Review
Review

Affiliation:
Department of Microbiology, Faculty of Medicine, Kuwait University, Safat 13110, Kuwait
Email: raj.raghupathy@ku.edu.kw
ORCID: https://orcid.org/0000-0002-7925-864X
Explor Immunol. 2022;2:414–427 DOI: https://doi.org/10.37349/ei.2022.00059
Received: December 08, 2021 Accepted: May 11, 2022 Published: June 27, 2022
Academic Editor: Dominique J. Charron, Hospital Saint Louis, France
The article belongs to the special issue Human Reproduction: Involvement of the Immune System
“There is many a slip twist the cup and the lip” is a proverb that dates back to the 3rd century. This proverb comes to mind while writing a review on pregnancy loss; so many complications can occur between fertilization and development of the embryo through the long period of gestation until successful delivery of the baby. These include failure of implantation of the embryo, spontaneous miscarriage in the first trimester, pre-eclampsia in the second trimester, premature rupture of fetal membranes, pre-term labour, and pre-term delivery. The maternal immune system which does a phenomenal job of protecting the host from a daunting variety of infections, sometimes also mounts adverse reactions that complicate pregnancy and endanger the fetus. Maternal immune reactions that can adversely affect pregnancy have been shown to be mediated by lymphocytes, macrophages and natural killer cells, and by cytokines secreted by these cellular effectors. This review summarizes the deleterious effects of cytokines leading to recurrent spontaneous miscarriage, pre-eclampsia and pre-term delivery, which are the major complications of pregnancy. It then goes on to discuss the potential use of progesterone and dydrogesterone, an orally-administered progestogen, as immunomodulatory molecules that can be considered for the prevention and/or treatment of these complications.
The immune system does a magnificent job of defending us from incessant onslaughts by an incredible variety of pathogens and toxins. Bestowed with a remarkable array of cells and molecules, the immune system protects us from viruses, bacteria, fungi, parasites and toxins using a variety of mechanisms and processes. This feat is accomplished by numerous cell types such as lymphocytes, macrophages, granulocytes, and by cytokines secreted by them. Unfortunately, this very same immune system uses the very same mechanisms and processes to mount undesirable actions that result in autoimmune tissue damage, hypersensitive and inflammatory reactions. And because the immune system interacts with all other systems in the body, such as the musculoskeletal system, the nervous system, the respiratory system, the gastrointestinal system and so on, adverse reactions by the immune system can be manifested on these systems. The reproductive system is no exception; immune effectors are known to interfere with fertilization and can also have a negative impact on pregnancy, causing several complications of pregnancy. This review summarizes the adverse impacts of maternal cytokines on pregnancy and then presents a few immunomodulatory approaches to prevent or treat these conditions.
The maternal immune system has been implicated in pregnancy complications such as recurrent spontaneous miscarriage (RSM), pre-eclampsia (PE), and pre-term labour (PTL) and delivery. Maternal immune cells, both in the periphery and at the maternal-fetal interface, that have been studied extensively in this context are lymphocytes [1], macrophages [2] and natural killer (NK) cells [3]. Much of the attention has been focused, justifiably, on the cytokines produced by these cells.
What is the relevance of cytokines to pregnancy complications? Cytokines are vital and essential mediators which play critical roles in numerous immune responses that include the activation of T helper (Th) cell responses, induction of antibody production, the activation of T cell cytotoxicity, the stimulation of macrophages, NK cells and granulocytes to name but a few. While cytokines are basically indispensable to the normal physiologic functioning of the immune system in terms of protecting us from pathogens, dysregulation of cytokine effector pathways can skew protective immunity to disease-associated immune pathology. These adverse reactions include the different types of hypersensitivity, autoimmune tissue damage and pathologic effects of acute inflammatory reactions. Clearly what matters is which cytokines are produced, where in the body they are produced, and at what levels they are produced.
