Review
Review

Affiliation:
School of Architecture, Victoria University of Wellington, Wellington 6011, New Zealand
Email: chengcheng.yin@vuw.ac.nz
ORCID: https://orcid.org/0009-0006-5276-9550
Affiliation:
School of Architecture, Victoria University of Wellington, Wellington 6011, New Zealand
ORCID: https://orcid.org/0000-0001-7896-5089
Affiliation:
School of Architecture, Victoria University of Wellington, Wellington 6011, New Zealand
ORCID: https://orcid.org/0000-0002-4761-8225
Explor Digit Health Technol. 2025;3:101160 DOI: https://doi.org/10.37349/edht.2025.101160
Received: February 07, 2025 Accepted: August 19, 2025 Published: September 04, 2025
Academic Editor: Subho Chakrabarti, Postgraduate Institute of Medical Education and Research (PGIMER), India
Virtual reality (VR) and digital health technologies have shown increasing potential in addressing psychological challenges such as homesickness and emotional distress, yet the role of emotional bonds, particularly place attachment, in shaping the design and effectiveness of these interventions remains underexplored. This study conceptualizes the integration of place attachment theory into digital health interventions, especially those utilizing VR, and proposes a theoretical and practical framework for designing emotionally resonant virtual environments. Two interrelated conceptual models are introduced: the Virtual Place Attachment Development Model (VPADM), which outlines psychological, social, environmental, and cultural dimensions that contribute to emotional bonding with virtual spaces, and the Cultural Adaptation System for Virtual Environments (CASVE), which addresses cross-cultural adaptation processes through assessment, implementation, and evaluation. These frameworks illustrate how virtual place attachment can be purposefully designed to enhance user engagement and emotional well-being, while also highlighting practical challenges such as accessibility, digital literacy, and the need for culturally responsive content. By integrating place attachment theory into digital mental health design, the paper offers a pathway to improve therapeutic outcomes in VR environments and provides a foundation for researchers and practitioners to develop emotionally supportive, culturally meaningful, and context-sensitive digital health interventions.
The rapid advancement of digital health technologies has fundamentally transformed mental healthcare delivery, offering innovative solutions to longstanding challenges in psychological intervention and treatment accessibility. These developments have become particularly significant in the context of global events such as the COVID-19 pandemic, accelerating the adoption of digital mental health solutions and emphasizing the need for scalable, high-quality care [1]. The global digital health market has experienced unprecedented growth, with mental health applications showing significant increases in adoption rates [2]. Within this evolving landscape, virtual reality (VR) technology has emerged as a particularly promising tool, demonstrating remarkable potential for creating immersive therapeutic environments that can address a wide range of psychological needs [3]. Clinical trials have shown that VR-based interventions can achieve comparable outcomes to traditional face-to-face therapy in treating conditions such as anxiety disorders, post-traumatic stress disorder (PTSD), and depression [4]. This technological revolution in mental healthcare has not only improved treatment accessibility but also opened new possibilities for personalized and immersive therapeutic experiences.
At the intersection of this technological evolution lies the well-established concept of place attachment, which has long been recognized as a fundamental component of psychological well-being. Place attachment theory, rooted in environmental psychology, describes the emotional bonds that individuals form with meaningful locations and the subsequent impact these connections have on mental health and emotional resilience [5]. The theory encompasses multiple dimensions, including person-related factors, place-related aspects, and psychological processes that influence how people connect with places [6]. Research has demonstrated that strong place attachments can serve as protective factors against various mental health challenges, promoting psychological stability and emotional well-being [7]. Studies have shown significant correlations between place attachment and improved mental health outcomes, including better stress management and emotional regulation [8]. Furthermore, emerging research in environmental neuroscience has begun to explore the neural correlates of place attachment, suggesting involvement of brain regions associated with emotional processing and memory formation [9]. Collectively, these findings highlight place attachment as not only a psychological phenomenon but also a potential therapeutic mechanism that can inform the development of supportive mental health environments and interventions.
Despite the growing recognition of both digital health technologies and place attachment theory, significant gaps remain in our understanding of their integration. Current research lacks a systematic theoretical framework for incorporating place attachment principles into virtual environments (VEs). While studies have explored VR applications in mental health [3], the specific mechanisms through which VEs can replicate the therapeutic benefits of physical place attachment remain largely unexplored [10]. The absence of standardized protocols for creating and evaluating VEs that effectively foster psychological connections has hindered progress in this promising field. Additionally, there is a notable absence of research examining these applications across different cultural contexts, where the experience and expression of place attachment may vary significantly [11], with current studies predominantly focused on Western populations [12]. These limitations point to a pressing need for interdisciplinary research that systematically examines how the therapeutic value of place attachment can be operationalized in virtual settings.
Building on this identified need for interdisciplinary inquiry, we propose a research agenda that centers on the following critical questions: (1) How can the essential elements of place attachment be effectively translated into VEs? (2) What are the key mechanisms through which VR-based place attachment influences psychological well-being? (3) How can these digital interventions be adapted to accommodate diverse cultural perspectives on place attachment? By investigating these questions, we aim to bridge the gap between traditional place attachment theory and contemporary digital health interventions, providing a comprehensive framework for understanding and implementing this integration. The significance of this research lies in its novel theoretical and practical contributions. Theoretically, this study extends the boundaries of place attachment theory by examining its application in digital environments, establishing new frameworks for assessing virtual place attachment (VPA), and developing culturally sensitive theoretical models. Our work synthesizes insights from environmental psychology, digital health technology, and cross-cultural psychology to create an integrated theoretical framework that can guide future research and development in this field. Practically, our findings will guide the design and implementation of more effective digital mental health interventions that leverage the therapeutic potential of place attachment across different cultural contexts. This includes developing specific guidelines for creating VEs that promote authentic place attachment experiences and establishing metrics for evaluating their effectiveness.
The integration of digital technologies into mental healthcare has redefined treatment delivery, improving accessibility and customization for diverse patient populations. Studies indicate that digital mental health tools are particularly effective in addressing common disorders such as depression, generalized anxiety disorder, and PTSD. Early interventions, including text-based cognitive behavioral therapy (CBT) apps and video-based teletherapy, have grown into multifaceted ecosystems powered by AI and machine learning [1]. For example, Andersson et al. [13] reported efficacy comparable to face-to-face therapy in multiple meta-analyses, while digital CBT interventions have achieved 30–50% symptom reduction across clinical trials [14]. These advancements enable real-time symptom monitoring, predictive analytics for mental health risks, and dynamic tailoring of interventions. However, disparities in digital literacy and internet access remain critical barriers to universal adoption.
