 Perspective
Perspective

Affiliation:
1Centro de Investigación Biomédica en Red Enfermedades Neurodegenerativas (CiberNed), National Institute of Health Carlos iii, 28031 Madrid, Spain
2Department of Biochemistry and Molecular Biomedicine, University of Barcelona, 08028 Barcelona, Spain
3Institute of Theoretical and Computational Chemistry (IQTC), University of Barcelona, 08028 Barcelona, Spain
Email: rfranco123@gmail.com; rfranco@ub.edu
ORCID: https://orcid.org/0000-0003-2549-4919
Affiliation:
4Department of Ophthalmology and Visual Sciences, Faculty of Medicine, University of British Columbia, Vancouver, BC V6T 1Z3, Canada
ORCID: https://orcid.org/0000-0003-4796-140X
Affiliation:
5Cowichan Valley Pain Management Society, Duncan, BC V9L 6J9, Canada
6Oxygen Treatment Authority, SW6 7EU London, UK
ORCID: https://orcid.org/0009-0005-6190-5625
Explor Neuroprot Ther. 2026;6:1004157 DOI: https://doi.org/10.37349/ent.2026.1004157
Received: April 07, 2026 Accepted: May 09, 2026 Published: May 28, 2026
Academic Editor: Shile Huang, Louisiana State University Health Science Center, USA
This Perspective explores why hyperbaric oxygen therapy (HBOT) deserves closer clinical and scientific attention as a possible treatment for ischemic stroke and a potential neuroprotective strategy in chronic central nervous system disorders, especially multiple sclerosis and other progressive or age-related neurological conditions. While HBOT is not yet widely accepted for these indications, three factors justify reconsideration: its strong safety profile, a biologically plausible mechanistic rationale, and recurrent signals of benefit from selected neurological studies. We review HBOT’s historical development, current accepted indications, and evidence that adverse effects are generally mild, uncommon, and reversible under modern protocols. In neurology, efficacy remains unproven, yet interest persists due to preliminary findings and repeated patient-reported improvements. A central argument is that the main barrier to progress is not safety, but evidence generation. Conventional randomized controlled trials face major challenges: difficult blinding, wide variation in dosing protocols, and uncertainty about meaningful outcomes in chronic neurological disease. Moreover, HBOT is non-patentable, which limits commercial investment and leaves a potentially valuable intervention underexplored. Mechanistically, we move beyond explanations centred solely on oxygen delivery or oxidative stress. As a working hypothesis, neurological benefits may partly arise from cumulative adaptive responses—including a rebound hormesis following repeated hyperoxic exposure. We conclude with a pragmatic research agenda: continuous, low-cost physiological monitoring in patients already receiving HBOT, coupled with a medium-term goal of adequately powered efficacy trials.
The early experiments with compressed air chambers in the 1800s initially focused on treating decompression sickness (also called “caisson disease” or “the bends”) in workers exposed to pressurized environments, particularly those working in underwater construction projects [1]. Beyond decompression sickness, early compressed air and hyperbaric therapy applications expanded to include pulmonary and neurological disorders throughout the 19th century [2–4].
The earliest, widely cited, milestone is Nathaniel Henshaw’s “Domicilium” (1662), a sealed room where pressure could be raised or lowered in an attempt to treat disease. Over the 1800s, hyperbaric and pressurized environments became tightly linked to industrial and diving physiology: compressed-air work in tunnels and caissons revealed what was later recognized as decompression sickness. In the late 19th century, Paul Bert clarified key physiology of pressure and breathing gases; his work helped establish that decompression illness is related to dissolved inert gas coming out of solution as pressure drops, and he also described oxygen toxicity phenomena (the “Paul Bert effect”).
Hyperbaric oxygen therapy (HBOT) is also established as an adjunctive therapy in selected severe or refractory wounds. Some patients receiving HBOT for such indications report broader improvements in well-being, although these observations remain nonspecific and require careful interpretation. They nevertheless raise the possibility that HBOT may have systemic effects beyond tissue repair alone.
We do not seek to survey the full spectrum of existing or proposed HBOT applications in healthy individuals, including athletes, or across the many diseases in which it has been considered; for a comprehensive overview, readers are referred to the Undersea and Hyperbaric Medical Society (UHMS) at https://uhms.org/. Rather, this Perspective examines what is needed to provide evidence of the potential of HBOT in the management of central nervous system (CNS) disorders, particularly those that are chronic, progressive, and substantially shaped by aging, where any genuine therapeutic effect would be of particular significance. We also assemble evidence indicating that HBOT has a strong safety record. This could reduce the need for a full Phase I trial and make it feasible to proceed more directly to studies evaluating efficacy in patients with neurological conditions already being treated with HBOT by some practitioners. Multiple sclerosis (MS) is perhaps the most representative example.
