







Aim:
Evaluate the associations between usage of the standalone SmartMoms Canada mHealth intervention, and gestational weight gain (GWG) guideline adherence and lifestyle improvements in pregnant individuals in the context of a pragmatic study.
Methods:
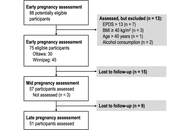
Participants (18–40 years, BMI 18.5–39.9 kg/m2) were recruited into a single-arm trial conducted in Winnipeg and Ottawa, Canada. All participants were provided with the app, a Fitbit® tracker, and a smart scale. Participants were assessed in early, mid-, and late pregnancy. Physical activity was measured with the Godin Leisure Time Exercise score, and the Fitbit® tracker (steps and time in physical activity). Fitbit® app was used to measure dietary intake. App usage and GWG were monitored. GWG guideline adherence was compared with data from the Statistics Canada Maternal Experiences Survey (MES). GWG adherence and lifestyle changes were compared between app usage groups (≥ median weekly app usage vs. < median) with multinomial logistic regressions or t tests. Trajectories in lifestyle changes were compared between groups with repeated measure analyses.
Results:
Of the 75 participants recruited in early pregnancy, 51 were followed through pregnancy (32% drop out). Overall app usage was low (median 1.30 min/wk). Adequate GWG was achieved by 35.7% (95% CI: 23.2–48.2) of participants vs. 32.6% in the MES; while excessive GWG occurred in 50.0% (95% CI: 36.9–63.1) vs. 48.7%. GWG adherence was not different between usage groups (P = 0.399), but a higher mean weekly app usage (continuous) was associated with lower odds of insufficient GWG (OR = 0.01, P = 0.035). There were no significant associations between app usage and changes in physical activity, but a lower increase in carbohydrate intake was observed in the higher usage group.
Conclusions:
Few associations were found between app usage and GWG or lifestyle outcomes. Lack of significant results could relate to low protocol and intervention adherence (Trial registration: http://www.isrctn.com/ISRCTN16254958).
Aim:
Evaluate the associations between usage of the standalone SmartMoms Canada mHealth intervention, and gestational weight gain (GWG) guideline adherence and lifestyle improvements in pregnant individuals in the context of a pragmatic study.
Methods:
Participants (18–40 years, BMI 18.5–39.9 kg/m2) were recruited into a single-arm trial conducted in Winnipeg and Ottawa, Canada. All participants were provided with the app, a Fitbit® tracker, and a smart scale. Participants were assessed in early, mid-, and late pregnancy. Physical activity was measured with the Godin Leisure Time Exercise score, and the Fitbit® tracker (steps and time in physical activity). Fitbit® app was used to measure dietary intake. App usage and GWG were monitored. GWG guideline adherence was compared with data from the Statistics Canada Maternal Experiences Survey (MES). GWG adherence and lifestyle changes were compared between app usage groups (≥ median weekly app usage vs. < median) with multinomial logistic regressions or t tests. Trajectories in lifestyle changes were compared between groups with repeated measure analyses.
Results:
Of the 75 participants recruited in early pregnancy, 51 were followed through pregnancy (32% drop out). Overall app usage was low (median 1.30 min/wk). Adequate GWG was achieved by 35.7% (95% CI: 23.2–48.2) of participants vs. 32.6% in the MES; while excessive GWG occurred in 50.0% (95% CI: 36.9–63.1) vs. 48.7%. GWG adherence was not different between usage groups (P = 0.399), but a higher mean weekly app usage (continuous) was associated with lower odds of insufficient GWG (OR = 0.01, P = 0.035). There were no significant associations between app usage and changes in physical activity, but a lower increase in carbohydrate intake was observed in the higher usage group.
Conclusions:
Few associations were found between app usage and GWG or lifestyle outcomes. Lack of significant results could relate to low protocol and intervention adherence (Trial registration: http://www.isrctn.com/ISRCTN16254958).
DOI: https://doi.org/10.37349/edht.2026.101197
Aim:
Cerebral palsy (CP) is one of the most common motor neurodevelopmental disorders, affecting approximately three in every thousand live births in North America. The study aims to investigate and identify the factors influencing manual dexterity performance among children with CP and typically developing (TD) children according to the Manual Ability Classification System (MACS) levels.
Methods:
A total of 100 children aged 4 to 12 years were enrolled, including 50 diagnosed with CP and 50 TD children. Manual dexterity performance was assessed across MACS levels. A Bayesian seemingly unrelated regression (BayesSUR) framework was applied to identify influential factors, explicitly accounting for interrelationships among multiple response variables. This probabilistic approach allowed for robust estimation under uncertainty while incorporating correlations across outcomes.
Results:
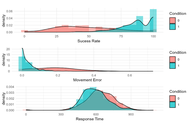
The BayesSUR analysis revealed distinct factor influences MACS levels. For children with mild CP (MACS level 1), object type had the strongest effect on response time. For moderately affected children (MACS level 2), direction most strongly influenced movement error, while age impacted both error and success rate. Among severely affected children (MACS level 3) and TD children, gender emerged as the dominant factor influencing response time. However, the low inclusion probabilities of other factors suggest that additional data and validation are warranted.
Conclusions:
The findings highlight the importance of considering both individual characteristics and task-specific factors when designing interventions to improve manual dexterity in children with CP. These results contribute to a better understanding of the key determinants influencing motor performance and may guide the development of more effective therapeutic and rehabilitation strategies. The Trial Registration Number: CTRI/2018/07/014900.
Aim:
Cerebral palsy (CP) is one of the most common motor neurodevelopmental disorders, affecting approximately three in every thousand live births in North America. The study aims to investigate and identify the factors influencing manual dexterity performance among children with CP and typically developing (TD) children according to the Manual Ability Classification System (MACS) levels.
Methods:
A total of 100 children aged 4 to 12 years were enrolled, including 50 diagnosed with CP and 50 TD children. Manual dexterity performance was assessed across MACS levels. A Bayesian seemingly unrelated regression (BayesSUR) framework was applied to identify influential factors, explicitly accounting for interrelationships among multiple response variables. This probabilistic approach allowed for robust estimation under uncertainty while incorporating correlations across outcomes.
Results:
The BayesSUR analysis revealed distinct factor influences MACS levels. For children with mild CP (MACS level 1), object type had the strongest effect on response time. For moderately affected children (MACS level 2), direction most strongly influenced movement error, while age impacted both error and success rate. Among severely affected children (MACS level 3) and TD children, gender emerged as the dominant factor influencing response time. However, the low inclusion probabilities of other factors suggest that additional data and validation are warranted.
Conclusions:
The findings highlight the importance of considering both individual characteristics and task-specific factors when designing interventions to improve manual dexterity in children with CP. These results contribute to a better understanding of the key determinants influencing motor performance and may guide the development of more effective therapeutic and rehabilitation strategies. The Trial Registration Number: CTRI/2018/07/014900.
DOI: https://doi.org/10.37349/edht.2026.101195
Aim:
To examine the behavioral signature of the “Algorithmic Self,” characterizing how users adapt their identity and behaviors in response to algorithmic reinforcement among active digital media users in Pakistan.
Methods:
A cross-sectional quantitative design was employed with 422 adults aged 18–45 years across five major cities. Participants completed a structured online questionnaire capturing demographic data, digital usage patterns, the Algorithmic Exposure Score (AES), and Algorithmic Self Behavioral Signature Scale (ASBSS). Validated instruments assessed social comparison, Fear of Missing Out (FoMO), self-esteem, and digital stress. Data were analyzed using descriptive statistics, Pearson correlations, and multiple linear regression in SPSS version 26, with significance set at p < 0.05.
Results:
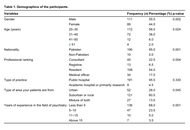
Participants demonstrated moderate-to-high levels of Algorithmic Self formation, with 39.8% classified in the high category. Higher daily screen time, greater platform diversity, stronger algorithmic trust, and elevated social comparison were associated with higher Algorithmic Self Scores. In multiple linear regression analysis, daily screen time (β = 0.34), social comparison (β = 0.31), algorithmic trust (β = 0.29), and algorithmic exposure (β = 0.28) emerged as significant predictors of Algorithmic Self formation, while FoMO was not a significant predictor (β = 0.11, p = 0.09). The final model explained 56% of the variance in Algorithmic Self formation (R2 = 0.56, adjusted R2 = 0.54, p < 0.001).
