 Review
Review

Affiliation:
1Department of Physiology, Faculty of Basic Medical and Health Sciences, College of Medicine, Lead City University, Ibadan 200255, Oyo State, Nigeria
Email: ajibare.ayodeji@lcu.edu.ng
ORCID: https://orcid.org/0000-0001-9600-8880
Affiliation:
1Department of Physiology, Faculty of Basic Medical and Health Sciences, College of Medicine, Lead City University, Ibadan 200255, Oyo State, Nigeria
ORCID: https://orcid.org/0009-0004-1079-8164
Affiliation:
1Department of Physiology, Faculty of Basic Medical and Health Sciences, College of Medicine, Lead City University, Ibadan 200255, Oyo State, Nigeria
ORCID: https://orcid.org/0000-0003-4231-5118
Affiliation:
2Department of Physiology, Faculty of Basic Medical Sciences, Ekiti State University, Ado-Ekiti 362103, Ekiti State, Nigeria
ORCID: https://orcid.org/0000-0002-6537-3639
Affiliation:
3Bioresources Development Centre, National Biotechnology Research and Development Agency, Ogbomoso 210211, Nigeria
ORCID: https://orcid.org/0000-0003-0071-0531
Explor Foods Foodomics. 2026;4:1010166 DOI: https://doi.org/10.37349/eff.2026.1010166
Received: November 14, 2025 Accepted: May 17, 2026 Published: June 11, 2026
Academic Editor: Guoliang Li, Shaanxi University of Science and Technology, China
The article belongs to the special issue Food Contaminants: Analysis, Occurrence and Risk Assessment
A variety of endocrine-relevant contaminant categories are now chronically co-exposed to the human population through the food chain, including direct dietary intake, packaging migration, and drinking-water pathway, such as per- and polyfluoroalkyl substances (PFAS), bisphenol analogues/phthalates, and micro- and nanoplastics (MNPs). There exists a fundamental incongruity between the current regulation of chemicals and our exposures to them. Regulatory agencies currently tend to test substances individually, but rising evidence on population-based studies shows that combined exposures are leading to thyroid ailments, metabolic issues, and negative reproductive outcomes. This review brings together mechanistic, toxicological, and human evidence that these structurally diverse contaminants functionally intersect three endocrine- and barrier-relevant signaling pathways: (i) the thyroid axis, (ii) nuclear receptor and steroidogenic signaling, (iii) gut barrier-inflammation circuits. Since the mixtures encountered in the real world cause cumulative stress on these common pathways, it is suggested that a pathway-based measurement be developed: the Pathway Disruption Load (PDL). PDL is operationalized: Tier 1 comprises pathway-specific biomarkers (TSH, free T4, sex-steroid panels, zonulin, LBP). Tier 2 is performed by applying receptor/enzyme assays (ER/AR/TR, TPO inhibition) of pertinent matrices (food extracts, water, serum) to measure the total endocrine activity, including unknown co-migrants. A combination of Tier 1 biological response and Tier 2 functional burden gives a realistic and chemical-agnostic foundation for cumulative risk evaluation, and provides a foodomics-relevant bridge between food-matrix signals (e.g., packaging/food extracts) and human biomonitoring/omics-derived biomarkers, and it also agrees with the current EFSA mixture guidance and key-characteristics frameworks. Operational priorities are re-analysis of biomarker-rich cohorts, pathway-level panels, and mixture toxicology at human-relevant doses.
Human biomonitoring over the past decade shows that most individuals carry multiple PFAS (per- and polyfluoroalkyl substances) in serum, alongside detectable bisphenol substitutes (BPS/BPF) and metabolites of high-use phthalates [1, 2]. The food chain is now a significant pathway of transfer of endocrine-relevant chemicals, with the vast majority of non-occupational exposure to PFAS estimated to be via diet and drinking water, usually at 70–90% of total exposure [3]. European economic analysis has claimed on the policy front that endocrine-disrupting chemicals are costing the European economy in the range of hundreds of billions of euros a year [4, 5]. This is the level of the problem we are attempting to make technically tractable.
In Europe and other countries, food-safety control systems already test a number of these chemicals in food using targeted chromatographic techniques [6], predominantly LC–MS/MS for PFAS, bisphenols, and phthalates, and GC or pyrolysis-GC–MS for polymer-related contaminants. This is supported by updated contaminant limits in Regulation [EU] 2023/915, including PFAS and other persistent contaminants [7], alongside routine occurrence data showing trace-to-low μg·kg–1 levels in market foods. Such data streams affirm that what biomonitoring detects in individuals parallels what food control laboratories detect in foods, providing the sampling platform on which a pathway-centered interpretation like PDL can be established [8]. Although we use the EU framework as an illustrative example, the PDL concept is intended to be jurisdiction-agnostic and compatible with national and Codex-aligned food safety systems that combine occurrence monitoring with risk-based decision-making.
In March 2024, Marfella et al. [9] published their report in the New England Journal of Medicine in which they reported that 58% of patients who received carotid endarterectomy contained polyethylene (PE) or polyvinyl chloride (PVC) particles in their atheroma, and that these patients had an adjusted risk of myocardial infarction, stroke, or death approximately 4.5-fold higher than a cohort without detectable MNPs (micro- and nanoplastics) in plaques. This observational study established that plastic particles are detectable in clinically relevant tissues and that their presence is statistically associated with worse cardiovascular outcomes—a signal warranting mechanistic investigation but not, by itself, establishing causation [9, 10]. Importantly, human dose-response thresholds for MNPs—the tissue burden at which measurable pathway dysfunction begins—remain unknown. This was closely followed by letters suggesting dangers of contamination during pyrolysis-GC/MS analysis and demanding more rigid procedural blanks [11, 12], although the association itself was not rejected. Findings such as these are uneasily placed next to the manner in which risk is yet to be computed. Food-control laboratories are generating quality occurrence data on a growing number of contaminants, but most risk characterization is being done on a substance-by-substance basis, with limited routine evaluation of whether co-occurring food-borne chemicals are simultaneously pressuring the same endocrine or barrier pathways. This review proposes an interpretive step to address that gap.
