 Review
Review

Affiliation:
1Department of Pharmaceutics, Shree Naranjibhai Lalbhai Patel College of Pharmacy, Umrakh 394345, Gujarat, India
Email: Yashdudhwala70@gmail.com
ORCID: https://orcid.org/0009-0006-6043-5665
Affiliation:
2Department of Pharmaceutics, Dr. Dayaram Patel Pharmacy College, Bardoli 394601, Gujarat, India
3Centre for Research Impact & Outcome, Chitkara College of Pharmacy, Chitkara University, Rajpura 140401, Punjab, India
Email: dev7200@gmail.com; deveshkapoor@dppc.ac.in
ORCID: https://orcid.org/0000-0003-4085-8936
Affiliation:
1Department of Pharmaceutics, Shree Naranjibhai Lalbhai Patel College of Pharmacy, Umrakh 394345, Gujarat, India
ORCID: https://orcid.org/0009-0002-3165-4608
Affiliation:
4Department of Quality Assurance, Shree Naranjibhai Lalbhai Patel College of Pharmacy, Umrakh 394345, Gujarat, India
Affiliation:
4Department of Quality Assurance, Shree Naranjibhai Lalbhai Patel College of Pharmacy, Umrakh 394345, Gujarat, India
ORCID: https://orcid.org/0009-0006-0973-2330
Explor Drug Sci. 2026;4:1008165 DOI: https://doi.org/10.37349/eds.2026.1008165
Received: April 13, 2026 Accepted: May 12, 2026 Published: July 06, 2026
Academic Editor: Zhengwei Huang, Jinan University, China
The article belongs to the special issue Nanoformulations for Non-Intravenous Drug Delivery
Schizophrenia affects approximately 24 million people worldwide, representing 0.3–0.7% of the global population, and remains a leading cause of years lived with disability. The disorder contributes to over 13 million disability-adjusted life years, underscoring its substantial global health and socioeconomic burden. This review critically examines the convergence of artificial intelligence (AI) and advanced oral drug delivery systems as an emerging strategy in schizophrenia management. Conventional diagnostic frameworks, reliant on subjective symptom assessment, often result in delayed or inaccurate diagnosis, while standard oral antipsychotics are limited by poor bioavailability, extensive first-pass metabolism, and inadequate brain targeting. Recent advances in AI, including natural language processing (NLP), neuroimaging analytics, electrophysiological modeling, and multi-omics integration, support diagnostic classification, risk prediction, symptom monitoring, and patient stratification. Simultaneously, nanotechnology-driven oral delivery platforms such as lipid nanoparticles, dendrimers, and proliposomes enhance pharmacokinetics, central nervous system targeting, and therapeutic adherence. The integration of AI with pharmacogenomics, wearable monitoring, and digital twin models further facilitates real-time dose optimization and personalized therapy. Despite promising preclinical and clinical outcomes, challenges related to data privacy, algorithmic bias, scalability, and regulatory translation persist. This review highlights a shift toward precision psychiatry, where AI-enabled diagnostics and smart oral therapeutics may support predictive, personalized, and adaptive care in schizophrenia.
Schizophrenia is a chronic and debilitating neuropsychiatric disorder that affects approximately 1% of the global population. It shows a relatively consistent lifetime prevalence across different geographic and cultural settings. The World Health Organization (WHO) notes that schizophrenia is a condition that causes more than 13 million disability-adjusted life years (DALYs) in the world, as it severely affects the functioning of individuals and the general health of the population [1]. Schizophrenia, which usually develops in late adolescence or in early adulthood, is characterized by a complex of positive (hallucinations, delusions), negative (avolition, social withdrawal), and cognitive symptoms. All these symptoms contribute to the occupational, interpersonal, and self-care impairment, which in most cases leads to lifelong reliance and socioeconomic marginalization [1, 2].
Despite advances in psychiatric diagnosis and pharmacotherapy, schizophrenia management remains largely reactive and often lacks sufficient precision. Existing diagnostic approaches, including the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and the International Classification of Diseases, 11th Revision (ICD-11), rely heavily on clinical observation and self-reported symptoms, which introduces subjectivity. Such frameworks neglect to identify the disorder at its prodromal stage, where it could have the greatest influence. Hence, diagnostic uncertainty is not uncommon during the initial phase of psychosis. Diagnostic misidentification and diagnostic switch are more pertinent in the context of first-episode psychosis and high clinical risk groups, where the symptoms of schizophrenia spectrum disorder can be confused with bipolar disorder with psychotic features, major depressive disorder with psychotic features, brief psychotic disorder, psychosis induced by substance abuse, among others. In such populations undergoing initial diagnosis, diagnostic inconsistency has been seen in many patients, with certain studies suggesting a diagnostic switch in one-third of patients. As such, diagnostic uncertainty is quite prevalent in early psychosis, especially in first-episode and clinical high risk (CHR) samples, due to symptom overlap with affective, substance-induced, and other psychotic conditions that can cause a diagnostic change. As such, any diagnostic error or inconsistency prevalence must be taken into account in relation to early psychosis groups, not as a general misdiagnosis rate for established schizophrenia [3].
In addition, the current tools have minimal predictive value in the areas of disease progression, treatment responsiveness, or risk of relapse, which are critical variables in individual intervention planning.
Conventionally, oral antipsychotic drugs have been impeded on the therapeutic side due to their low aqueous solubility, massive first-pass hepatic metabolism and lack of specific distribution. Such constraints lower efficacy and augment adverse effects prevalence, which partakes in low adherence and withdrawal of treatment. The metabolic syndrome, extrapyramidal symptoms, and cognitive dulling are frequently associated with long-term antipsychotic use and pose a significant threat to quality of life and overall outcomes [4].
Recent developments in artificial intelligence (AI) have the potential to substantially improve diagnostic and therapeutic decision-making. Machine learning (ML), natural language processing (NLP), and deep neural network-based AI tools are increasingly being explored for diagnostic classification, psychosis-risk prediction, relapse monitoring, treatment-response prediction, and patient stratification. These approaches analyze diverse data types, including speech and language patterns, structural and functional neuroimaging, electroencephalography (EEG), behavioral data, electronic health records (EHRs), pharmacogenomic profiles, and multi-omics datasets [5].
At the same time, the pharmacokinetic bottlenecks are being mitigated through the use of novel approaches to oral drug delivery, especially nanocarrier-based systems, which allow site-targeted drug delivery, enhanced mucosal absorption and reduced systemic exposure [6, 7]. The intersection of these fields, AI and smart therapeutics, provides a roadmap to precision psychiatry, in which diagnosis and treatment are dynamically modified to the changing clinical profile of a patient.
This review examines recent advances published between 2020 and 2025 in AI-assisted schizophrenia diagnostics and advanced oral drug delivery systems. It highlights the synergistic opportunities of these areas, critically reviews their translational preparedness, and defines the implementation challenges such as information integration, regulatory barriers, and ethical protections. The next section begins by providing a summary of the existing diagnostic standards and the limitations linked to them, which preconditions the AI-driven change in the area of psychiatric care [8].
The clinical diagnosis of schizophrenia is primarily based on the DSM-5, and the ICD-11. The two models are based on the existence and duration of typical symptoms, which include hallucinations, delusions, disorganized speech or behavior, and negative symptoms such as emotional flattening or avolition, and high-level functional impairment [9]. The DSM-5 states that the diagnosis must include two or more of these symptoms lasting at least one month, with persistent signs of disturbance for at least six months, as defined by the American Psychiatric Association (APA). Similarly, ICD-11 describes schizophrenia based on persistent psychotic symptoms over time while emphasizing that symptom assessment should be interpreted within the individual’s cultural and clinical context [10].