Conclusions:
AI-driven digital environments are associated with self-presentation, identity adaptation, and behavioral regulation among Pakistani users. These findings highlight the importance of enhancing digital literacy, improving awareness of algorithmic influence, and further investigating the psychological and societal implications of Algorithmic Self formation in digitally mediated environments.
Aim:
To examine the behavioral signature of the “Algorithmic Self,” characterizing how users adapt their identity and behaviors in response to algorithmic reinforcement among active digital media users in Pakistan.
Methods:
A cross-sectional quantitative design was employed with 422 adults aged 18–45 years across five major cities. Participants completed a structured online questionnaire capturing demographic data, digital usage patterns, the Algorithmic Exposure Score (AES), and Algorithmic Self Behavioral Signature Scale (ASBSS). Validated instruments assessed social comparison, Fear of Missing Out (FoMO), self-esteem, and digital stress. Data were analyzed using descriptive statistics, Pearson correlations, and multiple linear regression in SPSS version 26, with significance set at p < 0.05.
Results:
Participants demonstrated moderate-to-high levels of Algorithmic Self formation, with 39.8% classified in the high category. Higher daily screen time, greater platform diversity, stronger algorithmic trust, and elevated social comparison were associated with higher Algorithmic Self Scores. In multiple linear regression analysis, daily screen time (β = 0.34), social comparison (β = 0.31), algorithmic trust (β = 0.29), and algorithmic exposure (β = 0.28) emerged as significant predictors of Algorithmic Self formation, while FoMO was not a significant predictor (β = 0.11, p = 0.09). The final model explained 56% of the variance in Algorithmic Self formation (R2 = 0.56, adjusted R2 = 0.54, p < 0.001).
Conclusions:
AI-driven digital environments are associated with self-presentation, identity adaptation, and behavioral regulation among Pakistani users. These findings highlight the importance of enhancing digital literacy, improving awareness of algorithmic influence, and further investigating the psychological and societal implications of Algorithmic Self formation in digitally mediated environments.
DOI: https://doi.org/10.37349/edht.2026.101196
Aim:
To benchmark three deep learning-based retinal image registration methods RetinaRegNet, EyeLiner, and GeoFormer on the Fundus Image Registration (FIRE) dataset to compare registration accuracy and computational efficiency using mean landmark error (MLE) as the primary outcome measure.
Methods:
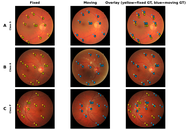
The three image registration approaches were evaluated using the FIRE dataset under consistent conditions across varying image overlap conditions (Classes S, A, and P). These included: (a) RetinaRegNet, which incorporates diffusion features, dual keypoint sampling through Scale-Invariant Feature Transform (SIFT) and random, two-stage outlier removal, and a multilevel registration hierarchy progressing from homography to polynomial transforms; (b) EyeLiner, which integrates anatomical segmentation with SuperPoint feature extraction, LightGlue matching, and thin-plate spline warping; (c) GeoFormer, which builds on Local Feature Transformers (LoFTR) through cross-attention mechanisms and Random Sampling Consensus (RANSAC)-based refinement. Registration performance was quantified using MLE.
Results:
Across all 134 FIRE image pairs, RetinaRegNet achieved the lowest overall MLE (3.12 pixels), outperforming EyeLiner (3.81 pixels) and GeoFormer (6.06 pixels). Class-specific analysis showed that RetinaRegNet delivered the highest accuracy in Class S images (1.70 pixels), competitive performance in Class A (5.24 pixels), and the strongest results in the most challenging Class P cases (4.57 pixels). GeoFormer demonstrated the shortest processing time at 0.32 seconds per image pair, compared with 4.92 seconds for EyeLiner and 31.23 seconds for RetinaRegNet. In Class P, RetinaRegNet achieved a 59.2% improvement in accuracy relative to GeoFormer (4.57 vs 11.20 pixels). The code is available at: https://github.com/ThenukaDharmaseelan/image_Registration.
Conclusions:
Overall, the evaluation reveals a clear trade-off between registration precision and computational speed. RetinaRegNet achieves the lowest MLE for complex clinical cases despite higher computational cost. EyeLiner balances precision and speed for routine use, while GeoFormer prioritizes rapid throughput where processing speed is critical.
Aim:
To benchmark three deep learning-based retinal image registration methods RetinaRegNet, EyeLiner, and GeoFormer on the Fundus Image Registration (FIRE) dataset to compare registration accuracy and computational efficiency using mean landmark error (MLE) as the primary outcome measure.
Methods:
The three image registration approaches were evaluated using the FIRE dataset under consistent conditions across varying image overlap conditions (Classes S, A, and P). These included: (a) RetinaRegNet, which incorporates diffusion features, dual keypoint sampling through Scale-Invariant Feature Transform (SIFT) and random, two-stage outlier removal, and a multilevel registration hierarchy progressing from homography to polynomial transforms; (b) EyeLiner, which integrates anatomical segmentation with SuperPoint feature extraction, LightGlue matching, and thin-plate spline warping; (c) GeoFormer, which builds on Local Feature Transformers (LoFTR) through cross-attention mechanisms and Random Sampling Consensus (RANSAC)-based refinement. Registration performance was quantified using MLE.
Results:
Across all 134 FIRE image pairs, RetinaRegNet achieved the lowest overall MLE (3.12 pixels), outperforming EyeLiner (3.81 pixels) and GeoFormer (6.06 pixels). Class-specific analysis showed that RetinaRegNet delivered the highest accuracy in Class S images (1.70 pixels), competitive performance in Class A (5.24 pixels), and the strongest results in the most challenging Class P cases (4.57 pixels). GeoFormer demonstrated the shortest processing time at 0.32 seconds per image pair, compared with 4.92 seconds for EyeLiner and 31.23 seconds for RetinaRegNet. In Class P, RetinaRegNet achieved a 59.2% improvement in accuracy relative to GeoFormer (4.57 vs 11.20 pixels). The code is available at: https://github.com/ThenukaDharmaseelan/image_Registration.
Conclusions:
Overall, the evaluation reveals a clear trade-off between registration precision and computational speed. RetinaRegNet achieves the lowest MLE for complex clinical cases despite higher computational cost. EyeLiner balances precision and speed for routine use, while GeoFormer prioritizes rapid throughput where processing speed is critical.
DOI: https://doi.org/10.37349/edht.2026.101194
This article belongs to the special issue Deep Learning Methods and Applications for Biomedical Imaging
This letter offers a critical appraisal of Riaz et al.’s study (Explor Digit Health Technol. 2026;4:101179. DOI: 10.37349/edht.2026.101179) on psychiatrists’ knowledge, perceptions, and willingness toward digital psychiatry in Pakistan. The mixed-methods design identifies critical gaps in competencies (e.g., 68.5% telepsychiatry familiarity vs. 32.5% VR) and barriers like infrastructure deficits (44.5%). However, methodological issues per STROBE guidelines such as absent response rates, convenience sampling bias, and incomplete bias mitigation limit representativeness. An adapted Newcastle-Ottawa Scale scores it 7/10, indicating moderate bias of risk from selection and non-response. Additional concerns include under-explored cultural factors. Recommendations propose a tailored LMIC digital health adoption framework emphasizing infrastructure, training, and policy to address Pakistan’s > 75% mental health treatment gap.
