 Review
Review

Affiliation:
1Department of Pediatrics, Division of Allergy and Immunology, Arkansas Children’s Hospital, Springdale, AR 72762, USA
Affiliation:
2Department of Pediatrics, Division of Allergy and Immunology, University of North Carolina, Chapel Hill, NC 27599, USA
Affiliation:
2Department of Pediatrics, Division of Allergy and Immunology, University of North Carolina, Chapel Hill, NC 27599, USA
Email: Allison_burbank@med.unc.edu
ORCID: https://orcid.org/0000-0002-5469-0225
Explor Asthma Allergy. 2026;4:1009119 DOI: https://doi.org/10.37349/eaa.2026.1009119
Received: January 07, 2026 Accepted: March 08, 2026 Published: March 27, 2026
Academic Editor: Laurent Mascarell, Stallergenes SAS, France
The article belongs to the special issue Climate Change, Allergy, and Immunotherapy
Climate change is reshaping the aeroallergen landscape, with rising temperatures, elevated CO2, shifting precipitation, and land-use change extending pollen seasons, increasing pollen loads and allergenicity, and expanding the geographic range of allergenic plants. These changes are accompanied by escalating air pollution from fossil fuel combustion and wildfires that act as an adjuvant with co-exposure with allergen exacerbate allergic airway disease. Vulnerable populations—particularly those in socioeconomically disadvantaged and marginalized communities in the US—experience disproportionate exposure to pollutants and allergens due to structural inequities that result in some populations being exposed to more environmental hazards than other groups. Climate-amplified aeroallergen exposure and air pollution are associated with higher sensitization, symptom burden, exacerbations, and healthcare use. Structural inequities magnify exposures to allergens and air pollution, while also influencing the social environment through concentration of poverty and diminished access to resources. This review synthesizes evidence linking climate change-related effects on aeroallergens and air pollution with allergic disease risk and the modification of this relationship by social vulnerability, with a focus on Europe and North America. We also highlight established and emerging strategies to mitigate the effects of climate change on allergic disease prevalence and morbidity, including anticipatory guidance, digital forecasting, community adaptation measures, and local, regional, and national policies that promote responsible land use, healthy housing, and equity-focused public health initiatives.
Climate change is increasingly recognized as a critical determinant of global health, with profound implications for respiratory and allergic diseases. Since the mid 18th century, dramatic shifts in material production, population dynamics, occupational opportunities, and social structure have defined human life on the planet. The industrial revolution, which according to most estimates, began in the British Isles in the 1760s, introduced the concept of mass population in urban areas. While the deleterious effects of this pollution and urbanization were obvious even by the early 19th century, the cumulative effects of what began as a triumph of engineering have led to an increased recognition of the true scope of the effects that pollution and urbanization have had on the human species. Simultaneously, human driven atmospheric changes, including rising temperatures, elevated atmospheric carbon dioxide (CO2), and shifting precipitation patterns, have altered the timing, intensity, and geographic distribution of pollens, leading to greater symptom burden in those with allergic rhinitis and asthma. These effects are amplified by co-exposure to fossil fuel combustion products and climate-driven increases in wildfires and extreme weather.
Allergic rhinitis affects up to 20% of people worldwide, even by conservative estimates [1], and asthma affects an estimated 3–4% of the global population. Urban dwellers bear a larger burden of allergic disease than their rural counterparts [2]. Urban, socioeconomically disadvantaged and racially minoritized communities often experience higher exposure to environmental hazards in the US. Not only are these groups more likely to be allergy sufferers, but as a result of structural inequities, they are also more likely to live in neighborhoods in close proximity to pollution sources and in substandard housing conditions where they are exposed to increased levels of indoor allergens such as mouse, cockroach, and molds [3]. These factors compound the health impacts of climate change, leading to increased prevalence and severity of allergic disease in populations already burdened by limited access to healthcare and other social determinants of health. In this way, climate change has been described as another social determinant of health, disproportionately affecting marginalized communities and amplifying the health impacts of other determinants such as poverty [4].
