Short Communication
Short Communication

Affiliation:
1Department of Occupational and Environmental Medicine, Epidemiology and Hygiene, Italian Workers’ Compensation Authority (INAIL), 00078 Monte Porzio Catone, Italy
Email: m.dovidio@inail.it
ORCID: https://orcid.org/0000-0002-5452-3312
Affiliation:
1Department of Occupational and Environmental Medicine, Epidemiology and Hygiene, Italian Workers’ Compensation Authority (INAIL), 00078 Monte Porzio Catone, Italy
ORCID: https://orcid.org/0000-0002-2553-0345
Affiliation:
1Department of Occupational and Environmental Medicine, Epidemiology and Hygiene, Italian Workers’ Compensation Authority (INAIL), 00078 Monte Porzio Catone, Italy
ORCID: https://orcid.org/0000-0002-7582-6179
Affiliation:
2Department of Environmental Biology, Sapienza University of Rome, 00185 Rome, Italy
Affiliation:
3Allergy and Clinical Immunology Unit, San Giovanni di Dio Hospital, 50143 Florence, Italy
ORCID: https://orcid.org/0000-0002-0658-2449
Affiliation:
4University Hospital Institute – Immun4Cure (IHU Immun4Cure), INSERM & UM, 34090 Montpellier, France
ORCID: https://orcid.org/0000-0002-6340-9300
Affiliation:
5Division of Respiratory and Allergic Diseases, High Speciality Hospital ‘A. Cardarelli’, 80131 Naples, Italy
6Respiratory Allergy School of Specialization in Respiratory Diseases, Federico II University of Naples, 80138 Naples, Italy
ORCID: https://orcid.org/0000-0002-0503-9428
Explor Asthma Allergy. 2026;4:1009120 DOI: https://doi.org/10.37349/eaa.2026.1009120
Received: November 28, 2025 Accepted: February 24, 2026 Published: April 01, 2026
Academic Editor: Uday Kishore, University of Oxford, England
The article belongs to the special issue Environment, Infectious Diseases, and Allergy
Occupational allergens are an important cause of diseases emerging in the workplace, both indoor and outdoor, causing conditions such as allergic asthma, dermatitis, and rhinitis. Numerous national and international institutions focus on sensitizing agents able to induce allergies in workplaces, which are also considered by the International Classification of Diseases (ICD)-11, underlining their increasing worldwide importance. There is thus the need to develop and implement new, multidisciplinary approaches to study and monitor these agents, taking into account different sources of exposure, environmental concentrations, co-factors of exposure, and individual susceptibility. This includes the integration between traditional and innovative methodologies applied to environmental and biological matrices, as well as the use of “omic” techniques. In this picture, information, training, and communication emerge as fundamental for workers. This kind of approach will permit us to attain a better management of exposure to allergens in the workplace, improving the well-being of workers worldwide.
Allergic diseases affect up to 40% of the population of the developed world [1] and, in particular, occupational allergies affect more than 300 million workers worldwide [2], representing a major health issue in the workplace. Among the most common occupational allergic diseases, there is allergic dermatitis, accounting for up to 90% of occupational skin diseases, and allergic asthma, accounting for 15–20% of all adult asthma cases [2]. Given their relevance, these health issues need to be accurately studied and monitored using appropriate methods and expertise, considering a holistic approach and preventive practices [1, 2].
In this short communication, we examine the need for and the advantages that can be granted by a multidisciplinary approach in the study, management, and prevention of occupational allergies.
The number and sources of allergens responsible for occupational diseases are constantly growing in Western countries during the industrialization era in the 20th century and more recently in different areas of the developing world [3]. Agricultural and industrial processing techniques and newer production technologies may introduce chemical and biological substances in workplaces, such as organic and inorganic dust, hazardous gases, bioaerosols that can cause allergic respiratory and skin disorders, as well as immunotoxic reactions in many categories of workers [3, 4]. Indoor and outdoor workers employed in different activities could be exposed to allergens of different origins (biological, chemical, and physical) [5].
The impact of occupational allergies is underlined by the analysis of the statistical database of the Italian Workers’ Compensation Authority (INAIL), based on the International Classification of Diseases (ICD)-10 Classification and referred to confirmed positive cases in different occupational sectors (Tables 1, 2, 3, and 4).