Chemical risk assessment of regulatory type still largely follows a single-substance paradigm. It was a rational approach to conventional high-dose and single-agent problems. It is less suited to chronic, low-dose, concurrent exposures that are endocrine- or barrier-acting [13, 14]. Contaminants are now measured in parts-per-trillion by analytic chemistry, and thus what was once background exposure is now a population burden [15]. The health burden of chronic non-communicable diseases has become predominant, and these disease conditions are responsive to long, low-grade endocrine and inflammatory perturbations [16]. Importantly, endocrine disruption science has itself normalized pathway-based thinking: La Merrill et al. outlined the defining features of endocrine-disrupting chemicals, and in 2024, the same group published a list of the defining features of metabolism-disrupting agents [17]; notably, in defining such agents, they included disruption of gut functionality and chronic inflammation [18]. A pathway-centered assessment is thus consistent with the existing scientific opinion. This highlights a gap in the form of a mere statement: exposure is plural, evaluation singular. This article argues that three key classes of food-chain contaminants—PFAS, bisphenol/phthalate replacements, and MNPs—converge on a limited number of endocrine- and barrier-relevant pathways, supporting a pathway-based assessment we term Pathway Disruption Load (PDL). Unlike existing cumulative-risk or mixture-assessment frameworks that aggregate chemicals by hazard or dose addition, PDL integrates biological pathway-level biomarkers with functional bioassay outputs, thereby linking exposure matrices directly to pathway perturbation in humans. This biological integration layer distinguishes PDL from current EFSA mixture guidance and exposome-based statistical frameworks, which primarily operate at the exposure or hazard-characterization level.
PDL: Conceptual Status and Distinguishing Features. Herein, PDL is proposed as a conceptual and research level integrative model, and not as a validated regulatory index. The objective is to arrange hypothesis testing, cohort re-analysis and NAM-based screening of food matrices; future validation studies will be needed to quantify hypothesis testing, cohort re-analysis, and NAM based screening of food matrices. PDL does not relate to three existing frameworks that it most closely resembles:
(i) Hazard Index (HI): The sum of chemical-specific hazard quotient, but does not assign exposures to shared biological pathways;
(ii) Margin of Exposure (MOE): which is a summation of dose-response ratio of individual substances, but does not assign exposures to shared biological pathways; and
(iii) Exposome Scores: which capture statistical associations between complex exposure mixtures and health outcomes without assigning exposures to shared biological pathways. The novelty of PDL is the functional bioassay layer (Tier 2) which fixes mixture activity directly to named endocrine and barrier pathways and makes it possible to have a biologically grounded integration that precedes and informs regulatory quantification.
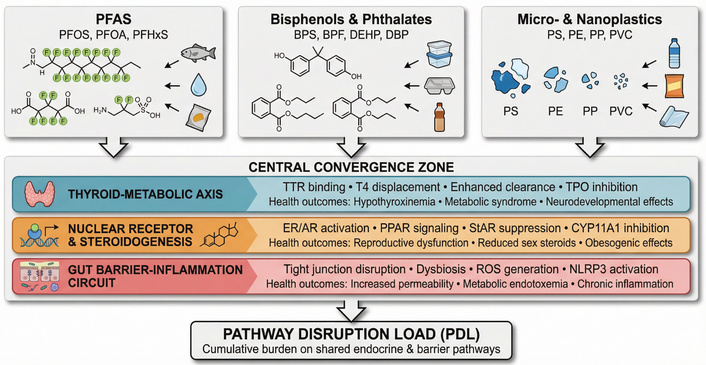
European food safety surveillance in Reg. [EU] 2023/915 has placed greater emphasis on mycotoxins, metals, and contaminants related to food processing [19], but further scientific data on the frequency of PFAS, plasticizers, and new particulate contaminants are now beginning to emerge, due to market baskets, studies on packaging migrations, and the use of sensitive LC-MS/MS analytical techniques. While this review uses the EU framework as a clear example, the underlying challenge of chronic, low-dose co-exposure through diet, drinking water, and food-contact materials is shared across jurisdictions, supporting broader relevance to global food-safety and chemical-management settings. These data demonstrate that many of the same compounds that are currently being observed in human serum are also observable in fish, bivalves, eggs, drinking water, ready-to-eat foods, and in foods that have come into prolonged contact with plastic surfaces [20–22]. Dietary patterns can shape exposure routes: Choices involving drinking-water sources and seafood/animal products may shift dietary contributions to PFAS, while reliance on packaged foods can increase contact-mediated exposures from food-contact materials and related co-migrants [3, 20–22]. The following, therefore, bridges the gap between three groups of contaminants that are proven to be present in the food chain and the endocrine-active pathways they converge at. This convergence of PFAS, bisphenol analogues/phthalates, and micro and nanoplastics on shared endocrine and barrier pathways is summarized in Figure 1. The convergent mechanistic actions are organized in Table 1. As shown in Table 1, PFAS, bisphenol substitutes, and food-borne microplastics all converge on thyroid, nuclear-receptor, and barrier pathways despite structural diversity [23–25]. The alignment of these mechanisms with mixture-risk and pathway-driven assessment frameworks is summarized in Table 2.

Convergent endocrine disruption pathways. Convergence of three major food-borne contaminant classes on shared endocrine and barrier pathways. PFAS (per- and polyfluoroalkyl substances), bisphenol analogues/phthalates, and micro- and nanoplastics (MNPs) from dietary and drinking-water sources converge on three critical biological systems: (i) the thyroid-metabolic axis, (ii) nuclear receptor and steroidogenic signaling, and (iii) gut barrier-inflammation circuits. The cumulative stress on these pathways forms the basis of the Pathway Disruption Load (PDL) framework.