VR applications have revolutionized exposure therapy, pain management, and stress reduction. VR’s immersive nature offers unparalleled control over environmental stimuli, enabling precise modulation of therapeutic challenges. In anxiety treatment, VR exposure therapy showed an 80% reduction in phobia symptoms compared to 60% for traditional methods [3]. Furthermore, new lightweight, standalone VR devices have enhanced feasibility in outpatient and home settings [15]. Recent advances in AI-powered digital health systems have further expanded these capabilities by emphasizing adaptive algorithms that enhance personalization, emotion recognition, and behavioral response within VEs. Studies published after 2023 have demonstrated that large language models (LLMs), emotion-aware sensors, and real-time content adjustment algorithms significantly improve therapeutic engagement and user adherence in mental health interventions. A recent systematic review has confirmed the effectiveness of machine learning algorithms in adjusting therapeutic content in real time based on biometric inputs such as heart rate and skin conductance [16]. These developments represent a significant evolution from static therapeutic environments to responsive, personalized digital spaces that adapt continuously to user needs.
The growing convergence of AI and human-centered design is increasingly reflected in digital mental health platforms that support multilingual interaction, cultural tailoring, and conversational support through AI-guided avatars or digital therapists [17–19]. This technological evolution addresses longstanding challenges in cross-cultural mental health delivery while maintaining therapeutic fidelity across diverse populations. Evaluations show that while LLMs are not yet ready to fully replace therapists, they can effectively assist in tasks like identifying and reframing unhelpful thoughts in CBT contexts [20]. Such advances underscore the importance of developing theoretical frameworks that can accommodate both technological sophistication and cultural sensitivity in digital therapeutic design.
Despite these achievements, challenges persist. User engagement, privacy concerns, and the digital therapeutic alliance are ongoing research priorities. Contemporary solutions integrating gamification, biofeedback, and AI-driven personalization show particular promise for improving efficacy and retention, while also addressing the need for culturally responsive and emotionally intelligent therapeutic systems [21–23]. The rapid pace of technological advancement necessitates theoretical models that can guide the ethical and effective implementation of these emerging capabilities in diverse mental healthcare contexts.
To explore how meaningful psychological bonds with places can be translated into VEs, it is essential to first establish a clear theoretical foundation. Place attachment theory provides a lens for understanding human relationships with their environments and has been widely applied in contexts ranging from urban planning to disaster resilience. Although the term “place attachment” is widely used, it is not a univocal concept. As highlighted by Inalhan et al. [24], definitions range from Lewicka’s [11] emphasis on psychological and affective components to organizational and spatial dimensions, particularly relevant in workplace or institutional contexts. In light of these variations, it is important to specify the theoretical stance adopted in this study.
This paper builds primarily on the psychological and environmental perspectives articulated by Scannell and Gifford [5], who conceptualize place attachment as a multidimensional construct consisting of person, process, and place dimensions. This tripartite framework represents the mainstream psychological definition and allows for an integrated understanding of emotional, cognitive, and behavioral bonds to a location. Scannell and Gifford’s [5] tripartite model emphasizes the emotional, cognitive, and behavioral dimensions of attachment, accounting for both individual and collective experiences. Accordingly, this study defines place attachment as the emotional, cognitive, and behavioral bonds that individuals or groups develop with specific places, shaped by personal experiences, social relationships, and the symbolic or functional meanings attached to those places. This definition provides a conceptual anchor for examining how such bonds might emerge, persist, or be transferred within non-traditional or VEs.
Building on this foundation, elements from Williams and Vaske [25] are incorporated, particularly their influential conceptualization of place identity and place dependence. Place identity refers to the extent to which a place contributes to an individual’s sense of self, while place dependence reflects the functional value that a place holds in fulfilling specific needs or goals. These two components have become widely adopted in quantitative research and can be meaningfully adapted to virtual settings, offering a useful structure for measuring place attachment in digitally mediated environments. In the context of this study, they also provide conceptual tools for examining how users interact with and assign meaning to immersive digital landscapes. By applying these dimensions to VEs, it becomes possible to assess not only whether users feel emotionally connected to a virtual space, but also whether they perceive it as fulfilling meaningful psychological or functional roles. Schultebraucks et al. [26] highlighted its neurobiological underpinnings, linking it to stress regulation and memory processing. Additionally, place attachment has been shown to enhance community identity and promote both well-being and pro-environmental behaviors [27].
However, the rise of global mobility, hybrid identities, and digital connectivity is reshaping how individuals experience place. As Ujang [28] notes, traditional spatial attachments are increasingly complicated by mobile and virtual ways of living, which give rise to more fluid and placeless forms of connection. In this evolving context, the concept of place attachment must be re-evaluated to remain relevant.
VEs, though lacking physical tangibility, may offer alternative spaces where emotional and symbolic bonds can still be cultivated, particularly for those who are displaced from familiar environments, such as international students or migrants. This study engages with the possibility that immersive virtual landscapes can support meaningful forms of attachment, drawing from established psychological models while adapting them to digitally mediated settings. In doing so, it aims to bridge the gap between traditional theories of place attachment and contemporary lived experiences shaped by digital technologies.
VEs offer innovative opportunities to simulate meaningful place experiences by blending sensory immersion with interactive design. In this study, the term “virtual reality” (VR) refers specifically to immersive VEs accessed through head-mounted displays (HMDs) such as Oculus Rift or HTC Vive. These systems allow users to navigate and engage with fully synthetic three-dimensional spaces in real time, often producing a strong sense of presence and psychological immersion. While related technologies such as augmented reality (AR), mixed reality (MR), and extended reality (XR) integrate virtual elements into the physical world to varying degrees, the focus here is on fully immersive VR that temporarily detaches users from their physical surroundings.
Effective virtual place-making relies on three primary components: presence [29], coherence [30], and interactivity [31]. These factors contribute significantly to emotional engagement, which is crucial in both therapeutic and affective design contexts. Prior research has shown that VR-based CBT can yield mental health outcomes comparable to or better than pharmacological treatments for conditions such as major depressive disorder [32]. Moreover, the emotional design of avatars and virtual characters can further enhance feelings of presence, engagement, and user empathy, an effect particularly relevant in therapeutic environments [30].
Recent empirical studies strengthen the view that VR can replicate some of the restorative qualities of real-world natural settings. For example, exposure to virtual green environments has been found to reduce cortisol levels, improve mood, and increase heart rate variability, physiological indicators associated with stress reduction [33]. These effects have been observed across a range of user groups, including individuals in high-stress occupations and patients with chronic pain or psychological conditions. A 2024 randomized controlled trial found that VR-based biofeedback interventions significantly outperformed traditional approaches in lowering subjective stress and anxiety, largely due to their immersive and adaptive design [34]. In a separate randomized controlled trial protocol, a VR-based positive psychological intervention was designed for dialysis patients with comorbid depression, aiming to enhance emotional well-being through immersive exposure to natural and therapeutic environments [35]. These findings suggest that even brief virtual exposure to natural landscapes can produce meaningful psychophysiological benefits, especially in settings where access to real environments is limited.
Additionally, research on user experience highlights that the sense of “being there” in a virtual landscape, achieved through coherent sensory cues and spatial design, can evoke emotions of familiarity, tranquility, and attachment [36, 37]. User experiences in VEs are significantly enhanced when the setting includes natural features such as forests or water bodies. These familiar and biophilic landscapes have been shown to promote relaxation and psychological restoration [38, 39]. Importantly, VEs can be both professionally guided (e.g., in clinical settings) and self-directed (e.g., in home-based emotional regulation), expanding their applicability and accessibility.
