. [53] | 57,703 adolescents between 11 and 18 years old | AAs who performed vigorous physical activity (at least 20 minutes more than 3 times per week) had less stress than AAs who did not (p < 0.05). |
| Rhee et al. [54] | 39 AA between 16 and 20 years old | AAs who were best prepared for the transition to adult asthma were the older ones (16–17 years vs. 18–20 years, p = 0.07). Older AA also had better appointment keeping and better follow-up of health problems (p = 0.002 and 0.02, respectively). Female AA had better medication management (p = 0.04), and those with better-controlled asthma communicated more with healthcare providers (p = 0.02). |
| Dinç et al. [55] | 52 AA between 14 and 18 years old | The AAs who underwent a hybrid educational intervention had significantly higher scores on the transition readiness (p < 0.001) and self-efficacy (p < 0.01) questionnaires than the AAs who did not undergo the intervention. |
AA: adolescents with asthma.
Biopsychosocial aspects in adolescents with asthma.
| Adolescent | Family and friends | School |
|---|---|---|
| Prevention, recognition, and management of mental health problems such as anxiety disorders, anxiety-depressive disorders, phobias, ADHD, and behavioral disorders | Parental education programs to improve the level of knowledge and self-confidence in managing their children’s asthma | Promote school participation and positive friendships |
| Education and development of cognitive/behavioral skills | Parenting programs for managing the difficulties in raising children and the stress caused by their adolescent child’s asthma | Conduct peer mentoring interventions so that newly diagnosed asthmatics can connect with experienced asthmatic peers |
| Recognition of preventive factors for mental health problems, such as resilience | Promoting positive affection from family and friends towards the adolescent with asthma | Training for schoolmates, school nurses, and physical education teachers on asthma and its implications |
| Regulation of risky or uncontrolled behaviors | Exploration of family resilience and modification of negative family behaviors towards the asthmatic adolescent | |
| Education and periodic review of the level of knowledge about asthma, perception of symptoms, and adherence to treatment (face-to-face, online videos, smartphones, or tablets) | Treatment of mental health conditions in family members living with the adolescent | |
| Promoting autonomy, self-efficacy, self-management, and responsibility | ||
| Identifying and improving difficulties in establishing friendships among peers | ||
| Promotion and supervision of physical activity, aerobic and recreational exercise | ||
| Complementary therapies for stress and anxiety management, such as yoga or mindfulness |
ADHD: attention-deficit hyperactivity disorder.
This study compiled the scientific evidence supporting the association between mental health problems and AA, identifying psychosocial risk and protective factors for emotional or behavioral disturbances in adolescents, as well as some preventative strategies that could be implemented at this age. The causes of the interaction between asthma and mental health problems are still unknown; however, advances in the study of the human genome have made it possible to find new genes common to asthma, anxiety, depression, and ADHD [56]. In particular, the bidirectional relationship between asthma and depression has been the subject of increasing studies in recent years. Major depressive disorder has been shown to be a predisposing factor for the development of asthma through mechanisms that are still unknown, which could include certain biological pathways of the nervous, endocrine, or immune systems, as well as unhealthy lifestyle factors such as smoking or a lack of concern for personal health [57]. Furthermore, it has been documented that asthmatics have a higher prevalence of depression than the general population, which may be influenced by the patients’ gender, family characteristics, the duration and degree of physical impairment caused by asthma [58]. The interaction between asthma and anxiety is also complex in adolescents and can develop even before adolescence [59]. Anxiety in asthma can have a dual effect; if it is mild to moderate, it can help with self-care and treatment adherence, but if it is severe or generalized, it can have a negative impact on asthma control [60]. Panic attacks were also frequently found in AA, especially among those who smoke. Emergency room physicians and respiratory specialists often see AA who present symptoms that could be classified as panic attacks. The cause of panic attacks in asthma is not yet fully understood, but it is believed that they may be mediated by learning about interoceptive threats (e.g., fear of suffocation), especially in contexts perceived as unpredictable or unsafe by patients [61]. ADHD is another frequent comorbidity in asthma in children and adolescents, with prevalences that fluctuate between 7 and 12%, depending on the geographical area studied [62, 63]. AA should gradually assume responsibility for managing their controller medication. When they also have ADHD, they may have difficulty adhering to controller treatment routines, risking treatment discontinuation. This group requires close monitoring by their physicians, school nurses, and parents to ensure treatment compliance without