Original Article
Original Article

Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
†These authors share the first authorship.
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
†These authors share the first authorship.
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
ORCID: https://orcid.org/0009-0002-1365-2887
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
ORCID: https://orcid.org/0009-0008-5168-7240
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
ORCID: https://orcid.org/0000-0003-0068-2614
Affiliation:
2Secretaría de la Defensa Nacional, Escuela Militar de Graduados de Sanidad, Ciudad de México, CDMX 11200, México
Affiliation:
2Secretaría de la Defensa Nacional, Escuela Militar de Graduados de Sanidad, Ciudad de México, CDMX 11200, México
ORCID: https://orcid.org/0000-0002-0813-3428
Affiliation:
2Secretaría de la Defensa Nacional, Escuela Militar de Graduados de Sanidad, Ciudad de México, CDMX 11200, México
ORCID: https://orcid.org/0000-0002-2518-2803
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
ORCID: https://orcid.org/0000-0002-1555-1740
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
ORCID: https://orcid.org/0009-0004-1462-935X
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
ORCID: https://orcid.org/0000-0003-1043-4905
Affiliation:
1Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan, Edo. Méx 52786, México
2Secretaría de la Defensa Nacional, Escuela Militar de Graduados de Sanidad, Ciudad de México, CDMX 11200, México
Email: jose.ibarra@anahuac.mx
ORCID: https://orcid.org/0000-0003-2489-4689
Explor Neuroprot Ther. 2026;6:1004156 DOI: https://doi.org/10.37349/ent.2026.1004156
Received: November 25, 2025 Accepted: March 05, 2026 Published: May 26, 2026
Academic Editor: Rafael Franco, Universidad de Barcelona, Spain
The article belongs to the special issue Role of Microbiota in Neurological Diseases
Aim: To assess the effect of a synbiotic supplement composed of Enterococcus faecium and agave inulin on cognitive function in older adults with mild cognitive impairment (MCI).
Methods: In a triple-blind randomized crossover trial, nineteen adults aged 64–85 years with MCI received either the synbiotic or an isocaloric vehicle for eight weeks, followed by a three-week washout and treatment crossover. Cognitive outcomes were assessed at baseline, after the first intervention, and after crossover using the Modified Mini-Mental State Examination (MMSE), Rey-Osterrieth Complex Figure Test (RCFT; copy and memory), and Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults (AERAC) self-efficacy scale. Paired and unpaired Student’s t-tests were used for statistical comparisons (p < 0.05).
Results: The synbiotic group showed significant improvement relative to baseline across all domains: MMSE (p = 0.05), AERAC (p = 0.005), RCFT-copy (p = 0.03), and RCFT-memory (p = 0.03). Post-treatment comparisons between groups also favored the synbiotic, with significant differences in MMSE (p = 0.001), AERAC (p = 0.001), RCFT-copy (p = 0.0095), and RCFT-memory (p = 0.001). After crossover, cognitive gains were sustained and reproduced. MMSE scores reached 17.89 ± 1.45 in the synbiotic-first group versus 18.20 ± 0.63 in the control-first group (p < 0.001). RCFT-copy remained high (29.83 ± 4.18 vs. 29.52 ± 5.60, p = 0.0157), while RCFT-memory scores differed (17.56 ± 6.73 vs. 17.20 ± 3.29, p = 0.0005). AERAC scores continued to improve during crossover (82.60 ± 10.49 vs. 85.46 ± 8.28, p < 0.001). No adverse effects occurred.
Conclusions: Synbiotic supplementation significantly improved global cognition, visuoconstructive ability, memory, and functional self-efficacy in older adults with MCI. Benefits persisted beyond the initial intervention and were replicated when the control group received the synbiotic, supporting its potential as a safe and effective strategy to mitigate age-related cognitive decline.
Cognition encompasses the mental processes that enable humans to perceive, interpret, and respond to their surroundings. Aging induces structural and physiological changes in the brain that compromise these functions, often resulting in cognitive decline. Mild cognitive impairment (MCI) represents deterioration greater than expected for age and education, yet without significant loss of independence, and is associated with a higher risk of dementia, particularly Alzheimer’s disease, within five years [1–4].
This progressive decline is linked to neuronal loss, mitochondrial dysfunction, and neuroinflammation, which impair neuroplasticity and cerebral metabolism, mainly affecting the hippocampus. Proinflammatory cytokines such as IL-1β, IL-6, and TNF-α downregulate brain-derived neurotrophic factor (BDNF), while oxidative stress from reactive oxygen species (ROS) contributes to cellular damage and apoptosis [5–9].