Diseases of the respiratory system, skin, and subcutaneous tissue defined/confirmed positive in total management (industry and services, agriculture, state account) in the INAIL database [6].
| ICD-10 sector | Year of registration | ||||||
|---|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2023 | 2024 | |||
| Diseases of the respiratory system (J00-J99) | 776 | 700 | 700 | 694 | 553 | ||
| Diseases of the skin and subcutaneous tissue (L00-L99) | 119 | 134 | 165 | 185 | 192 | ||
| ICD-10 sector | ICD-10 class | Year of registration | |||||
| 2020 | 2021 | 2022 | 2023 | 2024 | |||
| Diseases of the respiratory system (J00-J99) | Other diseases of upper respiratory tract (J30-J39) | 26 | 18 | 31 | 37 | 26 | |
| Chronic lower respiratory diseases (J40-J47) | 84 | 86 | 69 | 63 | 58 | ||
| Upper respiratory tract | Year of registration | ||||||
| ICD-10 sector | ICD-10 class | ICD-10 | 2020 | 2021 | 2022 | 2023 | 2024 |
| Diseases of the respiratory system (J00-J99) | Other diseases of upper respiratory tract (J30-J39) | Allergic rhinitis, unspecified | 6 | 5 | 9 | 12 | 6 |
| Chronic rhinitis, nasopharyngitis and pharyngitis | 1 | 1 | 0 | 0 | 1 | ||
| Lower respiratory tract | Year of registration | ||||||
| ICD-10 sector | ICD-10 class | ICD-10 | 2020 | 2021 | 2022 | 2023 | 2024 |
| Diseases of the respiratory system (J00-J99) | Chronic lower respiratory diseases (J40-J47) | Asthma | 4 | 11 | 7 | 3 | 5 |
| Predominantly allergic asthma | 29 | 24 | 23 | 24 | 19 | ||
| Mixed asthma | 1 | 1 | 0 | 0 | 0 | ||
INAIL: Italian Workers’ Compensation Authority; ICD: International Classification of Diseases.
Diseases of the respiratory system, skin, and subcutaneous tissue defined/confirmed positive in industry and services in the INAIL database [6].
| Disease or substance that causes it | Year of registration | |||||
|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2023 | 2024 | ||
| Predominantly allergic asthma (J45.0) with its direct consequences caused by agents not included in other headings | 12 | 12 | 18 | 16 | 8 | |
| Extrinsic allergic alveolitis with or without fibrotic evolution (J67) | 0 | 2 | 5 | 2 | 0 | |
| Allergic contact dermatitis (L23) caused by agents not included in other headings | 44 | 49 | 60 | 48 | 49 | |
| Disease or substance that causes it | Year of registration | |||||
| 2020 | 2021 | 2022 | 2023 | 2024 | ||
| Predominantly allergic asthma (J45.0) with its direct consequences caused by agents not included in other headings | Cereal dust and flours | 7 | 10 | 16 | 10 | 7 |
| Wood dust | 1 | 0 | 0 | 1 | 0 | |
| Animal derivatives: dermal (dandruff, hair, feathers), biological fluids (blood and urine), excrements | 1 | 0 | 0 | 2 | 0 | |
| Mites (of food and poultry) | 1 | 0 | 0 | 0 | 0 | |
| Mycetes | 0 | 1 | 0 | 0 | 0 | |
| Prepolymers, oligomers, catalysts for the polymerization of synthetic resins | 2 | 1 | 1 | 2 | 1 | |
| Metals (platinum, cobalt, palladium) | 0 | 0 | 1 | 0 | 0 | |
| Drugs | 0 | 0 | 0 | 1 | 0 | |
| Total | 12 | 12 | 18 | 16 | 8 | |
| Disease or substance that causes it | Year of registration | |||||
| 2020 | 2021 | 2022 | 2023 | 2024 | ||