hindering the development of the independence skills necessary for transitioning from both conditions into adulthood [64]. Stress associated with asthma in adolescents is a factor that has been shown to trigger mental health problems. Chronic stress and asthma duration have been reported as individual risk factors that affect resilience in asthmatic adolescents [65]. Asthmatic adolescents exposed to chronic stress at an individual, community, or family level may experience direct and indirect effects, which may lead to poor outcomes in their asthma [66]. The severity of asthma can negatively affect adolescents, causing social isolation, feelings of shame, brought on by teasing, bullying, and conflicts with their parents [67]. Risky behaviors of adolescence can also affect asthmatics. A recent study showed that adolescents (with and without asthma) who report respiratory symptoms have an increased risk of having used tobacco, nicotine vaping, or cannabis in the past month, the past 6 months, and throughout their lifetime [68]. This is particularly worrying in AA, in whom these substances have been shown to negatively affect disease control and quality of life [69]. Stress or mental health problems in parents were another factor found to be related to emotional disturbances in AA. Some adverse experiences in AA, such as parental separation/divorce or financial difficulties, are considered family biopsychosocial risk factors, which can increase the likelihood of having emotional or behavioral problems almost twofold if they occur separately and up to fourfold if they occur simultaneously [70]. Rurality is another factor that has been shown to be related to emotional problems in AA. Living with a single parent or in rural environments worsens the emotional state of AA, as this causes them to have more negative attitudes towards their illness [71]. The effect of rurality could increase the social isolation that is already present in the AA.
This review also identified biopsychosocial protective factors at the personal, family, school, and peer levels. Recognizing and addressing these factors is crucial for preventing emotional problems and requires treating physicians to dedicate additional time during consultations or to rely on asthma educator nurses within the hospital or school system. Furthermore, it is necessary to specify that professionals working with AA must have knowledge and training in topics specific to this stage of life, such as independence, close peer relationships, identity development, risk behaviors, and social networks [72]. The integrated healthcare model for chronic illness in children and adolescents requires a collaborative, multidisciplinary team focused on educating and supporting both the patient and their family, involving the school system and friends. In this model, it is increasingly important for pediatric pulmonologists to have basic knowledge of mental health, as well as ongoing support and contact with child and adolescent psychiatrists and psychologists [73].
The interventions that met the review criteria demonstrate that motivational interviews, short educational videos, hybrid education (face-to-face/online), mobile technology on phones or tablets, and physical activity have a positive impact on the health of the AA. Other interventions that have been reported as beneficial in both children and adolescents include educational programs and cognitive-behavioral skills enhancement programs, which aim to achieve greater knowledge and self-efficacy in emotional disorders [74]. Psychological interventions in the treatment of anxiety/depression have also been shown to be useful in reducing asthma symptoms or attacks and improving adherence to medication [75]. A recent meta-analysis reported that psychosocial interventions are beneficial for children and adolescents without adverse effects; however, the studies analyzed showed clinical variability and small sample sizes [76]. It has also been shown that some interventions, such as yoga or mindfulness, can be used to reduce stress and anxiety, as well as to improve the quality of life of asthma in children and adolescents [77]. The perception of the disease and its symptoms is a personal construct that involves cognition and emotion; Therefore, stimulating a positive perception towards the disease and educating about treatment beliefs can lead to better disease control and a better quality of life [78]. A recent study showed that AA who used peak expiratory flow with a feedback scheme of values were able to achieve better perception of their symptoms, higher levels of expiratory volume in the first second, and adherence, than those who did not use it [79]. At this age, treatment adherence can be impaired when parents stop supervising, and the adolescent forgets to administer it, or because the adolescent does not want to be treated since they feel stigmatized or ashamed, or when they have mental health comorbidities (anxiety, depression), or due to tobacco, vaping, or marijuana use [80]. Intentional loss of treatment adherence can be improved with motivational interviews and interventions to improve emotional state, while in unintentional loss of adherence, strategies that leverage technology, such as “mobile health”, which uses tablets or smartphones to improve self-management in AA, are recommended [81]. Mobile health enables AA to improve self-care, treatment