Recent evidence highlights the gut-brain axis as a regulator of cognitive health. The intestinal microbiota communicates with the brain through neural, immune, and metabolic pathways. A balanced microbiota produces short-chain fatty acids (SCFAs), particularly butyrate, which suppresses inflammation and upregulates BDNF. Conversely, dysbiosis reduces SCFA production, promoting neuroinflammation and cognitive decline [10–16].
Probiotics such as Enterococcus faecium enhance the growth of butyrate-producing bacteria (Faecalibacterium prausnitzii, Roseburia spp.) and stimulate IL-10 synthesis through Toll-like receptor signaling, favoring BDNF expression and cognitive improvement [17–21]. Prebiotics like agave inulin selectively promote beneficial bacteria and exert anti-inflammatory effects at doses around 8 g/day [22–28].
When combined as synbiotics, probiotics and prebiotics act synergistically to modulate microbiota composition and increase SCFA levels [29–31]. Given the growing prevalence of cognitive impairment and limited pharmacologic options, synbiotic supplementation emerges as a promising non-pharmacological strategy to preserve cognition and delay dementia progression.
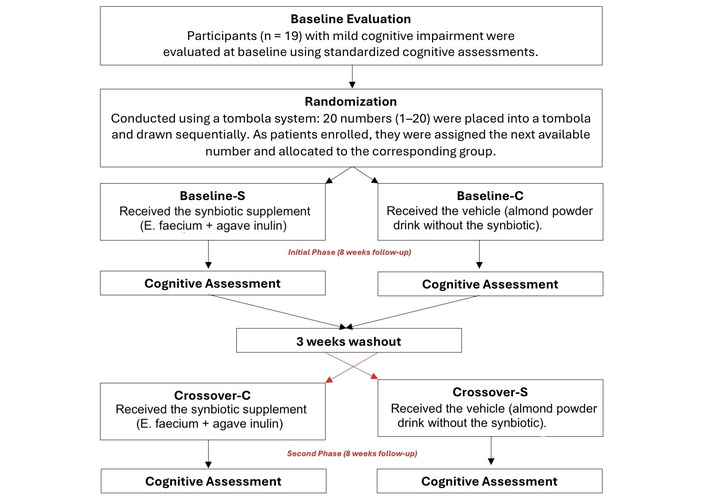
A triple-blind, randomized crossover trial with longitudinal follow-up was conducted to assess the association between cognitive performance in older adults and a synbiotic supplement. Participants, psychological assessors, and the statistical analyst were unaware of group assignments at all stages. The study was conducted at Universidad Anáhuac, México City, with recruitment beginning in mid-December 2022 and final baseline evaluations completed in mid-February 2023. Following completion of the baseline assessments, participants entered the intervention phase according to the study protocol. All procedures adhered to the Declaration of Helsinki and the Mexican standard NOM-012-SSA3-2012 for human research. Ethical approval was granted by the Universidad Anáhuac México, Campus Norte, Research Committee, Faculty of Health Sciences (Approval ID: CONBIOETICA-15-CEI-004-20160729). The trial was registered at ClinicalTrials.gov (NCT05688618).
Adults aged 64–85 years with aging-related cognitive decline consistent with MCI were eligible. Diagnosis was established by clinical and psychometric evaluation. All participants provided written informed consent prior to enrollment. Inclusion criteria: Age 64–85 years; signs of mild cognitive deterioration; signed informed consent. Exclusion criteria: Age 64–85 years without cognitive impairment; diagnosed advanced cognitive decline (e.g., Alzheimer’s disease); comorbidities known to affect cognition (e.g., diabetes mellitus, prior cerebral ischemia, traumatic brain injury, or obesity); refusal to provide written informed consent. Elimination criteria: Development of new comorbidities affecting cognition during the study; adverse effects attributable to the supplement; failure to take the synbiotic for > 1 consecutive week; withdrawal of consent; or missing three consecutive doses.
Nineteen participants completed all phases. Given the exploratory nature of the trial and the feasibility of close follow-up in a triple-blind crossover design, this sample size was deemed adequate to provide preliminary evidence of effect, allowing detection of an effect size of 0.1 and enabling both within-group and between-group comparisons across outcomes.