Although these criteria provide a standardized psychiatric classification framework, their symptom-oriented nature introduces subjectivity and may contribute to inter-rater variability and diagnostic inconsistency, particularly during prodromal or early-stage presentations. A meta-analysis study found that diagnostic concordance rates in first-episode psychosis can range from 60–70 percent between clinicians, mainly because of similarity with other neuropsychiatric disorders including bipolar disorder, schizophrenic disorder, and major depression with psychotic characteristics [3].
Moreover, currently, no validated biological or molecular markers of schizophrenia are used in diagnostic lists. This lack of objective tools helps to further prolong the diagnosis process, which usually takes one to three years since the onset of the symptoms, a critical period in which early intervention may significantly benefit the outcome at the end of the process [3]. Adding to this problem is the fact that there is also a phenomenon known as diagnostic migration where initial clinical diagnosis of the patient changes dramatically with time, usually because of the varying progression of symptoms and developing cognitive or functional impairments [11].
The issue goes beyond initial diagnosis to forecast progression and response to treatment of the disease. Although antipsychotic treatment is effective in positive symptoms among most patients, the effect of antipsychotics on negative symptoms and cognitive impairments is inconsistent. However, the existing diagnostic methods do not give much predictive information on treatment pathways, probability of response or risk of relapse, which are imperative to plan patient care at the individual level [12].
The inability to convert the neuroimaging, electrophysiological, and genomic findings into the clinical instruments is a major bottleneck as the research in these fields evolves. Neurobiological investigations like the ENIGMA Schizophrenia Consortium have repeatedly reported structural and functional brain dysfunctions like hippocampal volume and dysregulated prefrontal connections with the condition [13]. Nevertheless, the translation of such findings into diagnostic utility has remained elusive, in part because of the complexity and high dimensionality of such data, and the absence of powerful analytical frameworks that can be used to produce useful insights [14].
The diagnostic gap identified by this diagnostic opacity demonstrates a severe weakness within the existing work of psychiatry: the necessity of instruments with predictive capabilities, objectivity, and scalability. AI presents a very promising opportunity to solve this deficiency. Through the use of ML algorithms to predict and process complex multimodal data such as neuroimaging, voice records, genetic profiles, and behavioral markers AI can help to create measurable and personalized diagnostic signatures. These improvements have the potential to reduce the untreated psychosis (DUP) period, better stratify risk, and assist in the setting of the individualized therapy approach at its very beginning [15].
Contemporary developments in AI have substantially expanded the field of psychiatric diagnostics. Schizophrenia is a complex and heterogeneous disorder of cognitive, behavioral, and neurobiological functions that is an interesting opportunity for AI-enabled precision medicine [16]. The increased access to multi-modal data, including speech, neuroimaging, electrophysiology, and omics, has enabled data-driven insights that extend beyond conventional clinical models and existing diagnostic paradigms [17]. In this section, the four main areas in which AI is transforming the diagnostics of schizophrenia have been critically examined and they are NLP, neuroimaging analysis, electrophysiological modeling, and multi-omics integration [18]. Figure 1 describes the multi-modal AI workflow in order to visualize the structure of the integrated diagnostic tools. It shows how NLP, neuroimaging, electrophysiological modeling, and multi-omics data can be united in ML models to improve the detection and stratification of schizophrenia in the early phases of the disorder.
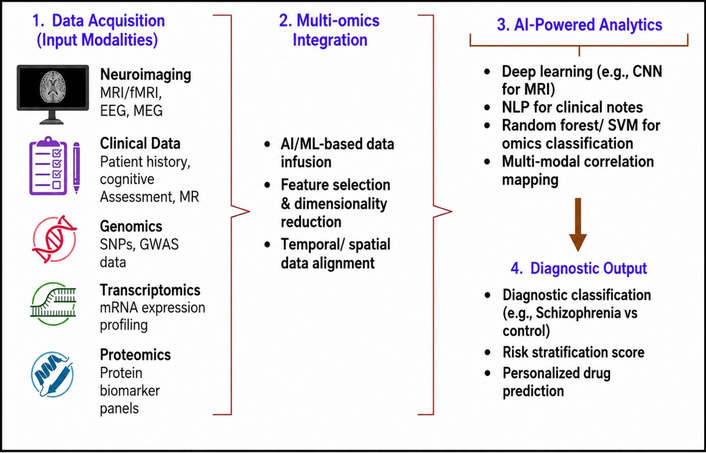
Multi-modal AI diagnostic workflow including multi-omics integration. AI: artificial intelligence; CNN: convolutional neural network; EEG: electroencephalography; fMRI: functional magnetic resonance imaging; GWAS: genome-wide association studies; MEG: magnetoencephalography; ML: machine learning; MR: magnetic resonance; MRI: magnetic resonance imaging; NLP: natural language processing; SNPs: single nucleotide polymorphisms; SVM: support vector machine.
While AI-based diagnostic paradigms have shown great potential, there is variability in terms of their clinical utility depending on the type of data. NLP-based paradigms are relatively easy to scale and cost-efficient since vocal recordings can be done remotely. However, there are limitations to their reliability, such as language, culture, education, and transcription quality. Neuroimaging-based paradigms provide extensive biological insights and detect structural and functional deviations that can lead to schizophrenia. Nevertheless, they are limited in widespread clinical application due to financial constraints, limited scanner access, data standardization, and external validity [13]. EEG and magnetoencephalography (MEG)-based paradigms are more mobile and time-sensitive, but signal noise and reproducibility of biomarkers need to be addressed. Finally, multi-omics models help understand heterogeneous pathophysiology and drug response in patients but rely heavily on annotated data and are not easily implementable in psychiatric practice. Thus, the most clinically useful strategy might not involve any single AI technology but rather multimodal AI models with careful validation and implementation [15].
Psychotic symptoms such as disorganized thought and speech disturbances manifest at a pre-psychotic stage and can be taken as the early signs of schizophrenia. Traditional measures are biased and liable to inter-rater reliability. NLP is a computationally scalable analytical approach to linguistic output, which is objective. Recent NLP-based studies suggest that linguistic features, including semantic coherence, syntactic complexity, speech fluency, pause patterns, and reduced semantic connectedness, may help identify schizophrenia-related speech disturbances and support objective assessment of thought disorder. However, much of the current evidence is derived from retrospective or exploratory datasets, and prospective validation is still required before NLP tools can be considered reliable for preclinical or early diagnostic use [19]. For example, NLP-based semantic analysis of transcribed interviews has been used to identify schizophrenia-related linguistic features and distinguish patients from healthy controls, demonstrating the potential of language-based biomarkers for clinical assessment [19, 20]. On the same note, deep learning-based NLP models have been applied to analyze speech and text data for identifying language patterns associated with mental health conditions. These findings highlight the potential of NLP tools to support AI-assisted psychiatric assessment and early identification when integrated with digital health technologies [21].
In addition to semantics, acoustic and prosodic elements, including pitch modulation, pause length, and speaking rate, are other diagnostic indicators. Neural networks to analyse the temporal structure of speech, where non-verbal correlates of thought disorder can be identified even in participants who do not have overt delusions and hallucinations. Their model has found that the atypical acoustic signatures were detected in 67 percent of CHR persons who developed schizophrenia. These findings are in line with converging semantic and acoustic NLP as an effective early warning system [22]. There is also the upcoming trend of cross-linguistic adaptability becoming a priority. Transformer-based models with multiple languages had the potential to be generalized on Danish and Dutch corpora and performed better than human raters in predicting the severity of symptoms [21]. Apps such as Winterlight Labs are currently able to provide passive, app-based speech-monitoring, so that clinicians can have high-frequency behavioral data in an unobtrusive way to signal clinical deterioration.