The practical centerpiece of this Perspective, however, is a proposal for a low-cost, low-barrier research program based on continuous physiological monitoring of patients already undergoing HBOT. This proposal is developed in full in the final section of the manuscript.
The safety profile of HBOT is strong enough that a Phase II clinical trial for a given neurological disease could be readily initiated without a full Phase I step. One of the most frequent criticisms of HBOT as a therapy for conditions ranging from neurological disorders to age-related diseases is the potential for oxygen toxicity, usually framed in terms of oxygen-induced oxidative stress. We address the mechanistic question of oxidative stress in the Mechanisms section (Mechanisms underlying HBOT efficacy) below; here we summarize the clinical safety data.
Clinical safety data are substantial. A retrospective analysis of 2,334 patients by Hadanny and colleagues [5] found that serious adverse events are infrequent and typically non-serious. A larger retrospective dataset of 1.5 million treatments concluded that “occurrence of adverse events associated with HBO therapy is infrequent and typically not serious. The findings of this study suggest that when administered according to the appropriate therapeutic protocols HBO therapy is a safe and low-risk intervention” [6]. A 2023 systematic review and meta-analysis of 24 randomized controlled trials involving 1,497 participants concluded that “HBOT is more likely to cause adverse reactions when the chamber pressure is above 2.0 ATA” [1 atmosphere absolute (ATA) being the atmospheric pressure of 760 mmHg at sea level] [7]. A longitudinal observational study further reported that pulmonary function is preserved across repeated HBOT sessions, even in patients with pre-existing respiratory disease [8]. The most common events are aural fullness, transient visual changes, fatigue, and occasional patient-related adverse events, such as hypoglycaemia or hypotension before chamber entry.
Aural fullness—the sensation that the ear is blocked, plugged, or under pressure—may occur whenever changes in ambient pressure exceed the rate at which middle-ear pressure can be equalized through the Eustachian tubes. The same mechanism operates during hyperbaric exposure as during aircraft descent. In most cases, symptoms are benign and self-limited; swallowing, yawning, chewing, or gentle Valsalva or Toynbee manoeuvres usually suffice. Risk is increased in patients with upper respiratory infection, sinus disease, allergic congestion, active otitis, structural or functional Eustachian tube abnormalities, or recent otologic surgery. Severe or progressive otalgia, persistent hearing loss, marked tinnitus, vertigo, or otorrhagia should prompt clinical evaluation, as these findings may indicate significant barotrauma or, rarely, tympanic membrane injury.
Repeated HBOT sessions have been associated with two consistent ocular effects. The first is a reversible myopic shift characterized by reduced distance vision and, in some cases, improved near vision. The second, less common but clinically more important adverse event, is accelerated progression of pre-existing nuclear cataracts after high cumulative exposure. HBOT does not appear to induce cataracts de novo, but this possibility should be disclosed during consent and considered in older adults or patients with known lens opacities. Treatment protocols that minimize cumulative high-partial pressure of oxygen (pO2) exposure while preserving therapeutic effect are an active area of dose-finding research.
In 1996, the recognized applications of HBOT included carbon monoxide poisoning, arterial gas embolism, decompression sickness, clostridial myonecrosis, necrotizing fasciitis, refractory osteomyelitis, acute traumatic ischemic injury, compromised skin grafts and flaps, anaemia due to exceptional blood loss, thermal burns, and difficult-to-heal wounds [9]. Three decades later, this therapeutic landscape has not broadened in any decisive way. Real-world use remains constrained by the limited strength of evidence for many indications and by the logistical dependence on dedicated hyperbaric facilities. HBOT has not been widely adopted into routine care across major public-health systems, where reimbursement or commissioning is generally confined to a limited set of approved indications. Apart from decompression illness, HBOT is approved and routinely funded for carbon monoxide poisoning and for the management of selected patients with complex wounds, particularly when conventional treatment alone is insufficient. A list of primary and adjunctive uses for HBOT, drawn directly from the 2023 UHMS recommendations [10] and FDA guidance, is provided in Supplementary Table S1.
Clinical trials and accumulated clinical experience suggest that HBOT may have therapeutic potential beyond its established indications, including in selected CNS conditions. However, the evidence remains insufficient for broad clinical acceptance. Trials conducted largely by a single Israeli research group have reported benefits in persistent post-concussion syndrome and post-stroke cognitive impairment, including medium-to-large effect sizes and improvements on validated cognitive scales [11–13]. These findings are encouraging but need to be amplified by further studies.