| Extrinsic allergic alveolitis with or without fibrotic evolution (J67) | Mycetes (Aspergillus, Penicillium, others) | 0 | 0 | 2 | 1 | 0 |
| Other chemical and plant-based agents that can cause extrinsic allergic alveolitis | 0 | 2 | 3 | 1 | 0 | |
| Total | 0 | 2 | 5 | 2 | 0 | |
| Disease or substance that causes it | Year of registration | |||||
| 2020 | 2021 | 2022 | 2023 | 2024 | ||
| Allergic contact dermatitis (L23) caused by agents not included in other headings | Cement | 2 | 6 | 4 | 2 | 5 |
| Metals not included in other headings | 0 | 1 | 2 | 2 | 0 | |
| Natural resins (rosin, shellac, latex, turpentine) | 1 | 3 | 2 | 1 | 3 | |
| Artificial resins (epoxy, phenolic, phenol formaldehydic, acrylic, melaminic) | 3 | 9 | 7 | 8 | 11 | |
| Organic dyes and dyes based on paraphenylenediamine, paratoluenediamine, para-aminophenol | 15 | 9 | 12 | 12 | 14 | |
| Rubber additives (dithiocarbamates, mercaptobenzothiazole, thiurams, hexamethylenetetramine, diphenylguanidine, paraphenyldiamine and its derivatives) | 4 | 2 | 4 | 5 | 7 | |
| Disinfectants and detergents | 3 | 1 | 4 | 1 | 1 | |
| Chemotherapeutics, antibiotics | 0 | 0 | 0 | 1 | 0 | |
| Plant and flower derivatives with allergenic effects | 2 | 0 | 2 | 2 | 0 | |
| Lubricating and cooling fluids | 6 | 7 | 5 | 4 | 4 | |
| Other skin sensitizing agents | 8 | 11 | 18 | 10 | 4 | |
| Total | 44 | 49 | 60 | 48 | 49 | |
INAIL: Italian Workers’ Compensation Authority.
Defined/confirmed positive allergic diseases in agriculture in the INAIL database [6].
| Disease or substance that causes it | Year of registration | ||||||
|---|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2023 | 2024 | |||
| Allergic contact dermatitis (L23) caused by agents not included in other headings | 0 | 2 | 1 | 0 | 1 | ||
| Predominantly allergic asthma (J45.0) | 5 | 5 | 2 | 4 | 2 | ||
| Extrinsic allergic alveolitis with or without fibrotic evolution (J67) | 0 | 9 | 4 | 6 | 1 | ||
| Disease or substance that causes it | Year of registration | ||||||
| 2020 | 2021 | 2022 | 2023 | 2024 | |||
| Allergic contact dermatitis (L23) caused by agents not included in other headings | Quinones | 0 | 0 | 0 | 0 | 1 | |
| Preservatives, stabilizers, and emulsifiers for feed | 0 | 0 | 1 | 0 | 0 | ||
| Derivatives of plants and flowers (primroses, chrysanthemums, geraniums, tulips) | 0 | 2 | 0 | 0 | 0 | ||
| Total | 0 | 2 | 1 | 0 | 1 | ||
| Disease or substance that causes it | Year of registration | ||||||
| 2020 | 2021 | 2022 | 2023 | 2024 | |||
| Predominantly allergic asthma (J45.0) | Grain dust | 2 | 1 | 0 | 1 | 0 | |
| Pollen from grass crops, Oleaceae, Compositae (sunflower) | 3 | 3 | 2 | 2 | 2 | ||
| Dermal derivatives (dandruff, hair, feathers), animal waste | 0 | 1 | 0 | 1 | 0 | ||
| Total | 5 | 5 | 2 | 4 | 2 | ||
| Disease or substance that causes it | Year of registration | ||||||
| 2020 | 2021 | 2022 | 2023 | 2024 | |||
| Extrinsic allergic alveolitis with or without fibrotic evolution (J67) | Spores of thermophilic actinomycetes | 0 | 2 | 1 | 4 | 0 | |
| Mycetes (Aspergillus, Penicillium, others) | 0 | 4 | 2 | 1 | 0 | ||
| Protein derivatives (avian, porcine, bovine) | 0 | 3 | 1 | 1 | 1 | ||
| Total | 0 | 9 | 4 | 6 | 1 | ||
INAIL: Italian Workers’ Compensation Authority.