As our understanding of the impacts of human driven atmospheric and climate change on allergy sufferers continues to grow, we will continue to see the very real changes that our species has wrought upon itself. require integration with equity-focused policies and public health initiatives. The interplay between climate change and social vulnerability, and their combined influence on allergic disease outcomes, is not well characterized, particularly in low and middle income countries, but is of increasing importance due to the rise in global wealth inequality. The biopsychosocial model of disease explains health and illness as the result of the dynamic interaction among biological, behavioral, psychological, and social and environmental factors (Figure 1). Understanding the mechanisms linking climate change, air pollution, and allergic disease, as well as the modifying role of social vulnerability, is essential for developing comprehensive strategies to improve allergic disease outcomes. This review synthesizes current evidence on climate-related drivers of allergic disease, while exploring both the biological and social pathways that mediate these effects and highlighting strategies for risk mitigation and adaptation. Given the limited literature describing this relationship in low and middle income countries, this review primarily includes European and North American studies.
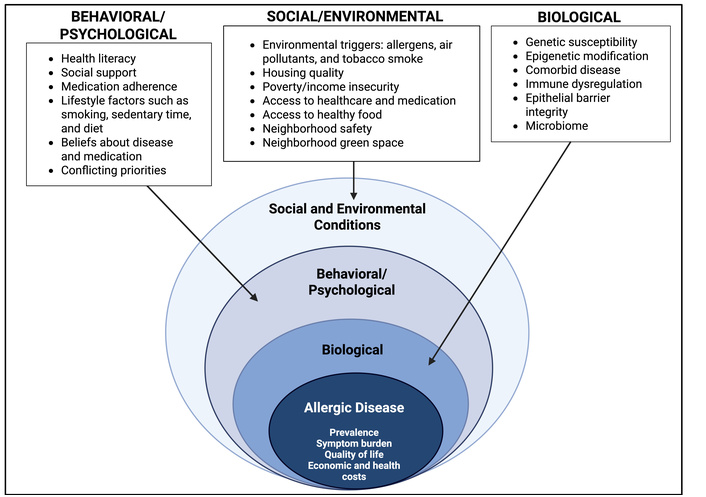
Biopsychosocial model of allergic disease. Created in BioRender. Burbank, A. (2026) https://BioRender.com/qju6pl0.
While the damaging effects of climate change are ubiquitous, their effects on pollen production, pollen distribution, and pollen allergenicity represent an additional burden on pollen-sensitized individuals that will only continue to increase. These effects have been well-documented over the last quarter century. The timing and duration of pollen release are directly affected by temperature and precipitation, particularly at higher latitudes [5, 6]. Increased global temperatures have been correlated with the earlier start of deciduous tree pollen season in the United States, from 3–22 days earlier over the past several decades [6]. Conversely, weed pollination season may be delayed by high maximum temperatures during the months of June and July, as observed in Central and eastern Europe [7], while delayed frosts were associated with a 13–27 days increase in duration of ragweed pollen season in North America [8]. Precipitation reduces airborne pollen in the short-term, but by promoting plant growth, may alter pollen production. The effects of precipitation on pollen production are variable depending on plant species; a systematic review of the effects of meteorological factors on pollen season characteristics observed a positive relationship between precipitation and grass pollen levels, while the associations with tree and weed pollens was variable [9]. Hamaoui-Laguel et al. [10] estimated that ragweed pollen levels will quadruple by 2050 in northern and eastern Europe, related predominantly to climate change and land use change that facilitates the growth and geographic spread of ragweed plants.
In addition to temperature and precipitation related changes to the timing of pollen production, increased atmospheric CO2 drives increased pollen production beyond simply providing an increased substrate for photosynthesis. While the growth of ragweed under increased CO2 conditions is significantly enhanced, pollen production is stimulated several times more [11]. Ladeau and Clark [12] demonstrated that Pinus taeda (loblolly pine) trees from high CO2 environments started producing pollen at much younger age than those grown at ambient CO2 levels. As more suitable growing temperatures advance towards the poles, allergens that were previously confined to more temperate climates are encroaching upon new territories. While plant distribution shifts have been modeled for decades, observed shifts in plant ranges are already occurring. Bermuda grass (Cynodon dactylon) is replacing cool weather forage above the traditional 33°N parallel in the southern US state of Georgia [13], while the distribution of red maple (Acer rubrum) and paper birch (Betula papyrifera) saplings has shifted northward by 20–35 km across eastern Canada [14]. Population-level pollen exposure is also influenced by land use and urbanization. Clearing of land in urban planning causes soil disturbance that favors the growth of ruderal species like ragweed. Within urban areas, a large percentage of airborne ragweed pollen can be attributed to vacant lots [15]. The urban heat island effect and concentrated fossil fuel combustion products may disproportionately increase pollen exposure in urban areas compared to non-urban areas through heat and CO2-related alteration of pollen season and pollen allergenicity [16–18]. Urban greening efforts, while important for cooling and as a sink for CO2, may contribute to increased pollen burden, particularly if pollinating plants and non-native or invasive plant species are used. Urbanization has been linked with increased amounts and diversity of pollen allergens related to the placement of pollinating plants in urban green spaces [19, 20]. Other land use changes, such as agricultural land use and reforestation efforts, have been observed to increase pollen abundance. Expansion of agricultural lands in the Mediterranean region was associated with a rise in Olea pollen (from olive growing) and Pinus pollen from pine reforestation [17, 18]. Shifts such as these, with more dramatic shifts modeled for the future, expose populations to new allergens and greater pollen allergen loads that may influence allergic sensitization and allergic symptom burden [16].