Participants were recruited via snowball sampling supported by community outreach, posters, and social media. Interested individuals telephoned the study team for brief screening, underwent baseline cognitive assessment, and were then randomized by simple lot to the control or experimental group. No age- or sex-stratification was performed.
Before recruiting patients, twenty numbers (from 1 to 20) were placed in a tombola. Afterwards, each number was randomly selected from the tombola and sequentially allocated to one of three groups, until reaching 10 numbers per group. Each number represented the time the patient was to be enrolled. This way, once the recruitment was initiated, the first patient was assigned number one; the second was number two, and so on. In this fashion, each patient was allocated (according to the time of enrollment) to the group to which their number corresponded. At the end of the study, one of the patients was eliminated because he did not follow the instructions for preparing the synbiotic.
The synbiotic consisted of E. faecium (SF68; 1 × 107 CFU) and agave inulin (8 g) provided as a tasteless, odorless, colorless powder dissolved in a powdered almond drink. The control (vehicle) was the almond drink without the synbiotic. Participants consumed one dose daily on an empty stomach for 8 weeks, followed by a 3-week washout. After washout, groups crossed over: the original control group received the synbiotic and the original experimental group received the vehicle for another 8 weeks, after which cognitive assessments were repeated (see Figure 1). Adherence was monitored by daily photographs submitted via WhatsApp and logged electronically; the same channel enabled real-time adverse-event reporting.
E. faecium SF68 is a strain that has decades of clinical use as a probiotic. It does not belong to the hospital-associated clade (A1) responsible for vancomycin-resistant enterococci (VRE). It lacks major acquired antibiotic resistance genes characteristic of pathogenic hospital strains; does not carry typical virulence genes, and has an extensive history of tolerability in children, adults, and elderly patients, including vulnerable populations in controlled trials [32–35].
Both synbiotic and placebo powders were prepared and packaged under strict aseptic conditions in a laminar-flow hood. All materials were disinfected with 70% ethanol and exposed to ultraviolet light for 30 minutes. Each daily dose contained 25 g of unsweetened almond powder; the experimental sachets included 8 g of synbiotic plus 17 g of almond powder. Packages were visually identical and labeled only with the study logo. To maintain blinding, each daily sachet was supplemented with 20 g of unsweetened almond beverage powder, matching the vehicle used in the placebo. In contrast, the placebo consisted solely of 25 g of commercially sourced unsweetened almond drink powder without any probiotic or prebiotic components. Both the synbiotic and placebo were repackaged in identical plastic sachets under laminar-flow sterile conditions to standardize appearance, texture, and handling across groups, preserving the triple-blind design of the study.
The supporting literature assures that restoration of an altered intestinal microbiota may require up to 40 days, and therefore the intervention was extended to 8 weeks to ensure adequate exposure beyond the natural restitution period and to allow stabilization of the synbiotic’s biological effects. Additionally, because probiotic activity diminishes when dosing occurs less frequently than every three days, daily administration was required to maintain effective concentrations of 107–108 CFU, preventing natural washout of the probiotic strain and ensuring consistent colonization potential throughout the trial. As a result, all participants entered the study with their habitual microbiota composition and underwent a supplementation period long enough to surpass the natural microbial turnover cycle, thereby maximizing the likelihood of detecting clinically meaningful cognitive changes attributable to the synbiotic. The synbiotic consisted of E. faecium [1 × 107 CFU; Alimentos Esenciales para la Humanidad (AEH) S.A. de C.V., Ciudad de México, México] and agave inulin (8 g; AEH S.A. de C.V., Ciudad de México, México) provided as a tasteless, odorless, colorless powder dissolved in a powdered almond drink (Almondlessa, Afenlessa Corporation S.A. de C.V., Ciudad de México, México).
Cognitive function was evaluated at baseline and post-intervention using three instruments:
Modified Mini-Mental State Examination (MMSE): A 19-item screening test for cognitive impairment in older adults; scores ≤ 13 suggest impairment [36]. Clinical interpretation of the total score is as follows: scores of 17–19 points are considered within the normal range; scores of 14–16 points are consistent with MCI; and scores ≤ 13 points are suggestive of dementia.
Rey-Osterrieth Complex Figure Test (RCFT): Assesses visuoconstructive ability and visual memory through copy and delayed recall; 18 figure elements are scored and converted to percentile ranks [37–39].
Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults (AERAC): A 26-item measure of self-efficacy in independence, social interaction, and health-protection domains; global scores are classified as low (0–23), moderate (24–56), or high (57–100) [18].
Analyses were performed using GraphPad Prism version 10.5.0 (GraphPad Software, USA). Descriptive statistics are presented as mean ± standard deviation (SD). Normality was assessed using the Shapiro-Wilk test.
For the first intervention period, between-group comparisons were conducted using unpaired Student’s t-tests, and within-group pre-post comparisons were analyzed using paired Student’s t-tests.
Given the crossover design, post-crossover data were analyzed by comparing within-subject changes after each treatment condition (synbiotic vs. control). Paired Student’s t-tests were used to evaluate treatment effects within individuals across periods. Additionally, between-group comparisons during the crossover phase were performed using unpaired t-tests. To minimize potential carryover effects, a three-week washout period was implemented between intervention phases. Although formal testing for period and carryover effects was limited by the sample size, the crossover analysis primarily focused on within-subject comparisons to strengthen inference regarding treatment effects. All tests were two-sided, and a p value < 0.05 was considered statistically significant.
The studied population consisted of 19 adults aged 64 to 85 years (mean ± SD: 77 ± 6.04 years), including 13 females and 6 males. Baseline psychometric assessments were conducted between December 2022 and February 2023 using the three validated instruments: the modified MMSE, the RCFT (memory and copy components), and the AERAC. After completion of the baseline assessments, participants proceeded to the intervention phase according to the study protocol. Table 1 summarizes the demographic characteristics of the participants and the baseline results of each test by group.
Baseline characteristics of participants in the synbiotic and control groups.
| Baseline characteristics | Synbiotic group | Control group | p value |
|---|---|---|---|
| n | 9 | 10 | - |
| Sex (female/male) | 6/3 | 7/3 | - |
| Age (years) | 79.33 ± 4.5 | 74.99 ± 6.6 | 0.11 |
| Baseline results (points) | |||
| Mini-Mental State Examination | 16.78 ± 0.97 | 16.10 ± 2.08 | 0.1923 |
| Rey-Osterrieth Complex Figure Test-memory | 11.06 ± 3.45 | 10.90 ± 2.75 | 0.9142 |
| Rey-Osterrieth Complex Figure Test-copy | 24.74 ± 7.22 | 24.70 ± 6.71 | 0.9891 |
| AERAC test | 68.52 ± 5.06 | 67.69 ± 6.62 | 0.4626 |
AERAC: Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults.
Before supplementation, all participants completed the three psychometric tests. Each test was scored individually, and results are presented as mean ± SD for both groups (Figures 2, 3, 4, 5). Independent t-tests were used for between-group comparisons, and paired t-tests for within-group analyses.
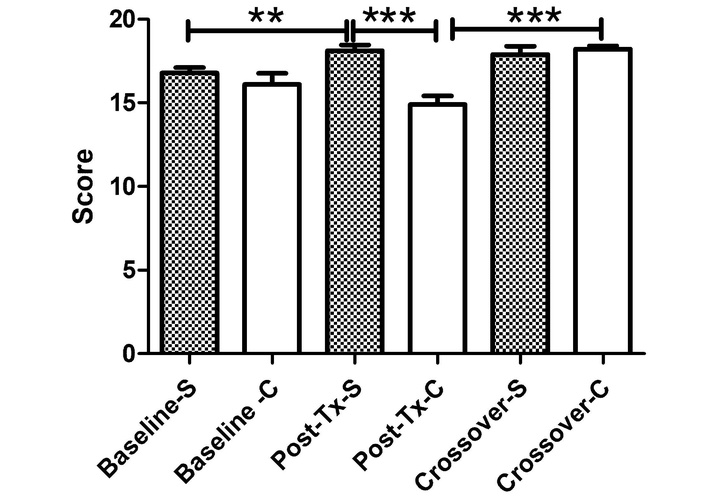
Mini-Mental State Examination (MMSE) scores before, after intervention, and after crossover. This figure illustrates MMSE performance in the synbiotic (S) and control (C) groups across the three assessment phases. During crossover, the former control group showed significant improvement after receiving the synbiotic, while the initially treated group maintained cognitive gains. p values: **p < 0.01; ***p < 0.001. Tx: treatment.