Despite the growing potential of VR in therapeutic and experiential applications, significant design challenges remain. One central dilemma involves balancing visual realism with emotional comfort. Excessively photorealistic VEs have been shown to evoke anxiety or uncanny responses, as explained by the uncanny valley effect [40, 41], while overly abstract environments may lack sufficient emotional engagement [42]. To mitigate this, adaptive systems incorporating real-time biofeedback, such as heart rate or skin conductance, are increasingly explored as a means to dynamically align VR stimuli with users’ physiological and emotional states [43].
Altogether, these findings support the idea that VR environments are not just technological novelties but can serve as psychologically meaningful places. By simulating natural settings and engaging users on sensory, emotional, and cognitive levels, immersive VR has the capacity to support place-like experiences and the formation of emotional bonds akin to those found in physical environments. This sets the stage for exploring whether and how users may develop a sense of place attachment in virtual landscapes, a question central to the following section.
Although place attachment is often described in universal psychological terms, the ways in which individuals form, interpret, and sustain emotional bonds with places are profoundly shaped by cultural contexts. Lewicka [11] highlighted how cultural background influences place attachment patterns, demonstrating that the way people connect with places is deeply rooted in their cultural context and social values. These cultural variations manifest in different ways people perceive, interact with, and form emotional bonds with both physical and VEs.
Digital health technologies face unique challenges in culturally heterogeneous populations. Torous et al. [1] emphasized the importance of cultural adaptation in digital mental health interventions, highlighting how tailoring digital solutions to specific cultural contexts can significantly improve user engagement and treatment outcomes. Cultural values significantly influence therapeutic expectations and engagement [10]. While Western mental health models often prioritize individual autonomy and privacy, collectivist societies may emphasize family involvement and communal support [44–46]. Digital therapeutic systems that incorporate culturally relevant elements, such as local symbols, architectural motifs, and familiar natural landscapes, have been shown to enhance emotional resonance and treatment effectiveness [47, 48]. This culturally adaptive approach fosters greater emotional engagement and user trust in mental health interventions.
Cultural sensitivity extends beyond visual design to encompass deeper aspects of human-environment interaction. Khilnani et al. [49] emphasized that technologies that accommodate cultural variations in communication patterns and social norms are more likely to achieve sustained user engagement and therapeutic effectiveness, particularly in diverse healthcare settings. This includes considerations of personal space preferences, color symbolism, social interaction styles, and even temporal orientations that vary across cultures. For instance, cultures with high-context communication styles may require more nuanced environmental cues and indirect therapeutic approaches in virtual settings, while low-context cultures might benefit from more explicit and direct therapeutic interactions.
Furthermore, the concept of “place” itself carries different cultural meanings. Indigenous communities often view places as sacred and interconnected with spiritual well-being, a perspective deeply rooted in their cultural and spiritual practices [50]. This presents both opportunities and challenges when designing digital therapeutic interventions that aim to support mental wellness in culturally diverse settings. Understanding these cultural nuances is crucial for developing effective cross-cultural digital mental health solutions that respect and leverage diverse cultural perspectives on place and healing.
Despite significant progress, critical gaps hinder the integration of digital technologies, place attachment theory, and mental healthcare. One major limitation is the lack of longitudinal research on the durability of place attachment formed in virtual settings. Current studies predominantly focus on short-term outcomes, leaving questions about the long-term psychological impact and sustained therapeutic benefits of VPA largely unanswered. Additionally, metrics for evaluating emotional engagement and psychological outcomes in VEs remain inconsistent, impeding cross-study comparisons. The absence of standardized assessment tools specifically designed for VPA creates challenges in establishing evidence-based guidelines for therapeutic VR design and implementation.
Another significant gap lies in understanding the neurobiological mechanisms underlying VPA. While neuroscientific research has begun to explore how the brain processes VEs, there is limited understanding of how VPA compares to physical place attachment at the neural level. This knowledge gap constrains the development of more effective therapeutic interventions based on brain-environment interactions.
Emerging research on augmented and MR environments offers exciting potential for blending physical and digital realms, enabling “phygital” therapeutic interventions. These hybrid approaches could address some limitations of purely VEs by maintaining connections to physical places while enhancing them with therapeutic digital elements. For instance, AR-based therapeutic tools could overlay calming virtual elements onto stressful real-world environments, creating personalized therapeutic spaces that users can access anywhere.
Meanwhile, adaptive algorithms leveraging AI can enhance personalization, dynamically adjusting virtual settings to user preferences and therapeutic responses. Machine learning approaches could analyze user behavior patterns, physiological responses, and self-reported outcomes to continuously optimize VEs for individual therapeutic needs. This personalization could extend to cultural adaptation, automatically adjusting environmental elements based on users’ cultural backgrounds and preferences.
Ethical considerations also present significant research opportunities and challenges. Issues of data privacy, informed consent in immersive environments, and the potential for technology dependence require careful investigation. Additionally, questions about equity and accessibility in digital therapeutic interventions need to be addressed to ensure that benefits are not limited to technologically privileged populations.
Bridging the gaps between theory, technology, and practice requires interdisciplinary collaboration. Future research should prioritize scalability, cultural adaptability, and ethical considerations to maximize the potential of digital therapeutic spaces in addressing global mental health challenges. This includes developing frameworks for integrating place attachment theory with emerging technologies, establishing international standards for virtual therapeutic environments, and creating training programs for mental health professionals to effectively utilize these new tools.
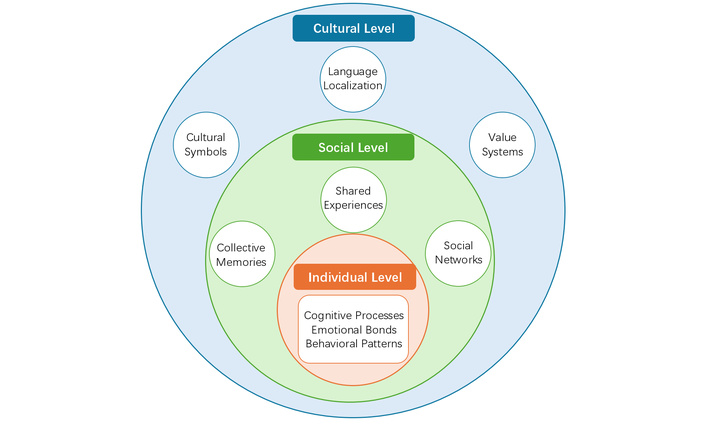
The integration of place attachment theory into digital health technologies presents a novel theoretical framework that merges environmental psychology with digital therapeutics (Figure 1). Traditionally, place attachment theory has been used to understand the emotional bonds between individuals and physical spaces [5]. However, the advent of digital environments, particularly immersive technologies like VR, necessitates a rethinking of these emotional connections. This framework posits that place attachment is not confined to physical spaces but can extend into virtual spaces, where individuals can form strong, meaningful emotional bonds [51].