This letter offers a critical appraisal of Riaz et al.’s study (Explor Digit Health Technol. 2026;4:101179. DOI: 10.37349/edht.2026.101179) on psychiatrists’ knowledge, perceptions, and willingness toward digital psychiatry in Pakistan. The mixed-methods design identifies critical gaps in competencies (e.g., 68.5% telepsychiatry familiarity vs. 32.5% VR) and barriers like infrastructure deficits (44.5%). However, methodological issues per STROBE guidelines such as absent response rates, convenience sampling bias, and incomplete bias mitigation limit representativeness. An adapted Newcastle-Ottawa Scale scores it 7/10, indicating moderate bias of risk from selection and non-response. Additional concerns include under-explored cultural factors. Recommendations propose a tailored LMIC digital health adoption framework emphasizing infrastructure, training, and policy to address Pakistan’s > 75% mental health treatment gap.
DOI: https://doi.org/10.37349/edht.2026.101193
Aim:
This study aims to explore the role of the hashtag #EndoTwitter on the social media platform X by examining its geographical distribution, user demographics, engagement patterns, and post sentiments. With the increasing prevalence of endocrine and metabolic diseases, rapid knowledge exchange is essential. #EndoTwitter provides a unique communication medium for healthcare professionals, researchers, advocacy groups, journalists, and patients; however, its impact has not yet been systematically studied.
Methods:
The Fedica research analytics tool was used to analyze X posts containing #EndoTwitter from July 1, 2019, to July 1, 2023. Parameters assessed included post volume, impressions, sentiment, co-occurring hashtags, and geolocation.
Results:
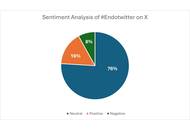
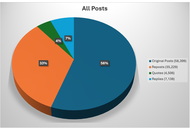
A total of 58,392 posts with #EndoTwitter were retrieved from around 21,000 users, generating 46.9 million impressions. These posts originated mainly from the United States (N = 29,546, 50.6%), followed by India (N = 6,567, 11.2%) and Mexico (N = 3,310, 5.7%). The top co-occurring hashtags included #MedTwitter, #Diabetes, and #NAFLD. Sentiment analysis revealed 16% positive sentiment, 8% negative, and 76% neutral among all posts.
Conclusions:
#EndoTwitter has the potential to foster evidence-based information sharing and inclusive communities, making it a valuable tool for endocrinology advocacy and patient care. Future research should explore specific post content to deepen insights into its impact.
Aim:
This study aims to explore the role of the hashtag #EndoTwitter on the social media platform X by examining its geographical distribution, user demographics, engagement patterns, and post sentiments. With the increasing prevalence of endocrine and metabolic diseases, rapid knowledge exchange is essential. #EndoTwitter provides a unique communication medium for healthcare professionals, researchers, advocacy groups, journalists, and patients; however, its impact has not yet been systematically studied.
Methods:
The Fedica research analytics tool was used to analyze X posts containing #EndoTwitter from July 1, 2019, to July 1, 2023. Parameters assessed included post volume, impressions, sentiment, co-occurring hashtags, and geolocation.
Results:
A total of 58,392 posts with #EndoTwitter were retrieved from around 21,000 users, generating 46.9 million impressions. These posts originated mainly from the United States (N = 29,546, 50.6%), followed by India (N = 6,567, 11.2%) and Mexico (N = 3,310, 5.7%). The top co-occurring hashtags included #MedTwitter, #Diabetes, and #NAFLD. Sentiment analysis revealed 16% positive sentiment, 8% negative, and 76% neutral among all posts.
Conclusions:
#EndoTwitter has the potential to foster evidence-based information sharing and inclusive communities, making it a valuable tool for endocrinology advocacy and patient care. Future research should explore specific post content to deepen insights into its impact.
DOI: https://doi.org/10.37349/edht.2026.101192
Aim:
To explore preliminary signals of change associated with a digitalized educational innovation—The Vital House (La Casa Vital)—on psychological flexibility and introspection among prospective secondary-school teachers in Spain, with the broader goal of promoting mental health competencies relevant to adolescent well-being.
Methods:
A total of 82 students enrolled in a Master’s program in teacher training at a Spanish public university participated in a 10-session intervention over 2.5 months (approximately 20 hours total). The Vital House model, a metaphorical representation of personal identity through “rooms” symbolizing life roles, was adapted into a digital format. Each room included interactive resources designed to address key psychosocial variables, including self‑efficacy, emotional regulation, and cognitive defusion. Participants reflected on their learning histories and the influence of significant figures, including teachers, on adult identity. Pre- and post-intervention measures assessed components of the ACT Hexaflex model (ad-hoc questionnaire) and introspective capacity (Self-Reflection and Insight Scale-Short Form).
Results:
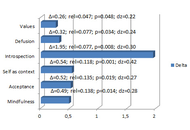
Paired-sample analyses indicated pre–post differences on five of six ACT processes: values (p = 0.048), mindfulness (p = 0.014), self-as-context (p < 0.001), cognitive defusion (p = 0.034), acceptance (p = 0.019), and on introspective capacity (p = 0.008). Effect sizes were in the small‑to‑moderate range, with Cohen’s d values ranging from 0.22 (small) to 0.42 (moderate). These findings should be interpreted cautiously given the design.
Conclusions:
In this pilot‑level, single‑group study, Vital House showed preliminary indications of promise for enhancing psychological flexibility and introspection in teacher training. However, the absence of a control/comparison group, the potential influence of concurrent course content, maturation, historical events, and repeated‑testing effects, as well as the lack of post‑intervention follow‑up, limit causal inference and claims about durability. Future controlled studies with follow‑up are warranted to evaluate efficacy, mechanisms, and maintenance, and to assess scalability across educational contexts.
Aim:
To explore preliminary signals of change associated with a digitalized educational innovation—The Vital House (La Casa Vital)—on psychological flexibility and introspection among prospective secondary-school teachers in Spain, with the broader goal of promoting mental health competencies relevant to adolescent well-being.
Methods:
A total of 82 students enrolled in a Master’s program in teacher training at a Spanish public university participated in a 10-session intervention over 2.5 months (approximately 20 hours total). The Vital House model, a metaphorical representation of personal identity through “rooms” symbolizing life roles, was adapted into a digital format. Each room included interactive resources designed to address key psychosocial variables, including self‑efficacy, emotional regulation, and cognitive defusion. Participants reflected on their learning histories and the influence of significant figures, including teachers, on adult identity. Pre- and post-intervention measures assessed components of the ACT Hexaflex model (ad-hoc questionnaire) and introspective capacity (Self-Reflection and Insight Scale-Short Form).
Results:
Paired-sample analyses indicated pre–post differences on five of six ACT processes: values (p = 0.048), mindfulness (p = 0.014), self-as-context (p < 0.001), cognitive defusion (p = 0.034), acceptance (p = 0.019), and on introspective capacity (p = 0.008). Effect sizes were in the small‑to‑moderate range, with Cohen’s d values ranging from 0.22 (small) to 0.42 (moderate). These findings should be interpreted cautiously given the design.
Conclusions:
In this pilot‑level, single‑group study, Vital House showed preliminary indications of promise for enhancing psychological flexibility and introspection in teacher training. However, the absence of a control/comparison group, the potential influence of concurrent course content, maturation, historical events, and repeated‑testing effects, as well as the lack of post‑intervention follow‑up, limit causal inference and claims about durability. Future controlled studies with follow‑up are warranted to evaluate efficacy, mechanisms, and maintenance, and to assess scalability across educational contexts.
DOI: https://doi.org/10.37349/edht.2026.101191
This article belongs to the special issue Digital Health Innovations in the Battle Against Psychological Problems: Progress, Hurdles, and Prospects
Telepsychiatry has transitioned from a supplementary modality to a sustained component of contemporary mental healthcare, driven by technological advancement, workforce shortages, and the COVID-19 pandemic. This narrative review synthesizes current evidence on clinical effectiveness, service models, technological integration, and ethical–legal considerations, and contextualizes these domains through institutional implementation experience in Türkiye. Across major diagnostic groups, including mood, anxiety, psychotic, neurodevelopmental, and substance use disorders, published studies generally indicate comparable outcomes and patient satisfaction to face-to-face care when delivered within structured clinical frameworks. We further articulate the theoretical foundations of clinical equivalence, emphasizing language-mediated therapeutic mechanisms, alliance formation in video-based settings, and behavioral factors influencing adherence. The manuscript introduces a system-level perspective for Türkiye, positioning telepsychiatry as a capacity-extending model within geographically uneven workforce distribution. Institutional applications, including disaster response, postpartum screening pathways, and hybrid specialty clinics, illustrate context-sensitive implementation strategies. Emerging innovations such as digital phenotyping, artificial intelligence, and virtual reality are discussed alongside regulatory, equity, and data governance considerations. We conclude that telepsychiatry represents not merely an emergency substitute but an increasingly integrated and policy-relevant model of care.