Convergent mechanistic actions of emerging food contaminants.
| Contaminant class | Example compounds | Dominant food/food-contact sources (illustrative) | Primary Mode of Action (MoA) | Target pathway | Specific mechanism (evidence-based) | Supporting evidence (key citations) |
|---|---|---|---|---|---|---|
| PFAS | PFOS, PFOA, PFHxS | Dietary intake via the food chain (e.g., seafood/animal products) and drinking water | Chemical/structural mimicry of thyroid-hormone transport | Thyroid axis (transport and clearance) | PFAS bind transthyretin (TTR) and can displace T4, lowering effective TH availability; some PFAS promote TH clearance, reproducing thyroid-disrupting patterns in experimental models. | [28–30] |
| PFAS | PFOS, PFOA, mixed-chain PFAS | Dietary intake via the food chain and drinking water (mixtures in population exposure) | Receptor-mediated activation (PPAR-centric) | Metabolic/nuclear-receptor signaling | PFAS activate PPARα/γ and related lipid–glucose program consistent with the metabolism-disrupting profile described for endocrine-active chemicals. | [72] |
| Bisphenol analogues | BPS, BPF, BPAF | Food-contact materials and packaging migration (e.g., linings/plastics) contributing to dietary exposure | Hormone mimicry/substitution | ER/AR-linked nuclear-receptor signaling | BPS and BPF show ER-agonist activity comparable to BPA and exhibit anti-androgenic interference, explaining obesogenic and reproductive signals in newer cohorts. | [31] |
| Phthalates | DEHP, DBP, monoester metabolites | Food-contact plastics and packaging migration; dietary exposure via contact with plastic surfaces | Enzyme-level interference in steroidogenesis | Gonadal/adrenal steroidogenic pathway (StAR, CYP11A1) | Environmentally relevant phthalate mixtures downregulate key steroidogenic genes/proteins and reduce steroid output, matching recent animal and in vitro data. | [73–75] |
| Micro- and nanoplastic (MNPs) | Polystyrene | Food processing/contact surfaces and packaged foods; ingestion via contaminated foods and drinking water | Physical barrier injury and inflammation | Gut-barrier integrity and gut–liver axis | PS-MPs induce gut microbiota dysbiosis, disrupt tight junctions, and cause metabolic disorders in mice, creating secondary endocrine–metabolic disturbance. | [76] |
| MNPs as chemical vectors | PS, PE, PP particles detected in foods/water | Particles present in foods and drinking water; packaging/processing as entry routes with co-migrants | Vector-mediated co-exposure amplification | Cross-cutting endocrine pathways (thyroid, metabolic, reproductive) | MNP surfaces adsorb legacy EDCs (BPA, phthalates, PCBs) and can desorb them in the GI tract, effectively turning particle exposure into an EDC-mixture exposure, which current EFSA mixture guidance can already handle. | [77] |
This table organizes three major food-relevant contaminant groups into a mechanistic grid, showing that PFAS, bisphenol/phthalate plasticizers, and MNPs converge on a small number of endocrine, metabolic, and barrier pathways. BPA: bisphenol A; BPAF: bisphenol AF; BPF: bisphenol F; BPS: bisphenol S; EDCs: endocrine-disrupting chemicals; EFSA: European Food Safety Authority; MNPs: micro- and nanoplastics; PCBs: polychlorinated biphenyls; PE: polyethylene; PFAS: per- and polyfluoroalkyl substances; PFHxS: perfluorohexanesulfonic acid; PFOA: perfluorooctanoic acid; PFOS: perfluorooctanesulfonic acid; PP: polypropylene; PS: polystyrene; PS-MPs: polystyrene-microplastics; TH: thyroid hormone; TTR: transthyretin.
Alignment of convergent mechanisms with pathway-driven and mixture-risk frameworks.
| Mechanistic node (from Table 1) | Representative contaminants | Recognized/policy-relevant endpoint | Applicable framework/hook | How it supports PDL | Key sources |
|---|---|---|---|---|---|
| Thyroid-axis disruption via TTR competition and enhanced clearance | PFAS in the food chain | Altered circulating thyroid hormone; developmental thyroid concerns | EFSA Scientific Committee 2019 guidance on combined exposure; KC “alters hormone transport” | Group all TTR-active PFAS and other TTR-active food contaminants for thyroid risk | [25, 77] |
| PPAR-centered metabolic signaling activation | PFAS, some plasticizers | Dyslipidemia, insulin resistance, metabolic-syndrome-like outcomes | Consensus on key characteristics of metabolism-disrupting agents; EFSA combined-exposure workflow | Clusters PFAS with other MDAs that hit the PPAR/metabolic node | [18, 72] |
| ER/AR perturbation by bisphenol analogues | BPS, BPF, BPAF | Reproductive, obesogenic, and anti-androgenic signals are already recognized for BPA | KC EDC paper; EFSA grouping logic | Prevents regrettable substitution by keeping BPA replacements in the same cumulative group | [37, 39, 77] |
| Steroidogenesis interference by phthalate monoesters | DEHP, DBP, DnBP metabolites | Reduced sex-steroid output, male reproductive endpoints | EFSA 2019 combined-exposure guidance; KC “alters hormone synthesis” [77] | Maps any co-migrant or phthalate that suppresses StAR/CYP11A1 into a single reproductive-risk lane | [35, 46] |
| Gut-barrier injury and dysbiosis from MNPs | PS, PE, PP microplastics in food/water | Increased intestinal permeability and low-grade inflammation | 2024–2025 MNP gut-toxicity reviews | Defines barrier-inflammatory as a horizontal pathway for particles and co-ingested EDCs | [50, 59, 72] |
| Co-exposure amplification by particle-bound chemicals | Food-borne MNPs carrying BPA, phthalates, PCBs | Effective EDC-mixture exposure (higher internal dose than chemical alone) | EFSA 2019 and 2021 grouping documents | Places “MNP + adsorbed EDC” in the same cumulative group as free EDCs | [52, 53, 77] |
This table shows that the mechanistic nodes in Table 1 can be plugged directly into existing European and international tools for combined exposure and endocrine-disruptor evaluation. It links thyroid, metabolic, reproductive, and barrier endpoints to EFSA’s 2019 guidance on combined exposure. BPA: bisphenol A; BPAF: bisphenol AF; BPF: bisphenol F; BPS: bisphenol S; DBP: dibutyl phthalate; DEHP: di(2-ethylhexyl) phthalate; DnBP: di-n-butyl phthalate; EDC: endocrine-disrupting chemicals; EFSA: European Food Safety Authority; ER/AR: estrogen receptor/androgen receptor; KC: key characteristics; MDAs: metabolism-disrupting agents; MNPs: micro- and nanoplastics; PCBs: polychlorinated biphenyls; PDL: Pathway Disruption Load; PE: polyethylene; PFAS: per- and polyfluoroalkyl substances; PP: polypropylene; PPAR: peroxisome proliferator-activated receptor; PS: polystyrene; TTR: transthyretin.