At its core, the framework rests on three critical assumptions: (1) the psychological mechanisms behind place attachment are not inherently tied to physical spaces, (2) digital environments, when designed appropriately, can foster meaningful emotional connections, and (3) VR technology can create therapeutic spaces that support psychological well-being. This theoretical approach is supported by evidence from neuroscience research examining how VEs can stimulate neural responses similar to real-world spaces [52]. For instance, studies have demonstrated that virtual spaces can activate brain regions associated with spatial navigation, memory, and emotional regulation, functions typically associated with physical places [53].
The framework operates on several analytical levels: individual (micro), social (meso), and cultural (macro), enabling a comprehensive analysis of how digital environments can foster attachment and facilitate therapeutic outcomes. At the individual level, the framework investigates cognitive processes, emotional bonding mechanisms, and behavioral adaptations in VEs. Research on cognitive psychology highlights how spatial cognition and learning affordances in VEs can shape memory and attention, processes central to the formation of place attachment [54]. Social-level dynamics in VEs include how they facilitate collective identity formation, social support networks, and shared meaning-making. Research shows that online communities, such as VR-based mental health groups, strengthen group cohesion through shared identity and provide peer-based emotional support [55, 56]. Additionally, collaborative virtual spaces (e.g., multiplayer games) enable shared meaning-making by fostering structured social interactions [57]. At the cultural level, virtual spaces must accommodate diverse norms and values. Studies indicate that cultural adaptation, such as tailoring content to local health literacy levels, reduces alienation and improves engagement [58]. Cross-cultural research further confirms that social presence in VEs varies significantly across cultures, necessitating culturally sensitive design [59].
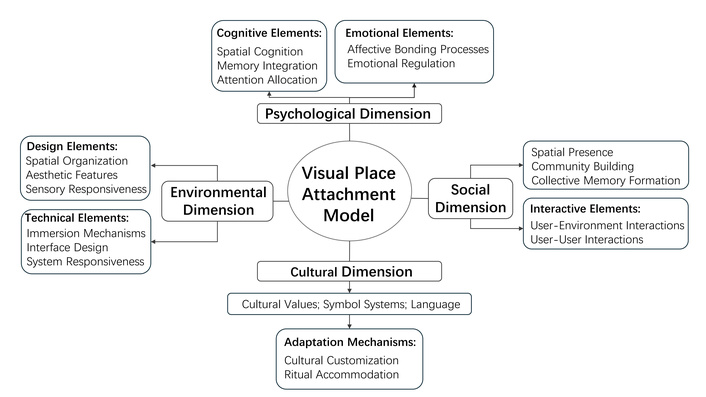
Building on the premise that emotional bonds can form in digital environments, the concept of VPA emerges as an extension of traditional place attachment theory. The Virtual Place Attachment Development Model (VPADM), proposed here, provides a comprehensive framework for understanding the development of emotional bonds to virtual spaces. This model consists of four key dimensions: psychological, social, environmental, and cultural, each of which plays a critical role in how VEs are experienced and how attachments are formed (Figure 2).
The psychological dimension encompasses both cognitive and emotional elements. Cognitive aspects include spatial cognition, memory integration, and attention allocation, which are crucial for users to navigate and emotionally invest in digital spaces. Research in VEs has shown that users develop spatial understanding and mental models through interaction with digital spaces, similar to how they navigate physical environments, which contributes to their sense of presence and attachment [60]. On the emotional side, affective bonding processes and emotional regulation in virtual spaces are essential for attachment formation. Studies on emotional experiences in digital environments suggest that users’ ability to regulate and express emotions in virtual settings can significantly influence their engagement levels and psychological well-being [61].
The social dimension emphasizes the role of interpersonal dynamics in virtual spaces. VEs provide opportunities for social presence, community building, and collective memory formation, all of which contribute to the emotional attachment users feel toward these spaces [62]. Research in social psychology has shown that shared experiences in virtual spaces, such as collaborative therapeutic activities, can create strong bonds among users, enhancing the therapeutic efficacy of digital health interventions [63]. Additionally, interactive elements such as user-environment and user-user interactions play an important role in fostering group dynamics and strengthening attachment [64].
The environmental dimension involves both design and technical elements that shape the virtual space. Design elements like spatial organization, aesthetic features, and sensory stimulation are critical in creating a sense of immersion, which has been shown to enhance emotional connection in VEs [65]. The technical dimension focuses on aspects like immersion mechanisms, interface design, and system responsiveness, which determine how users interact with and feel engaged in the VE. As Slater and Wilbur [66] demonstrate, the technological aspects of immersion and the resulting psychological sense of presence are crucial to fostering user engagement, as they enable more natural and emotionally resonant interactions within the VE.
Finally, the cultural dimension addresses the ways in which virtual spaces can be adapted to reflect cultural values, symbols, and practices. The integration of cultural elements such as language, symbol systems, and value representations ensures that VEs are not only accessible but meaningful to users from diverse backgrounds [67]. This dimension also includes adaptation mechanisms like cultural customization and ritual accommodation, which, as demonstrated in cross-cultural design research, are essential for creating digital health interventions that effectively engage diverse user populations and promote inclusive therapeutic experiences [68].
To demonstrate the comprehensive implementation of the VPADM model, consider a sophisticated digital mental health intervention called “Cultural Bridge VR”, specifically designed for international students experiencing homesickness and cultural adjustment difficulties. This platform exemplifies how each dimension of the VPADM can be operationalized into concrete therapeutic features and design elements.
The psychological dimension is implemented through advanced spatial cognition support and emotion regulation mechanisms. The platform creates personalized VEs that mirror users’ hometown landscapes, utilizing machine learning algorithms to analyze users’ interaction patterns and automatically adjust environmental elements to optimize emotional responses. For instance, when biometric sensors detect elevated stress levels, the system might gradually introduce familiar environmental cues such as childhood neighborhood sounds, seasonal changes from the user’s home region, or architectural elements that trigger positive autobiographical memories. Memory integration is facilitated through interactive storytelling features where users can create and share virtual representations of significant personal spaces, allowing them to process emotional experiences while maintaining a connection to their cultural roots.
Social dimension implementation focuses on creating meaningful interpersonal connections through culturally-informed community features. The platform establishes virtual cultural centers where users from similar backgrounds can participate in synchronized activities such as traditional cooking sessions, religious or spiritual practices, and cultural celebrations. These shared experiences are designed to recreate the collective memory formation processes that occur in physical communities. Advanced avatar systems allow users to express cultural identity through customizable appearance, clothing, and gesture patterns that reflect their cultural communication styles. Peer mentorship programs pair newcomers with more experienced international students within virtual guidance spaces, facilitating knowledge transfer and emotional support networks.