Given their multifaceted and potent capabilities, cytokines have received a great deal of attention in maternal-fetal immunology. Th cells, besides macrophages, dendritic cells, NK cells, etc., are major producers of cytokines that “help” a variety of immune responses and also mediate inflammatory reactions. Several subsets of Th cells have been identified and characterized; the major subsets Th1 and Th2 cells have very different functions due to the different and distinct cytokine production patterns [4–6]. Th1 cells produce interferon (IFN)-γ, tumor necrosis factor (TNF)-β, TNF-α, and interleukin (IL)-2, and these are cytokines that activate and support strong cell-mediated and inflammatory reactions like cytotoxicity, acute local inflammatory reactions and delayed-type hypersensitivity. Th1 cytokines have been implicated in strong inflammatory reactions such as rejection of tissue grafts, autoimmune diseases and acute inflammatory tissue damage. The cytokines produced by Th2 cells, IL-4, IL-5, IL-6, IL-10, and IL-13, induce the production of antibodies by B cells and thus are responsible for the activation of humoral immunity; many of these Th2 cytokines are anti-inflammatory in nature. Th1 and Th2 cells mutually inhibit each other; some Th1 cytokines downregulate the functions of Th2 cells and vice versa [4–6]. Some pro-inflammatory Th1 cytokines have been shown to be deleterious to the conceptus in animal experiments [7–9]. The administration of the Th1 cytokines TNF-α, IFN-γ and IL-2 into pregnant mice leads to fetal resorptions, and the administration of anti-TNF-α antibodies reverses abortion in a murine model of natural, immunologically-mediated abortion [7]. TNF-α and IFN-γ have been shown to inhibit the outgrowth of human trophoblast cells in vitro [8] and induce the apoptotic killing of human trophoblast cells [9].
We will now proceed to examine the relevance of cytokines to three major complications of pregnancy: RSM, PE and PTL.
Spontaneous miscarriage is the spontaneous loss of a fetus before 20 weeks of pregnancy, and RSM is the loss of two or more consecutive fetuses.
Immunological studies on RSM have generally focused on comparing women around 12 weeks of gestation with healthy pregnant women at similar stages of gestation and at normal delivery; subjects were in the age group of 28–35.
The stimulation, with human trophoblast antigens, of peripheral blood lymphocytes from women having a history of RSM results in the production of elevated levels of Th1 cytokines with embryotoxic activity [10]. We then demonstrated that the stimulation, with a mitogen, of lymphocytes from women having unexplained RSM produces significantly higher levels of the inflammatory Th1 cytokines IL-2, IFN-γ and TNF-α; on the other hand, women with a history of healthy pregnancy produce significantly lower levels of Th1 cytokines, and higher levels of anti-inflammatory Th2 cytokines IL-4, IL-5, and IL-10 [11, 12]. The activation of maternal peripheral blood lymphocytes with either autologous placental cells or trophoblast antigens yielded a similar pattern of cytokine production [13]. Our contention of an association between Th1 cytokine dominance and RSM was substantiated by the demonstration of higher ratios of pro-inflammatory cytokines to anti-inflammatory cytokines in women who had a history of RSM as compared to women with a history of healthy pregnancy [14].
Cytokine patterns in the placenta and endometrium in women with RSM show similarities to the situation in the periphery. Lower numbers of T cells producing anti-inflammatory cytokines were found in the decidua of women with unexplained RSM than in the decidua of women undergoing healthy pregnancy [15]. The expression of pro-inflammatory cytokines is higher, and that of anti-inflammatory cytokines is lower in the endometrium of women with idiopathic recurrent miscarriage as compared to healthy subjects [16].
Thus, women with unexplained recurrent miscarriage have elevated levels of Th1 cytokines, while women with healthy pregnancy have decreased levels of Th1 cytokines and increased levels Th2 cytokines (Table 1A). RSM is associated with an upregulation of Th1 responses and downregulation of Th2 responses.
Levels of cytokines in unexplained RSM, PE and pre-term delivery (PTD)
| Location | Increased levels (Ref number) | Decreased levels (Ref number) | ||
|---|---|---|---|---|
| A. RSM | ||||
| PBMC | IL-2 [11, 12] | IL-4 [11–13] | ||
| IFN-γ [11, 12] | IL-5 [11–13] | |||
| TNF-α [10–13] | IL-10 [10–12] | |||
| TNF-β [10] | ||||
| Placenta | Th2 cells [15] | |||
| Endometrium | IL-1β [16] | IL-4 [16] | ||
| TNF-α [16] | IL-10 [16] | |||
| TNF-β [16] | ||||
| B. PE | ||||
| PBMC | IL-1β [27] | IL-4 [31, 35] | ||
| IL-2 [28] | IL-5 [32, 35] | |||
| IFN-γ [29, 35] | IL-10 [33–35] | |||
| TNF-α [30, 33] | ||||
| Placenta | IL-1β [22] | IL-10 [26] | ||
| IL-2 [23] | ||||
| IL-18 [24] | ||||
| IFN-γ [25] | ||||
| TNF-α [26] | ||||
| C. PTD | ||||
| PBMC | IL-2 [40] | IL-10 [43] | ||
| IFN-γ [40] | ||||
| Sera | IL-1β [41, 43] | IL-10 [43] | ||
| TNF-α [41] | ||||
| Placenta | IL-12 [46] | IL-4 [46] | ||
| IFN-γ [26] | IL-10 [46] | |||
PBMC: peripheral blood mononuclear cells
PE is a severe and dangerous complication associated with increased blood pressure and proteinuria. It affects several systems and organs, and results in a high proportion of maternal and infant deaths. PE is defined as the occurrence of new-onset hypertension and proteinuria or new-onset hypertension with significant end organ damage; it usually manifests after 20 weeks of gestation. About 2–10% of pregnant women are affected by PE [17] which accounts for 14% of maternal deaths worldwide [18].