PFOS, PFOA, PFHxS, and shorter-chain replacement PFAS continue to be detected at low μg/kg or ng/L levels in targeted surveys of seafood, drinking water, eggs, and composite foods, mirroring the PFAS profile commonly observed in serum biomonitoring [3, 22, 26]. In non-occupational populations, diet and drinking water are the dominant routes of PFAS exposure [3, 27], making PFAS a suitable model for pathway-based assessment of food-chain mixtures.
PFAS are among the best-characterized contaminant groups for endocrine relevance because both mechanistic and epidemiologic data support thyroid-axis perturbation. Mechanistically, PFAS can bind thyroid-hormone transport proteins (e.g., transthyretin) and compete with T4 [28, 29], interfere with thyroid hormone synthesis via thyroid peroxidase (TPO) inhibition [29–31], and increase hepatic clearance through enzyme induction and enhanced glucuronidation/biliary excretion [29, 30]. Consistent with these mechanisms, Du et al. synthesized evidence linking PFAS mixtures with shifts in thyroid hormones across pregnant women, adolescents, and adults [32].
PFAS exposure in the general population occurs as mixtures. Populations are hardly ever single-contaminant cohorts of either PFOS or PFOA; most are mixed groups of PFOS, PFOA, PFHxS, PFNA, and occasionally of shorter-chain replacements [23]. Summarized cohorts reported low single-digit ng/mL median serum concentrations—similar to national biomonitoring levels—supporting relevance to general-population exposure [32, 33]. This is relevant to developmental windows: Adequate maternal thyroid hormone supply during pregnancy is critical for fetal brain development [25, 34], and maternal hypothyroxinemia has been associated with lower offspring cognitive scores and increased risk of ADHD in some cohorts [35]. Accordingly, even modest PFAS-associated shifts toward higher TSH and lower free T4 during early pregnancy may be clinically meaningful at the population level.
Similarly, recent mixture studies using BKMR or WQS have reported that adults—particularly women—with higher combined PFAS exposure are more likely to exhibit metabolic syndrome, central adiposity, and dyslipidemia [33], although some analyses (including all-sex models) report null or inverse associations. Such heterogeneity is common in endocrine outcomes and may reflect effect modification by sex, adiposity, and life stage. These patterns are more consistent with chronic, low-dose pathway perturbation than with metabolic inertness of PFAS.
The use of food-contact materials continues to be a viable cause of bisphenol and phthalate exposure despite restrictions imposed on BPA in certain products [20, 36]. BPA, BPS, BPF, and phthalate plasticizers in food simulants are still detected in migration tests of can linings, polycarbonate replacements [8, 20, 37], and some flexible packaging; these findings align with human biomonitoring trends in which BPA has declined while BPS/BPF detection has increased. This convergence of occurrence in food-contact settings and internal exposure supports joint consideration of these compounds as a class. Although BPS and BPF have substituted bisphenol A due to endocrine issues, the receptor-binding motif was not eliminated by structural replacement. A 2015 systematic review in the Environmental Health Perspectives by Rochester and Bolden [38] revealed that BPS and BPF bind to estrogen receptors ERα and ERβ, stimulate estrogen-responsive reporter systems, and in some instances are weak androgen receptor antagonists, with potencies comparable to BPA in some assays [39]. Subsequent studies also have found interactions of certain bisphenol analogs with thyroid hormone receptors, suggesting that nuclear-receptor interference in this family is not limited to the estrogen–androgen axis [37, 40]. The fact that the structure does not correspond to safety is straightforward: Phenolic rings and hydroxyl groups that cause BPA to be a good estradiol mimic are still present in BPS and BPF [41]; alteration of the bridging moiety may change kinetics and lipophilicity, without necessarily erasing the pharmacophore.
The action of phthalates is a complementary action, equally well-described. On exposure, high-molecular-weight phthalates like DEHP, DBP, BBzP, or DiNP are quickly hydrolyzed to monoesters, and these monoesters inhibit important steroidogenic enzymes, including 3β-hydroxysteroid dehydrogenase and 17β-hydroxysteroid dehydrogenase [42, 43]. They also repress the expression of steroidogenic acute regulatory (StAR) protein, which regulates the transport of cholesterol into the mitochondria, a rate-limiting step in the metabolism of steroid hormones [32, 44]. The human fetal testis is particularly susceptible during the androgen window (or gestational weeks 8–14), during which androgens define the distance between the sexes and masculinization of the reproductive tract [45]; disrupting androgen production at this stage has long-term effects. Several phthalates do the same steroidogenic pathway with varying strengths; that is just the type of thing where component-based, pathway-centered grouping is more realistic than treating each phthalate as an independent entity. In 2024, an adult literature review demonstrated that increased urinary phthalate metabolites are also linked to reduced serum testosterone in men, by about 5–15% across four levels of exposure, individually modest, but consistent with environmental disruption of endocrine systems [46].