Neuroimaging studies have consistently identified structural and functional abnormalities in schizophrenia; however, their clinical diagnostic application remains limited by interpretive complexity and high data dimensionality. AI [and, specifically, the convolutional neural network (CNN) and graph neural networks] is now able to derive high-value features of structural and functional imaging data with progressively greater accuracy. Deep learning, particularly CNNs, has demonstrated promising performance in MRI-based schizophrenia classification by identifying disease-associated structural brain alterations, including abnormalities in the hippocampus, thalamus, and prefrontal cortex [23].
Resting-state functional MRI (fMRI) studies have also indicated altered network connectivity in schizophrenia. Recurrent neural networks have been used to model time-series fMRI patterns for predicting CHR conversion, with an area under the curve (AUC) of over 0.90. Biomarkers with high temporal resolution are provided by EEG and MEG. EEG-based deep learning can reliably detect event-related potential (ERP) abnormalities, such as P300, mismatch negativity, and gamma-band oscillations associated with working memory dysfunction [24].
Disrupted network topology in schizophrenia has been discovered in graph-based models of the whole-brain connectomes using fMRI and diffusion tensor imaging (DTI). Graph convolutional networks to structural-functional matrices, with 91% diagnostic accuracy in early-onset schizophrenia, and the revelation of perturbed executive subnetwork hubs. Further improvements have been made through multi-view learning, which is a type of learning that involves the combination of several imaging modalities. A stay-at-attention-fusion framework integrating sMRI, fMRI, and DTI features achieved an AUC of 0.93 for differentiating prodromal subjects from controls [25]. Longitudinal neuroimaging is also becoming popular. CNNs that learn using baseline fMRI scan data of the NAPLS-3 cohort forecasted the development of symptoms in CHR individuals within a 12-month timeframe with 76 percent accuracy, suggesting the possibilities of imaging-based dynamic risk models.
Electrophysiological biomarkers are cost-efficient and portable methods of diagnostic refinement. Support vector machines (SVMs) and deep autoencoders are only some examples of ML models that are enhancing the fineness and usability of EEG and MEG data interpretation. The time-frequency EEG feature SVMs are classification accuracy of over 85% [26]. Fingerprints of functional and electrophysiological connectivity to create personalized networks and improve the sphere of precision diagnostics [27].
Recent work has focused on nonlinear aspects of EEG features such as spectral entropy, fractal dimension, and signal complexity. Autoencoders trained on these latent features have achieved diagnostic accuracies exceeding 87% for schizophrenia subtype classification [28]. These models were more effective than ERP-based classifiers in identifying resting-state abnormalities that are difficult to detect using conventional averaging methods. AI-based analysis of electrophysiological signals has also demonstrated potential for identifying brain activity patterns and supporting objective neurophysiological assessment, although further validation is required [29].
The real-time data capture in outpatient settings is being made possible by the increasing accessibility of mobile EEG systems such as the one offered by Cognionics and Emotiv, combined with the go-anywhere deployable AI algorithms. Continuous monitoring is the first area that these systems are being experimented with to reduce diagnostic latency and enhance longitudinal symptom monitoring.
Polygenic schizophrenia, as indicated by genome-wide association studies (GWAS) and polygenic risk score (PRS) has not produced clinical tools with any strength because of low effect sizes and absence of integrative modeling. Multi-layered biological data can be synthesized through AI in an encouraging perspective. The combination of genomic, transcriptomic, proteomic, metabolomic, and epigenomic data into unified predictive models is now a possibility [30].
ML to combine genomic and proteomic signatures to predict psychosis in those with an increased risk, with more than 80 per cent accuracy. Efforts such as PsychENCODE and UK Biobank are establishing powerful neurogenetic repositories in order to be used in the training of such models. Biological interpretability of computational predictions is currently facilitated by explainable AI (XAI) schemes [31].
There are also schizophrenia subtypes that have been revealed by unsupervised ML. Variational autoencoders of methylomic and proteomic data have revealed three subgroups with synaptic or inflammatory dysregulation, with each having distinctive treatment response patterns. Such early endophenotypes would be able to guide the intervention approaches and subsequent drug development pipelines [32].
Table 1 provides a summary of diagnostic performance of different AI techniques. This comparative overview has pointed out the advantages and disadvantages of both techniques, and this supports the argument that hybrid models that integrate multimodal insights can be used to enhance clinical decision-making. Multi-omics models are becoming a driving force in the treatment decisions. Trained miRNA-plasma proteomics-gut microbiome ensemble AI predictive of risperidone responsiveness in first-episode patients, with 79% balanced accuracy. These tools have the potential to improve pharmacotherapy selection and move treatment beyond the conventional trial-and-error approach. Collaborative multi-omics datasets in schizophrenia, including open-source initiatives such as SCHEMA, are expanding and may support the development of AI-based diagnostic models for future real-world regulatory evaluation [33].
Reported diagnostic performance of selected AI-based approaches in SZ-related studies.
| AI technique | Input data & feature type | Diagnostic task | Performance | Reference | AI technique |
|---|---|---|---|---|---|
| CNN on EEG spectrogram images | Multichannel EEG → spectrogram conversion | SZ vs. healthy control | 98% accuracy | [34] | CNN on EEG spectrogram images |
| CNN-LSTM on EEG signals | Raw EEG via CNN-LSTM architecture | SZ diagnosis | 99.25% accuracy | [33] | CNN-LSTM on EEG signals |
| Lightweight 3D-CNN + ensemble on structural MRI | T1-weighted 3D MRI volumes | SZ vs. control | 92.22% accuracy | [35] | Lightweight 3D-CNN + ensemble on structural MRI |
| 2D- & 3D-CNN on diffusion + structural MRI | sMRI + DTI, pre-trained and scratch CNNs | Classification | ~90–95% (AUC ~0.90) | [36] | 2D- & 3D-CNN on diffusion + structural MRI |
Note: the performance values summarized in this table are study-reported outcomes and should not be interpreted as directly comparable across modalities. The included studies differ in sample size, data type, diagnostic task, preprocessing method, model architecture, validation strategy, and outcome metric. Therefore, the table is intended to provide an overview of reported AI applications rather than a ranking of EEG-, MRI-, ERP-, or multimodal approaches. AI: artificial intelligence; AUC: area under the curve; CNN: convolutional neural network; DTI: diffusion tensor imaging; EEG: electroencephalography; ERP: event-related potential; LSTM: long short-term memory; MRI: magnetic resonance imaging; SZ: schizophrenia.
Even though oral antipsychotics continue to be the main modality of schizophrenia treatment, traditional preparations have numerous pharmacological and clinical deficiencies that compromise success in the long-term treatment of the condition [37]. These constraints are multifactorial- they include issues with pharmacokinetics, central nervous system (CNS) targeting, patient compliance as well as systemic side effects. These limitations highlight the need for more intelligent, flexible, and patient-centered oral drug delivery approaches [37, 38].