Lastly, the effects of climate change are not only influencing pollen production and distribution but are also modifying the allergenicity of airborne allergens. In a mouse model, Rauer and colleagues [21] demonstrated that pollen from ragweed plants grown under high CO2 conditions provoked a greater inflammatory response, increased mucous production, and higher ragweed-specific immunoglobulin E (IgE) levels than plants grown under ambient CO2 conditions. Silva and colleagues [22] demonstrated that sensitized patients’ sera showed enhanced IgE binding to pollen protein extracts that were subjected to higher CO2 levels.
The effects of climate change on the production, distribution, and allergenicity of pollen coincide with an increase in the prevalence of allergic sensitization [23], allergic rhinitis and asthma [24–28]. Savouré et al. [24] conducted a study of the worldwide prevalence of rhinitis in adults, observing for the first time an overall increase in the global prevalence of rhinitis from the 1970s to 2020, albeit with significant variability by geographic region (with the highest increases observed in Europe and China). In urban environments, the prevalence of allergic rhinitis in children outpaces that of their peers from rural, less developed areas for reasons discussed previously [29]. European models of future ragweed pollen levels predicted a doubling of ragweed sensitization prevalence in Europe by 2041–2060, particularly in areas where sensitization is currently less common, such as France, Germany, and Poland [30]. This increase in sensitization was attributed to climate impacts on plant phenology and the spread of invasive species. Changes in plant phenology are also linked to increased allergic rhinitis disease burden. In US adults, those living in counties with a very early start or very late start of tree pollen season had a 14% and 18% higher odds of reporting allergic rhinitis symptoms, respectively [31]. This relationship was strengthened in Non-Hispanic Black individuals, older adults, and individuals with lower educational attainment. Studies in Australia [32] and Croatia [33] similarly linked rising pollen levels with an increase in allergic rhinitis symptoms. A small number of studies have observed an association between increased healthcare usage for allergic rhinitis and increased pollen levels or altered pollen seasons [34–37]. In the UK, high counts of grass and nettle pollens were associated with a three times higher likelihood of physician consultation for allergic rhinitis (relative risk 3.33, 95% confidence interval 2.69 to 4.12) [34]. Similar observations were reported for Ambrosia pollen levels and consultations for allergic rhinitis in Montreal, Canada [35]. This relationship was disproportionately stronger in high income groups who were more likely to receive consultation visits than low income groups. Quantitative estimates of healthcare expenditures attributable to pollen in the context of climate change are very limited and highly dependent on region, allergen species, and methodology used. Simulations of annual allergy-related costs from ragweed pollen exposure in Austria and southern Germany under current climate conditions predicted a tripling of annual costs by 2050 [38]. Factoring in different degrees of climate change, the predicted 2050 annual costs increased by 20–40%. The effects of climate change and other human-influenced changes in our natural landscape will continue to alter how individual patients and communities as a whole experience and respond to pollen and other airborne allergens.