Harch (2022) applied the Centre for Evidence-Based Medicine (CEBM) levels of evidence and the American Society of Plastic Surgeons (ASPS) grading framework to this literature, concluding that the 1.5 ATA HBOT protocol meets CEBM Level 1 criteria and supports an ASPS Class A recommendation for persistent post-concussion syndrome [14]. This grading, however, derives from an independent systematic review and should not be interpreted as an official ASPS clinical practice guideline.
A 2022 meta-analysis provided solid evidence that HBOT is beneficial in the treatment of diabetic foot ulcers, particularly by improving healing and reducing the risk of amputation [15]. The UHMS/Wound clinical practice guideline [16] and the DAMO2CLES randomized multicenter trial [17] together support the narrower and more defensible conclusion that HBOT benefits selected patients with ischemic or refractory diabetic foot ulcers, rather than all patients with diabetic foot ulcers, and this is now reflected in the way most health systems commission the therapy. As discussed below, even if routine use were recommended, ensuring equitable and timely access to HBOT would be difficult because treatment depends on the availability of specialized hyperbaric facilities.
Current guidance from the Wilderness Medical Society does not issue a formal recommendation for HBOT in frostbite [18], and Cochrane reviews have emphasized the absence of randomized controlled trials for this indication. Nevertheless, recent comparative and case-based studies, including those by Magnan and colleagues [19, 20], have suggested improved tissue preservation and digit salvage when HBOT is incorporated into multimodal management, particularly in combination with iloprost, a drug used to treat pulmonary arterial hypertension.
A recent review of HBOT in neurodegenerative disease summarizes preclinical data suggesting plausible benefit across cerebral ischemia, stroke, Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, MS, and amyotrophic lateral sclerosis (ALS) [21]. In addition, Hadanny and colleagues [22] reported cognitive improvements in a randomized controlled trial of healthy older adults.
At present, there is no neurological or neuropsychiatric condition for which HBOT has been conclusively established as an efficacious treatment. There is, however, observational evidence beyond the subjective reports of individuals who describe improved well-being and cognition after treatment. This evidence comes mainly from the experience accumulated in MS, where several thousand patients across long-established oxygen therapy centres in the UK and elsewhere continue to use HBOT and report consistent improvements in activities of daily living, although the studies were not placebo-controlled.
In several neurological conditions, HBOT is supported by an increasing mechanistic rationale and a growing body of preliminary clinical observations, yet robust evidence from adequately powered, indication-specific trials remains limited. As in frostbite, this creates a tension between therapeutic promise and evidentiary standards, such that HBOT may be regarded as a potentially valuable adjunctive strategy while still falling short of broad inclusion in formal clinical guidelines.
In neurological disorders such as ALS, the available evidence is restricted to two case series: a Phase I clinical trial involving only five patients that reported promising results, followed by a Phase II trial that failed to replicate those findings [23, 24]. Overall, the limited available evidence does not support a consistent benefit of HBOT in ALS. This conclusion may have contributed to a decline in further investigation in this area, despite the urgent need for efficacious therapies for diseases for which no treatments have proven effective in the long term.
HBOT has been the subject of investigation in MS for over four decades. Early randomized studies reported benefit in selected patients: Fischer and colleagues [25], in a double-blind placebo-controlled trial of 40 patients conducted between 1980 and 1982, observed improvement in 12 of 17 treated patients compared with 1 of 20 controls, with the clearest effect in less severely affected cases; Neubauer and colleagues [26] reported clinical benefit; and James [27] reviewed the rationale and early clinical experience. These studies have been influential, particularly in shaping patient advocacy and routine practice in the UK network of oxygen therapy centres, but they do not meet current standards for randomization, allocation concealment, blinding integrity, pre-registration, and patient-reported outcome selection.
The 2010 meta-analysis by Bennett and Heard [28], building on the earlier Cochrane review by Kleijnen and Knipschild, pooled nine randomized trials and concluded that the available evidence did not support routine clinical use of HBOT in MS. Their caution was appropriate given the heterogeneity of protocols, endpoints, and disease phenotypes across the pooled studies, and the absence of any single large, modern, multicenter trial. The National Center for Complementary and Integrative Health has reached a similar conclusion.
Continued HBOT use by several thousand people with MS, especially in long-established oxygen therapy centres in the UK, together with consistent uncontrolled reports of benefit in fatigue and daily functioning, represents a signal worth testing in a modern trial. Such a trial should prioritize outcomes that matter to patients, including fatigue, cognition, quality of life, and the Symbol Digit Modalities Test, rather than relying only on traditional disability scales. A complete history of HBOT in MS should cite the Neubauer et al. [26], James [27], and Fischer et al. [25] contributions alongside the later meta-analyses; Murray’s 2022 overview [29] is valuable as a history of MS diagnosis and treatment but does not, by design, cover the hyperbaric literature in depth.