Telepsychiatry has transitioned from a supplementary modality to a sustained component of contemporary mental healthcare, driven by technological advancement, workforce shortages, and the COVID-19 pandemic. This narrative review synthesizes current evidence on clinical effectiveness, service models, technological integration, and ethical–legal considerations, and contextualizes these domains through institutional implementation experience in Türkiye. Across major diagnostic groups, including mood, anxiety, psychotic, neurodevelopmental, and substance use disorders, published studies generally indicate comparable outcomes and patient satisfaction to face-to-face care when delivered within structured clinical frameworks. We further articulate the theoretical foundations of clinical equivalence, emphasizing language-mediated therapeutic mechanisms, alliance formation in video-based settings, and behavioral factors influencing adherence. The manuscript introduces a system-level perspective for Türkiye, positioning telepsychiatry as a capacity-extending model within geographically uneven workforce distribution. Institutional applications, including disaster response, postpartum screening pathways, and hybrid specialty clinics, illustrate context-sensitive implementation strategies. Emerging innovations such as digital phenotyping, artificial intelligence, and virtual reality are discussed alongside regulatory, equity, and data governance considerations. We conclude that telepsychiatry represents not merely an emergency substitute but an increasingly integrated and policy-relevant model of care.
DOI: https://doi.org/10.37349/edht.2026.101190
This article belongs to the special issue Telepsychiatry in Low-and Middle-income Countries: an Update
Aim:
The aim of this study is to analyse the digital patient journey in medical tourism, with a particular focus on Ukraine’s experience under conditions of military challenges and global crises. The study examines how digital tools support inclusivity, accessibility, continuity of care, and patient trust, with special attention to rehabilitation services and vulnerable patient groups affected by war.
Methods:
The study employs a mixed-methods approach combining a review of scientific literature with empirical research and modelling of the digital patient journey. Primary data were collected through an online survey of 150 healthcare consumers and semi-structured interviews with 15 experts representing medical institutions involved in medical tourism. Quantitative and qualitative analyses were used to examine patient experience, inclusivity barriers, and the role of digital services.
Results:
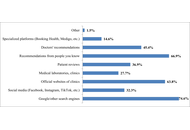
The results indicate that key stages of the digital patient journey include online information search and clinic selection, remote consultations, digital support for travel and treatment organization, and post-treatment follow-up and rehabilitation. Ukrainian clinics actively implement CRM systems, telemedicine solutions, and digital communication tools, enabling continuous patient engagement even during crisis conditions. At the same time, significant barriers were identified, including limited inclusiveness of digital services, data security concerns, uneven digital literacy, and infrastructural constraints. Based on the findings, a conceptual model of the digital patient journey integrating service quality, inclusivity, and AI-supported personalization was developed.
Conclusions:
The findings demonstrate that the digital patient journey is becoming critically important for the development of medical tourism under conditions of global uncertainty. The integration of digital tools with inclusive and patient-centred approaches enhances the resilience of medical services, strengthens patient trust, and provides competitive advantages for medical institutions. The proposed model may be useful for countries experiencing military conflicts or systemic crises and contributes to the broader development of digital and inclusive healthcare.
Aim:
The aim of this study is to analyse the digital patient journey in medical tourism, with a particular focus on Ukraine’s experience under conditions of military challenges and global crises. The study examines how digital tools support inclusivity, accessibility, continuity of care, and patient trust, with special attention to rehabilitation services and vulnerable patient groups affected by war.
Methods:
The study employs a mixed-methods approach combining a review of scientific literature with empirical research and modelling of the digital patient journey. Primary data were collected through an online survey of 150 healthcare consumers and semi-structured interviews with 15 experts representing medical institutions involved in medical tourism. Quantitative and qualitative analyses were used to examine patient experience, inclusivity barriers, and the role of digital services.
Results:
The results indicate that key stages of the digital patient journey include online information search and clinic selection, remote consultations, digital support for travel and treatment organization, and post-treatment follow-up and rehabilitation. Ukrainian clinics actively implement CRM systems, telemedicine solutions, and digital communication tools, enabling continuous patient engagement even during crisis conditions. At the same time, significant barriers were identified, including limited inclusiveness of digital services, data security concerns, uneven digital literacy, and infrastructural constraints. Based on the findings, a conceptual model of the digital patient journey integrating service quality, inclusivity, and AI-supported personalization was developed.
Conclusions:
The findings demonstrate that the digital patient journey is becoming critically important for the development of medical tourism under conditions of global uncertainty. The integration of digital tools with inclusive and patient-centred approaches enhances the resilience of medical services, strengthens patient trust, and provides competitive advantages for medical institutions. The proposed model may be useful for countries experiencing military conflicts or systemic crises and contributes to the broader development of digital and inclusive healthcare.
DOI: https://doi.org/10.37349/edht.2026.101189
Background:
Urine screening is a critical diagnostic tool in healthcare that supports the detection of a wide range of health conditions, including kidney diseases, metabolic disorders, and infections. Traditionally, urine tests are performed in clinical settings with results that often take time to be delivered. Such delays can hinder timely diagnosis, treatment initiation, and effective disease management. Recent advancements in digital health technologies, particularly the Internet of Things (IoT), machine learning (ML), and artificial intelligence (AI) algorithms, create opportunities for real-time data acquisition, integration, and analysis within routine urine screening. This systematic review synthesizes the current landscape of IoT-enabled urine screening technologies and evaluates their clinical, engineering, and computational foundations. The review also examines their integration with digital health architectures, edge computing systems, and tech driven personalized care.
Methods:
A structured literature search was conducted across PubMed, IEEE Xplore, Scopus, and Google Scholar for studies published between 2000 and 2025. Predefined search terms related to urinalysis, IoT, digital health, and microfluidics were applied. Sixty-five studies met the inclusion criteria. Data extraction focused on sensor technologies, digital health platforms, and reported case studies that demonstrated successful system deployment across diverse healthcare settings.
Results:
IoT-based urine screening technologies support real-time monitoring of biomarkers such as glucose, protein, and pH, which are essential for diagnosing conditions including diabetes, kidney disease, and urinary tract infections (UTIs). Emerging devices utilize optical, and acoustofluidic modalities, while BLE, Wi-Fi, and LPWAN serve as the primary connectivity standards.
Discussion:
IoT-driven digital transformation demonstrates strong potential to enhance the accessibility, efficiency, and diagnostic accuracy of urine screening. The convergence of biosensing, microfluidics and HDTs enables scalable, continuous, and personalized urine monitoring solutions. Despite these advancements, challenges related to data privacy, infrastructure readiness, and regulatory compliance remain significant barriers.
Background:
Urine screening is a critical diagnostic tool in healthcare that supports the detection of a wide range of health conditions, including kidney diseases, metabolic disorders, and infections. Traditionally, urine tests are performed in clinical settings with results that often take time to be delivered. Such delays can hinder timely diagnosis, treatment initiation, and effective disease management. Recent advancements in digital health technologies, particularly the Internet of Things (IoT), machine learning (ML), and artificial intelligence (AI) algorithms, create opportunities for real-time data acquisition, integration, and analysis within routine urine screening. This systematic review synthesizes the current landscape of IoT-enabled urine screening technologies and evaluates their clinical, engineering, and computational foundations. The review also examines their integration with digital health architectures, edge computing systems, and tech driven personalized care.