Climate change and air pollution are interconnected in several important ways and are both heavily driven by man-made sources (predominantly the burning of fossil fuels) as well as natural sources (burning biomass and agriculture). In 2023, global CO2 emissions from energy production reached an all-time high [39]. As the generation of greenhouse gases increases, more heat is trapped in the atmosphere, leading to rising global surface temperatures. This warming contributes to an increase in severe weather events, such as extreme heat, droughts, intense tropical storms, and major flooding events. Higher temperatures also increase the demand for energy production, generating more greenhouse gases, principally CO2, and emitting more particulate matter (PM), especially PM less than 2.5 um in diameter (PM2.5), and gaseous pollutants like volatile organic compounds (VOCs) and nitrogen oxides (NOx), which perpetuate the cycle by trapping more heat. Higher surface temperatures favor the production of ground-level ozone (O3) from VOCs and NOx. An increasingly hot, dry climate increases the frequency of sand and dust storms as well as wildland fires that emit large amounts of PM2.5 into the air.
Though population exposure to PM2.5 decreased on a global level from 2016–2021, divergent regional trends were observed. Higher income countries in North America and Europe observed reduced overall exposure to pollutants like PM2.5 due to reduced reliance on coal and other fossil fuels, while populations in East and South Asia, the Middle East, and Sub-Saharan Africa experienced increased exposure to PM2.5 [40]. Globally, exposure to NOx increased across major cities from 2000–2019, with a similar pattern on regional differences, with reductions in exposure observed in North America and Europe, while South Asia, the Middle East, and Sub-Saharan Africa experienced increases in NOx exposure [40]. Similarly, global exposure to ground level O3 increased during this period, with North America and Europe observing a reduction in O3 exposure owing to reduced emission of precursors (VOCs, NOx), while Africa, South Korea, and India experienced the largest increase in O3 exposure. Increased exposure to wildfire-sourced air pollution was observed across the globe from 2010–2019 compared to the prior decade, with low income countries experiencing 4 times greater exposure than high income countries [41].
These changes have major relevance to human health. Exposure to byproducts of fossil fuel combustion has been linked with increased prevalence of asthma [42–46], allergic sensitization [42, 47, 48], and allergic rhinitis [42, 46, 49]. Short term increases in pollution exposure were associated with reduced lung function [42, 50–53], increased incidence of emergency department (ED) visits [54, 55], particularly among young children under 4 years. A recent study by Wang et al. [56] reported that wildfire-associated PM2.5 was associated with higher risk of ED visits for asthma, chronic obstructive pulmonary disease and upper respiratory tract infection than non-wildfire-associated PM2.5, suggesting that wildfire-generated PM may have uniquely toxic effects on human airways. A similar increased in hospitalizations for asthma exacerbation [53, 57–59] and increased odds of asthma mortality [60] were observed during wildfire smoke events. Wildfire-specific increases in PM were strongly associated with asthma-related ED visits, with a recent metanalysis observing an 11% increase in asthma ED visits per unit increase in PM exposure [61]. Young children are especially vulnerable to the effects of wildfire-specific PM2.5, with one study observing that compared to other sources of PM2.5, wildfire-attributed PM2.5 exposure was associated with a 10 times higher increase in emergency room and urgent care visits among children 0–5 years of age [62]. Wildland firefighters and outdoor workers are also at elevated risk of negative health effects from wildfire-generated PM2.5 [63, 64].
A well-documented interaction is observed between air pollution and aeroallergens. Risk of asthma-related hospitalizations increased as daily levels of aeroallergen and ambient PM2.5 increased [65]. The precise mechanism for the pollution-allergen interaction is incompletely understood and may occur through direct and/or indirect effects. Air pollutants may have direct effects on allergens through chemical modifications that enhance the allergenicity of pollen and fungal spores. Kankaanpää et al. [66] observed that birch tree pollen collected from major roadways contained 2.6-fold higher concentrations of Bet v 1 relative to samples from a low traffic residential area. Aspergillus fumigatus demonstrated a 2-to-5-fold increase in the allergenicity of the spores when grown under exposure to ambient air nitrogen dioxide (NO2) and O3 collected from an urban area in Israel [67]. Separate experiments by the same investigators showed the allergenicity of Aspergillus fumigatus increased with increasing NO2 exposure in a dose dependent manner. There was no significant relationship with increasing O3 exposure, though proteomics analysis revealed significant protein modifications (including allergenic proteins) occurred with both O3 and NO2 exposure. Pollutant-mediated nitration of proteins may alter the allergenicity of the principal allergens such as Bet v 1 in birch tree pollen. Allergen-specific T cell lines stimulated with experimentally nitrated Bet v 1 showed greater proliferative responses compared to unaltered Bet v 1, suggesting that pollutant-associated nitration of allergenic proteins may be a mechanism by which pollutants increase the immunogenicity of birch tree pollen and other allergens [68]. Similar experiments conducted with antigen presenting cells (APCs) reported that nitrated Bet v 1 was associated with increased allergen presentation by APCs [69]. It is also postulated that particulate air pollutants facilitate the transport of allergens to the small airways, where they induce allergic airway inflammation in sensitized individuals [70, 71]. Knox et al. [72] detected diesel exhaust particles (DEP) bound to major grass pollen allergens, supporting the theory that air pollutants can deliver allergens to the airways.