Oxygen toxicity should be distinguished from the normal physiological role of oxygen. Under room-air conditions at 1 ATA, haemoglobin in the red blood cells of healthy individuals is already more than 95% saturated, so the main physiological effect of HBOT is not a major further increase in haemoglobin-bound oxygen but an increase in oxygen dissolved in plasma.
Whether increased oxygen availability during a typical 1-hour HBOT session produces immediate CNS effects remains uncertain. Preclinical studies suggest enhanced adenosine triphosphate (ATP) production and beneficial cellular responses [30, 31], but comparable acute metabolic activation has not been convincingly demonstrated in humans. Outside settings of active injury or repair, increased oxygen availability alone may therefore be insufficient to explain claimed CNS effects.
Although representing only a small fraction of body mass, the brain accounts for a disproportionately large share of whole-body oxygen consumption [32]. This dependence on continuous oxygen delivery has motivated the hypothesis that neurodegeneration with aging may be driven in part by gradual reductions in cerebral oxygen availability, whether due to vascular ageing, microcirculatory impairment, defective neurovascular coupling, or exposure to medications that diminish cerebral oxygen delivery by reducing perfusion or ventilation [33]. Neurodegenerative disease is intrinsically multicellular, involving coordinated dysfunction among neurons, astrocytes, oligodendrocytes, microglia, endothelial cells, and blood-brain barrier elements [34]. Any beneficial effect of HBOT in this context is unlikely to be explained simply by an acute rise in neuronal ATP production but may instead reflect parallel effects on several oxygen-sensitive pathways operating across multiple CNS cell types. Thus, even in the absence of evidence for an immediate generalized metabolic activation, HBOT could still exert biologically meaningful effects in the CNS by modulating a vulnerable, oxygen-dependent multicellular system. This may include the recruitment or functional recovery of metabolically compromised ‘idling’ neurons.
Ischemic preconditioning is an endogenous protective mechanism in which brief, nonlethal episodes of ischemia and reperfusion protect tissues from injury during subsequent prolonged ischemic events. First described by Murry and colleagues [35] in 1986, this phenomenon can reduce heart infarct size by up to 75% in experimental models and remains the gold standard against which all cardioprotective interventions are judged. At first glance, ischemic preconditioning appears to represent the opposite of what HBOT offers. This interpretation may not hold, however, if HBOT is considered an intervention capable of eliciting preconditioning-like responses after treatment (see below).
Clinical evidence for remote ischemic conditioning (RIC) in cerebrovascular disease is promising but mixed. The RICAMIS trial randomized 1,893 patients with acute moderate ischemic stroke in China and reported that RIC, administered twice daily for two weeks as an adjunct to standard care, increased the proportion of patients achieving an excellent neurological outcome. These findings suggest that repeated, brief, non-injurious ischemic stimuli may induce systemic adaptive responses with clinically meaningful neuroprotective effects (modified Rankin Scale 0–1) at 90 days from 62.0% to 67.4% (risk difference 5.4%; odds ratio 1.27, 95% CI 1.05–1.54; P = 0.02) [36]. The RESIST trial, conducted in Denmark with 1,500 patients randomized prehospital and continued for seven days, used a 20 mmHg sham-cuff control and reported no significant effect on the 90-day modified Rankin Scale (shift-analysis odds ratio 0.95) [37]. A 2025 Cochrane review of 20 randomized trials (7,687 participants) concluded that RIC probably reduces stroke recurrence modestly and may slightly increase excellent functional outcomes [38]. These results demonstrate that sham-controlled randomized trials of RIC are feasible; they do not support the claim that credible placebo-controlled trials in RIC are essentially impossible. Preclinical data further suggest that RIC may be useful in Parkinson’s disease models [39], though translation to clinical practice remains difficult. The open question is whether RIC-type signalling, including the form elicited after repeated HBOT sessions, translates to chronic neurodegenerative disease, where the relevant endpoints, trial durations, and sham strategies remain to be defined.
The mechanisms of HBOT in decompression sickness are the best characterized, largely because the physics of gas behaviour under changing pressure is well understood. The way decompression chambers work is a useful starting point for thinking about the further benefits claimed for HBOT in other indications.