MNPs are not as homogeneous as PFAS or bisphenols, which is why they should be described more anatomically. Food-production and food-packaging processes are now a recognized source, as the abrasion of food-processing equipment, cutting boards, and plastic wrapping may liberate micro-scale food particles into directly-consumable ready-to-eat food [47], and multiple recent surveys have reported polymer fragments in table salt, bottled water, and seafood that are meant to be consumed directly [48, 49]. Microplastics (1–5 μm) are retained in the gut lumen or taken up by the Peyer patches, where they can cause local inflammation and change barrier integrity primarily due to mechanical interactions, reactive oxygen species (ROS) generation, and cytokine release [50, 51]. Nanoplastics (less than 1 μm) are able to traverse epithelial barriers, be distributed in the circulation, and secondary organs [52]; animal experiments have shown distribution to the liver, spleen, and even the placenta [53]. Polymer type also matters. The surface chemistries, sorption properties, and (probably) inflammatory potential of PE, PVC, polystyrene (PS), and polypropylene (PP) differ, and the PS particles used in experimental studies are not necessarily representative of all food-relevant polymers.
The post-2024 NEJM article contamination debate is noteworthy in that it unveiled the point of the procedure most susceptible to compromise [9]. The polymers can be detected by pyrolysis-GC/MS, although laboratory air includes airborne plastic particles, surgical drapes, tubing, and gloves may release microplastics, and handling of samples may introduce particles unless processed in very clean conditions [54, 55]. The May 2024 letters pointed to procedural blanks that were required, polymer-specific controls, and clean-room conditions. However, the authors responded by using further controls, and most importantly, contamination should be random, not necessarily concentrated in the plaques of patients who subsequently developed poor clinical outcomes [9]. The fact that the clinical association went on despite these concerns makes the signal worthy of integration, and further refinement of methodology is still needed. Methodological uncertainty remains a key limitation in MNP detection because contamination control, procedural blanks, polymer-specific controls, and reporting of detection limits can materially influence measured tissue burdens and cross-study comparability [56]. Standardized clean-lab workflows and inter-laboratory comparisons are therefore essential for translating occurrence signals into interpretable exposure metrics.
In terms of mechanism, the two ways that MNPs can place stress on pathways are both applicable to PDL. Particle-induced pathway includes downregulation of tight junction proteins, including ZO-1 and occludin, ROS production and inflammasome activation, including NLRP3, resulting in a leakier gut and low-grade systemic inflammation [57]. The chemical-carrier pathway takes advantage of the hydrophobic surface of plastic particles [58], which may absorb PFAS, bisphenols, and polycyclic aromatic hydrocarbons in the environment or in the food-production chain. These adsorbed chemicals may be released on an acidic or surfactant-rich portion of the gastrointestinal tract, effectively delivering a focused burst of EDCs to the epithelium. Correspondingly, assuming particles can reach plaques as the NEJM study indicates, they can presumably reach or at least penetrate other tissues, and animal studies already demonstrate liver and placenta accumulation [9]. Both pathways contribute to the barrier-inflammation axis already strained by PFAS and endocrine-active plastics. These two mechanistic routes by which micro and nanoplastics damage the gut barrier and amplify endocrine-disrupting co-exposures are illustrated in Figure 2.
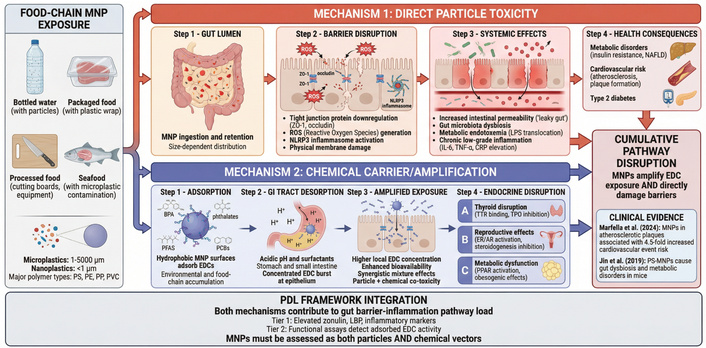
Micro- and nano plastics: dual pathway mechanisms. MNPs contribute to pathway disruption through two complementary mechanisms.
Mechanism 1 (direct particle toxicity): MNPs cause physical barrier disruption through tight junction downregulation (ZO-1, occludin), ROS generation, and NLRP3 inflammasome activation, leading to increased intestinal permeability, dysbiosis, and metabolic endotoxemia.
Mechanism 2 (chemical carrier/amplification): Hydrophobic MNP surfaces adsorb endocrine-disrupting chemicals (BPA, phthalates, PFAS) and release them in the gastrointestinal tract, amplifying EDC exposure and contributing to thyroid, reproductive, and metabolic disruption. Both mechanisms contribute to the gut barrier-inflammation component of PDL. Clinical evidence includes Marfella et al. (2024) showing MNPs in atherosclerotic plaques [9] and Jin et al. (2019) demonstrating gut dysbiosis and metabolic disorders in mice [59].
The importance of this convergence is that it involves three pathways: Thyroid-metabolic, nuclear receptor/steroidogenesis, and gut barrier-inflammation, which are all connected to the prevalence of common chronic diseases.
The thyroid-metabolic axis controls basal metabolic rate, lipid metabolism, and, during pregnancy, neurodevelopment of the fetus [60]. Maternal hypothyroxinemia (TSH above pregnancy-optimised ranges, free T4 at the lower end) has been linked in multiple cohorts with worse offspring cognitive scores and increased risk of ADHD [34]. Subclinical hypothyroidism in the case of adults (TSH 4-10 mIU/L and normal T4) is associated with dyslipidaemia and cardiovascular disease development [61]. Even environmentally chemical-induced, population-wide changes in TSH and free T4 of even minimal magnitude will thus shift the prevalence of metabolic syndrome in the wrong direction.