Pregnant women with PE manifest endothelial lesions in various organs, perivascular edema, hemorrhage, small vessel thrombosis and glomerular endotheliosis; in other words, PE causes a generalized dysfunction of the maternal endothelium [19]. This maternal endothelial damage is caused by an exaggerated systemic inflammatory response that involves maternal leukocytes and pro-inflammatory cytokines [20, 21].
In the studies highlighted below, subjects with PE were in weeks 28–36 of gestation, and healthy controls were 37 weeks pregnant. The mean ages of the pre-eclamptic and healthy subjects were 29 and 26 respectively.
One of the early pathogenetic steps in PE is an aberrant maternal immune response against the placenta. This is supported by the demonstration of a significant increase in the expression of the pro-inflammatory cytokines IL-1 [22], IL-2 [23], IL-18 [24], IFN-γ [25] and TNF-α [26] in pre-eclamptic placentas. On the other hand, PE is associated with decreased placental production of the anti-inflammatory cytokine IL-10 [26].
In addition to the production of higher levels of inflammatory cytokines at the maternal-fetal interface mentioned above, peripheral blood lymphocytes from women with RSM have been shown to produce elevated levels of IL-1 [27], IL-2 [28], IFN-γ [29] and TNF-α [30]. Interestingly, a reduction has been shown in the production of the anti-inflammatory cytokines IL-4 [31], IL-5 [32] and IL-10 [33, 34] by peripheral blood lymphocytes. Our laboratory has reported significantly higher secretion of IFN-γ and TNF-α by lymphocytes from women with PE as compared to women with healthy pregnancy, who on the contrary showed significantly greater production of IL-4, IL-5, and IL-10. We demonstrated a significantly higher ratio of Th1/pro-inflammatory to Th2/anti-inflammatory cytokines in PE as compared to healthy pregnancy [35]. Similarly, sera from subjects with PE have been shown to have increased Th1/Th2 cytokine ratios [35]. In summary, PE is associated with increased levels of pro-inflammatory Th1 cytokines in PE, both at the maternal-fetal interface and in peripheral blood (Table 1B) [36].
PTL and PTD are major causes of maternal morbidity and mortality [37]. PTL is labour that begins before 37 weeks of gestation, and PTD is any birth that occurs before 37 weeks of gestation; pre-term birth occurs in about 12% of pregnancies [38]. Inflammation in the uterus is a central aspect of the pathogenesis of PTL [39]; this implies etiologic roles for immunological mediators such as cytokines.
In the studies cited below, the gestational age of subjects with PTD ranged from 21 to 34 weeks, and healthy controls had normal term delivery, and the mean ages of the subjects ranged from 23 to 31.
We have demonstrated the dominance of Th1 cytokines in a significant proportion of women with unexplained PTD [40]; while peripheral blood lymphocytes from women undergoing healthy pregnancy produce higher levels of the Th2 cytokines IL-4, IL-5 and IL-10, women with PTD produce higher levels of the Th1 cytokines IL-2 and IFN-γ. The ratios of Th1:Th2 cytokines are higher in PTD, indicating a stronger Th1 cytokine bias in PTD.
Elevated levels of the pro-inflammatory cytokines TNF-α, IL-1, IL-6, IL-8 and IL-12 have been reported in sera of women with pre-term birth as compared to those with normal term birth [41–43]. Higher levels of inflammatory cytokines are also seen in uterine tissues [44], cervicovaginal fluid [45] as well as in the placenta [46, 47] of women with PTD.