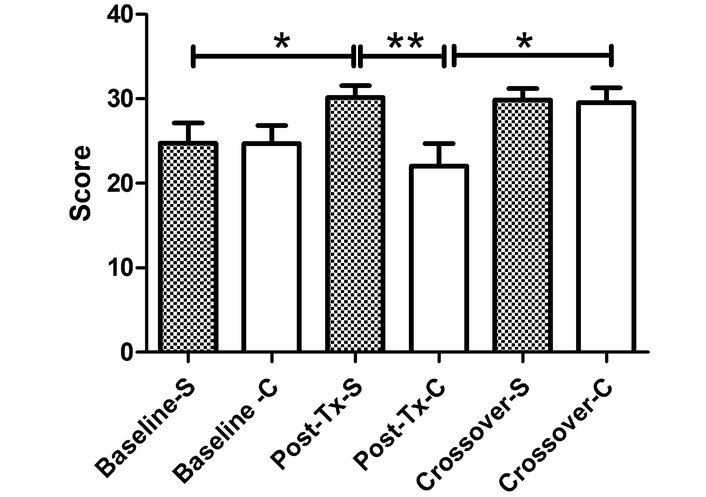
Rey-Osterrieth Complex Figure Test (RCFT)-copy test scores before, after intervention, and after crossover. Bar graph illustrating visuoconstructive performance across baseline, post-treatment, and crossover phases. Participants who switched to synbiotic supplementation during crossover exhibited significant improvement relative to their prior performance. p values: *p < 0.05; **p < 0.01. C: control; S: synbiotic; Tx: treatment.
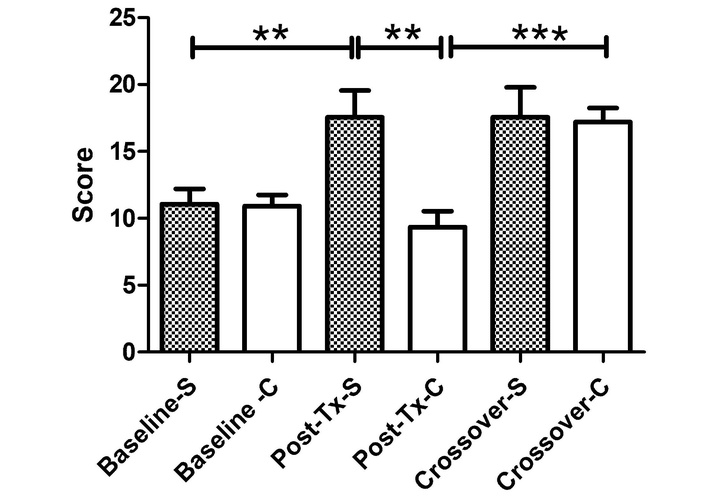
Rey-Osterrieth Complex Figure Test (RCFT)-memory test scores before, after intervention, and after crossover. Bar graph showing visual memory performance assessed through the RCFT-memory test in the synbiotic (S) and control (C) groups across baseline, post-treatment, and crossover phases. During the crossover phase, participants who switched from control to synbiotic demonstrated a marked and statistically significant improvement relative to their post-treatment values, achieving scores comparable to the group originally treated with the synbiotic. These results indicate that synbiotic supplementation consistently enhances visual memory recall, regardless of treatment order. p values: **p < 0.01; ***p < 0.001. Tx: treatment.
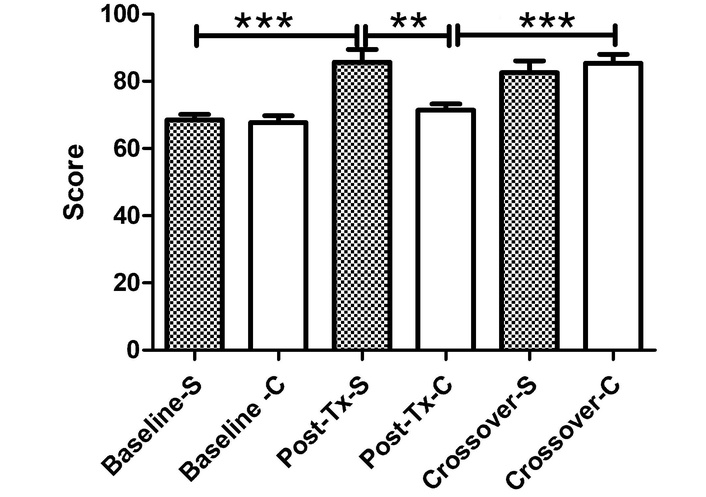
Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults (AERAC) scores before, after intervention, and after crossover. This figure shows AERAC scores, which reflect perceived self-efficacy in daily functioning. During the crossover, both groups demonstrated further functional gains. The former control (C) group improved significantly relative to its own post-treatment performance, while the initially synbiotic (S)-treated group maintained high perceived functional capacity. p values: **p < 0.01; ***p < 0.001. Tx: treatment.