The steroidogenic and nuclear receptor impairment is directly applicable to male reproductive health [62], and it has been demonstrated that a decline in testosterone is linked to increased central adiposity, insulin resistance, and loss of bone density with age [63]. Anti-androgenic exposure during the womb, which reduces the length of the anogenital distance, is predictive of cryptorchidism, hypospadias, and perhaps reduced sperm counts in adulthood [64]. Bisphenol estrogenicity is of concern because of earlier puberty in girls and cancer sensitivity to hormones [36]; cause and effect are unconfirmed, but the mechanism is reasonable.
The disruption of gut barriers and low-grade inflammation is currently becoming a mainstream cause of non-alcoholic fatty liver disease, insulin resistance, and type 2 diabetes [65]. In these states, zonulin and LBP are increased; translocation of bacterial lipopolysaccharide through a permeable barrier results in the generation of metabolic endotoxaemia and a sustained increase in IL-6/CRP that increases cardiovascular risk [66]. When MNPs, together with emulsifiers, together with endocrine-active migrants of packaging weaken the barrier, they will increase the very process of these inflammation-metabolism interactions.
Technically, this would be two measurement layers.
In the case of the thyroid axis, free T4 is more informative than that of total T4 since only the unbound hormone is bioavailable and since chemicals that bind can alter total, but not the free. A TSH of between 0.4–4.0 mIU/L is termed normal, but there is persistence above, say, 2.5 mIU/L, which may signify subclinical pressure, particularly during pregnancy. Free T3 is an indicator of the peripheral deiodinase activity, which is subject to certain chemicals [67]. In steroidogenesis, precursor/product ratios are useful: A high ratio of androgens produced to testosterone may indicate 17β-HSD inhibition [68], and LC–MS/MS panels can measure multiple steroids simultaneously. To the gut barrier, zonulin is an indication of tight-junction control, LBP is the intestinal injury of bacterial products, and intestinal FABP2 is the injury of enterocytes [69]. These biomarkers are already present and measurable, with literature associating them with metabolic and liver disease.
Mammalian cell lines (e.g., HEK293) transfected with ER, AR, or TR and a luciferase reporter can be subjected to food extracts, water concentrates, or serum [70]. In the case of receptor agonists or antagonists in the sample, transcription is altered, and the light production is measured in 96-well plates. To further make these assays more realistic, they can include phthalates and other chemicals that require metabolic activation, and they can be spiked with a liver S9 fraction to simulate bioactivation, as would occur in vivo. This represents true endocrine activity as compared to the testing of parent compounds.
Tier 1 and Tier 2, together, inform us that the pathway of the person is in motion, and that the exposure matrix that the person is exposed to has pathway-active agents. That is the core of PDL. An operational schematic of how Tier 1 biomarkers and Tier 2 functional assays combine into a PDL score is shown in Figure 3.
Pathway Disruption Load (PDL) two-tier measurement architecture. Operational framework for assessing cumulative pathway-level disruption.
For each pathway p (thyroid; nuclear receptor/steroidogenesis; gut barrier–inflammation), PDL can be represented as: The following pseudo-equation is illustrative and not intended as a finalized scoring algorithm; the weights (w1, w2) are hypothetical placeholders that await empirical calibration from future mixture toxicology and cohort reanalysis studies.
PDLp = w1·Z(Tier-1 biomarker deviation)p + w2·A(Tier-2 functional activity)p
where Z(·) denotes standardized deviation within a reference population distribution (e.g., percentile or z-score) and A(·) summarizes net receptor/enzyme activity measured in relevant matrices (e.g., TR antagonism; ER/AR activity; TPO inhibition). In early implementations, Tier-1 and Tier-2 components should be reported side-by-side in an ordinal or percentile-based format (e.g., low/moderate/high relative to the reference cohort distribution) before any pathway-specific weighting (w1, w2) has been empirically calibrated. These weights are explicitly hypothetical placeholders at this stage; numerical PDL scoring is not supported by current datasets and should not be inferred from the formulation above.
Operationally, the workflow is:
(i) Define the pathway panel (Tier 1 biomarkers + Tier 2 assays), (ii) standardize Tier 1 values to population distributions, (iii) quantify Tier 2 net activity in relevant matrices, and (iv) integrate results into a pathway-level interpretation of relative load (e.g., low/moderate/high within-cohort distribution).
Tier 1 comprises pathway-specific biomarkers measured in human samples: thyroid axis (TSH, free T4, and free T3), steroidogenesis (testosterone, estradiol, DHEA-S, precursor/product ratios via LC-MS/MS), and gut barrier integrity (zonulin, LBP, intestinal FABP2). Tier 2 comprises functional receptor/enzyme assays applied to exposure matrices (food extracts, water concentrates, serum): receptor assays (ER, AR, TR agonist/antagonist activity), enzyme inhibition (TPO, 17β-HSD, aromatase), and total mixture activity capturing unknown co-migrants. Integration of Tier 1 biological response and Tier 2 functional burden yields a pathway-level PDL score (PDLp = w1·Z(Tier-1 deviation)p + w2·A(Tier-2 activity)p), classified as low, moderate, or high relative to reference population distributions.
PDL is intentionally positioned as a foodomics-relevant bridge between (i) food-matrix exposure signals and (ii) biological response signals in humans. In practical terms, Tier 2 functional assays can be applied to extracts of packaged foods, can linings, food-contact materials, and drinking-water concentrates to quantify integrated pathway activity (e.g., ER/AR/TR modulation or TPO inhibition), including unknown co-migrants that may be missed by targeted chemistry. Tier 1 then anchors these exposure-proxy signals to pathway movement in humans using biomonitoring/omics-compatible biomarkers (e.g., TSH–free T4 for thyroid; LC–MS/MS steroid panels for steroidogenesis; zonulin, LBP, and related permeability/inflammation markers for barrier circuits).