Methods:
A structured literature search was conducted across PubMed, IEEE Xplore, Scopus, and Google Scholar for studies published between 2000 and 2025. Predefined search terms related to urinalysis, IoT, digital health, and microfluidics were applied. Sixty-five studies met the inclusion criteria. Data extraction focused on sensor technologies, digital health platforms, and reported case studies that demonstrated successful system deployment across diverse healthcare settings.
Results:
IoT-based urine screening technologies support real-time monitoring of biomarkers such as glucose, protein, and pH, which are essential for diagnosing conditions including diabetes, kidney disease, and urinary tract infections (UTIs). Emerging devices utilize optical, and acoustofluidic modalities, while BLE, Wi-Fi, and LPWAN serve as the primary connectivity standards.
Discussion:
IoT-driven digital transformation demonstrates strong potential to enhance the accessibility, efficiency, and diagnostic accuracy of urine screening. The convergence of biosensing, microfluidics and HDTs enables scalable, continuous, and personalized urine monitoring solutions. Despite these advancements, challenges related to data privacy, infrastructure readiness, and regulatory compliance remain significant barriers.
DOI: https://doi.org/10.37349/edht.2026.101188
Aim:
To assess healthcare professionals’ awareness, attitudes, and utilization of community-based digital health platforms for preventive care in underserved districts of Khyber Pakhtunkhwa, Pakistan, and to identify key barriers associated with routine use.
Methods:
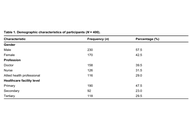
A cross-sectional survey was conducted between December 2024 and February 2025 among 400 healthcare professionals (doctors, nurses, and allied health practitioners) working in primary, secondary, and tertiary facilities in Swabi and Mardan. Participants were recruited using purposive, stratified (quota-based) sampling. The questionnaire captured knowledge/awareness, attitudes, self-reported utilization, and perceived barriers (infrastructure, training, and privacy). Descriptive statistics were produced, and multivariable regression was used to examine factors associated with utilization.
Results:
Among the 400 respondents, 332 (83.0%) reported awareness of digital health platforms and 312 (78.0%) reported positive attitudes toward their use. Overall, 297 (74.3%) reported using digital health platforms in practice. The most frequently reported barriers were lack of infrastructure (n = 309, 77.3%), limited training (n = 297, 74.3%), and data privacy concerns (n = 295, 73.8%). In the adjusted logistic regression model, greater knowledge of digital health platforms was associated with higher odds of routine use (aOR = 10.56, 95% CI: 2.36–47.35; p = 0.002), whereas attitude and infrastructure barriers were not significant (p > 0.05).
Conclusions:
Healthcare professionals in Swabi and Mardan reported high awareness and favorable attitudes toward community-based digital health platforms, but infrastructure gaps, limited training, and data privacy concerns were common barriers. Greater platform knowledge predicted routine use. Strengthening facility readiness, workflow-based training, and practical safeguards to address data privacy concerns may enable safer, more equitable scale-up; findings are context-specific due to non-probability sampling.
Aim:
To assess healthcare professionals’ awareness, attitudes, and utilization of community-based digital health platforms for preventive care in underserved districts of Khyber Pakhtunkhwa, Pakistan, and to identify key barriers associated with routine use.
Methods:
A cross-sectional survey was conducted between December 2024 and February 2025 among 400 healthcare professionals (doctors, nurses, and allied health practitioners) working in primary, secondary, and tertiary facilities in Swabi and Mardan. Participants were recruited using purposive, stratified (quota-based) sampling. The questionnaire captured knowledge/awareness, attitudes, self-reported utilization, and perceived barriers (infrastructure, training, and privacy). Descriptive statistics were produced, and multivariable regression was used to examine factors associated with utilization.
Results:
Among the 400 respondents, 332 (83.0%) reported awareness of digital health platforms and 312 (78.0%) reported positive attitudes toward their use. Overall, 297 (74.3%) reported using digital health platforms in practice. The most frequently reported barriers were lack of infrastructure (n = 309, 77.3%), limited training (n = 297, 74.3%), and data privacy concerns (n = 295, 73.8%). In the adjusted logistic regression model, greater knowledge of digital health platforms was associated with higher odds of routine use (aOR = 10.56, 95% CI: 2.36–47.35; p = 0.002), whereas attitude and infrastructure barriers were not significant (p > 0.05).
Conclusions:
Healthcare professionals in Swabi and Mardan reported high awareness and favorable attitudes toward community-based digital health platforms, but infrastructure gaps, limited training, and data privacy concerns were common barriers. Greater platform knowledge predicted routine use. Strengthening facility readiness, workflow-based training, and practical safeguards to address data privacy concerns may enable safer, more equitable scale-up; findings are context-specific due to non-probability sampling.
DOI: https://doi.org/10.37349/edht.2026.101187
Background:
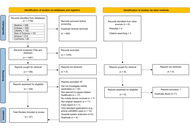
Sepsis is a major cause of disease worldwide. Mobile applications (apps) have been developed to assist clinical practice. Current evidence evaluating such apps is diverse. This scoping review aimed to map currently available literature investigating the usage of mobile apps for sepsis-related healthcare. This will highlight evidence gaps, and areas for future innovation and app development.
Methods:
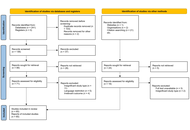
Databases MEDLINE, Embase, CINAHL, Cochrane, Scopus, and Web of Science were searched in June 2023 (updated in July 2024). Studies containing original research investigating mobile apps for sepsis-related healthcare were included and analysed in three categories identified from the primary purpose of the app: (1) education and awareness, (2) clinical assistance, and (3) biomarker or pathogen detection.
Results:
A total of 1,755 studies were identified and 27 included following screening, of which 19 (70%) were published in 2020 or later. Most of the 27 studies investigated apps for clinical assistance (70%, n = 19). These apps were diverse, acting as digital solutions for data collection (n = 2), triage (n = 6), clinical guideline access (n = 5), alert delivery (n = 1), and outcome prediction (n = 5). There were five apps (19%) used to assist biomarker or pathogen detection. Of these, most (80%, n = 4) mobile apps were used to detect and quantify colorimetric signals in combination with assays, and all five apps had attachments necessary for laboratory processes. Lastly, three apps (11%) were designed to enhance education and awareness, two targeting medical education and one targeting public awareness.
Discussion:
Mobile applications offer innovative and exciting digital solutions for biomarker detection, education, and clinical support in sepsis-related healthcare. Current literature is highly heterogenous and rapidly developing.
Background:
Sepsis is a major cause of disease worldwide. Mobile applications (apps) have been developed to assist clinical practice. Current evidence evaluating such apps is diverse. This scoping review aimed to map currently available literature investigating the usage of mobile apps for sepsis-related healthcare. This will highlight evidence gaps, and areas for future innovation and app development.
Methods:
Databases MEDLINE, Embase, CINAHL, Cochrane, Scopus, and Web of Science were searched in June 2023 (updated in July 2024). Studies containing original research investigating mobile apps for sepsis-related healthcare were included and analysed in three categories identified from the primary purpose of the app: (1) education and awareness, (2) clinical assistance, and (3) biomarker or pathogen detection.
Results:
A total of 1,755 studies were identified and 27 included following screening, of which 19 (70%) were published in 2020 or later. Most of the 27 studies investigated apps for clinical assistance (70%, n = 19). These apps were diverse, acting as digital solutions for data collection (n = 2), triage (n = 6), clinical guideline access (n = 5), alert delivery (n = 1), and outcome prediction (n = 5). There were five apps (19%) used to assist biomarker or pathogen detection. Of these, most (80%, n = 4) mobile apps were used to detect and quantify colorimetric signals in combination with assays, and all five apps had attachments necessary for laboratory processes. Lastly, three apps (11%) were designed to enhance education and awareness, two targeting medical education and one targeting public awareness.
Discussion:
Mobile applications offer innovative and exciting digital solutions for biomarker detection, education, and clinical support in sepsis-related healthcare. Current literature is highly heterogenous and rapidly developing.