These observations suggest an overall association of some pro-inflammatory Th1 cytokines with pre-term labor and delivery (Table 1C). There is therefore evidence for an “intrauterine inflammatory response syndrome” as being responsible for PTL [48].
Having summarized the association between certain cytokines and pregnancy complications, we will examine immunomodulatory approaches to prevent or treat these complications.
Approaches that have been explored for immunomodulation of recurrent pregnancy loss include paternal leukocyte immunization, intravenous immunoglobulin (IVIg) and intralipid [49, 50].
Immunization of women with lymphocytes from their partner was proposed about forty years ago, but the benefit of this approach was questioned in the early 2000s. Recent meta-analyses have however supported the effectiveness of lymphocyte immunization therapy (LIT) in recurrent miscarriage [51] as several studies have shown improved pregnancy outcomes after treatment. Proposed mechanisms underlying this treatment include increased production of potentially beneficial factors such as anti-paternal antibodies, progesterone-induced blocking factor (PIBF) and anti-idiotypic antibodies as well as reducing the ratio of Th1/Th2 cytokines [52].
IVIg treatment has been explored for its potential benefit in RSM based on its use in treating autoimmune diseases. One study reported that 86.3% of women who received IVIg had successful pregnancy as compared to 42% who did not; this was associated with increased levels of T regulatory (Treg) cells and decreased levels of Th17 cells that produce the inflammatory cytokine IL-17 [53]. An early systematic review done in 2007 on 8 randomized controlled trials comparing IVIg to placebo concluded that IVIg treatment led to a significantly increased rate of live birth in secondary recurrent miscarriage but not in primary recurrent miscarriage [54]. Results of trials however have not been consistent, with different conclusions emerging from them; for example, in 2011, a comparison of six randomized controlled trials concluded that IVIg is not beneficial [55]. In 2015, a randomized, double-blind, placebo-controlled trial on women who had previously had at least 4 miscarriages reported that IVIg treatment did not increase the live birth rate [56]. A recent meta-analysis of randomized controlled trials concluded that IVIg treatment did not have a significant effect on live birth rates [57].
Therapy with intralipid, a fat emulsion containing soybean oil, glycerin and egg phospholipids, has been suggested to be beneficial in recurrent miscarriage [50, 58–60]. While such studies are promising and suggest that intralipid acts by targeting high levels of NK cells, more studies on larger sample sizes are needed to confirm the effectiveness of this modality as well as the underlying mechanisms of action [61].
Considering that TNF-α has been implicated in recurrent miscarriage [10–16] and PE [26, 30, 35, 36, 62], this inflammatory cytokine has been considered for rational “targeted therapy” [50, 63, 64]. A randomized controlled trial on etanercept, a TNF inhibitor, was reported to result in significantly higher number of successful deliveries, accompanied by a reduction in levels of TNF-α, as compared to placebo treatment [65]. Studies showing improved incidence of live births after treatment with TNF-α agonists such as adalimumab or etanercept are encouraging [50].
In addition to its myriad endocrinological properties which make progesterone indispensable to pregnancy, progesterone is also endowed with very interesting immunomodulatory properties. More than fifty years ago progesterone was christened “nature’s immunosuppressant” [66] based on studies that showed that it was able to suppress some in vitro immune reactions such as lymphocyte activation and proliferation. It was proposed then that progesterone protects the conceptus by suppressing maternal anti-fetal immune reactivity [67].
Recent studies have confirmed some of the down-regulatory capabilities of progesterone on immune responses, especially inflammatory responses. Progesterone down-regulates the activation of murine dendritic cells [68], macrophages [69] and NK cells [70]. Exposure of rat dendritic cells to progesterone results in a significant reduction in the release of the pro-inflammatory cytokines TNF-α and IL-1 [71]. Thus, progesterone has immunomodulatory capabilities that are relevant to the protection of the fetus and thus to the success of pregnancy [72].
A landmark study by Choi et al. [73] showed that progesterone inhibits Th1 cytokine production by trophoblast antigen-activated blood cells from women with unexplained RSM. Progesterone also favors the in vitro development of Th2 cells supporting the contention that progesterone nurtures survival of the fetus by inducing Th2 cytokine production [74]. This naturally led to the assessment of progesterone supplementation for the treatment of pregnancy complications [75].