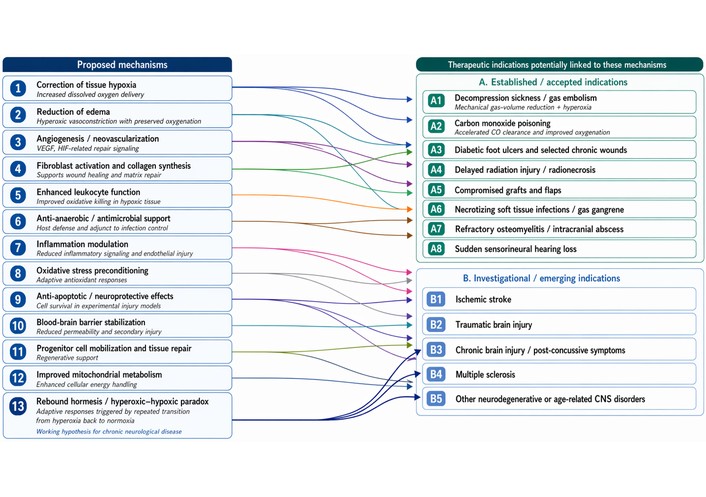
Figure 1 should be read not simply as a catalogue of possible HBOT effects, but as a physiological map of how pressure makes oxygen therapeutically available to tissues that are under-supplied. In Oxygen and the Brain, James [32] repeatedly returns to the central proposition that “there is no substitute for oxygen”, especially in the brain, and that the practical purpose of a pressure chamber is to correct oxygen deficiency by increasing the oxygen dissolved in plasma, not merely the oxygen carried by haemoglobin. This distinction is crucial for neurological diseases, because James’s model emphasizes impaired microcirculation, blood-brain-barrier disturbance, inflammation, oedema, and reduced tissue oxygenation as linked barriers to recovery. Figure 1, therefore, provides a visual bridge between the older gas-law logic of hyperbaric medicine and the broader biological mechanisms now proposed for HBOT: improved oxygen diffusion, reduced swelling, restoration of capillary function, modulation of inflammation, and adaptive signalling responses that may support repair in vulnerable CNS tissue.
Concerns about oxygen toxicity during HBOT have historically been framed in terms of oxygen-induced oxidative stress. A large proportion of the supporting evidence derives from in-vitro systems, immortalized cell lines, and rodent models, and the translation of these findings to clinically relevant human injury under standard HBOT protocols remains incomplete. Pulmonary function across longitudinal HBOT courses appears to be preserved, even in patients with pre-existing respiratory disease [8], and large retrospective clinical series have not identified a consistent pattern of oxygen-driven tissue injury [5, 6]. At the same time, Harch and Rhodes [41] have drawn attention to the possibility of cumulative CNS oxygen effects during prolonged pediatric courses and the uncertain thresholds that govern them, reinforcing the case for careful cumulative-dose monitoring. On balance, it seems reasonable to conclude that routine HBOT at 1.5–2.0 ATA is not associated with clinically meaningful oxidative injury in the human data currently available.
In the early twentieth century, decompression theory and treatment became systematic. John Scott Haldane (Edinburgh, 1860–1936) developed foundational decompression models (inert-gas uptake and saturation across tissues), and during and after World War II, navies refined standard recompression treatment tables for divers. Modern clinical practice for serious decompression sickness commonly involves recompression in a chamber with high inspired oxygen using protocols such as U.S. Navy treatment tables (e.g., TT5, TT6, and extensions), which have been iterated over decades [42].
HBOT’s clearest mechanism is in decompression illness, where gas physics directly explains the therapeutic benefit. According to Henry’s Law, inert gases dissolve in blood and tissues under pressure; during rapid decompression, these gases can form bubbles. Recompression reduces bubble volume according to Boyle’s Law, while high inspired oxygen promotes inert-gas washout and improves oxygen delivery to compromised tissues. This mechanism, however, cannot simply be extrapolated to neurological or chronic inflammatory diseases, where any benefit would need to arise from additional biological responses, which remain incompletely explored at present.
The essential role of HBOT in carbon monoxide poisoning arises from the combination of an oxygen-rich atmosphere and increased pressure. These effects merge as pO2, which at 2 ATA breathing 100% oxygen is approximately 1,520 mmHg (2 × 760 mmHg). This high value minimizes the time required to eliminate carbon monoxide from haemoglobin and substitute it with oxygen.
In HBOT treatments of healthy individuals breathing 100% oxygen at 2 ATA, arterial oxygen tensions generally range from 1,200 to 1,400 mmHg, depending on the arterial-to-alveolar oxygen ratio (a:A ratio), which remains relatively constant across different pressures [41, 42]. The a:A ratio in normal subjects is typically around 0.83, meaning arterial pO2 ≈ 0.83 × alveolar pO2 [42]. Hyperbaric oxygen at 2–3 ATA can result in arterial oxygen tensions exceeding 2,000 mmHg in some cases [3]. At 3 ATA with 100% oxygen, the dissolved oxygen content in blood reaches approximately 6 mL/dL—sufficient to meet resting cellular oxygen requirements without any contribution from haemoglobin-bound oxygen [9, 10].