DOI: https://doi.org/10.37349/edht.2026.101186
Multicenter imaging studies are increasingly critical in epidemiology, yet variability across scanners, acquisition protocols, and reconstruction algorithms introduces systematic biases that threaten reproducibility and comparability of quantitative biomarkers. This paper reviews the major sources of heterogeneity in MRI, CT, and PET-CT data, highlighting their impact on epidemiologic inference, including misclassification, reduced statistical power, and compromised generalizability. We outline harmonization strategies spanning pre-acquisition standardization, phantom-based calibration, post-acquisition intensity normalization, and advanced statistical and machine learning methods such as ComBat and domain adaptation. Illustrative examples from MRI flow quantification and radiomic feature extraction demonstrate how harmonization can mitigate site effects and enable robust large-scale analyses.
Multicenter imaging studies are increasingly critical in epidemiology, yet variability across scanners, acquisition protocols, and reconstruction algorithms introduces systematic biases that threaten reproducibility and comparability of quantitative biomarkers. This paper reviews the major sources of heterogeneity in MRI, CT, and PET-CT data, highlighting their impact on epidemiologic inference, including misclassification, reduced statistical power, and compromised generalizability. We outline harmonization strategies spanning pre-acquisition standardization, phantom-based calibration, post-acquisition intensity normalization, and advanced statistical and machine learning methods such as ComBat and domain adaptation. Illustrative examples from MRI flow quantification and radiomic feature extraction demonstrate how harmonization can mitigate site effects and enable robust large-scale analyses.
DOI: https://doi.org/10.37349/edht.2026.101185
Aim:
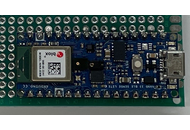
Neonatal jaundice or neonatal hyperbilirubinemia is a common medical condition impacting newborns and pathological jaundice if left untreated, leads to neurological encephalopathy and/or death. The majority of pathological jaundice cases occur in low and middle- income countries (LMIC). Phototherapy has been determined to be the safest and most effective treatment for jaundice. Although inexpensive light-emitting diodes are available on the market, commercial phototherapy devices are expensive (~US$2,000), which creates a barrier to access for these devices in LMIC. Efforts to construct cost-effective phototherapy units have been implemented in the past, but need a method to validate the intensity and wavelength of light received by the infant at a distance away from the source.
Methods:
To enable low-cost phototherapy units to be used clinically, this study provides an open-source, low-cost, distributed manufacturing approach to create a light sensor to calibrate phototherapy units. This instrument is a necessary component of any open-source phototherapy treatment used in a clinical setting. This novel instrument was validated by comparing its irradiance and wavelength reading to the commercially calibrated Ocean Insight UV-VIS spectrometer under varying lighting conditions, including that of the existing Datex-Ohmeda Giraffe Spot PT Lite phototherapy equipment accessible through Victoria Children’s Hospital Neonatal Care Ward in London, Ontario, and Kiambu County Hospital in Kenya.
Results:
The results of this study have demonstrated that for under US$150, a phototherapy calibration device can be constructed capable of measuring up to 200 uW/cm2/nm with an accuracy of 98.6% and detect the peak wavelength within ±12.5 nm.
Conclusions:
It can be concluded that 3D printed open-source irradiance meters are a viable option for calibrating phototherapy units in LMIC to treat hyperbilirubinemia.
Aim:
Neonatal jaundice or neonatal hyperbilirubinemia is a common medical condition impacting newborns and pathological jaundice if left untreated, leads to neurological encephalopathy and/or death. The majority of pathological jaundice cases occur in low and middle- income countries (LMIC). Phototherapy has been determined to be the safest and most effective treatment for jaundice. Although inexpensive light-emitting diodes are available on the market, commercial phototherapy devices are expensive (~US$2,000), which creates a barrier to access for these devices in LMIC. Efforts to construct cost-effective phototherapy units have been implemented in the past, but need a method to validate the intensity and wavelength of light received by the infant at a distance away from the source.
Methods:
To enable low-cost phototherapy units to be used clinically, this study provides an open-source, low-cost, distributed manufacturing approach to create a light sensor to calibrate phototherapy units. This instrument is a necessary component of any open-source phototherapy treatment used in a clinical setting. This novel instrument was validated by comparing its irradiance and wavelength reading to the commercially calibrated Ocean Insight UV-VIS spectrometer under varying lighting conditions, including that of the existing Datex-Ohmeda Giraffe Spot PT Lite phototherapy equipment accessible through Victoria Children’s Hospital Neonatal Care Ward in London, Ontario, and Kiambu County Hospital in Kenya.
Results:
The results of this study have demonstrated that for under US$150, a phototherapy calibration device can be constructed capable of measuring up to 200 uW/cm2/nm with an accuracy of 98.6% and detect the peak wavelength within ±12.5 nm.
Conclusions:
It can be concluded that 3D printed open-source irradiance meters are a viable option for calibrating phototherapy units in LMIC to treat hyperbilirubinemia.
DOI: https://doi.org/10.37349/edht.2026.101184
Aim:
This study aims to evaluate the outreach achieved by psychiatry-related posts using the hashtag #YouthMentalHealth, highlighting how social media platforms can shape public discourse on adolescent mental health.
Methods:
We utilized the Fedica research analytics tool to characterize posts containing #YouthMentalHealth from January 10, 2018, to January 10, 2023. This analysis examined the #YouthMentalHealth activity timeline, identifying the number of posts containing the hashtag and the geographical distribution to assess the effectiveness of hashtag campaigns.
Results:
The #YouthMentalHealth movement resulted in 58,000 posts shared by around 25,000 X users, generating 292.7 million impressions (views). The top three countries from which most posts containing #YouthMentalHealth were shared included the United States (35.14%), Canada (29.15%), and the United Kingdom (14.37%). The three largest contributor groups were management companies (20.6%), educational advocacy organizations (17.5%), and social advocacy groups (14%).
Conclusions:
This first-of-its-kind study explores the impact and utilization of #YouthMentalHealth globally, reporting trends and patterns from digital media platforms. By mapping the hashtag’s global footprint, the study offers novel insights into how digital advocacy can amplify youth mental health awareness and connect multidisciplinary stakeholders. These findings contribute to emerging frameworks in digital psychiatry by underscoring the role of social media as a complementary tool for mental health promotion and community engagement, while illuminating diverse strategies to aid the psychiatric community in effectively addressing the mental health needs of adolescents.
Aim:
This study aims to evaluate the outreach achieved by psychiatry-related posts using the hashtag #YouthMentalHealth, highlighting how social media platforms can shape public discourse on adolescent mental health.
Methods:
We utilized the Fedica research analytics tool to characterize posts containing #YouthMentalHealth from January 10, 2018, to January 10, 2023. This analysis examined the #YouthMentalHealth activity timeline, identifying the number of posts containing the hashtag and the geographical distribution to assess the effectiveness of hashtag campaigns.
Results:
The #YouthMentalHealth movement resulted in 58,000 posts shared by around 25,000 X users, generating 292.7 million impressions (views). The top three countries from which most posts containing #YouthMentalHealth were shared included the United States (35.14%), Canada (29.15%), and the United Kingdom (14.37%). The three largest contributor groups were management companies (20.6%), educational advocacy organizations (17.5%), and social advocacy groups (14%).
Conclusions:
This first-of-its-kind study explores the impact and utilization of #YouthMentalHealth globally, reporting trends and patterns from digital media platforms. By mapping the hashtag’s global footprint, the study offers novel insights into how digital advocacy can amplify youth mental health awareness and connect multidisciplinary stakeholders. These findings contribute to emerging frameworks in digital psychiatry by underscoring the role of social media as a complementary tool for mental health promotion and community engagement, while illuminating diverse strategies to aid the psychiatric community in effectively addressing the mental health needs of adolescents.
DOI: https://doi.org/10.37349/edht.2026.101183
Background:
To synthesize evidence on how medical thermography, integrated with artificial intelligence (AI), blockchain, 5G (5th Generation mobile networks), and Internet of Things (IoT), enhances diagnostics, fraud prevention, and personalized health insurance in emerging markets, addressing cost escalation and access gaps.