Allergic diseases defined/confirmed positive in the state account in the INAIL database [6].
| Disease or substance that causes it | Year of registration | |||||
|---|---|---|---|---|---|---|
| 2020 | 2021 | 2022 | 2023 | 2024 | ||
| Predominantly allergic asthma (J45.0) with its direct consequences caused by agents not included in other headings | 0 | 0 | 1 | 0 | 0 | |
| Disease or substance that causes it | Year of registration | |||||
| 2020 | 2021 | 2022 | 2023 | 2024 | ||
| Predominantly allergic asthma (J45.0) with its direct consequences caused by agents not included in other headings | Animal derivatives: dermal (dandruff, hair, feathers), biological fluids (blood and urine), excrement | 0 | 0 | 1 | 0 | 0 |
| Total | 0 | 0 | 1 | 0 | 0 | |
INAIL: Italian Workers’ Compensation Authority.
As reported in the database, the number of cases is not very high compared to other occupational diseases (a possible reason should be attributed to an under notification), but they are high enough to not be ignored. At the same time, it is necessary to highlight that the sources of exposure are numerous and derived from biological, chemical, and physical agents.
Various categories of workers may be exposed to biological allergens, including those employed in woodworking activities who are routinely exposed to wood dust. These workers have been shown to exhibit a high prevalence of respiratory disorders, including occupational asthma, rhinitis, allergic alveolitis, cough, sneezing, dyspnea, persistent wheezing, and other adverse health effects such as eye irritation, conjunctivitis, dermatitis [7]. In particular, regarding occupational allergies, workers exposed to wood dust have shown blood serum IgE concentration more than double that of controls (0.69 μg/mL vs. 0.28 μg/mL) and similar values for IgG (8.86 mg/mL vs. 5.36 mg/mL) [7], also having significant respiratory issues. Dust derived from wood processing is therefore a heterogeneous mixture of inorganic and organic components, including wood fragments, microorganisms, endotoxins, mycotoxins, and sensitizing agents able to induce allergies, as well as other low molecular weight (LMW) chemical substances that can negatively impact respiratory health. Though a different classification as “protein agents” and “non-protein agents” was recently proposed, also based on the arbitrary nature of the former classification and the lack of a molecular weight threshold [8]. As evidenced in a study, in the European Union, workers employed in different woodworking activities such as construction, furniture and builders’ carpentry industries, sawmilling and forestry were the highest exposed to inhalable wood dust [9].
Numerous chemical agents used both in domestic and industrial settings, particularly within production processes, in the form of mixtures or derivatives, may pose risks to the health and/or safety of users. Among these are terpenes, a heterogeneous group of organic compounds derived from isoprene units and naturally produced by plants, occurring in fruits, flowers, spices, and trees. They are major constituents of essential oils, such as menthol, limonene, geraniol, and citronellal, and are widely used in perfumes, foods, over-the-counter pharmaceuticals, synthetic chemicals, rubber products, fragrances, flavorings, and the biofuel industry. Research has shown that terpenes may provide several health benefits, including anti-inflammatory, antioxidant, antibacterial, antiallergic, and anticancer effects. However, according to the European Chemicals Agency (ECHA) Classification, Labelling and Packaging (CLP) notifications, high exposure to terpene oxidation products can lead to adverse effects, including allergic skin and respiratory conditions. These substances may trigger skin allergic reactions [5, 10], and manufacturers and importers must notify ECHA of their classification and labeling in accordance with Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH) and CLP regulations. Although terpenes are generally considered to have low, dose-dependent toxicity and are commonly used as food flavorings and pharmaceutical ingredients, most available evidence comes from in vitro and animal studies [10]. Well-designed clinical trials are still needed to confirm their efficacy, establish safe exposure limits, and clarify their mechanisms of action in humans.
In occupational settings, certain workers, such as woodworkers, are exposed to volatile terpenes released from wood during mechanical processing (e.g., sawing and planing), often in combination with wood dust. Since wood contains significant amounts of terpenes in addition to cellulose, hemicellulose, and lignin, these compounds contribute to inhalation exposure at the workplace. Terpenes act as both primary pollutants and precursors of secondary pollutants, with their role as primary contaminants being particularly relevant in occupational environments. Therefore, workplaces using essential oils, fragrances, or wood materials should implement targeted control measures to reduce inhalation exposure and protect workers from potential adverse health effects.