The environmental dimension is operationalized through sophisticated design implementation protocols that translate cultural preferences into immersive technical features. Visual design elements include culturally appropriate color palettes, architectural styles, and natural landscape representations that align with users’ aesthetic expectations and emotional associations. Spatial organization reflects cultural concepts of privacy, community interaction, and sacred versus secular spaces. Advanced technical implementation includes haptic feedback systems that recreate tactile experiences from users’ home environments, spatial audio that reproduces familiar soundscapes, and dynamic lighting systems that adjust according to cultural preferences for brightness, warmth, and temporal rhythms. Interface design adapts to cultural interaction patterns, supporting both direct and indirect communication styles through customizable interaction modalities.
Cultural adaptation represents the most sophisticated aspect of the implementation, translating abstract cultural values into concrete intervention strategies. Language localization extends beyond translation to incorporate culturally appropriate communication styles, including hierarchical address forms, indirect communication patterns, and culture-specific therapeutic terminology. Visual symbolism integration includes meaningful cultural motifs, religious or spiritual symbols, and traditional artistic elements that enhance emotional resonance. Therapeutic approach adaptation combines evidence-based Western psychological interventions with traditional healing practices, such as integrating mindfulness meditation techniques rooted in Buddhist traditions, family-oriented therapy approaches reflecting collectivist values, or Indigenous wellness concepts that emphasize human-nature connection. Ritual accommodation features allow users to participate in virtual versions of important cultural practices, such as prayer spaces, meditation gardens, or ceremonial environments that support spiritual and emotional well-being.
This comprehensive implementation demonstrates how the VPADM framework transforms abstract psychological constructs into actionable design elements and therapeutic strategies within digital health platforms. The model’s effectiveness lies in its systematic approach to creating VEs that foster genuine emotional attachment through culturally resonant, socially meaningful, and psychologically engaging experiences. By addressing all four dimensions simultaneously, the framework enables the development of digital therapeutic spaces that not only provide clinical benefits but also serve as bridges between users’ cultural identities and modern mental health interventions, potentially revolutionizing cross-cultural therapeutic practice in digital contexts.
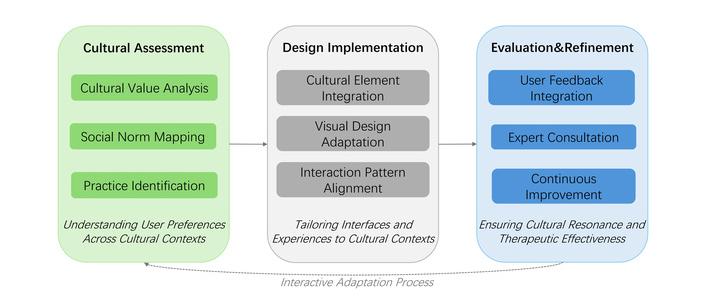
Cultural adaptation represents a fundamental prerequisite for effective virtual mental health interventions, as therapeutic outcomes are intrinsically linked to cultural resonance and user acceptance. A central aspect of this framework is the recognition of cross-cultural dynamics in virtual spaces, particularly the need for cultural adaptation. The Cultural Adaptation System for Virtual Environments (CASVE) is designed to ensure that digital health technologies are culturally appropriate and effective across diverse populations. The system consists of three main components: cultural assessment, design implementation, and evaluation and refinement.
The cultural assessment framework involves analyzing cultural value systems, social norms, and traditional practices to understand the needs and preferences of different user groups. This comprehensive assessment must consider multiple cultural dimensions beyond the traditional individualism-collectivism dichotomy, including power distance, uncertainty avoidance, temporal orientation, and communication patterns. This is particularly important in therapeutic settings, where cultural sensitivity can greatly affect engagement and therapeutic outcomes [69]. For example, some cultures may emphasize community-based therapy, while others may prioritize individual healing, influencing how virtual spaces should be designed and utilized. Recent systematic reviews have highlighted the critical importance of cultural adaptation in digital mental health interventions. For example, recent empirical evidence by Albor et al. [70] highlights how cultural adaptation significantly improves the user experience of digital mental health tools. Their study investigated internet-delivered CBT programs adapted for college students in two Latin American countries. By integrating culturally relevant elements, such as localized language, familiar visual metaphors, and context-specific scenarios, the intervention achieved greater user satisfaction, engagement, and psychological outcomes. Additionally, McDermott et al. [71] demonstrated in their systematic review that culturally adapted psychological interventions for refugees and asylum seekers showed significantly higher treatment engagement and efficacy compared to standardized approaches, with effect sizes increasing by 40–60% when cultural elements were appropriately integrated.
These findings align with the goals of the CASVE model, underscoring that cultural alignment is not merely an ethical imperative but also a determinant of clinical efficacy. Similarly, research in Asian contexts has demonstrated that incorporating traditional healing symbols and family-oriented therapeutic approaches into digital interventions significantly enhances user acceptance and therapeutic engagement compared to Western-standardized tools [48].
The design implementation protocol focuses on integrating cultural elements into virtual spaces, ensuring that visual design, spatial organization, and interaction patterns align with cultural preferences [72]. This includes adapting language, modifying treatment approaches, and adjusting communication styles to ensure cultural relevance and user comfort. Cultural adaptation must extend beyond surface-level modifications to encompass deeper structural elements of the VE, including avatar representation, social interaction mechanics, and therapeutic goal-setting approaches.
For instance, in collectivist cultures, such as many Asian or Latin American societies, therapeutic environments that emphasize community, shared ritual, or family-oriented interaction may foster stronger virtual experiences and be more effective. Designing VR environments that reflect these orientations, through avatar interaction styles, space layout, or symbolic content, can support stronger emotional engagement and place attachment. A recent study suggests that when users perceive their avatars to be self-congruent, aligned with their personal or cultural identity, their sense of social presence in VEs is significantly enhanced [73]. These factors are critical in virtual therapeutic contexts, as increased presence is known to support stronger therapeutic alliance and engagement, particularly among culturally diverse populations [74]. Technical implementation considerations include culturally appropriate color schemes (such as avoiding white in contexts where it symbolizes mourning), spatial configurations that reflect cultural concepts of privacy and community, and interaction modalities that align with cultural communication patterns (direct versus indirect communication styles). Additional considerations include culturally appropriate sound design, gesture recognition systems that accommodate culture-specific nonverbal communication, and adaptive user interfaces that reflect cultural preferences for information hierarchy and visual organization.
Finally, the evaluation and refinement system ensures that the VE is effective in promoting cultural resonance. The Intercultural Sensitivity Scale (ISS), adapted for use in VR, serves as a validated instrument to assess users’ perception of cultural authenticity and belongingness within virtual therapeutic environments. It captures dimensions like interaction engagement, respect for cultural differences, confidence, and enjoyment, offering measurable insights into how culturally tailored VR content fosters psychological engagement [75]. Continuous improvement processes, such as integrating user feedback and expert consultation, allow for the refinement of virtual spaces to better meet the needs of diverse populations [76] (Figure 3).