Methods:
This systematic review followed AMSTAR 2 and PRISMA guidelines, synthesizing 25 sources (22 peer-reviewed articles, 3 industry reports) from a pre-analyzed dataset. Inclusion focused on relevance to thermography, insurance, or synergistic technologies; exclusions included non-peer-reviewed or irrelevant items. Data extraction via Microsoft Excel (version 2409) covered diagnostics, applications, synergies, and contexts. Quality appraisal used the Mixed Methods Appraisal Tool (MMAT) to assess methodological rigor. Narrative synthesis addressed heterogeneity, without meta-analysis due to design diversity and resource limits.
Results:
Thermography achieves 83–98% sensitivities for breast cancer (asymmetries > 3.0°C), diabetic foot ulcers (DFUs; 96.71% with AI), and rheumatoid arthritis (RA; inflammation > 0.5°C), reducing triage times by 25% and costs by 30% in mobile settings. Blockchain’s six-layer architecture, with Practical Byzantine Fault Tolerance and InterPlanetary File System, secures data at US$0.028 per transaction, potentially reducing fraud through enhanced verification. In emerging markets like India and Brazil, portable thermography with 5G supports screening, aligned with standards like T/ZADT 005-2002.
Discussion:
These integrations enable early detection (saving US$8,000–12,000 per DFU), fraud mitigation, and equitable access, though protocol variances and biases require attention. Recommendations include standardization, pilots in rural areas, and bias-mitigating AI frameworks to optimize health insurance outcomes.
Background:
To synthesize evidence on how medical thermography, integrated with artificial intelligence (AI), blockchain, 5G (5th Generation mobile networks), and Internet of Things (IoT), enhances diagnostics, fraud prevention, and personalized health insurance in emerging markets, addressing cost escalation and access gaps.
Methods:
This systematic review followed AMSTAR 2 and PRISMA guidelines, synthesizing 25 sources (22 peer-reviewed articles, 3 industry reports) from a pre-analyzed dataset. Inclusion focused on relevance to thermography, insurance, or synergistic technologies; exclusions included non-peer-reviewed or irrelevant items. Data extraction via Microsoft Excel (version 2409) covered diagnostics, applications, synergies, and contexts. Quality appraisal used the Mixed Methods Appraisal Tool (MMAT) to assess methodological rigor. Narrative synthesis addressed heterogeneity, without meta-analysis due to design diversity and resource limits.
Results:
Thermography achieves 83–98% sensitivities for breast cancer (asymmetries > 3.0°C), diabetic foot ulcers (DFUs; 96.71% with AI), and rheumatoid arthritis (RA; inflammation > 0.5°C), reducing triage times by 25% and costs by 30% in mobile settings. Blockchain’s six-layer architecture, with Practical Byzantine Fault Tolerance and InterPlanetary File System, secures data at US$0.028 per transaction, potentially reducing fraud through enhanced verification. In emerging markets like India and Brazil, portable thermography with 5G supports screening, aligned with standards like T/ZADT 005-2002.
Discussion:
These integrations enable early detection (saving US$8,000–12,000 per DFU), fraud mitigation, and equitable access, though protocol variances and biases require attention. Recommendations include standardization, pilots in rural areas, and bias-mitigating AI frameworks to optimize health insurance outcomes.
DOI: https://doi.org/10.37349/edht.2026.101182
Digital twin technology is emerging as a transformative paradigm in healthcare, shifting practice from provider-centered models toward more personalized forms of medicine. As dynamic virtual representations of the human body, digital twins integrate biometric data, lifestyle patterns, and clinical records to simulate, monitor, and predict health trajectories in real time. Their growing use raises not only technical possibilities but also important questions about how patients relate to these data-driven counterparts, particularly when twins inform everyday health decisions in chronic care, such as diabetes or oncology. This perspective examines these relational dynamics and their ethical, cultural, and experiential implications for autonomy, decision-making, and the lived experience of being represented in data. To guide this analysis, we introduce a scale framework with three intersecting lenses: time, distinguishing asynchronous from synchronous updating; twining, ranging from close mirroring to more augmentative forms of representation; and control, spanning human-led to twin-driven decision authority. Using this framework, we position four common types of digital twins: mirror, shadow, intelligent, and simulacra as an evolution from basic representation to transformative modeling. We argue that future healthcare and public health policy must go beyond technical innovation to address patients’ lived experiences, ensuring that digital twins enhance rather than diminish autonomy, trust, and equity. This perspective thus calls for a patient-centered approach in designing and implementing digital twin technologies.
Digital twin technology is emerging as a transformative paradigm in healthcare, shifting practice from provider-centered models toward more personalized forms of medicine. As dynamic virtual representations of the human body, digital twins integrate biometric data, lifestyle patterns, and clinical records to simulate, monitor, and predict health trajectories in real time. Their growing use raises not only technical possibilities but also important questions about how patients relate to these data-driven counterparts, particularly when twins inform everyday health decisions in chronic care, such as diabetes or oncology. This perspective examines these relational dynamics and their ethical, cultural, and experiential implications for autonomy, decision-making, and the lived experience of being represented in data. To guide this analysis, we introduce a scale framework with three intersecting lenses: time, distinguishing asynchronous from synchronous updating; twining, ranging from close mirroring to more augmentative forms of representation; and control, spanning human-led to twin-driven decision authority. Using this framework, we position four common types of digital twins: mirror, shadow, intelligent, and simulacra as an evolution from basic representation to transformative modeling. We argue that future healthcare and public health policy must go beyond technical innovation to address patients’ lived experiences, ensuring that digital twins enhance rather than diminish autonomy, trust, and equity. This perspective thus calls for a patient-centered approach in designing and implementing digital twin technologies.
DOI: https://doi.org/10.37349/edht.2026.101181
Aim:
Diagnosing and treating major depressive disorder (MDD) remains a pressing global health challenge. Generative-AI tools, by lowering technical barriers and offering rapid visual feedback, may open new avenues for art-based assessment and intervention.
Methods:
In this exploratory qualitative pilot, we conducted reflexive thematic analysis of semi-structured interviews with N = 10 young adults at elevated risk for depression who generated self-representative images in Midjourney during a 45-minute session. Participants were selected from a larger cohort described elsewhere; no quantitative analyses were conducted in the present paper.
Results:
Qualitative findings suggested therapeutic-like mechanisms that mirror—and in some cases amplify—those reported for traditional art therapy, including the experience of flow and spontaneity, a heightened sense of creative agency, and the safe externalization of difficult or extreme emotions. Some participants described abrupt “sentiment switches,” where joyful imagery was immediately followed by scenes of sudden, intrusive self-criticism. Importantly, the generative process also surfaced idiosyncratic “resource images” (e.g., nature motifs, hobbies, values, loved ones) that participants experienced as calming or empowering, hinting at personalised anchors for future interventions.
Conclusions:
In line with prior quantitative work showing that more negative prompt sentiment statistically relates to higher BDI scores, the present qualitative narratives offer an interpretive account of how such negativity may emerge during AI-assisted self-representation. However, the current study does not integrate datasets or perform mixed-methods triangulation and uses those prior findings solely for contextualization. We conclude that, with appropriate ethical safeguards, generative-AI image making may serve as a flexible, low-cost adjunct to existing diagnostic and art-therapeutic practices, offering clients and clinicians a shared visual language for exploring the multi-layered experience of depression.
Aim:
Diagnosing and treating major depressive disorder (MDD) remains a pressing global health challenge. Generative-AI tools, by lowering technical barriers and offering rapid visual feedback, may open new avenues for art-based assessment and intervention.
Methods:
In this exploratory qualitative pilot, we conducted reflexive thematic analysis of semi-structured interviews with N = 10 young adults at elevated risk for depression who generated self-representative images in Midjourney during a 45-minute session. Participants were selected from a larger cohort described elsewhere; no quantitative analyses were conducted in the present paper.