Operationally, a foodomics-informed PDL workflow can be implemented as: (i) characterize the food/exposure matrix using Tier 2 functional readouts; (ii) measure Tier 1 pathway biomarkers in cohort samples (or re-analyze existing cohorts with banked biospecimens); and (iii) integrate both layers into pathway-specific load distributions within the population (e.g., low/moderate/high relative burden). This approach makes it possible to relate food-system exposures (dietary patterns, packaging choice, and water source) to measurable pathway-level biological perturbations without requiring complete chemical identification of all contributors.
PDL can be conceptualized as a composite load on a route, and not a single definitive number. The comparison is cardiovascular risk scoring: Several moderately abnormal inputs are added together to create a level of concern. In this case, various mildly pathological endocrine or barrier signals are added to a pathway load.
Illustrative example (hypothetical): An individual in a preconception/pregnancy cohort shows persistently high-normal TSH with low-normal free T4 (Tier 1), alongside detectable PFAS and bisphenol analogues in biomonitoring, and measurable TR antagonism in a packaged-food extract or drinking-water concentrate using a reporter assay (Tier 2). In a PDL framing, the aligned Tier-1 axis movement and Tier-2 functional burden would indicate elevated thyroid-PDL relative to the reference distribution, even if no single chemical exceeds its health-based guidance value.
At the theoretical level, PDL combines the deviations of Tier 1 biomarkers (e.g., TSH shifting up, free T4 in the low-normal range, zonulin increasing, and LBP increasing) with positive Tier 2 biomarker signals (e.g., TR antagonism, ER agonism in food extracts). This then leads to the question of whether this is a pathway that is experiencing more stress than is normal for this population. A more practical answer to that is to make use of population distributions: In the event that thyroid-axis PDL components put an individual systematically above the 75th or 90th percentile, this can motivate closer characterization of food-matrix exposure sources and targeted risk-communication within research, surveillance, or clinical prevention settings.
Personal differences should be considered: genetic polymorphism in metabolism, life stage (pregnancy, puberty), baseline disease (pre-existing thyroid nodules, Hashimoto’s), sex, and adiposity all vary in the manner in which a particular exposure profile is translated into pathway movement. This is why PDL must be based on real population distributions, and not expert-determined weights. It further describes the reason behind why single-chemical assessment would frequently report all clear when PDL would report that the thyroid axis is under cumulative stress: PFOS 8 ng/mL + BPS 1–2 ng/mL + DEHP metabolites in the upper quartile + TSH 3.8 mIU/L + free T4 at low-normal + 15% TR antagonism in food extracts is not identical to each exposure below its limit.
What is unclear is the best way to weight each part and the way to deal with interactions. Dose addition is a reasonable default until mixture studies, at realistic doses, are published, since that is the case with several groups of pesticides already of cumulative risk. But a portion of the PDL research program is to operate the binary and ternary mixtures, which will inform us when we should start to deviate from that default.
At present, PDL is proposed as a conceptual and research framework rather than a regulatory-ready metric; translation into policy would require calibration studies, reference distributions, and harmonized Tier-2 assay validation.
PDL is proposed as a pathway-centered interpretive framework, and several uncertainties should be acknowledged. First, mixture toxicology at human-relevant doses is not fully characterized: Dose addition is a pragmatic default, but interaction patterns (additivity, synergy, or antagonism) may differ across pathways and life stages. Second, Tier-1 biomarkers vary with sex, adiposity, pregnancy, puberty, and baseline disease, so small shifts require interpretation against appropriate population distributions and clinical context. Third, food matrices are chemically complex and temporally variable; unknown co-migrants and fluctuating diets can contribute to exposure misclassification, which is a central reason for incorporating Tier-2 functional assays. Fourth, MNP measurement and functional bioassays are sensitive to laboratory method variability, including detection limits and contamination control, which can limit cross-study comparability without standardized blanks, reporting, and inter-laboratory harmonization. These limitations do not negate the utility of PDL; rather, they define priorities for calibration studies, standardized methods, and cohort-based reanalyses that can empirically refine pathway panels and weighting.
Multiple cohorts in existence are suitable for reanalysis in the PDL style. The Norwegian Mother, Father and Child Cohort (MoBa) contains more than 100,000 banked pregnancy samples; many of them already have PFAS and phthalate data. By including thyroid and gut-barrier markers, we would be able to determine whether cumulative exposure is reflected in pathway movement during pregnancy, the most sensitive window [71]. The European HBM4EU project has standardized biomonitoring between various nations; the retrospective measurement of zonulin, LBP, and sex steroids on such samples would provide a cross-country perspective of the pathway stress. In the U.S., NHANES cycles, which now already include a huge amount of chemical biomonitoring, might include even a partial panel of pathway biomarkers in a sub-sample to determine national PDL distributions.
The PFOA + BPS, PFOA + DEHP, BPS + DEHP, and a ternary mixture of PFOA + BPS + DEHP at low (25th percentile), medium (50th), and high (75th) human-equivalent doses can be used as the basis of a mixture toxicology. The mouse models were developed that were able to read out levels of thyroid hormones in dams and pups, anogenital distance, gut permeability signatures, and liver histology. This would require 3 to 5 years to fully set up these studies, but would have a direct impact on PDL weighting. Harmonization of the MNP method inter-laboratory comparison with clean-room processing and standardized blanks should be a 2–3 year goal.