At baseline, cognitive and functional performance were comparable between the synbiotic and control groups across all administered assessments. MMSE scores did not differ significantly between groups (16.78 ± 0.97 vs. 16.10 ± 2.08, p = 0.1923), indicating similar global cognitive status at study entry. Likewise, visuospatial memory measured by the RCFT-memory test showed no significant group differences (11.06 ± 3.45 vs. 10.90 ± 2.75, p = 0.9142), and visuoconstructive ability assessed through the RCFT-copy test was nearly identical (24.74 ± 7.22 vs. 24.70 ± 6.71, p = 0.9891). Baseline functional self-efficacy, evaluated with the AERAC scale, also showed no significant differences between the synbiotic and control groups (68.52 ± 5.06 vs. 67.69 ± 6.62, p = 0.4626). These results confirm that both groups began the intervention under equivalent cognitive and functional conditions.
After eight weeks of supplementation—during which the control group received almond powder alone and the synbiotic group received the same formulation with E. faecium and agave inulin, the same tests were administered to evaluate cognitive changes.
At baseline, global cognitive performance measured by the MMSE was comparable between the synbiotic and control groups (16.78 ± 0.97 vs. 16.10 ± 2.08, respectively; p = 0.1923), indicating similar initial cognitive status.
After eight weeks, participants receiving the synbiotic demonstrated a significant within-group improvement, increasing their MMSE score to 18.11 ± 1.05 (p = 0.0066 vs. baseline). In contrast, the control group showed lower post-treatment scores (14.90 ± 1.59). The between-group comparison at this time point strongly favored the synbiotic (p < 0.001) (Figure 2).
During the crossover phase, participants who initially received the control formulation exhibited a marked cognitive improvement after switching to the synbiotic, reaching 18.20 ± 0.63 (p < 0.001 vs. their own post-treatment values). Meanwhile, participants originally treated with the synbiotic maintained stable cognitive performance during crossover (17.89 ± 1.45). These findings indicate that synbiotic supplementation exerted a reproducible and sustained positive effect on global cognition.
At baseline, visuoconstructive performance assessed through the RCFT-copy task was comparable between groups (24.74 ± 7.22 vs. 24.70 ± 6.71; p = 0.9891).
After eight weeks, the synbiotic group showed significant within-group improvement (30.14 ± 4.22; p = 0.0354 vs. baseline), whereas the control group exhibited lower post-treatment scores (22.00 ± 8.52). The between-group comparison at this time point favored the synbiotic (p = 0.0095). During crossover, participants who switched from control to synbiotic demonstrated further improvement (p = 0.0157 vs. their post-treatment values), achieving scores comparable to the initially treated group (29.52 ± 5.60 vs. 29.83 ± 4.18). These results indicate a robust and reproducible enhancement in visuoconstructive ability following synbiotic supplementation (Figure 3).
Baseline visual memory performance was similar between groups (11.06 ± 3.45 vs. 10.90 ± 2.75; p = 0.9142). Following intervention, the synbiotic group demonstrated significant within-group improvement (17.56 ± 5.96; p = 0.0060 vs. baseline), whereas the control group remained at lower post-treatment values (9.35 ± 3.70). The between-group comparison strongly favored the synbiotic (p = 0.001). During crossover, individuals who switched from control to synbiotic showed marked improvement (p = 0.0005 vs. post-treatment), reaching scores comparable to the initially treated group (17.20 ± 3.29 vs. 17.56 ± 6.73). These findings demonstrate consistent and reproducible benefits of synbiotic supplementation on visual memory (Figure 4).
Baseline AERAC scores were similar between groups (68.52 ± 5.06 vs. 67.69 ± 6.62; p = 0.4626). After eight weeks, the synbiotic group demonstrated a significant within-group improvement (85.70 ± 11.63; p < 0.001 vs. baseline). The control group showed lower post-treatment scores (71.48 ± 5.66), and the between-group comparison favored the synbiotic (p = 0.0015).