A recent meta-analysis of 11 randomized controlled trials on 2,359 women which compared progesterone supplementation with placebo or no treatment for the prevention of miscarriage concluded that progesterone therapy “probably reduces the rate of miscarriage in subsequent pregnancies” [76]. A systematic review of randomized, placebo-controlled trials showed that supplementation with vaginal micronized progesterone leads to increased live birth rates, and concluded that women with recurrent miscarriage can benefit from vaginal progesterone [77]. Thus, supplementation with progesterone leads to higher live birth rates [78]. It should be noted that not all studies have reported a significant beneficial effect of progesterone in recurrent miscarriage. It is suggested that this lack of unequivocal support for strong beneficial effects of progesterone in RSM is due to studies done on subjects who were not pre-selected for a poor prognosis or for having immune etiologies [79].
Progesterone supplementation to prevent PTL was thought to be ineffective, but there is now a resurgence of interest in using it, based on analyses of randomized, placebo-controlled trials which have shown that progesterone is effective in preventing PTD in those who have had previous pre-term births [80, 81]. A recent extensive analysis of 112 reviews focused on a variety of approaches to prevent PTL including diet, exercise, supplementation with calcium and zinc, low dose aspirin and progesterone supplementation; the authors concluded that only a few interventions are effective in preventing pre-term birth; progesterone is one of them [82].
Dydrogesterone (6-dehydro-9β, 10α-progesterone, Duphaston®) is an orally-administered progestogen used to treat menstrual disorders, luteal insufficiency, threatened abortion and in hormone replacement therapy. The molecular structure and pharmacological effects of dydrogesterone are similar to those of progesterone, but dydrogesterone is more potent, has higher affinity for the progesterone receptor [83] and has more bioavailability than progesterone [84].
We showed that when PBMC from women with unexplained recurrent miscarriage are cultured with dydrogesterone, these cells secrete significantly decreased levels of IFN-γ and TNF-α, and significantly increased levels of IL-4 and IL-6 [85]. Exposure of PBMC to dydrogesterone results in a significant decrease in Th1/Th2 cytokine ratios, indicating a decrease in Th1 or pro-inflammatory cytokine bias. We reported that dydrogesterone also suppresses the production of the potent pro-inflammatory and chemotactic cytokine IL-17 [86]. It is of interest that IL-17 has been associated with embryonic loss in animal studies [87] and with miscarriage in humans [49, 88]. Thus, dydrogesterone has effective and appropriate immunomodulatory properties as demonstrated by the inhibition of cytokines that are antagonistic to healthy pregnancy [89].
Dydrogesterone supplementation has been shown to benefit women with a history of RSM. A randomized study showed that miscarriage occurred in 12.5% of women treated with dydrogesterone as compared to 18.4% of women who received conservative management [90]. A recent randomized, double-blind, placebo-controlled study by Kumar et al. [91] demonstrated that dydrogesterone supplementation resulted in a significant decline in the incidence of miscarriages and increased mean gestational age at delivery. Carp’s meta-analysis concluded that the rate of miscarriage in women who received dydrogesterone was 10.5% compared to 23.5% in control subjects, and that there was a real treatment effect as evinced by a 29% reduction in the odds for miscarriage [92]. Another recent meta-analysis of 13 studies comprising of a total of 2,454 patients confirmed a higher success rate of pregnancy in women treated with dydrogesterone [93]. A systematic review and meta-analysis of ten randomized controlled trials by Saccone et al. [94] concluded convincingly that dydrogesterone supplementation reduces the rate of miscarriage.
In the interventional studies cited above the mean ages of subjects ranged from 20 to 39. In some studies supplementation with progestogen treatment was done until 12 weeks or 16 weeks of gestation [77], in some cases until 24 weeks and even 36 weeks [76, 80]. However, a majority of studies reported progestogen supplementation from confirmation of pregnancy until 12–16 weeks [93, 94].
In addition to these promising reports on the potential benefit of using dydrogesterone for recurrent miscarriage, it has been proposed for use in preventing or treating other pregnancy complications such as PTL and PE [95, 96]. Dydrogesterone supplementation of women at high risk for PE was shown to have a reduced incidence of hypertension, proteinuria, fetal growth retardation, PTL as well as a significant reduction in the incidence of PE [97]. Pregnancies that followed assisted reproductive techniques have been shown to have reduced incidence of PE in women who were treated with dydrogesterone [98].