Results:
Qualitative findings suggested therapeutic-like mechanisms that mirror—and in some cases amplify—those reported for traditional art therapy, including the experience of flow and spontaneity, a heightened sense of creative agency, and the safe externalization of difficult or extreme emotions. Some participants described abrupt “sentiment switches,” where joyful imagery was immediately followed by scenes of sudden, intrusive self-criticism. Importantly, the generative process also surfaced idiosyncratic “resource images” (e.g., nature motifs, hobbies, values, loved ones) that participants experienced as calming or empowering, hinting at personalised anchors for future interventions.
Conclusions:
In line with prior quantitative work showing that more negative prompt sentiment statistically relates to higher BDI scores, the present qualitative narratives offer an interpretive account of how such negativity may emerge during AI-assisted self-representation. However, the current study does not integrate datasets or perform mixed-methods triangulation and uses those prior findings solely for contextualization. We conclude that, with appropriate ethical safeguards, generative-AI image making may serve as a flexible, low-cost adjunct to existing diagnostic and art-therapeutic practices, offering clients and clinicians a shared visual language for exploring the multi-layered experience of depression.
DOI: https://doi.org/10.37349/edht.2026.101180
This article belongs to the special issue Digital Health Innovations in the Battle Against Psychological Problems: Progress, Hurdles, and Prospects
Aim:
A comprehensive understanding of current digital literacy and perspectives of the psychiatric workforce is important to introduce appropriate digital psychiatry interventions and implement contextually relevant measures in Pakistan. This study aims to address a gap in the existing literature by assessing psychiatrists’ knowledge, attitudes, perceived barriers, and willingness to integrate digital psychiatry into their clinical practice.
Methods:
A cross-sectional online survey was conducted from January 2023 to June 2023 across psychiatric departments of 18 public hospitals in Pakistan. The study included psychiatry residents, fellows, and consultants. A 48-item questionnaire, internally and externally validated, assessed knowledge, perceptions, and willingness to adopt digital psychiatry tools—telepsychiatry, artificial intelligence, mental health applications, and virtual reality. Data were analyzed using Statistical Package for the Social Sciences (version 26) for descriptive statistics, correlation, and regression analyses, while thematic analysis of open-ended responses was performed using Quirkos.
Results:
A total of 200 participants (56.0% aged 20–30 years, n = 112; 55.5% male, n = 111) were part of this study. 68.5% (n = 137) understood the applications of telepsychiatry, while 72.5% (n = 145) agreed that it is time-efficient and cost-effective. Only 39.5% (n = 79) of participants had received relevant artificial intelligence training to incorporate it in their psychiatric clinical practice. 62.0% (n = 124) of respondents reported unfamiliarity with the use of mental health applications. Regarding virtual reality, 32.5% (n = 65) were familiar with the technology, but only 42.5% (n = 85) were aware of its applications in psychiatric care. Thematic reflexive analysis revealed major challenges, including a ‘lack of infrastructure/resources’ (44.5%, n = 89) and a ‘lack of education/awareness’ (21.5%, n = 43).
Conclusions:
This study represents the first cross-sectional examination of digital psychiatric literacy in Pakistan’s healthcare system, which revealed significant gaps in digital health competencies among psychiatrists. Given the vast potential of emerging technologies in addressing mental health challenges, there is an urgent need for mental health professionals in Pakistan to integrate digitization in psychiatric practice.
Aim:
A comprehensive understanding of current digital literacy and perspectives of the psychiatric workforce is important to introduce appropriate digital psychiatry interventions and implement contextually relevant measures in Pakistan. This study aims to address a gap in the existing literature by assessing psychiatrists’ knowledge, attitudes, perceived barriers, and willingness to integrate digital psychiatry into their clinical practice.
Methods:
A cross-sectional online survey was conducted from January 2023 to June 2023 across psychiatric departments of 18 public hospitals in Pakistan. The study included psychiatry residents, fellows, and consultants. A 48-item questionnaire, internally and externally validated, assessed knowledge, perceptions, and willingness to adopt digital psychiatry tools—telepsychiatry, artificial intelligence, mental health applications, and virtual reality. Data were analyzed using Statistical Package for the Social Sciences (version 26) for descriptive statistics, correlation, and regression analyses, while thematic analysis of open-ended responses was performed using Quirkos.
Results:
A total of 200 participants (56.0% aged 20–30 years, n = 112; 55.5% male, n = 111) were part of this study. 68.5% (n = 137) understood the applications of telepsychiatry, while 72.5% (n = 145) agreed that it is time-efficient and cost-effective. Only 39.5% (n = 79) of participants had received relevant artificial intelligence training to incorporate it in their psychiatric clinical practice. 62.0% (n = 124) of respondents reported unfamiliarity with the use of mental health applications. Regarding virtual reality, 32.5% (n = 65) were familiar with the technology, but only 42.5% (n = 85) were aware of its applications in psychiatric care. Thematic reflexive analysis revealed major challenges, including a ‘lack of infrastructure/resources’ (44.5%, n = 89) and a ‘lack of education/awareness’ (21.5%, n = 43).
Conclusions:
This study represents the first cross-sectional examination of digital psychiatric literacy in Pakistan’s healthcare system, which revealed significant gaps in digital health competencies among psychiatrists. Given the vast potential of emerging technologies in addressing mental health challenges, there is an urgent need for mental health professionals in Pakistan to integrate digitization in psychiatric practice.
DOI: https://doi.org/10.37349/edht.2026.101179
This article belongs to the special issue Telepsychiatry in Low-and Middle-income Countries: an Update
Artificial intelligence (AI) is transforming healthcare by equipping clinicians and patients with tools that support more efficient, patient-centered care. In pediatrics, however, the implementation of AI demands a higher threshold for responsibility, transparency, and family-centered engagement. This perspective explores the opportunities and challenges of AI in pediatric healthcare, highlighting the unique ethical and developmental considerations that distinguish children’s care from adult medicine. Drawing on Kaiser Permanente’s seven principles for responsible AI, the article emphasizes the importance of augmentation over automation, the need for pediatric-specific validation, and the necessity of trustworthiness and fairness in clinical deployment. It outlines how AI can support primary care providers through enhanced decision support, early screening for developmental and behavioral disorders, including the potential for AI to create personalized developmental trajectories, moving beyond static population norms to provide earlier, more precise insights into a child’s neurodevelopmental progress, improved electronic health record usability, and risk prediction models. However, without careful governance, AI poses risks of bias, inequity, and erosion of clinician judgment. Policy recommendations include redesigning family consent models, ensuring robust clinician training, and mandating pediatric-specific testing of AI systems with diverse, representative datasets. Ultimately, AI should function as a supportive tool that strengthens, not replaces, human empathy, clinical expertise, and family-centered values. Responsible innovation is essential to ensure that children benefit equitably from AI while maintaining trust, safety, and compassion in pediatric healthcare.
Artificial intelligence (AI) is transforming healthcare by equipping clinicians and patients with tools that support more efficient, patient-centered care. In pediatrics, however, the implementation of AI demands a higher threshold for responsibility, transparency, and family-centered engagement. This perspective explores the opportunities and challenges of AI in pediatric healthcare, highlighting the unique ethical and developmental considerations that distinguish children’s care from adult medicine. Drawing on Kaiser Permanente’s seven principles for responsible AI, the article emphasizes the importance of augmentation over automation, the need for pediatric-specific validation, and the necessity of trustworthiness and fairness in clinical deployment. It outlines how AI can support primary care providers through enhanced decision support, early screening for developmental and behavioral disorders, including the potential for AI to create personalized developmental trajectories, moving beyond static population norms to provide earlier, more precise insights into a child’s neurodevelopmental progress, improved electronic health record usability, and risk prediction models. However, without careful governance, AI poses risks of bias, inequity, and erosion of clinician judgment. Policy recommendations include redesigning family consent models, ensuring robust clinician training, and mandating pediatric-specific testing of AI systems with diverse, representative datasets. Ultimately, AI should function as a supportive tool that strengthens, not replaces, human empathy, clinical expertise, and family-centered values. Responsible innovation is essential to ensure that children benefit equitably from AI while maintaining trust, safety, and compassion in pediatric healthcare.
DOI: https://doi.org/10.37349/edht.2026.101178