Climate change contributes not only to global warming but also to prolonged periods of extreme cold in different continents. Extreme cold, although less investigated than heat, represents an important environmental stressor capable of worsening cutaneous conditions such as cold urticaria and impairing airway function [11, 12]. Evidence from several countries indicates that cold spells significantly increase asthma exacerbations, emergency visits, and asthma related mortality, and may even predict new onset asthma within one to two years [13, 14]. Increasing climatic variability—with more frequent and intense temperature fluctuations—has relevant implications for occupational health, particularly concerning allergic respiratory outcomes [15]. Several studies have examined the association between occupational cold exposure and the development of airway symptoms. Epidemiological data from northern Sweden show significant associations between occupational cold exposure and airway symptoms, including wheeze (OR 1.3; 95% CI 1.1–1.4), chronic cough (OR 1.2; 95% CI 1.1–1.4), and productive cough (OR 1.3; 95% CI 1.1–1.4), independent of asthma, COPD, age, sex, and smoking [16]. Prospective findings further corroborate these results. Among workers without prior airway disease, any level of occupational cold exposure on numerical rating scales (NRS > 1) predicted incident wheeze (adjusted OR 1.41; 95% CI 1.06–1.87) and incident productive cough (adjusted OR 1.37; 95% CI 1.06–1.77), while no significant association emerged for long standing cough. Notably, leisure time cold exposure showed no association with respiratory outcomes, suggesting that occupational settings—with longer exposure duration, physical workload, and reduced avoidance capacity—constitute the primary risk context.
These findings support the integration of cold exposure risk assessment into occupational health frameworks and underscore the need to establish exposure thresholds to guide preventive strategies, particularly for individuals with preexisting respiratory vulnerability [17].
The multidisciplinary approach gains more importance also in regard to the latest version 11 of the ICD (https://icd.who.int/en). Allergic and hypersensitivity conditions have been considered in ICD-11, also permitting more accurate accounting for mortality due to anaphylaxis, and comparable epidemiological data [18]. At the same time, an optimization of the allergen classification has been performed, resulting in 297 additional allergens and, among them, a 6.5% classified as occupational and 4% as miscellaneous [19].
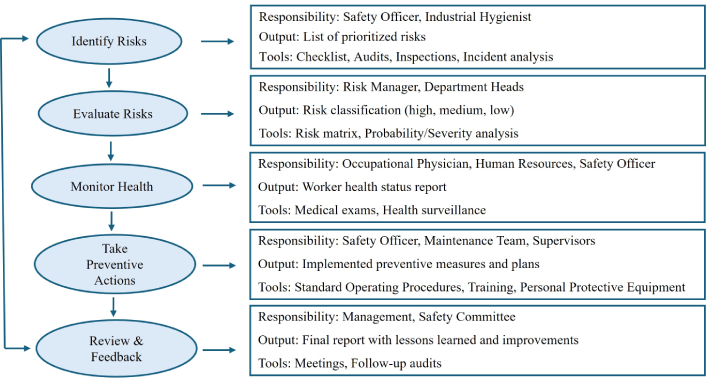
It is also necessary to improve the knowledge on occupational allergies, with a focus on agents able to induce allergies, clinical manifestations, and early recognition, with the aim of achieving better prevention and management. Our studies are addressed to a multidisciplinary and integrated approach for occupational allergies considering different sources of exposure, environmental monitoring, co-factors of exposure, individual susceptibility, integration between traditional and innovative methodologies applied to environmental and biological matrices, collaboration with medical surveillance and with all the prevention system, and research [20–22]. A multidisciplinary workflow in health, safety, and environmental management, encompassing medical surveillance and risk assessment, relies on a structured integration of specialized expertise, with each role having well-defined yet interconnected responsibilities. The workflow implemented in this study is summarized in Figure 1, which depicts how exposure assessment, surveillance, and risk management are integrated within a framework designed for continuous prevention.