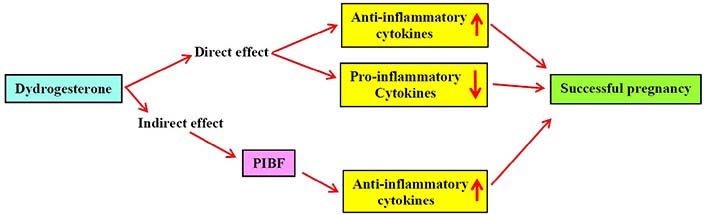
Thus, dydrogesterone offers a promising strategy for the manipulation of the maternal immune system towards a pregnancy-conducive milieu (Figure 1).
A protein secreted by lymphocytes treated with progesterone, first described in 1985 [99], has serendipitously been shown to have extremely interesting properties. This protein, PIBF appears to be critical to the success of pregnancy. Blocking this factor during early pregnancy in mice leads to impaired implantation and increased abortion; this is associated with increased levels of peripheral and decidual NK cells [100]. Moreover, blocking the production of PIBF results in Th1-dominant cytokine production, significantly increased NK activity, and fetal loss [101].
Perhaps the most relevant of the properties of PIBF is its ability to induce the production of Th2 cytokines. Lymphocytes from women with recurrent miscarriage and women with PTD when exposed to PIBF produce lower levels Th1-type cytokines and increased levels of Th2-type cytokines [102]. Indeed, low levels of PIBF in women are associated with spontaneous termination of pregnancy [103]. Dydrogesterone has been shown to be beneficial in women undergoing threatened miscarriage, and this benefit is associated with elevated levels of PIBF [104]. In addition to its ability to directly shift the cytokine balance to a Th2-dominated profile, dydrogesterone appears to mediate its immunomodulatory effects by stimulating the production of PIBF which induces a Th2-dominant cytokine response, thereby skewing the Th1/Th2 balance in favor of pregnancy (Figure 1). The administration of dydrogesterone to women at high risk of PTL resulted in significantly greater production of PIBF and Th2 cytokines, and reduced production of Th1 cytokines; this suggests that PIBF is a promising candidate for prevention or management of PTL and delivery [105]. The fact that dydrogesterone is an orally-administered progestogen with a good safety profile makes it particularly attractive.
Numerous complications can occur between conception and parturition, and these can lead to pregnancy loss. The major complications are spontaneous miscarriage, PE and PTD, and the maternal immune system can contribute to the etiopathogenesis of these complications. Cytokines produced by the maternal immune system can have deleterious effects on the conceptus and thus on the outcome of pregnancy. Several immunological approaches have been explored for the modulation of maternal immune reactions to create a milieu that is conducive to healthy pregnancy. Dydrogesterone, a progestogen that is administered orally, is an immunomodulator that can shift the maternal cytokine balance from a dominant Th1 status to a Th2-biased milieu. Studies on dydrogesterone supplementation in women with these complications provide scope for optimism that dydrogesterone “can be considered for effective and safe treatment.
IFN: interferon
IL: interleukin
IVIg: intravenous immunoglobulin
NK: natural killer
PBMC: peripheral blood mononuclear cells
PE: pre-eclampsia
PIBF: progesterone-induced blocking factor
PTD: pre-term delivery
PTL: pre-term labour
RSM: recurrent spontaneous miscarriage
Th: T helper
TNF: tumor necrosis factor
This paper is dedicated to the memory of Gerard Chaouat, brilliant scientist, flamboyant human being, dear friend.
The author contributed solely to this paper.
The author declares that he has no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2022.
Copyright: © The Author(s) 2022. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Gustaaf Albert Dekker, Pierre Yves Robillard
Kushaan Khambata ... Satish K. Gupta
Gursaran P. Talwar ... Krishna M. Ella
Julia Szekeres-Bartho
Shigeru Saito ... Sayaka Tsuda
Noémie Abisror ... Arsene Mekinian
Ruchi Sachdeva, Rahul Pal
Shibin Cheng ... Surendra Sharma
Betcy Susan Johnson, Malini Laloraya
Alison McCallion ... Chandrakant Tayade
Pier Luigi Meroni ... Francesco Tedesco
Marijke M. Faas
Alaa Kazhalawi ... Nathalie Lédée
Chiara Agostinis ... Roberta Bulla
Mickey V. Patel ... Charles R. Wira
Thanh Luu ... Joanne Kwak-Kim