Evaluation must also consider how cultural context mediates user perceptions of “presence”, safety, and emotional connectedness in VR. Contemporary research emphasizes the need for culturally adapted assessment frameworks that move beyond traditional Western-derived metrics [77]. While comprehensive evidence is still emerging, research has shown that integrating culturally grounded and Indigenous community-based evaluation principles may enhance the validity and user engagement of digital mental health interventions in specific cultural contexts [78]. For instance, McNeill [79] integrated kaupapa Māori principles, including pōwhiri ceremonies and whakapapa storytelling, into virtual agent designs, resulting in stronger cultural resonance and improved engagement measures among Māori participants. Similarly, the Shifa VR project (2021) employed Somali community-based participatory assessment tools, co-developed with community members, demonstrating culturally informed VR platforms’ greater acceptance and trust [80]. These studies highlight the importance of embedding Indigenous evaluation frameworks to accurately capture therapeutic outcomes across diverse cultural groups. For example, collectivist cultures may require assessment tools that evaluate group cohesion and social harmony within VEs, while individualist cultures may focus more on personal agency and self-efficacy measures. Furthermore, evaluation protocols must account for intergenerational differences within cultural groups, as digital natives and older adults may experience VEs differently, regardless of shared cultural background.
In summary, the CASVE model recognizes that cultural diversity is not a challenge to be minimized but a core design principle in developing emotionally resonant VEs. As global mental health disparities continue to widen, culturally adapted VR interventions represent a scalable solution for reaching underserved populations while maintaining therapeutic effectiveness. As digital mental health interventions become increasingly global, designing for cross-cultural place attachment will be essential for achieving therapeutic outcomes across diverse populations. Future research should prioritize the development of automated cultural adaptation systems that can dynamically adjust VEs based on user cultural profiles, potentially revolutionizing the scalability and effectiveness of cross-cultural digital mental health interventions.
The implementation of this theoretical framework requires the integration of technical, therapeutic, and cultural mechanisms. Successful implementation demands a multi-stakeholder approach addressing technological capabilities, clinical workflows, and cultural acceptance. The technical implementation includes the development of VR platforms, interface design, and integration protocols to ensure seamless user experiences. Moreover, the platform must incorporate interaction mechanisms, customization tools, and feedback systems to enhance engagement [81]. The therapeutic implementation focuses on clinical integration, involving the development of treatment protocols, progress monitoring, and outcome assessment tools. These tools are essential for ensuring that digital health interventions are effective and adaptable to individual therapeutic needs. Additionally, professional support mechanisms, including therapist training and supervision protocols, are critical to ensuring that clinicians can effectively use VR in therapy [82]. From a cultural perspective, the implementation process involves adapting digital platforms to reflect cultural contexts. This includes integrating culturally appropriate symbols, language localization, and adapting treatment approaches to ensure they resonate with users from different cultural backgrounds [83].
While this framework presents transformative opportunities for digital health, implementation faces substantial challenges requiring coordinated solutions. Theoretically, bridging physical and virtual attachment requires new conceptual frameworks and validation methodologies. Current assessment metrics, developed for traditional therapy, may inadequately capture VE therapeutic mechanisms, necessitating VR-specific outcome measures. Technically, challenges include hardware limitations, software interoperability, and accessibility requirements [84]. Cost barriers remain significant, requiring substantial infrastructure investment and ongoing maintenance. Additionally, patient data security, cross-platform compatibility, and user-friendly interfaces for varying technological literacy levels present ongoing challenges. Clinically, barriers include treatment validation, safety protocols, and professional training requirements. Reimbursement challenges represent a critical barrier, as insurance coverage for VR therapy remains limited [85]. Healthcare providers identify lack of reimbursement as the biggest adoption barrier [86]. Clinical integration requires new workflow protocols, supervision guidelines, and quality assurance frameworks.
Despite these challenges, the framework offers unprecedented opportunities for revolutionizing mental health care. Longitudinal studies will provide insights into virtual attachment durability, while cross-cultural investigations will establish generalizability across diverse populations. AI integration with VR presents extraordinary opportunities for personalized interventions. Machine learning can analyze user patterns, physiological responses, and engagement metrics to optimize therapeutic content and predict outcomes. Global health applications represent the most significant opportunity, as VR can deliver evidence-based interventions to underserved populations worldwide, transcending geographical barriers. Future priorities include automated cultural adaptation systems, standardized protocols, comprehensive training curricula, and large-scale effectiveness trials across diverse settings.
VR has emerged as a promising medium in psychological therapy, offering immersive environments that can simulate natural or culturally meaningful spaces to support emotional regulation and mental well-being. Recent meta-analytic evidence confirms that VR interventions are effective in treating anxiety disorders, with effect sizes comparable to traditional cognitive behavioral approaches [87]. These benefits are largely attributed to VR’s ability to evoke strong senses of presence and embodiment, which are critical for engaging users in therapeutic tasks. One of the most widely used applications of VR in therapeutic settings is the simulation of restorative natural environments. Browning et al. [88] demonstrated that daily exposure to virtual green and blue spaces significantly reduced anxiety symptoms among university students. Their findings align with a growing body of research that supports nature-based VR as a tool for emotional regulation, especially in populations with limited access to real-world natural settings. Beyond natural simulations, the recreation of personally meaningful or culturally resonant environments in VR has shown promise in enhancing emotional safety and user engagement during therapy [89]. Such environments allow therapists to incorporate autobiographical memories and cultural identity into the therapeutic process, strengthening users’ psychological connection to the virtual setting.
Furthermore, customization and modularity are increasingly recognized as key strengths of VR-based therapy. Lindner et al. [90] illustrated that even single-session, consumer-grade VR exposure therapies, such as public speaking scenarios, can produce clinically significant reductions in anxiety symptoms. These customizable environments allow for graduated exposure, user control, and adaptive feedback, enabling highly individualized treatment plans. Graham et al. [91] extended this line of inquiry by systematically reviewing self-guided VR therapies. They found that user-led interventions targeting specific anxieties, such as social or phobic disorders, were both effective and well-received, highlighting the potential of VR to democratize access to mental health care.
The emotional and cultural resonance of VEs is a critical determinant of their effectiveness in therapeutic contexts. Recent advances in neuroarchitecture and user-centered design underscore the importance of tailoring spatial, visual, and sensory features to elicit positive emotional states [92, 93].
Research has demonstrated that daylight dynamics, ambient color, and spatial geometry significantly influence emotional experiences in virtual spaces. For instance, Payedar-Ardakani et al. [94] used EEG (electroencephalogram) data to show that variations in daylight illumination levels within VR office environments impact users’ architectural perception and mood. Similarly, Jain et al. [95] proposed an adaptive virtual neuroarchitecture system that dynamically modifies virtual spatial layouts and lighting to align with users’ physiological and affective responses, illustrating the potential for emotionally intelligent VR spaces.