Furthermore, information, training, and communication are essential for a higher level of allergy management in different occupational settings. In the current era of big data, the development of innovative technologies—such as genomics, transcriptomics, proteomics, metabolomics, and epigenomics—combined with advances in bioinformatics, artificial intelligence (AI), machine learning algorithms, and the availability of specialized datasets from multiple sources, holds great potential to transform the diagnosis and management of allergic diseases, including asthma, rhinitis, and contact dermatitis. The scientific literature already highlights how computational technologies, particularly AI, can enhance occupational health and safety and improve productivity, with the overarching goal of making workplaces more efficient and effective. Moreover, AI also plays a crucial role in the field of sensors and biosensors: advanced systems can estimate workers’ real time exposure to environmental hazards, improving allergy surveillance, reducing days lost from work, and helping public health authorities anticipate seasonal allergy peaks [23, 24]. In this regard, AI enabled mobile applications and wearable sensors can integrate real time environmental data—such as pollen concentrations, pollutants, humidity, and temperature—with clinical information to generate personalized preventive recommendations, including adjustments to inhaled corticosteroids or antihistamines. A notable example is the AI‑assisted clinical decision support system @IT‑2020, which incorporates environmental pollen data and patient symptoms to support specialists in providing customized allergen immunotherapy recommendations, within the broader context of AI‑driven decision support approaches described in contemporary allergy management frameworks [25]. Although designed for clinical use, this system can be readily applied to workers exposed to occupational allergens, as it allows the integration of environmental, individual, and behavioral data into robust predictive models. In healthcare more broadly, AI and machine learning enhance medical imaging analysis, drug discovery, remote patient care, and diagnostics, improving the predictive sensitivity of novel biomarkers and therapeutic targets for precision medicine [26]. For example, PandaOmics is an AI-driven platform for identifying potential therapeutic targets in asthma, eczema, and food allergies by analyzing publicly available datasets [27]. Similarly, platforms such as Molecular Twin integrate clinical and multi-omics data to predict disease symptoms and support the development of individualized treatments. Because multi-omics technologies generate highly complex datasets, it is essential that computational methods integrate and analyze these data effectively in order to deepen the understanding of disease mechanisms, detect early biomarkers, and advance personalized therapies. However, the generation and management of omics platforms require substantial financial investment, considerable time, and a high degree of technical and analytical expertise [28]. Despite these promising advancements, AI technologies still face several limitations and challenges, including data heterogeneity, limited generalizability, lack of standardization, insufficient information sources, and important bioethical considerations. Additionally, the cost of integrating AI into public health systems and the need for real world clinical validation remain significant barriers to widespread implementation [25]. In conclusion, a multidisciplinary and integrated approach represents the near future of both clinical and occupational allergy management. The adoption of innovative and traditional technologies, supported by AI based integration of heterogeneous data sources, will enable researchers and clinicians to better investigate occupational allergic diseases—from personalized treatment and prevention to early diagnosis.
Therefore, the early identification and complete avoidance of causal occupational agents are increasingly recognized as essential strategies for preventing work‑related allergic diseases [29, 30]. Effective prevention requires integrating engineering controls to minimize exposure, targeted education and training to improve workplace and cleaning practices, and structured medical surveillance to detect high‑risk workers promptly and optimize long‑term management.
AI: artificial intelligence
CLP: Classification, Labelling and Packaging
ECHA: European Chemicals Agency
ICD: International Classification of Diseases
MCD: Conceptualization, Investigation, Supervision, Visualization, Writing—original draft, Writing—review & editing. PC: Conceptualization, Investigation, Supervision, Visualization, Writing—original draft, Writing—review & editing. DP: Conceptualization, Investigation, Supervision, Visualization, Writing—original draft, Writing—review & editing. AL: Conceptualization, Investigation, Supervision, Visualization, Writing—original draft, Writing—review & editing. LC: Supervision, Visualization, Writing—review & editing. IAM: Supervision, Visualization, Writing—review & editing. GD: Conceptualization, Supervision, Visualization, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Aurelia S. Monk ... Adam J. Kimple
Cristiano Caruso ... Stefano Del Giacco
Aimuanmwosa Frank Eghomwanre, Henrietta Onyinye Ogbebor