In selected difficult-to-heal wounds, these effects are most plausibly explained by restoration of oxygen-dependent repair processes, including angiogenesis, collagen deposition, re-epithelialization, immune-cell function, and control of anaerobic infection. This provides a clearer mechanistic rationale for wound indications than for chronic neurological disorders, where the relevant pathways remain more speculative.
Beyond chronic diabetic foot ulcers and Clostridium-related gangrene, HBOT is not routinely recommended for the treatment of most open wound infections [15, 16]. However, some infectious agents, in addition to Clostridium, proliferate more readily under low-oxygen conditions. In such cases, HBOT may help by inhibiting the growth of anaerobic pathogens while simultaneously enhancing oxygen-dependent host processes, including bacterial killing by immune cells and tissue repair.
In-vitro work in an endothelial cell line has shown that a clinically relevant HBO protocol upregulates genes related to antioxidant defence, cytoprotection, and immediate-early response pathways, and is accompanied by enhanced cellular resistance to oxidative challenge; the authors propose that HBO acts as a mild hormetic stimulus that induces protective mechanisms in endothelial cells and may promote healthy ageing and wound-healing responses, particularly in populations with impaired wound healing [43]. While this work demonstrates that HBOT induces antioxidant gene expression, oxidative-stress-related mechanisms do not obviously account for the benefits attributed to HBOT in neurological and neuropsychiatric disorders. What, then, might the relevant mechanism be?
We propose here an adaptive response, which we term “rebound hormesis”, within the broader framework of the hyperoxic-hypoxic paradox. According to this hypothesis, repeated transitions from hyperoxia back to normoxia may elicit adaptive signalling responses that would not be captured by measuring oxygenation during a single HBOT session alone.
Hadanny and Efrati [40] have proposed that, after repeated hyperoxic exposures, antioxidant scavengers may remain elevated longer than reactive oxygen species (ROS) once the exposure ends; on return to normoxia, the intracellular ROS/scavenger ratio may transiently shift toward a state resembling hypoxic signalling, reducing degradation of hypoxia-inducible factor 1 subunit α (HIF-1α) and activating downstream adaptive pathways. This framework is often referred to as the hyperoxic-hypoxic paradox or as rebound hormesis. Other plausible mechanisms—direct modulation of mitochondrial function [30], transcriptional changes in cerebral endothelial cells [43], anti-inflammatory actions on microglia, and effects on cerebral perfusion and neurovascular coupling—may operate concurrently or be more important in specific indications. The transient fatigue some patients report after HBOT and the clinical impression that repeated sessions are more important than isolated exposures, are compatible with a cumulative-adaptation model; however, neither observation provides direct evidence for it. Hadanny and Efrati [40] themselves acknowledge that the dose, pressure, timing, and number of exposures needed to elicit these effects are not fully defined.
This hypothesis may provide a coherent framework for understanding putative effects of HBOT on the CNS, which are difficult to attribute to the direct physiological consequences of a single 1-hour exposure and may instead reflect cumulative adaptive responses elicited across repeated sessions. It also predicts that real-time physiological measurements during and after HBOT should reveal a consistent set of session-by-session changes, which is one of the motivations for the monitoring program proposed in the final section below.
Generating high-quality evidence for HBOT faces obstacles that are, in part, inherent to the nature of the intervention itself.
The gold standard for therapeutic evaluation—a double-blind, placebo-controlled randomized trial—is challenging, though not impossible, to implement in HBOT research. A key difficulty lies in the design of an appropriate sham condition. In some studies, “control” participants enter identical hyperbaric chambers pressurized to a lower, ostensibly sub-therapeutic level (typically 1.1–1.3 ATA) while breathing slightly enriched air. Yet even small increases in oxygen partial pressure may have physiological effects; changes of as little as 10% have been shown to be biologically active. Such sham conditions, therefore, may not function as true controls. For device-based interventions, blinding can be achieved through the use of an identical but inactivated apparatus, or an activated apparatus fitted with a barrier to block the therapeutic component. However, the sensory experience of pressurization—ear-popping and awareness of an altered environment—may compromise blinding integrity in a proportion of participants, particularly those with prior HBOT exposure. The success of blinding must therefore be formally tested in each trial, as recommended in the Phase-III MS trial methodology literature [44].
HBOT is currently administered across widely varying pressures (1.5–2.4 ATA), session durations, and frequencies, making cross-study comparisons unreliable and limiting the validity of meta-analyses. Before large efficacy trials can be meaningfully designed, dose-finding studies are required.