Following crossover, participants who switched to synbiotic supplementation showed further improvement (85.46 ± 8.28; p < 0.001 vs. post-treatment), while the initially treated group maintained high functional performance (82.60 ± 10.49). These results confirm sustained and reproducible improvements in perceived functional self-efficacy (Figure 5).
This study aimed to evaluate the effects of a synbiotic supplement composed of a calculated mixture of E. faecium and agave inulin on cognitive decline in older adults. Nineteen participants diagnosed with MCI were randomized to receive either the synbiotic or a vehicle control. The findings demonstrate that supplementation with the synbiotic significantly improved cognitive performance in older adults with MCI. Improvements were observed across all psychometric assessments. Both inter- and intra-group analyses showed statistically significant differences compared with the control condition.
These results are consistent with previous studies reporting the potential of synbiotics to enhance cognitive function [13]. The observed improvements may be attributed to modulation of the gut microbiota induced by the synbiotic. Enhanced microbiota balance promotes the production of beneficial metabolites such as SCFAs, which are known to support brain health by reducing inflammation and improving neuronal plasticity.
Dalile et al. (2019) [20] described how gut microbiota influence synaptic plasticity—essential for memory formation—through microbial metabolite production and regulation of hippocampal neurogenesis, the brain region most closely associated with memory storage. Similarly, Clarke et al. (2014) [32] reported how alterations in gut microbiota composition may affect attention and higher cognitive processes through changes in neurotransmitter levels, particularly dopamine. Language processing and comprehension rely on neural networks within Broca’s and Wernicke’s areas, which can be impaired by neuroinflammatory and oxidative-stress processes resulting from microbial imbalance. Dalile et al. (2019) [20] further highlighted the role of SCFAs in microbiota-gut-brain communication, demonstrating their ability to reduce inflammation and enhance cognitive function. These findings support the hypothesis that the synbiotic used in this study, which promotes SCFA production—especially butyrate—may exert neuroprotective and neurorestorative effects in older adults with MCI.
In addition, synbiotic supplementation may increase BDNF levels, contributing to the reduction of clinical symptoms associated with cognitive decline [40–46]. BDNF levels decrease markedly with aging and are linked to synaptic loss, brain atrophy, and cognitive deterioration [47]. Butyrate, a key metabolite generated through synbiotic supplementation, has been shown to enhance BDNF expression while suppressing proinflammatory cytokines. In experimental models, the synbiotic used in this study has been reported to increase butyrate production, and this elevation in butyrate has been directly associated with enhanced BDNF expression and reduced neuroinflammation.
In experimental models, the synbiotic used in this study has been reported to increase butyrate production, and this elevation in butyrate has been associated with enhanced BDNF expression and reduced neuroinflammation. Consistent with these observations, previous research suggests that older adults may exhibit reduced expression or activity of the anti-aging gene sirtuin 1 (SIRT1), a key regulator of cognitive function and memory processes. SIRT1 plays a critical role in hippocampal function, regulation of BDNF release, synaptic plasticity, and modulation of neuroinflammatory pathways [48]. Reduced SIRT1 activity has been associated with cellular senescence, impaired metabolic regulation, and increased susceptibility to neurodegeneration in aging populations [49]. Importantly, butyric acid has been shown to activate SIRT1 signaling pathways, contributing to reduced amyloid-β accumulation and improved cognitive performance in experimental models of neurodegeneration [49]. In this context, the potential role of the synbiotic supplement evaluated in the present study as a modulator or indirect activator of SIRT1 represents an area of considerable interest for probiotic research and for strategies aimed at preventing cognitive decline in older populations. Furthermore, modulation of the gut microbiota through synbiotic supplementation may contribute to reducing lipopolysaccharide (LPS)-mediated neurotoxicity, which has been implicated in cognitive impairment and neuroinflammatory progression.
Borre et al. (2014) [50] proposed that modulation of the gut microbiota during critical life periods can influence the risk of later neurological disorders, suggesting that early synbiotic intervention could help prevent or delay cognitive decline in older adults.
Overall, this study achieved its primary objective by demonstrating that synbiotic supplementation can improve cognitive processes in older adults. The significance of these results lies in the potential use of synbiotics as a safe, non-pharmacological strategy for managing cognitive decline. Such interventions may represent an accessible alternative to conventional treatments, which are often costly and associated with adverse effects.