adherence, and learn about action plans for symptom management [82]. It has recently been reported that mixed interactive technology (augmented reality, virtual reality, or holographic technology) could be a useful tool for AA and emotional problems. However, it should be combined with face-to-face care, and individualized assessments should be made of adolescents who would benefit most from this therapy [83]. Text messaging via cell phones is a technological tool that has proven to be effective in caregivers of adolescent asthmatics, allowing them to improve their knowledge and management of their children’s asthma [84, 85]. Physical activity has benefits for AA, helping them feel better, achieve a better connection with their parents and friends, as well as improve their skills in managing asthma [86]. It has also been shown that game-based physical activity programs for AA can help keep them motivated, reducing social barriers such as embarrassment or the inability to keep up with their peers during conventional exercise [87]. Additionally, pulmonary rehabilitation is considered a non-pharmacological intervention shown to improve the quality of life and pulmonary function of asthmatic children and adolescents [88–90]. The transition from adolescent to adult asthma is complex—it is a difficult stage for the patient and their family, during which it is recommended to identify negative emotions regarding the disease, address the adolescents’ concerns or anxieties, often in one-on-one sessions with the patients, establishing a relationship of trust and using the best possible communication skills. The level of knowledge, adherence, effectiveness, and self-control should also be assessed, which will allow for the design of transition plans together with the parents [91]. Parents may have negative perceptions regarding the preparation for the transition of their AA, so they should receive early emotional support and education to improve the management of their children’s asthma [92]. A multidisciplinary Task Force systematically details the practical needs and resources required for pediatric and adult health professionals to address the transition of asthma during adolescence in a coordinated manner [93].
A limitation of this review is the heterogeneity of the selected studies. Although we separated them into four categories, there were differences in the number of patients and age ranges. Another of such was that most studies did not report asthma controller treatment in detail. This is important, as some neuropsychiatric symptoms are known to be related to high doses of inhaled corticosteroids, frequent or prolonged use of oral corticosteroids, or leukotriene receptor antagonists. There were also differences in the instruments used to measure mental health alterations. Some studies used anxiety/depression scales, while others used scales of self-esteem, resilience, communication, behavior, peer relationships, quality of life, etc.
As described in this review, the mental health problems that an adolescent with asthma may experience are varied and depend on their genetics, personal characteristics, life history, family background, school system, and friendships. Addressing the needs of an adolescent with these characteristics cannot and should not be done by a single person; it requires a trained, cohesive, multidisciplinary team that also gains the trust of the patient and their family.
Future research in this area should include: analyzing common genetic factors and neurobiological pathways related to emotional disturbances in AA; searching for biomarkers or designing predictive models using artificial intelligence to identify AA and their risk of mental health disorders; early assessment of the mental health of adolescents with severe asthma and ongoing monitoring; measuring the effect of non-pharmacological alternative therapies for anxiety management; designing hybrid (in-person/online) programs with a specific focus on each adolescent’s particular mental health challenges; increasing parental and school education regarding asthma and mental health comorbidities; and maintaining ongoing training and communication among multidisciplinary healthcare teams that support AA and emotional problems.
AA: adolescents with asthma
ADHD: attention deficit hyperactivity disorder
We would like to thank Maribel Garrido and Rocío Ballesteros, both assistants at the SAVAL Center, for their collaboration in the search for scientific information for the preparation of this manuscript.
AV: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Visualization, Validation, Writing—original draft, Writing—review & editing. MM: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Visualization, Validation, Writing—original draft, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
The primary data for this systematic review were sourced online from databases listed in the methods. Referenced articles are accessible on PubMed, Medline, Web of Science, EBSCO Host, PsycINFO, ScienceDirect, Scopus, and Google Scholar. Additional supporting data are available from the corresponding author upon request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 2026
Download: 37
Times Cited: 0
Amar P. Garg ... Bajeerao Patil
Graziella Chiara Prezzavento
Jim E. Banta ... James M. Banta
Nassiba Bahra ... Samira El Fakir
Silvina Monica Alvarez ... Nidia Noemi Gomez