The present-day approval procedure of new food-contact compounds typically uses a logic of migration-exposure-threshold-of-concern. What is lacking is an endocrine or thyroid pathway activity check on the migrated material. A process that is aware of PDL could screen Tier 2 (ER/AR/TR, TPO inhibition) on the migrated extract. When it happens that it is negative, the approval is made as it is. A second-tier 28-day study using the pathway biomarkers (TSH, free T4, testosterone, gut-barrier markers) might be a possibility in case it is positive. In case such a study establishes pathway movement, the applicant might be asked to show that the material would not impose any significant additional burden on the concerned pathway, as compared to typical co-exposures (PFAS, bisphenols and phthalates). This is similar to the reasoning of data requirements stacking up with tonnage in REACH; in this case, it is the activity pathway of functional activity that can become accumulable. This would inform market-basket surveillance when packaged foods consistently elicit positive endocrine responses in reporter assays, regulators may track down the source material and may consider requesting reformulation.
The majority of what PDL needs is already in the standard laboratory menu; TSH and free T4 are common and cheap. LC–MS/MS sex steroid panels are becoming more accessible. PFAS, bisphenol, and phthalate panels are offered in specialized and some commercial labs, but this is cost- and insurance-limited. The only thing lacking is decision support that can take inputs such as upper-normal TSH, low-normal free T4, elevated PFAS, detectable BPS, and higher phthalate metabolites, and return a pathway-level interpretation (e.g., higher thyroid-axis disruption load), particularly for sensitive windows such as preconception and pregnancy. This could be incorporated into preconception counseling, antenatal visits, and endocrinology follow-up as a cumulative-exposure interpretation layer rather than as a diagnostic label. Although reversal at the individual level might be uncertain, at the population level, risk communication on feasible exposure-source modifications (e.g., drinking-water and food-contact pathways) may be inexpensive and consistent with the literature on developmental origins.
Practical interpretation can be structured as a simple sequence: (i) identify the pathway of concern (thyroid; steroidogenic/nuclear receptor; gut barrier–inflammation), (ii) review Tier-1 biomarkers relative to life-stage appropriate distributions, (iii) evaluate Tier-2 net activity in relevant food/water/packaging matrices when available, and (iv) integrate both layers as a pathway-level load signal to guide follow-up in research, surveillance, or preventive counseling contexts. In this way, “pathway load” functions as decision support for cumulative exposure patterns rather than as a diagnostic label.
MNPs require dose-response information in humans: What tissue burden causes measurable dysfunction of barrier function or systemic inflammation? Effects that are specific to polymers should be explained: Is PVC more inflammatory than PE, does PS leach more biologically active monomer, and do surface additives alter inflammatory potential? The clearance kinetics (lifelong particle accumulation or clearance or hepatobiliary and renal clearance) have not been adequately investigated.
Mixture effects must be mapped: Are PFAS-bisphenol mixtures additive, or do PFAS-bisphenol mixtures have more-than-additive TR or TPO effects? Do MNPs indirectly potentiate endocrine-disruptor action with a larger gut permeability and subsequent systemic absorption of the co-ingested EDCs? Do they encounter any antagonisms, e.g., induction of hepatic clearance of one chemical by another?
Vulnerability during life stages ought to be characterized in terms of PDL: The endocrine baselines during infancy, puberty, pregnancy, and aging are all different, and pathway loads cannot be simply compared across them. PFAS have been implicated in diminished vaccine response in addition to endocrine and barrier pathways, and some bisphenols have been found to have neuroactive effects; the question remains whether these are independent pathways of action or downstream of the described pathways.
Exposure of humans to new food-related contaminants is overlapping, chronic, and endocrine-mediated. PFAS binding to transport proteins triggering hormone clearance, bisphenol and phthalate substitutes retaining receptor-activity, MNPs disrupting gut barrier or adsorbing EDCs, all lead to three central pathways of metabolic, reproductive, and cardiovascular health. Experiments (e.g., Jin et al. on microplastics and gut barrier [59]), human meta-analyses (Du et al. [32] and subsequent PFAS-thyroid analyses), clinical observations (Marfella et al. [9] on MNPs in plaques), and consensus papers on the mechanisms all indicate the same direction.
Three take home messages: First, real-world food-chain exposure is pathway-convergent: PFAS, bisphenol/phthalate analogues, and MNPs independently and collectively stress the thyroid-metabolic axis, nuclear receptor and steroidogenic signaling, and gut barrier-inflammation circuits—the same pathways linked to prevalent chronic diseases.
Second, PDL offers a biologically coherent integration layer: By combining pathway-specific biomarkers (Tier 1) with functional bioassay outputs from relevant matrices (Tier 2), PDL translates chemical-agnostic mixture activity into interpretable pathway-level signals that neither single-substance assessment nor purely statistical mixture methods currently provide.
Third, foodomics and functional assays enable mixture-aware surveillance: Tier 2 assays applied to food extracts, packaging migrants, and drinking-water concentrates can capture total endocrine activity-including unknown co-migrants and link food-system exposures to measurable biological perturbations, supporting more effective and sustainable food safety decision-making.
BPF: bisphenol F
BPS: bisphenol S
MNPs: micro- and nanoplastics
PDL: Pathway Disruption Load
PE: polyethylene
PFAS: per- and polyfluoroalkyl substances
PP: polypropylene
PS: polystyrene
PVC: polyvinyl chloride
ROS: reactive oxygen species
StAR: steroidogenic acute regulatory protein
TPO: thyroid peroxidase
AJA: Conceptualization, Methodology, Investigation, Writing—original draft, Writing—review & editing, Visualization, Project administration, Supervision. TAK: Investigation, Writing—review & editing. OOA: Investigation, Writing—review & editing, Validation. IAO: Investigation, Writing—review & editing. AOA: Writing—review & editing, Supervision, Validation. All authors read and approved the final manuscript.
The authors declare no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
No specific funding was received for this work.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 626
Download: 24
Times Cited: 0
Olga Pardo, Francesc A. Esteve-Turrillas
Clara Ochoa-Esteso ... María Jesús Lerma-García
Daniel Gallart-Mateu
Gabriel Mustatea ... Elena L. Ungureanu
Serkan SUGEÇTİ
Andrea Monsalve-Vidal, Daniel Gallart-Mateu
Paula Ponz-Perelló ... David Pérez-Guaita