Multisensory integration also plays a pivotal role. A study by Masters et al. [96] emphasizes the stress-reducing effects of combining visual, auditory, olfactory, and thermal cues in virtual nature environments. This form of holistic sensory engagement has also been shown to improve emotional regulation, particularly in individuals under high-stress conditions. For instance, Roberts et al. [97] found that mindfulness-oriented interventions incorporating multisensory and interoceptive awareness techniques significantly enhanced emotional regulation in chronic pain patients facing long-term stress. Likewise, a systematic review by Tjasink et al. [98] reported that arts-based interventions effectively reduced burnout and emotional distress among healthcare professionals, one of the most stress-exposed populations. A 2024 systematic review in Virtual Reality further confirms that immersive VR environments integrating soundscapes, spatial texture, and other sensory modalities significantly enhance presence and emotional engagement, thereby strengthening the psychological efficacy of VR-based therapies [99].
Cultural adaptation is another cornerstone of emotionally responsive design. The choice of landscape types, color palettes, and architectural motifs must reflect users’ cultural expectations and spatial familiarity. As demonstrated by Frontiers in Virtual Reality (2024), culturally coherent sensory cues, particularly olfactory elements, can amplify therapeutic impact by triggering autobiographical memory and emotional grounding [100]. Their findings highlight the value of embedding personally meaningful symbols and atmospheres in therapeutic VR design.
Finally, user feedback and iterative evaluation are essential to refining these virtual spaces. Real-time physiological monitoring and post-session feedback, as shown in Mostafavi et al. [101], provide actionable data on users’ comfort, arousal levels, and emotional responses. Such data-driven design allows for continuous improvement, enabling personalized, culturally sensitive, and emotionally attuned virtual therapeutic environments.
The implementation of VR-based therapeutic interventions raises important ethical considerations that must be carefully addressed. Privacy concerns are paramount, as highlighted by Hale et al. [102] in their comprehensive analysis of VE applications in healthcare. They emphasize the need for robust encryption protocols and transparent data handling practices to protect sensitive therapeutic information.
Accessibility remains a critical challenge in the widespread adoption of VR-based interventions. Research by Howard and Gutworth [103] identifies significant disparities in access to digital health technologies among different socioeconomic groups. These disparities are particularly pronounced when considering the substantial upfront costs of VR hardware and the digital infrastructure requirements necessary for effective implementation. These findings highlight the importance of addressing both technological and social barriers in healthcare delivery. To address these challenges, Garrett et al. [104] examine approaches for developing inclusive VR solutions and implementing community-based programs to improve technological accessibility among underserved populations.
Special consideration must be given to adapting VR interventions for diverse user groups. Research by Roberts et al. [105] demonstrates successful adaptations for elderly users through modified interface designs and adjusted interaction parameters, showing significant improvements in usability among older participants. Similarly, Zhao et al. [106] have investigated guidelines for creating accessible VR experiences for users with various physical limitations, emphasizing the importance of customizable interaction methods and alternative feedback mechanisms. Cultural adaptation represents another critical dimension, extending beyond mere language translation to encompass culturally relevant VEs, appropriate therapeutic frameworks, and respect for diverse cultural perspectives on mental health and technology acceptance.
Building upon these foundational ethical and accessibility concerns, several interconnected barriers continue to limit equitable access to VR-based therapeutic interventions. Socioeconomic factors, including the high cost of VR hardware, inadequate internet infrastructure in rural and underserved areas, and disparities in digital literacy, create significant obstacles for vulnerable populations. Rural communities face particular challenges due to limited broadband connectivity, while older adults and individuals with lower educational attainment often experience greater difficulties with technology adoption [107, 108]. These limitations risk reinforcing existing inequalities in mental healthcare access, particularly among marginalized groups.
To address these multifaceted challenges, several strategic approaches warrant consideration. First, the development of lightweight, mobile-compatible VR experiences can reduce hardware costs and improve feasibility in low-resource settings. Second, incorporating multi-language interfaces and culturally adapted content can improve engagement across diverse user groups. This cultural adaptation should encompass not only linguistic elements but also visual representations, narrative frameworks, and therapeutic approaches that align with diverse cultural values and beliefs. Third, community-based deployment models, such as implementation through schools, libraries, or public health centers, can facilitate broader access while simultaneously building local digital health literacy capacity. Additionally, partnerships with community organizations and healthcare providers can help establish sustainable support networks and ensure ongoing technical assistance. These approaches underscore the importance of designing with inclusion as a foundational principle, ensuring that VPA technologies benefit not only tech-savvy urban users but also those historically underserved by mental health systems.
The convergence of place attachment theory and VR technologies has expanded the conceptual boundaries of therapeutic environmental design. Traditionally rooted in physical settings, place attachment is now being adapted to digital spaces, offering new insights into how individuals form emotional bonds with VEs. Recent research by Pantelidis et al. [109] demonstrates that users can develop meaningful connections to VR landscapes, particularly in rural tourism contexts, where dimensions such as accessibility, personal memories, and enhanced spatial understanding contribute to digital place attachment. These findings support the applicability of place attachment theory in immersive environments and affirm its value as a foundational framework for designing emotionally resonant VR therapies.
The integration of AI further enriches this theoretical space. In a Cedars-Sinai pilot, a GPT-4-powered conversational avatar embedded in VR effectively delivered motivational interviewing and CBT to patients with alcohol-associated cirrhosis. The study reported high usability and therapeutic acceptance [110]. Additionally, Steenstra et al. [111] developed an LLM-based virtual counselor whose motivational interviewing matched human-level empathy in alcohol counseling scenarios. These findings illustrate AI avatars’ potential in sustaining emotional connection and personalized guidance in digital environments.
To understand these interactions at a conceptual level, we must revisit theories of presence and affordance. Immersive VR provides affordances, spatial agency, embodiment, and interactivity that underpin users’ sense of presence and emotional engagement [112, 113]. This theoretical extension moves beyond physical-world parallels and highlights VR as an active, emotionally engaging space.
Moreover, real-world and VPA may differ in origin and strength. Users without prior physical attachments to a place can still form strong emotional ties to its virtual counterpart, suggesting that VR-designed environments can stand alone as therapeutic spaces [114]. Together, these insights point to an expanded theoretical framework that combines place attachment, digital embodiment, and AI responsiveness, crucial for designing next-generation VR therapies where emotional resonance, adaptive interaction, and cultural relevance intersect.
The translation of theoretical insights into practical applications has yielded significant advances in digital mental health interventions. Research by Blackmore et al. [115] demonstrates how presence and immersion principles can inform the design of more effective virtual therapeutic environments, resulting in improved treatment outcomes across mood and anxiety disorders. Their mixed-methods study showed that VR-supported mindfulness significantly reduced state anxiety and negative affect while enhancing mindfulness-related cognitive components such as curiosity and decentering.
The impact of this theoretical framework extends beyond clinical applications to influence policy development and technological innovation. A systematic review by Riches et al. [116] documents how VR and immersive technologies are being implemented to promote workplace mental well-being. While reporting generally positive outcomes, the review highlights the absence of consistent implementation frameworks and the need for culturally sensitive adaptation, particularly in diverse organizational and population settings.