Limitations of traditional oral antipsychotics are not applicable to all medicines; rather, they vary depending on physicochemical and pharmacokinetic properties of each medicine. Second-generation antipsychotics, including risperidone, olanzapine, and quetiapine, show differences in aqueous solubility, first-pass metabolism, cytochrome P450 (CYP) enzyme-mediated metabolic pathways, oral bioavailability, and efflux mechanisms involving P-glycoprotein (P-gp). Such differences affect pharmacokinetics of the drugs, which determines the efficiency of therapy, dosing schedule, variations in efficacy, and possibility of interactions. Hence, a comparative analysis of drugs can be valuable in order to determine what kind of pharmacokinetic obstacles can be resolved using nanoformulation and AI.
The drug-specific pharmacokinetic limitations of representative oral antipsychotics are summarized in Table 2, emphasizing solubility, first-pass metabolism, CYP pathways, oral bioavailability, and P-gp-related barriers. It becomes evident from this analysis that the requirement for an advanced formulation system for oral delivery depends on the characteristics of each drug. For risperidone, the two major obstacles to overcome besides systemic absorption are the CYP2D6 variability and the P-gp effect on its entry into the brain. Olanzapine’s insufficient water solubility and extensive first-pass metabolism in the liver call for the application of lipid-based, amorphous, and nanosized formulations to improve solubility and eliminate pharmacokinetic variability. The extremely low bioavailability due to extensive CYP3A4 metabolism is a major argument in favor of advanced delivery for quetiapine. This also affects the complexity of the implementation of AI approaches. If the parameters of a drug formulation are defined, including the particle size, the rate of dissolution, and entrapment efficiency, the drug is a good fit for AI optimization. When transporter activity, genotype, and brain entry are considered, the data are more complex.
Comparative pharmacokinetic limitations of representative oral antipsychotic drugs.
| Drug | Solubility/BCS profile | First-pass metabolism | Major CYP metabolic pathway | Approximate oral bioavailability | P-gp substrate characteristics | Formulation relevance |
|---|---|---|---|---|---|---|
| Risperidone | Poor aqueous solubility; commonly classified as BCS class II | Moderate hepatic first-pass metabolism | Mainly CYP2D6; minor contribution from CYP3A4 | Approximately 70% | Risperidone and 9-hydroxyrisperidone interact with P-gp, which may limit brain exposure | Solubility enhancement, controlled release, and transporter-aware brain delivery may improve consistency of exposure |
| Olanzapine | Poor aqueous solubility; BCS class II drug with high permeability | Extensive hepatic metabolism and first-pass effect | Mainly CYP1A2; minor CYP2D6 contribution; glucuronidation also involved | Approximately 60% | Evidence suggests P-gp can limit brain penetration of olanzapine | Lipid-based and solubility-enhancing systems may improve dissolution and reduce exposure variability |
| Quetiapine | Low aqueous solubility at intestinal pH; BCS class II behavior | Extensive hepatic first-pass metabolism | Mainly CYP3A4 | Approximately 9% | Reported as a P-gp substrate; transporter involvement may influence CNS disposition | Oral bioavailability enhancement, lymphatic transport, and sustained-release systems are particularly relevant |
BCS: Biopharmaceutics Classification System; CNS: central nervous system; CYP: cytochrome P450; P-gp: P-glycoprotein.
Extensive first-pass metabolism is one of the greatest pharmacokinetic barriers. Various commonly used second generation antipsychotics, including risperidone, quetiapine, or olanzapine, are greatly hepatically transformed by CYP enzymes, especially CYP2D6 and CYP3A4. This metabolic clearance can substantially reduce oral bioavailability and may require higher oral doses to achieve therapeutic plasma concentrations [39]. Such high dose level increases the risk of systemic toxicity, and also leads to the broad interpatient ranges in drug exposure because of genetic polymorphisms in the metabolic enzymes.
In addition, there are other obstacles to ideal absorption in the gastrointestinal (GI) environment. Isolubility of the drug depends on pH, emptying of the stomach varies, and the efflux transporters found in the intestinal epithelia are some of the factors that make pharmaceutical absorption unpredictable. The lipophilic antipsychotics often have low aqueous solubility that limits their solubility in the gastric lumen. For example, the dissolution and absorption of poorly water-soluble antipsychotics may be affected by gastrointestinal pH changes, gastric emptying variability, and proton pump inhibitor use, particularly in older adults [40]. These not only interfere with the pharmacokinetic profile but also make the design of formulation and dosing more difficult.
The fact that the conventional oral formulations have a low capacity to guarantee effective delivery of CNS is an equally problematic issue. The blood-brain barrier (BBB) is a very selective physiologic interface that helps to limit the passage of most therapeutic agents into brain parenchyma. The majority of antipsychotics are dependent on passive diffusion, and additional inhibitors include the efflux proteins like the P-gp that actively deliver drugs out of the CNS. These transporters have been reported to be upregulated in patients with schizophrenia and this may be one of the reasons as to why they are resistant to treatment [41]. Consequently, despite adequate plasma levels, brain concentrations may remain below therapeutic levels, thereby limiting clinical efficacy and necessitating higher doses.
Clinically, low compliance has continued to be one of the problems of schizophrenia treatment. Cognitive disabilities, poor insight, and avolition may all minimise the chances of regular oral medication taking. It has been observed that oral antipsychotic therapy is discontinued by almost 60 percent of patients during the first year of study and most times not under the advice of a medical professional [42]. The result of this discontinuation is high rates of relapse, hospitalization and total healthcare burden. Besides, non-targeted systemic distribution side effects like sedation, weight gain, hyperprolactinemia, and metabolic syndrome further reduce adherence and patient confidence in treatment.
The other major shortcoming is the strict pharmacokinetic characteristics of traditional oral formulations. Fixed release tablets or capsules lack the flexibility to address the reality of differences between metabolism, circadian variation and comorbidities. They also have a low flexibility in relation to time release or location specificity, which are essential in directing treatment to vulnerable groups, such as the ageing or patients with gastro intestinal comorbidities [43].
All these constraints highlight how insufficient the existing system of oral delivery is to address the generalized needs of schizophrenia therapy in the long term. More advanced methods are necessary because it is evident in clear platforms that could be able to improve the targeting of the CNS and bioavailability, besides alleviating the ill effects and aiding compliance. This clinical need has led to the renewed interest in nanotechnology-based responsive and patient-centric drug delivery systems that are discussed in the next section [44].
In a bid to curb the natural drawbacks of traditional antipsychotic preparations, recent studies have been directed towards development of nanotechnology-based oral drug delivery systems. These systems improve the dissolution, stability, and delivery specificity of antipsychotic drugs that provide regulated release profiles and higher CNS bioavailability [45]. Various systems have been proposed to be used in schizophrenia therapy, such as lipid-based nanoparticles, polymeric carriers, proliposomes, stimuli-responsive, and ligand-targeted nanocarriers, which have demonstrated high potential in preclinical and early clinical trials.
The nanocarriers described in this section cannot be considered to have equivalent designs for translation. The translational success of each carrier platform is based on the physicochemical characteristics of the drug, as well as its stability in the GI environment, manufacturability, ability to increase the concentration in the brain, and compatibility with AI in formulation design. The advantages of using lipid nanocarriers include increased solubility and lymphatic uptake; nevertheless, their physical stability and lipid phase transitions may limit predictions and large-scale production [46]. Polymeric nanoparticles are advantageous when precise control over particle size, surface functionalization, and release rate are required; but they are generally harder to manufacture. Despite offering precision in terms of surface modification, dendrimers have issues linked to toxicity, high cost, and regulation difficulties. On the other hand, proliposomes and self-emulsifying drug delivery system (SEDDS) can be relatively easily modified into oral formulations and thus be more compatible with manufacturing processes. However, they might offer less biological specificity in terms of delivering drugs to the CNS without the use of other targeting methods [45]. As far as stimuli-responsive systems or ligand-targeted delivery systems are concerned, they can be considered the most biologically specific, yet they will be the most difficult systems for implementation using AI because the model would need to consider several parameters related to triggering and biological activity.
Solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs) are biocompatible carriers that entrap lipophilic antipsychotics within a lipid core, shield antipsychotics against enzymatic degradation and allow the sustained release. Olanzapine-loaded SLNs have been investigated to improve oral drug delivery by enhancing solubility, stability, and overall bioavailability compared with conventional formulations [46]. NLCs, which contain a mixture of solid and liquid lipids, have better drug loading and colloidal stability. These systems too are surface modifiable and can undergo the process of increased intestinal uptake through the M cells in the Peyer patches.
Polymeric nanoparticles, e.g., poly(lactic-co-glycolic acid) (PLGA), or polyethylene glycol (PEG)-coated dendrimers have been extensively investigated as sustained-release drug carriers and because of their capacity to penetrate biological barriers. They are versatile hence can be loaded with drugs and surface ligands. PEGylated dendrimer-based quetiapine nanoparticles that were found to have enhanced brain infiltration and behavioral recovery in rodent schizophrenia models. These carriers have been shown to improve drug stability, bioavailability, and delivery efficiency, thereby enhancing the overall therapeutic performance of drug formulations [47].
Proliposomes are dry powders that produce liposomes on hydration that provide increased stability and specific delivery. They especially work well in enhancing the solubility of drugs that are not very soluble in water. Aripiprazole proliposome capsules had a 2.8-fold greater AUC than conventional preparations due to the lymphatic transport and lesser gastric degradation. Likewise, SEDDS has been used to increase the absorption of risperidone, with more reproducible pharmacokinetic behavior and less inter-subject variability [48].
Improvements in the responsive delivery of drugs have resulted in the development of nanocarriers that release drugs in response to particular physiological stimuli. pH-sensitive systems dissolve at intestinal pH levels, preventing the drug in the acidic stomach. pH-sensitive nanogels (loaded with risperidone) doing selective release of the drug at a pH of 6.5 and above, which demonstrated a 2.4-fold increase in systemic exposure [49]. Intestinal enzymes responsive systems, including 2-glucuronidase and azoreductase, can be used to release drugs into specific areas of the GI tract in order to achieve a better spatial control to reduce systemic exposure [50]. Table 3 summarizes recent developments in the oral nanocarrier systems that are customized to treat schizophrenia. It contains the latest studies published in 2020 to 2025 with demonstrations of the innovations in the formulation strategies, CNS targeting efficiency, and therapeutic outcomes.
Recent studies of advanced oral drug delivery systems.
| Delivery system | AI role/innovation | Key findings/benefits | Reference |
|---|---|---|---|
| LRP1-targeted nanoparticle delivering KS-133 | AIguided ligand design for BBB transcytosis | Achieved brain penetration in schizophrenia mouse model; improved CNS exposure of peptide therapeutic | [51] |
| Weekly oral risperidone formulation | Algorithm-assisted PK modelling to extend dosing interval | Once-weekly oral dosing matched daily risperidone efficacy; maintained plasma levels and clinical stability | [52] |
| Intranasal brexpiprazole NLCs | AIinspired nanoformulation design | Enhanced brain targeting of antipsychotic via nasal path, suggesting alternative to oral route | [53] |
| NS-136 (M4 PAM Oral Candidate) | AI-assisted medicinal chemistry and PK prediction | Oral Phase I candidate with pro-cognitive effect designed via AI; targets schizophrenia and Alzheimer’s | [54] |
| Evenamide (NW-3509) AddOn Therapy | AI-supported pharmacodynamic and repurposing profiling | Oral adjunct therapy reduced symptoms in treatment-resistant schizophrenia in Phase II/III studies | [55] |
AI: artificial intelligence; BBB: blood-brain barrier; CNS: central nervous system; NLCs: nanostructured lipid carriers; PK: pharmacokinetics.
Ligand-conjugated nanoparticles have been developed to target the CNS to evade efflux mechanisms and increase CNS targeting by utilizing receptor-mediated transcytosis. Active transport is directed at transferrin, insulin, and lactoferrin receptors on the intestinal epithelium and brain endothelial cells. Nanoparticles carrying olanzapine inside transferrin-functionalized PLGA exhibited more than 2.5-fold higher brain accumulation in vivo than non-targeted systems. Dual-targeted systems, including chitosan folate conjugates, have both the benefit of mucoadhesive and receptor-mediated delivery [56].
Collectively, these platforms represent an important advancement in oral antipsychotic delivery. They have a great potential to overcome the adherence and efficacy issues in the management of schizophrenia by enhancing bioavailability, decreasing dose frequency, and providing specific CNS delivery [57]. These systems are integrated with AI-based formulation optimization, and the following section discusses it. A schematic of the modern oral drug delivery systems, which have AI formulation tools, is presented in Figure 2. It describes the optimization of lipid nanoparticles, dendrimers and receptor-targeted platforms with respect to CNS targeting and bioavailability optimization using predictive modeling [58].
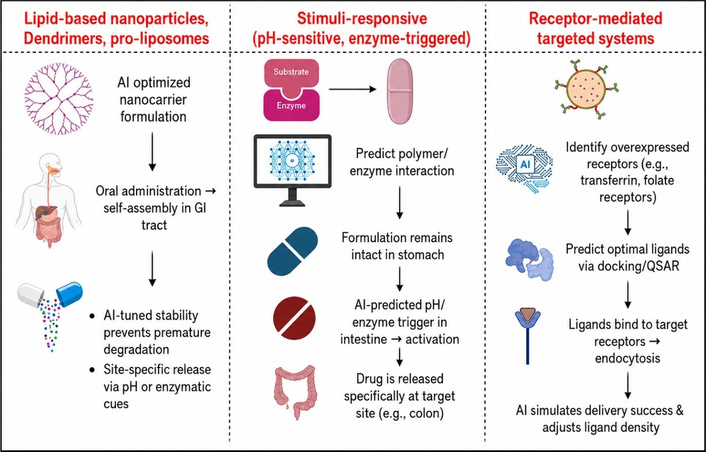
Schematic of AI-enhanced targeted oral drug delivery approaches. AI: artificial intelligence; GI: gastrointestinal; QSAR: quantitative structure-activity relationship.
Traditional formulation development and dosing strategies in schizophrenia therapy are largely empirical and often rely on standardized protocols and fixed dosing regimens. This empirical method can not consider the patient specific variation in drug absorption, distribution, metabolism, and elimination, resulting in variable results [59]. Recent innovations in AI have provided new opportunities of precision pharmacokinetics and personalised drug delivery. Using massive amounts of data and ML algorithms, AI is facilitating the dynamic modelling of formulation properties and optimisation of dose to the patient [60].
The prediction of critical quality attributes (CQAs) of oral nanocarrier formulations, including particle size, drug loading, and kinetics of release, is increasingly being done through AI. Formulation datasets have been trained on ML models such as SVMs, random forests (RFs) and artificial neural networks (ANNs) to find the best input parameters. As an example, deep learning structure that can utilize over 1,200 formulation histories of antipsychotics like risperidone and aripiprazole [61]. The model made accurate predictions of the release profile under different pH conditions and excipient ratios, which cut the workload of the experiments by 70 percent. The tools are currently being integrated into quality-by-design (QbD) pipelines, rational design of formulations that are based on early development [62].