Although E. faecium is not typically considered a highly virulent pathogen, it has been investigated for its potential nosocomial pathogenicity, particularly in hospital settings [51]. Its clinical relevance is mainly associated with its capacity to develop resistance to multiple antibiotics, including vancomycin, which complicates treatment of infections in immunocompromised patients. Nonetheless, a previous study reported no complications in subjects treated with the probiotic strain of E. faecium [52], suggesting that while pathogenic potential exists, it may not necessarily manifest as clinical infection in non-immunocompromised individuals [53, 54]. No adverse effects or clinical alterations were observed among participants in this study.
The strengths of this research include its randomized controlled design and the use of validated psychometric instruments. All cognitive tests employed have been previously validated in the Mexican population and consistently demonstrated improved performance following synbiotic supplementation. In all cases, post-treatment scores suggest that, synbiotic is able to improve and maintain (at least for 8 weeks) cognitive function.
This study has some limitations that should be considered when interpreting the findings. First, the sample size was relatively small, which limits generalizability and statistical power, although the crossover design partially mitigates this limitation. Second, although mechanistic pathways involving SCFAs, BDNF, and inflammatory cytokines are discussed, no biological biomarkers were directly measured in this study. Therefore, the proposed mechanisms underlying the cognitive improvements remain hypothetical and are based on prior experimental and clinical literature rather than direct biochemical evidence from the present trial. Third, the study duration was limited to two 8-week intervention periods, and long-term sustainability of cognitive benefits beyond the follow-up phase cannot be established. Finally, it is important to note that although the present study did not include a large number of participants, the reproducible and reliable results observed following the crossover phase indicate a favorable and promising outlook for future research. Further studies involving larger cohorts will be required to confirm and validate these findings.
Future studies incorporating microbiome sequencing, inflammatory markers, SCFA quantification, and neurotrophic factors are warranted to validate the biological pathways suggested in this work.
The results of this study suggest that supplementation with the synbiotic formulation containing E. faecium and agave inulin exerts beneficial effects on cognitive function in older adults with MCI. This finding highlights the potential of synbiotic as a promising intervention for the prevention and management of age-related cognitive decline. Future studies with larger sample sizes and longer follow-up periods are recommended to confirm and extend these findings.
AEH: Alimentos Esenciales para la Humanidad
AERAC: Abbreviated Instrument for Expectations of Self-Efficacy for Daily Activities in Older Adults
BDNF: brain-derived neurotrophic factor
MCI: mild cognitive impairment
MMSE: Mini-Mental State Examination
RCFT: Rey-Osterrieth Complex Figure Test
SCFAs: short-chain fatty acids
SD: standard deviation
SIRT1: sirtuin 1
OMDC, AEC, NRS, and EMG: Conceptualization, Investigation, Data curation. APIG, IIM, EMAM, and MAVH: Data curation, Validation. MPHV, PRE, SGSÁ, and MESH: Writing—original draft, Visualization, Writing—review & editing. AI: Supervision, Project administration, Funding acquisition, Writing—review & editing, Writing—original draft, Formal analysis. All authors read and approved the submitted version.
Antonio Ibarra, who is the Editorial Board Member and Guest Editor of Exploration of Neuroprotective Therapy, Andrea P. Ibarra García who is the Guest Editor of Exploration of Neuroprotective Therapy, had no involvement in the decision-making or the review process of this manuscript. The other authors declare no conflicts of interest.
The study was approved by the Universidad Anáhuac México, Campus Norte, Ethics on Research Committee, Faculty of Health Sciences (Approval ID: CONBIOETICA-15-CEI-004-20160729). The trial was registered at ClinicalTrials.gov (NCT05688618).
Informed consent to participate in the study was obtained from all participants.
Not applicable.
The datasets supporting the findings of this study are available from the corresponding author upon reasonable request.
This work was supported by the research support fund number [202007], Universidad Anáhuac (awarded to Antonio Ibarra). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 769
Download: 22
Times Cited: 0
Adnan Akhtar Shaikh ... Niveditha Nair
Salomón Páez-García ... Miguel Germán Borda
Zhengrui Li ... Jing Li
Diego Fernández-Lázaro ... Juan Mielgo-Ayuso
Ericka C. Loza López ... Felipe Esparza Salazar
Fernando Leal-Martínez, Irene Alejandra Berumen Coronado
Alejandro Borrego-Ruiz, Juan J. Borrego
Elisa García-Vences ... Antonio Ibarra