Outcome selection is critical. Trials must incorporate clinically meaningful primary endpoints. For MS, this means moving beyond traditional disability scales to include fatigue, cognition, and quality of life. The Symbol Digit Modalities Test has emerged as the cognitive measure of choice following comprehensive psychometric analyses across MS disease-modifying registration trials, given its sensitivity to impairment, correlation with brain pathology, and ability to detect clinically meaningful change. For mild cognitive impairment (MCI), parallel neuropsychological batteries with neuroimaging biomarkers as secondary endpoints are needed. Trial duration is equally critical: effects on neuroplasticity may require months to manifest, and trials of insufficient follow-up will systematically underestimate benefit. Comorbidity-adjusted outcome selection, as highlighted in the MS trial literature [45], is particularly important for a chronic multisystem condition of this kind.
A further obstacle is economic. HBOT is a non-patentable procedure, and no pharmaceutical or device company is positioned to recover the cost of large efficacy trials through market exclusivity. As with other non-patentable or repurposed interventions, rigorous evaluation is therefore likely to depend on public, philanthropic, or non-profit funding [46]. This is a textbook market failure: private-sector incentives for off-patent and repurposed therapies are structurally weak [47] and bridging the resulting evidence gap requires coordinated public funding [48].
The appropriate funders are national health research agencies—the National Institutes of Health (NIH), the National Institute for Health and Care Research (NIHR), the European Health and Digital Executive Agency (HaDEA) under Horizon Europe—together with disease-specific foundations such as the Michael J. Fox Foundation, the MS Society, the ALS Association, and the Alzheimer’s Association. From a health-economics perspective, this investment is defensible: HBOT, if proven efficacious, would be a generically deliverable intervention with no ongoing licensing costs, and the societal savings from even modest reductions in disability progression in MS, or delay of dementia conversion in MCI, would far exceed trial costs. Non-patentable therapies may prove cheaper in the long term than patented drugs of equivalent efficacy, making the investment in their rigorous evaluation doubly justified from a public-health standpoint [46, 48].
This section contains the paper’s principal practical recommendation. While the design and funding of definitive randomized controlled trials remain a medium-to-long-term objective, a meaningful and mechanistically informative research agenda can be initiated immediately, at low cost, and without modification of existing clinical protocols. Patients already undergoing routine HBOT sessions represent an underutilized observational opportunity: the controlled, time-limited, and reproducible nature of each session makes it an ideal setting for continuous physiological profiling. Figure 2 summarizes the proposed core parameters, each of which is either already recorded in most hyperbaric facilities or obtainable with inexpensive, widely available equipment.
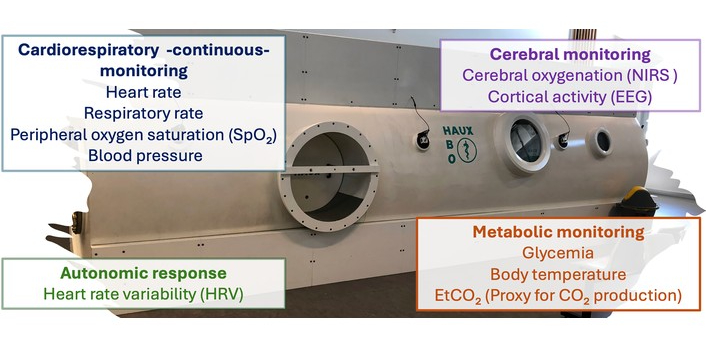
Physiological monitoring during controlled exposure to hyperoxia under pressure. Parameters needed to define physiological response patterns and to support a mechanistic understanding of HBOT. Cardiorespiratory continuous monitoring: heart rate, respiratory rate, peripheral oxygen saturation (SpO2), and blood pressure. Cerebral monitoring: cerebral oxygenation (near-infrared spectroscopy, NIRS) and cortical activity (electroencephalography, EEG). Autonomic response: heart rate variability (HRV). Metabolic monitoring: glycaemia, body temperature, end-tidal carbon dioxide (EtCO2) as a proxy for CO2 production. Each of these measurements is low-barrier: most are already routine in hyperbaric facilities or can be added at modest cost without altering existing treatment protocols.
The core proposal is the systematic collection of the following parameters during each session (Figure 2). Cardiorespiratory continuous monitoring: includes heart rate, respiratory rate, peripheral oxygen saturation (SpO2), and non-invasive continuous blood pressure (achievable via finger photoplethysmography at negligible additional burden). Metabolic monitoring: glycaemia, body temperature, and end-tidal carbon dioxide (EtCO2) as a practical proxy for CO2 production, directly reflecting the ventilatory response to acute hyperoxia. Autonomic response: heart rate variability (HRV), derivable from the electrocardiographic signal without additional hardware, provides a continuous index of autonomic nervous system modulation—a dimension of particular relevance given well-documented dysautonomia in both MS and MCI populations. Cerebral monitoring: includes near-infrared spectroscopy (NIRS) for non-invasive, continuous measurement of cerebral oxygenation and regional haemodynamics, which is fully compatible with the hyperbaric environment; and, where hyperbaric-compatible equipment is available, electroencephalography (EEG) for session-by-session characterization of cortical activity.