Furthermore, this framework has contributed to the development of more sophisticated evaluation models for virtual health interventions. Studies increasingly advocate for combining quantitative measures, such as presence, emotional regulation, and engagement scales, with qualitative approaches that capture subjective experience [117]. For example, Blackmore et al. [115] incorporated semi-structured interviews alongside structured scales to evaluate not just therapeutic outcomes but also how users made sense of the VE, a critical factor in long-term efficacy. Similarly, Yin et al. [118] employed an evidence-based experimental approach combining psychometric assessments with perceptual feedback to examine how virtual restorative environments affected psychological well-being in university students, reinforcing the value of mixed methods in immersive health research.
The complexity of user experience in virtual therapeutic environments, particularly in relation to cultural adaptation and personalization, necessitates evaluation strategies that move beyond traditional quantitative instruments. While standardized measures are essential for ensuring comparability, a comprehensive understanding of how users experience and interpret digital spaces requires qualitative insights. Riches et al. [116] emphasize that cultural symbolism, spatial preferences, and the emotional significance of visual and auditory cues must be considered when designing environments for culturally diverse users.
Following this recommendation, the application of the VPADM and CASVE frameworks should be supported by a mixed-methods evaluation paradigm that includes both structured instruments and exploratory tools such as narrative journals, photo elicitation, and user interviews. This approach is particularly valuable for pilot implementations, cross-cultural adaptations, and longitudinal studies of therapeutic engagement. It allows researchers to capture not only whether interventions are effective, but also how and why they work for different populations.
Acknowledging this methodological imperative, this paper proposes that future validation of the proposed frameworks adopt iterative, mixed-methods strategies aligned with the transdisciplinary nature of digital mental health design. Such strategies ensure that the development of culturally adaptive virtual therapeutic environments is continuously refined based on both performance metrics and lived user experience, preserving the centrality of human-centered design in technologically mediated mental health care.
The quantitative assessment of VEs’ impact on mental health remains a crucial area for future research. While current studies show promising correlational effects, recent methodological reviews stress the need for more robust, standardized metrics. For example, Lundin et al. [119] highlight inconsistent reporting of VR adverse effects, such as cybersickness, and call for better-designed assessment tools to ensure safety and efficacy. Cieślik et al. [120] and Riva [121] stress the lack of unified evaluation protocols in clinical VR research, pointing to the heterogeneity of outcome measures as a critical barrier to progress. This underscores the importance of developing standardized evaluation frameworks for therapeutic VR.
Long-term effects of sustained engagement with virtual therapeutic environments present both opportunities and challenges. XR (encompassing VR/AR/MR) interventions have shown sustained reductions in anxiety and depression and demonstrated cost-effectiveness in preliminary economic evaluations [119, 122]. However, more longitudinal studies are needed to understand how benefits persist or evolve and to balance therapeutic gain against potential habituation or adverse effects.
Ethical considerations and cultural sensitivity are increasingly recognized as critical. AR and VR applications in psychoeducation and stigma reduction have demonstrated effectiveness in improving empathy, attitudes, and knowledge regarding mental illness [121, 123]. But studies also call attention to sample bias and limited cultural diversity, urging more inclusive and representative research design [124, 125]. Ensuring cultural relevance and avoiding cultural mismatch thus remains a vital challenge in therapeutic VR design.
Emerging technologies like AR and MR offer new frontiers for therapeutic intervention. Systematic reviews of AR-based exposure therapy demonstrate clinical efficacy and strong patient-therapist working alliances, while noting limited but promising early results in anxiety and phobia treatment [126]. These innovations could complement VR approaches and create hybrid treatment pathways.
Finally, bridging disciplinary silos is essential. XR interventions combine clinical psychology, user experience design, software engineering, and health economics. As BMC Digital Health’s 2023 review notes, cost-effectiveness evaluations of XR-based care are mixed and often limited by inconsistent reporting, underscoring the need for collaborative, integrative research that spans methodological and domain boundaries [122]. Only such transdisciplinary efforts can realize effective, accessible, and culturally sensitive digital therapeutic environments.
The integration of place attachment theory with digital health technologies represents a paradigm-shifting approach in mental healthcare delivery, offering profound implications for both theoretical development and practical applications. This paper has demonstrated how the systematic incorporation of place attachment principles into virtual therapeutic environments can significantly enhance mental health interventions while expanding our understanding of human-place relationships in digital contexts.
Our theoretical synthesis has revealed several crucial insights. First, the psychological mechanisms underlying place attachment can be effectively translated into VEs, challenging traditional assumptions about the nature of place-based emotional connections. For example, meta-analytic evidence shows that VR exposure therapy yields large effect sizes (Hedges’ g ≈ 1.29) across anxiety-related conditions, confirming that virtual spaces can evoke authentic emotional responses and foster therapeutic connections equivalent to those in the physical world [87]. Second, the successful implementation of place attachment principles in digital health technologies has demonstrated remarkable practical value. Systematic reviews indicate that well-designed VR and AR environments achieve outcomes comparable to traditional therapy, with additional benefits such as enhanced accessibility and customization for underserved and remote populations [126]. Our analysis has also uncovered important implications for cross-cultural applications. The flexibility of VEs, when combined with culturally informed design principles, enables the creation of therapeutic spaces that resonate deeply across diverse users. However, this rapid expansion brings ethical challenges, particularly in user privacy. Experimental studies have shown that adversarial VR designs can inadvertently expose users’ personal data from motion telemetry, raising serious confidentiality concerns that must be addressed [127]. Furthermore, emerging technologies such as AR offer new opportunities for therapeutic interventions. Recent systematic reviews report AR exposure therapies achieve clinically significant reductions in phobic anxiety and sustain strong therapist-patient working alliances, suggesting AR can effectively complement VR in place-based therapy models [126]. Finally, addressing the diverse challenges facing this field will require cross-disciplinary collaboration. Economic analyses and safety evaluations remain uneven in digital therapeutic research, underscoring the need for integrative efforts across psychology, user experience design, engineering, and ethics to ensure interventions are effective, accessible, and culturally sensitive [126, 127].
In conclusion, this integration of place attachment theory with digital health technologies is not merely an incremental advance but a fundamental reconceptualization of therapeutic relationships in virtual spaces. The theoretical frameworks and evidence highlighted provide a foundation for future research and implementation, while the identified challenges and opportunities outline a roadmap for advancing this promising field. As mental healthcare increasingly embraces digital modalities, understanding and harnessing VPA will be critical to creating effective, scalable, and culturally attuned interventions.
AR: augmented reality
CASVE: Cultural Adaptation System for Virtual Environments
CBT: cognitive behavioral therapy
LLMs: large language models
MR: mixed reality
PTSD: post-traumatic stress disorder
VEs: virtual environments
VPA: virtual place attachment
VPADM: Virtual Place Attachment Development Model
VR: virtual reality
XR: extended reality
CY: Conceptualization, Methodology, Writing—original draft, Writing—review & editing. JM: Conceptualization, Methodology, Writing—review & editing, Supervision. BM: Conceptualization, Writing—review & editing, Supervision. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.