Inverse design, which is driven by AI, is also becoming popular. The desired output characteristics, including a desired drug release curve or dissolution rate, can be used to define the desired properties that those algorithms can back-calculate the best combination of polymers, surfactants, and stabilizers. The ability will minimize formulation cycles and increase reproducibility. Additionally, AI models are being combined with digital twin models, which model in vivo behaviour, and virtual testing of a number of formulation candidates under simulated physiological conditions can be performed [63].
AI-based precision dosing is not to be conflated with non-AI precision psychiatry. Precision dosing with guidance from pharmacogenomic testing, therapeutic drug monitoring, systematic evaluation of side effects, symptom rating scales, and clinical risk stratification does not depend on sophisticated AI algorithms but is capable of providing more personalized treatment for antipsychotics. Differences in gene expression related to CYP2D6, CYP3A4, and CYP1A2 may affect exposure to certain antipsychotic drugs, and therapeutic drug monitoring can aid the adjustment of treatment if there are concerns about medication adherence, interactions between substances, and metabolic irregularities. The role of AI is to enhance the use of these traditional methods of precision medicine through integration into extensive multimodal databases, which include data on pharmacokinetics, pharmacogenomics, patient compliance, wearables, medical history, and practical results.
In addition to formulation, AI is also being utilized in optimizing dose regimens when they depend on individual pharmacodynamic and pharmacokinetic procedures. The clinical variables included in these models comprise body weight, hepatic function, CYP450 genotype, drug-drug interactions, and real-time adherence patterns [64]. Reinforcement learning to optimize doses of risperidone in a simulated schizophrenia patient cohort. Due to the AI agent, the process of dosing was dynamically controlled, which minimized adverse events and kept therapy levels in the plasma more effectively than the fixed-dose protocols [65].
AI is also being used to improve physiologically based pharmacokinetic (PBPK) models, which traditionally have been used to make regulatory submissions, to address real-world patient variability. Software systems such as GastroPlus and Simcyp have started adopting ML functionality to produce absorption, metabolism, and clearance in a wide range of patient populations. These simulations provide assistance in preclinical dose projection, formulation selection, and risk mitigation prior to the clinical trial [66].
The attempt to introduce AI-mediated formulation and dosing into clinical practice is picking up steam. A 2024 study at King’s College London used a real-life experiment to deploy an AI-driven clinical decision support system (CDSS) into the EHR to customize the dose of risperidone based on pharmacogenomic information. This system has the potential to improve therapeutic monitoring and support safer, more individualized treatment approaches compared with conventional care [67].
Regulatory agencies are starting to appreciate the use of AI to develop medicines. The European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) have published draft guidelines that promote the utilisation of validated AI models in drug dosage and formulation design. With the development of digital health systems, AI-enhanced platforms will become part of clinical pharmacology and regulatory science [68].
All these AI innovations are transforming the landscape of formulation to be predictive rather than reactive, as oral antipsychotic treatment is now customized to the individual biology and behavior of the patient, both on a molecular scale and the unique biological and behavioral patterns of the patient.
Over the past decade, oral nanocarriers and targeted drug delivery systems have shown considerable progress in the preclinical development of schizophrenia therapeutics. Nevertheless, the ultimate measure of innovation is successful clinical translation, which has historically been limited by formulation instability, manufacturing challenges, and regulatory uncertainty [69]. Between 2022 and 2025, several advanced oral drug delivery approaches and AI-supported therapeutic strategies have progressed through preclinical evaluation, early clinical investigation, or computational validation. These studies highlight recent advances in AI-supported therapeutic strategies and targeted drug delivery systems, demonstrating encouraging progress toward clinical translation, although broader clinical confirmation remains necessary [69, 70].
Recent methods of formulating and dosing drugs in schizophrenia are still predominantly empirically based, relying on fixed-dose regimens and generalized pharmacokinetic modeling. This conventional approach does not fully account for interindividual biological variability, which can influence treatment response and therapeutic outcomes [71]. This makes therapeutic results highly variable, with side effects being unpredictable. The development of AI is an interesting solution. Based on practical data and sophisticated ML models, AI is facilitating personalized formulation modeling and dose-specific adjustments to patients to facilitate a more accurate and flexible treatment paradigm.
In 2023, it began its Phase I/IIa trial (NCT05732091) to assess the safety and pharmacokinetics of an oral risperidone capsule which is driven by nanoparticles. This formulation strategy incorporated advanced nanocarrier design principles to improve oral drug delivery and therapeutic performance [72]. The trial recorded a 1.9-fold rise in bioavailability, reduced interindividual plasma variability, and minimum adverse event peak as compared to the traditional risperidone. No dose-limiting toxicities occurred and the scores on tolerability were rated highly by patients compared with the case with the standard formulations [73].
At the same time, a Phase I study published by Clinical Pharmacokinetics involved an aripiprazole proliposure system, which was to be administered as a one-dose oral tablet. The formulation achieved an average due to the 24-hour sustained release of drugs and averting a fall in plasma trough by 38%. Pharmacokinetic modeling can help evaluate whether modified-release antipsychotic formulations maintain therapeutic drug exposure over extended dosing intervals, which may support adherence in outpatient schizophrenia care [74].
In a 2024 observational study of St. Mary’s Hospital in Seoul, an integrated AI-based decision support tool on oral doses of olanzapine was evaluated with reference to its clinical utility. This system was based on real-time pharmacogenomic data such as the genotype of CYP1A2, the hepatic function, and the history of prior side effects to recommend personalized dose adjustment [75]. In 97 schizophrenic patients under enrolment, AI-guided dosing resulted in 30 per cent higher rate of therapeutic plasma concentrations and 25 per cent less adverse drug reactions than retrospective controls. Such an intelligent approach of smart formulation and AI-based personalization is an example of transitioning to smart patient-centered schizophrenia treatment [76].
Although such promising outcomes have been achieved, there remain critical issues with the translation of such technologies into the clinical practice. The ability to reproduce in large scale production is a key bottleneck, especially with complex nanocarrier systems. There are challenges of batch-to-batch variability of the size, loading, and release kinetics of the particles, which is a challenge in regulatory standardization [77]. At the same time, the platforms for assessing adaptive delivery systems and AI-assisted platforms remain in development. Nevertheless, other programs like the FDA program Emerging Technology Program (ETP) are working hard to integrate the regulatory aspects of these innovations. There are several AI-developed oral therapeutics currently at the pre-investigational new drug (pre-IND) consultation stage, indicating institutional preparedness for these next-generation platforms [78].
These novel oral delivery systems are on the verge of being used widely as the ongoing trials are likely to produce strong clinical information. They are a major advancement in the history of schizophrenia treatment, which balances the gap between technological innovation and the impact on patients in real-life scenarios through increased bioavailability, greater tolerability, and customized dosing.
The changing concept of schizophrenia as a heterogeneous and multifaceted neuropsychiatric disease has highlighted the shortcomings of single-size-fits-all pharmacological treatment. The inconsistencies in the symptom manifestation, disease progression, pharmacodynamics, and pharmacokinetics call for more adaptive and individualized treatment. Although the current development and innovations in the system of oral drug delivery have allowed progress in the stability of formulations and CNS targeting, their maximum value will be achieved only with the adoption of AI. Such tools are increasingly influencing formulation development, dose optimization, and real-time therapeutic monitoring, supporting the broader movement toward personalized and precision psychiatry in schizophrenia management [79].