Pollutants may potentiate allergic airway inflammation through several possible mechanisms, including oxidative damage, epithelial barrier disruption, immune dysregulation, and epigenetic modification. Air pollutants induce epithelial barrier dysfunction [73, 74] through oxidative stress-related tissue damage [75], disruption of tight junctions [76], impaired mucociliary clearance [75, 77], and airway inflammation [78, 79], and that could increase allergen penetration into the airway epithelium [71, 80]. PM was air pollutants like DEP may act as adjuvants that promote a T helper cell type 2 (T2) inflammatory response promote both allergic sensitization through allergen-specific IgE production and exacerbation of established allergic disease [81, 82]. Allergic volunteers exposed intranasally to ragweed allergen experienced a greater T2 inflammatory response when co-exposed to DEP, with higher nasal concentrations of IL-4, IL-5, and IL-13 as well as 16-fold increase in ragweed-specific serum IgE [82]. Pollution exposure may induce epigenetic modifications that alter risk of developing allergic disease. Exposure to PM2.5, carbon monoxide (CO), and O3 in early life was linked with altered methylation of CpG sites in immunoregulatory genes, FOXP3, IL-10, and IFNγ [80, 83], which could affect later risk of developing allergic disease. Epigenetic modifications may be passed to offspring, influencing allergic disease prevalence in future generations [73].
Existing health, wealth, and environmental inequities exacerbate the negative effects of climate change on allergic disease and asthma (Figure 2). In the US, racially minoritized and low income populations are disproportionately exposed to pollution in their neighborhoods, schools, and homes [84–87]. Neighborhood disadvantage goes hand-in-hand with increased exposure to environmental hazards such as air pollution, a concept known as environmental injustice, in which some groups are exposed to environmental hazards to a greater degree than other groups. Historical and ongoing residential segregation practices have resulted in the siting of industrial polluting facilities, major roadways, and bus depots in socioeconomically disadvantaged neighborhoods with a high proportion of people of color [86, 88]. Black race, lower education level, and lower income were associated with greater likelihood of living within one mile of a polluting industrial facility [89]. Racial and ethnic minority populations and groups with lower socioeconomic status are more likely to live, work, and go to school in close proximity to major roadways [90, 91]. As such, Non-Hispanic Black and Hispanic children were exposed to higher levels of traffic-related air pollution than White children and were more likely to experience symptoms of asthma [92]. Non-Hispanic Black race was associated with a disproportionately higher likelihood of living in areas with the greatest projected increase in mortality due to climate-change related increases in PM2.5 [93]. Black children and children from families with low income and low educational attainment were more likely to live in areas with the highest projected increase in PM2.5-attributed new asthma diagnoses and asthma related ED visits.
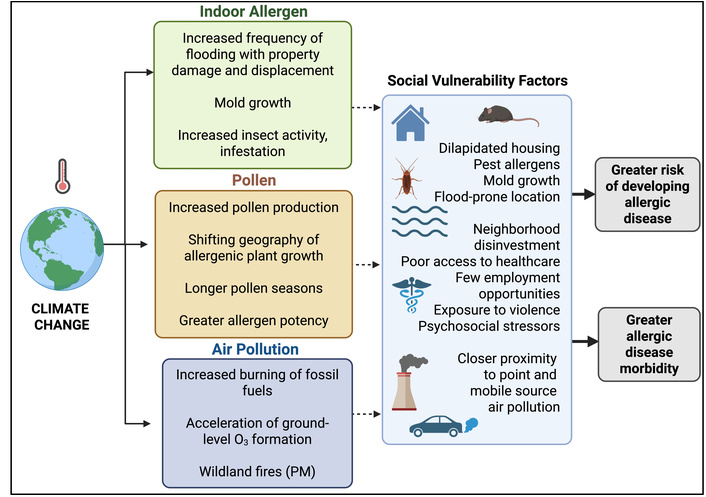
Interplay of climate change and social vulnerability. PM: particulate matter. Created in BioRender. Burbank, A. (2026) https://BioRender.com/kohs73e.