Cerebral monitoring deserves particular emphasis. Given that the putative therapeutic rationale for HBOT in neurological conditions centres on correction of cerebral hypoxia and on the promotion of adaptive neuroplasticity—including activity-dependent synaptic remodeling, angiogenesis, modulation of neuroinflammation, and metabolic support for repair—monitoring should extend beyond systemic oxygen exposure to include brain-relevant physiological responses. EEG data would be particularly informative for cognitive outcomes in MCI.
Taken together, even a modest observational dataset, systematically collected across patients, sessions, and clinical profiles, would yield several scientifically valuable outputs. It would characterize the normal physiological trajectory of an HBOT session in neurological patients, identify inter-individual variability in physiological response, generate hypotheses regarding which response patterns correlate with clinical benefit, and provide the biological-plausibility data that funding bodies increasingly require before committing to large-trial investment. Crucially, this program requires no randomization, no control arm, no additional clinical intervention, and no substantial funding—only the systematic application of available technology and a commitment to record, share, and analyze the data thus generated.
This Perspective does not present HBOT as an established neuroprotective therapy. Rather, it makes a narrower and, in our view, more defensible argument: that HBOT’s strong safety record, combined with a plausible—though still not demonstrated—mechanistic rationale, justifies a focused, modern program of clinical and physiological investigation in chronic neurological disease.
MS may represent the most appropriate starting point for such a program, given the existence of previous clinical experience, patient-reported signs of benefit, and a relatively well-defined need for improved symptomatic and disease-monitoring strategies. However, this should not preclude parallel consideration of other chronic neurological disorders, including Alzheimer’s disease and related dementias, where effective disease-modifying therapies remain limited and even modest, reproducible improvements in cognition or function would be clinically meaningful. Because HBOT has a favorable safety profile when delivered under modern protocols, any potential cognitive benefits in these conditions should be evaluated as early and rigorously as possible, rather than dismissed because definitive efficacy data are not yet available.
The practical recommendation is the continuous-monitoring program outlined in the previous section and summarized in Figure 2. It is low-cost, requires no randomization, does not disrupt existing protocols, and would begin generating the mechanistic and biological-plausibility data that funders now reasonably expect before committing to Phase III trials. Alongside this, rigorous, independently led, multicentre efficacy trials—using patient-centred outcomes—remain the essential medium-term objective. Given HBOT’s non-patentable nature, coordinated public funding is likely the only realistic pathway to achieving them.
a:A ratio: arterial-to-alveolar oxygen ratio
ALS: amyotrophic lateral sclerosis
ASPS: American Society of Plastic Surgeons
ATA: atmosphere absolute
ATP: adenosine triphosphate
CEBM: Centre for Evidence-Based Medicine
CNS: central nervous system
EEG: electroencephalography
EtCO2: end-tidal carbon dioxide
HaDEA: European Health and Digital Executive Agency
HBOT: hyperbaric oxygen therapy
HIF-1α: hypoxia-inducible factor 1 subunit α
HRV: heart rate variability
MCI: mild cognitive impairment
MS: multiple sclerosis
NIH: National Institutes of Health
NIHR: National Institute for Health and Care Research
NIRS: near-infrared spectroscopy
pO2: partial pressure of oxygen
RIC: remote ischemic conditioning
ROS: reactive oxygen species
SpO2: peripheral oxygen saturation
UHMS: Undersea and Hyperbaric Medical Society
The supplementary table for this article is available at: https://www.explorationpub.com/uploads/Article/file/1004157_sup_1.pdf.
RF: Conceptualization, Methodology, Investigation, Writing—original draft, Writing—review & editing, Supervision. CAS: Conceptualization, Investigation, Writing—review & editing, Validation. AP: Investigation, Writing—review & editing, Resources. All authors read and approved the final manuscript.
Rafael Franco, who is the Editor-in-Chief, and Christopher A. Shaw, who is the Associate Editor of Exploration of Neuroprotective Therapy, had no involvement in the decision-making or the review process of this manuscript. Andrew Paterson is the owner of a registered hyperbaric facility (Cowichan Valley Pain Management Society) and is a director of the Oxygen Treatment Authority. These interests are disclosed in the interests of transparency; they had no influence over the content, conclusions, or recommendations of this Perspective.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1351
Download: 21
Times Cited: 0