AI is transforming the nature of drug formulation science, which allows predicting key pharmacokinetic parameters of the drug in terms of its reaction to patient-specific variables. They are genetic polymorphisms (such as CYP450 isoenzymes), age, sex, body mass index, hepatic and renal functioning, eating habits, and co-medication records [80]. Using these data in ML models, researchers are able to predict drug absorption, bioavailability, distribution, and clearance with an unprecedented degree of accuracy. The formulation properties that can be optimized in-silico using these models include the choice of the polymer, the size of the nanoparticles, the release behavior, and the mucosal adhesion characteristics.
Tanaka multi-input ANN to predict plasma olanzapine levels depending on drug formulation, differences in genotypes, and the consumption of dietary fat. Their model had an error of less than 10% on the mean error, which enabled proper prediction of therapeutic ranges in simulated populations [80, 81]. These tools are being incorporated in formulation design platforms to minimize empirical testing and hasten the process of clinical trials of optimized nanocarriers.
Besides, AI can be used to dynamically optimize by connecting real-time physiological data (hormone levels, inflammatory markers, and circadian metrics) with drug release properties. Adaptive modeling may be used to optimize drug release characteristics and dosing strategies based on patient-specific physiological and therapeutic requirements, thereby supporting personalized treatment approaches [82]. The design of smart tablets and AI to design oral dosage forms are among the abilities being considered.
Of particular interest is the idea of a library of formulations that are AI-driven. Within this context, the AI algorithms trained on pharmacogenomic and clinical outcome data will be used to match databases of pre-formulated nanocarriers to the individual patient profiles. After assessing the patient, the AI will choose the most fitting formulation, which saves a lot of time on aligning with the therapeutic process [83]. This approach is especially relevant for treatment-resistant patients and elderly populations, who often show variable metabolic and therapeutic response profiles.
It is also being associated with AI tools with sophisticated manufacturing methods, including 3D printing or automated microfluidics, to print a custom dosage of oral medication on demand. This specifically holds promise in the creation of patient-specific fixed dose combinations, polypills and modified-release matrices adjusted to circadian requirements or co-morbidities [84].
In addition to formulation, AI continues to be applied to monitor treatment effectiveness and make changes to the dosage based on a combination of wearable and ingestible devices. Physiological parameters that a smart wearable sensor can monitor are heart rate variability, galvanic skin response, movements, sleep cycles, and even facial affect. Such data streams can be input into AI models, which have been trained to identify early signs of psychotic relapse or drug side effects, which allows for taking measures ahead of time [85].
Systems that involve ingestible sensor devices or digital pills have been considered as methods to ensure drug ingestion and adherence in psychiatry. It is important to note that such tools can be considered an integral part of a digital monitoring system rather than a standalone approach that will serve as a closed-loop management system [86]. Wearable sensors, mobile-based markers of behavior, sleep and activity monitoring, speech monitoring, electronic monitoring of medication events, and clinician-controlled dashboards might give us more data on adherence, relapse risks, and tolerability. Currently, there is a lack of research regarding the effectiveness of closed-loop dose adjustments in schizophrenia, and most studies need prospective validation [87].
These systems may support a semi-closed-loop model of care in which digital signals alert clinicians to possible non-adherence, relapse risk, or emerging adverse effects. However, autonomous dose modification remains premature in schizophrenia care. At the current stage, AI-generated alerts or dosing suggestions should be reviewed by clinicians and interpreted alongside symptom assessment, medication history, adverse-effect profile, and patient preference. The mobile applications can be integrated with these systems to give both patients and providers just-in-time behavioral prompts or alerts. Another significant benefit is real-time adherence monitoring [88]. Ingestible sensors such as etectRx and digital pills cleared under Abilify MyCite assist in confirming the dose intake and commanding AI models which imitate and adjust dose according to missed doses or fluctuating pharmacokinetics.
The behavioral and environmental data with biological metrics are now being integrated into AI systems. Passive indicators of the state of mind are being tracked by smartphone-based geolocation data, patterns of social media usage, frequency of speech, and digital interaction [89]. The relapse prediction based on a week of multimodal data with AI models trained on such data reached 88 percent sensitivity. These devices are especially helpful in the outpatient environment where close clinical observation is restricted.
Notably, AI-driven systems have the capability of assisting the recalibration of doses when there is a missed dose or when there is the development of side effects. In case a patient fails to take two doses in a row or displays indicators of metabolic side effects, which include rapid weight gain or increased resting glucose, the system is capable of automatically calculating compensatory dosing or the need for clinical follow-up [90]. As shown in Figure 3, AI-based feedback loops utilize sustained inputs of wearable and ingestible items. These systems, coupled with the simulations of the digital twins, enable real-time adaptive therapeutic and adjusting the profile depending on the changing physiological and behavioral characteristics of a patient.
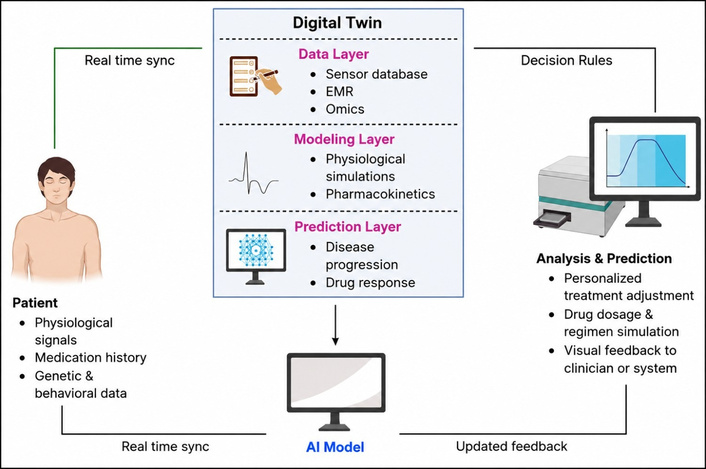
AI-integrated feedback loop model incorporating digital twin. AI: artificial intelligence; EMR: electronic medical record.
One of the most sophisticated uses of AI in personalized medicine is the concept of the digital twin, which refers to a continually refined digital replica of a specific patient. For schizophrenia management, a digital twin would need to integrate multimodal variables that describe the current state of the patient, biological predisposition, medication administration, changes in behavior, and treatment response. Potential input variables might comprise demographic information, age at disease onset, duration of illness, symptom ratings, past relapses, hospital admission details, exposure to antipsychotics, compliance history, previous side effects, pharmacogenetic factors such as CYP2D6, CYP3A4, and CYP1A2 genotypes, levels of medication in the blood, metabolism, neuroimaging characteristics, electrophysiology, sleep/activity patterns, speech attributes, and behavioral signals collected by smartphones or wearables. For digital twin development, multimodal inputs may include relatively stable variables such as genomic data, periodically updated clinical or neuroimaging data, and frequently updated digital biomarkers from wearable, ingestible, or smartphone-based technologies [91].
For digital twin modeling to provide meaningful information for the treatment process, its validation should go beyond just evaluating the model itself. The following aspects should be considered as validation criteria: sensitivity and specificity for predicting disease relapse or non-responsiveness, area under the ROC curve for classification tasks, comparison of predicted vs. observed risk through calibration curves, positive and negative predictive values in external cohorts, and clinical validity assessment via decision-curve analysis [92]. For pharmacokinetics or optimal dose findings, mean prediction error, root mean square error, bias, precision, and the agreement between predicted and observed drug concentrations in plasma should be provided [89].
In schizophrenia, digital twins are being trained using data from longitudinal studies, neuroimaging repositories, pharmacogenomics datasets, wearable sensor feeds, and clinical trial outcomes. Digital twin model based on 1,000 schizophrenia patients simulates the outcomes of three different oral antipsychotic regimens. The model achieved 82% accuracy in predicting optimal regimen-patient matches and flagged metabolic concerns in high-risk profiles [92].