Neighborhood deprivation is also associated with poor quality and dilapidated housing infrastructure. Neighborhood disinvestment leads to a higher proportion of poorly insulated and poorly ventilated housing with pest infestation (cockroaches, rodents), lack of air conditioning, and moisture damage with mold and mildew growth. Exposure to poor quality housing has been extensively linked with allergic disease and asthma prevalence and morbidity [94–97]. Non-Hispanic Black individuals are more likely to live in poor housing conditions compared to White individuals and are also more likely to become sensitized to cockroach, mold, and seasonal pollens [98, 99]. As climate change brings increasingly intense and frequent storms, exposure to these indoor allergens is likely to increase. Low income and racial and ethnic minority neighborhoods are more likely to be sited in low-lying, flood-prone areas [100]. A survey of residents of Long Island, Queens, and Staten Island following Hurricane Sandy observed that individuals residing in areas with the lowest household income and the highest proportion of non-white residents were more likely to have experienced flooding. Older age was also a risk factor for experiencing flooding [101]. Women and Black individuals in Texas were significantly more likely to be hospitalized for asthma during the year following Hurricane Harvey, compared to men and White individuals, respectively [102]. Flooding events lead to water damage and promote growth of mold. Increasing temperatures and moisture increase insect activity and reproduction, facilitating worsening of pest infestations in these vulnerable communities [103]. These communities tend to have fewer resources to repair the damage or to relocate to safer housing. As such, these populations are exposed to higher levels of indoor mold that have been linked to increased allergic rhinitis and asthma morbidity [104–106].
In addition to poor housing stock, community disinvestment is associated with fewer opportunities for employment and education, reduced access to quality healthcare, nutritious food, green spaces for recreation and increased exposure to violence and psychosocial stressors, and increased odds of adverse childhood experiences. These factors have been associated with higher odds of asthma diagnoses [107–109] and more frequent asthma symptoms and healthcare utilization [110–113].
Multiple approaches beyond reduction of greenhouse gas emissions are needed to address climate change-related effects on allergic disease, from individual and community-led programs to state and federal policy changes that direct efforts to the most climate-vulnerable communities (Table 1). Richter et al. [38, 114] demonstrated significant cost savings to the healthcare system of ragweed management through surveillance, control, and selective eradication measures in Austria and southern Germany. Real-time pollen monitoring and forecasting systems, increasingly powered by artificial intelligence (AI), enable individuals to anticipate high pollen days and adjust behaviors or medication timing accordingly. However, currently there are few automated systems with this capability. The small number of automatic pollen samplers with independently reviewed performance data demonstrated 80 to 90% accuracy for identifying pollen species, eliminating the need for time-consuming manual analysis [115]. Machine learning is being incorporated into real-time monitors to enhance the ability to correctly differentiate pollen species, with promising preliminary results [116]. In another example of technological mitigation strategies, a recent study by Holzmann et al. [117] demonstrated that amongst grass pollen-allergic participants, use of an allergy smartphone application (app) with pollen forecasting functionality was associated with increased medication use, fewer reported symptoms and lower activity impairment compared to a form of the app that included only symptom tracking and general information about allergies. Enhanced reporting systems for aeroallergen levels, emerging allergens, and geographic shifts in allergenic plants are critical. Integrating pollen and air quality alerts into public health platforms and mobile apps ensures timely communication to healthcare professionals and community members, supporting preventive measures and reducing exposure. Preemptive use of intranasal corticosteroids during anticipated high pollen or poor air quality periods was suggested as an evidence-based strategy for reducing allergic rhinitis exacerbations [118, 119].
Mitigation and adaptation strategies for climate change impacts on allergic diseases.
| Strategies | Examples | References |
|---|---|---|
| Surveillance of allergenic species and targeted eradication |
| [38, 114] |
| Real-time pollen monitoring and forecasting |
| [115–122] |
| Public health considerations in land use |
| [123, 124] |
| Engineering solutions for adaptation to increased flood risk |
| [125, 126] |
| Municipal, state, and federal policy |
| [127, 128] |
| Improvements to housing infrastructure |
| [129–133] |
| School-based health programs |
| [134–136] |
| Community investment |
| [137, 138] |
Social determinants such as poverty, systemic racism, and inadequate housing amplify allergy and asthma burden [123, 139]. Alongside larger scale efforts to reduce the drivers of climate change, interventions targeting these inequities—such as housing mobility programs, housing remediation after natural disasters, community-driven health communication, and school-based health programs—are critical to protecting climate-sensitive populations [129, 130, 134]. Incorporating public health considerations into land use planning and zoning decisions is needed to reduce the inequitable distribution of environmental hazards [123, 124]. Collaborative approaches involving health professionals and community stakeholders ensure alignment with equity and environmental resilience goals. Integrated pest management programs, which combine sanitation, structural repairs, and judicious pesticide use, effectively reduce indoor allergen exposure [132, 135]. Implementation of education and multicomponent environmental assessment and remediation in schools and residential settings has demonstrated reductions in pest allergens, reduced asthma symptom days, missed school days, and acute care visits, as well as improved quality of life among asthma patients [135, 140, 141]. Green housing initiatives, including enhanced ventilation and moisture control, are needed to reduce asthma morbidity in individuals living in substandard housing [106]. Mold remediation programs, guided by multidisciplinary teams, significantly reduce exacerbations and healthcare utilization [142], underscoring the importance of healthy housing interventions. Anti-idling campaigns near schools and transitioning public transportation fleets to electric or low-emission vehicles reduce exposure to DEP and PM [127]. These measures are projected to reduce the burden of asthma and allergic disease in urban environments.
The intersection of climate change, air pollution, and allergic disease represents a growing public health challenge with profound implications for global health equity. Climate change is intensifying allergic disease through convergent pathways: earlier and longer pollen seasons, increased pollen production and allergenicity, and the poleward spread of allergenic taxa, along with greater exposure to air pollutants like PM, NOx, and O3. Upstream social determinants—including poverty, substandard housing, neighborhood disinvestment, and proximity to traffic and industrial sources—enhance allergic disease risk in socioeconomically disadvantaged communities.
The expansion of automated aeroallergen monitoring and AI-enhanced forecasting provides opportunities to integrate environmental surveillance with patient-centered decision support. Anticipatory guidance informed by real-time pollen and air quality data can blunt peaks in symptoms and exacerbations. Environmental interventions—allergenic plant species monitoring and eradication programs, engineering solutions to adapt to changing climate, and enforcement of air quality regulations—address dominant exposure sources for many individuals. Public health policies that promote healthy housing, access to necessary health services, and support of community-based health programs are a crucial component of interventions to mitigate the downstream consequences of climate change. Directing resources to climate-vulnerable neighborhoods—those in close proximity to polluting facilities, major roadways, high flood risk, and inadequate housing—is essential to reduce health disparities.
In summary, the effects of climate change on allergic disease represent an urgent challenge but one that can be overcome through cooperative efforts to address and build resilience against the biological, environmental, and social drivers of allergic disease that are amplified by climate change.
AI: artificial intelligence
APCs: antigen presenting cells
app: application
CO2: carbon dioxide
DEP: diesel exhaust particles
ED: emergency department
IgE: immunoglobulin E
NO2: nitrogen dioxide
NOx: nitrogen oxides
O3: ozone
PM: particulate matter
PM2.5: particulate matter less than 2.5 um in diameter
T2: T helper cell type 2
VOCs: volatile organic compounds
AI-assisted work statement: During the preparation of this work, authors used Microsoft Copilot to improve the readability of the manuscript. After using the tool, authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
MCB: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. CMT: Investigation, Visualization, Writing—original draft, Writing—review & editing. AJB: Conceptualization, Investigation, Project administration, Supervision, Visualization, Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 2080
Download: 23
Times Cited: 0
Nhan Pham-Thi, Pascal Demoly
Alessandro Cinquantasei ... Marcello Albanesi
Jean-Pierre Besancenot, Laurent Mascarell
Nicolas Visez ... Romain Courault
Jeremy Corriger ... Julien Goret
Natalia Rodríguez-Otero