They are now being simulated to bring co-treatment situations such as antipsychotics with mood stabilizers, antidiabetics, or nootropics. In Mayo Clinic, three adjunctive therapy combinations were simulated using a digital twin to compare them in 200 patients [93]. The twin-predicted optimal regimen matched observed real-world results in 74% of the cases, and therefore, has high translational potential.
Optimization of clinical trials is also being tried with digital twins. Virtual controls made using digital twin models can lower the costs of a trial, time, and ethical overheads of using placebo arms. The regulatory agencies, such as the FDA and EMA, have developed investigative frameworks for validating digital twin models in the adaptive trial designs. This may transform the trial methods in psychiatry by their use in dose-ranging, safety testing and individual risk stratification [94, 95].
In the future, the combination of digital twins and formulation libraries and real-time monitoring systems will allow moving towards a dynamic, responsive therapeutic ecosystem. These systems may be able to produce intervention results depending on new either behavioral or physiological inputs, and prompt automatic changes in formulation or dosing [96]. With this system, schizophrenia care would be changed from reactive crisis management to the proactive precision psychiatry that is data-driven.
Nevertheless, several limitations exist concerning the use of AI-supported formulation design and pharmacokinetic prediction. The ability of AI algorithms to predict accurately is significantly influenced by the quality and quantity of information used during training. In nanomedicines, existing datasets may not always be sufficient or homogeneous since they are produced from distinct experimental setups. Hence, AI models built based on small or heterogeneous datasets may have high internal validity but weak external validity. Moreover, most of these models cannot yet be fully transparent, thus hindering their adoption by formulators, clinicians, and regulators. Hence, AI should only be used as a decision-making tool but not an alternative to empirical experiments. It can save time and effort in the development of formulations and help determine probable components of drug formulations and rationalize dose customization.
Although the future of AI and oral drug delivery has a bright future in treating schizophrenia, there are various technical, clinical, and ethical issues that need to be resolved before the innovations become a common part of everyday care. With oral nanocarriers, the in vivo performance of drugs is influenced not only by carrier release characteristics but also by gastrointestinal physiology, mucus interaction, intestinal absorption, lymphatic transport, first-pass metabolism, and, for CNS-targeted systems, blood-brain barrier penetration [97]. This part examines the existing barriers, ethical issues, and a research roadmap that should be developed to realize long-term clinical implementation of AI-based oral therapeutics.
Reproducibility and generalizability remain among the most important challenges for AI models in schizophrenia care. Most ML models are trained on data that represents narrow geographic/institutional populations and hence, when implemented in different real-life environments, result in performance differences [98]. This training data heterogeneity is one of the reasons why the models are not robust to different clinical subtypes, ethnicities, and environmental factors. The problem is especially decisive in such a sphere as psychiatry, where the manifestation of symptoms and the reaction to treatment is extremely individual.
Furthermore, a large number of AI models are limited to proof-of-concept or preclinical level. Very few have been subjected to intensive external validation or prospective testing by randomized clinical trial. The clinical implementation is also limited by infrastructural factors, including the problem of interoperability of wearable devices, ingestible sensors, and the EHR of hospitals [99]. While the real-time patient monitoring device data stream integration into clinical workflows is technically complex and resource-intensive.
Scalability is also complicated by the absence of standardized protocols on the AI-enhanced oral drug formulation. Nanocarrier systems are normally associated with manufacturing flaws in terms of particle size distribution, surface charge, and encapsulation efficiency. These inconsistencies are a great hindrance to regulatory permission and mass manufacturing [100]. The technology of the AI-assisted formulation design has not yet reached a level of current good manufacturing practice (cGMP) standards, which restricts industrial translation. Also, AI implementation into the formulation process must balance datasets in formulation chemistry, pharmacokinetics, and patient-specific variables a multifactorial problem still unsolved completely [101].
Clinically, adoption has low levels of digital literacy in healthcare providers on AI assisted tools. A significant number of clinicians do not believe in model accuracy and are not usually keen on leaving therapeutic choices to systems that are viewed as black boxes. Moreover, the vast majority of AI-generated results cannot be explained, and a clinician may not find it easy to judge the model predetermination [102]. These are the obstacles to the adoption of trust and uptake by psychiatrists and pharmacists as the gatekeepers to schizophrenia management.
AI application in psychiatry presents special ethical challenges, especially in terms of data management, transparency of models, and bias possibilities. The use of wearable technology, ingestible sensors, and mobile health applications produces continuous and granular data feeds that contain physiological, behavioral, and even geolocation data. Though such data have immense clinical value, collection and storage of such data are a great threat to privacy and autonomy. In schizophrenic patients who already might be paranoid or distrustful of such surveillance may worsen the symptoms or reduce the level of adherence to treatment [103].
The processes of informed consent should be modified to handle the dynamism and evolving aspects of AI monitoring. Formal consent forms are not always adequate to present dynamic systems which learn and adapt as they are used [104]. The patients should be provided with the option to refuse to be collected in particular forms of data or have their data not be utilized to create an algorithm. The patient identities should be safeguarded with the help of transparent data stewardship schemes, such as federated learning, and differential privacy [105].
Another issue that is burning is algorithmic bias. AI systems trained using biased or non-representative data might strengthen or increase healthcare inequalities. As an example, NLP speech analysis models can be inefficient with speech from underrepresented language groups, which results in incorrect diagnoses or late intervention [106]. A 2023 study found that an NLP tool, which was applied to determine the risk of psychosis, discovered that its false negative rate was 25% higher in non-English speakers than in native English speakers. The solution to these disparities is a deliberate data diversification throughout training, and periodic performance auditing between demographical subgroups [107].
Prediction of false positives poses a particularly salient ethical challenge in prodromal and high-risk groups. AI-powered systems that wrongly predict someone as having a high risk of psychosis can create distressing experiences for those involved, stigmatization, unnecessary clinical monitoring, and even premature pharmacological treatment. The relevance of this problem lies in the fact that only some people in the clinically high-risk group eventually develop psychosis. Thus, AI-based prodromal detection must not be used on its own as a classification system. It should be employed as an aid in the diagnosis process together with clinical evaluation, monitoring over time, family history, deterioration in functioning, and personal preference of the patient.
Elucidation is one of the significant obstacles to the ethical incorporation of AI tools. Deep learning models and especially multimodal data fusion models tend to generate results that are not easily understandable by clinicians and patients. It does not make therapeutic decisions easy to defend without a clear understanding of the contribution of the input variables to the outputs. Such XAI methods as attention mapping, SHAP (Shapley additive explanations), and decision tree approximations have to be developed and made standard to use in clinical psychiatry [108]. Thorough model reporting and post hoc interpretability are required to make AI usage in schizophrenia care responsible and accountable.
In order to get the best out of AI-powered oral therapeutics, a multi-faceted research agenda should be undertaken. To begin with, datasets on which AI models are being trained must be increased to cover a wide range of patient populations, symptom clusters, and environmental factors. This can be enabled by federated learning platforms, which allow multiple institutions to train shared models without directly exchanging sensitive patient-level data [109]. Global healthcare settings will have to be cross-validated to be able to define generalizability. In addition, AI generated results ought to be compared with those of expert clinicians to determine practical utility.
Secondly, regulatory engagement should also be proactive. Regulatory authorities such as FDA, EMA, and CDSCO (Central Drugs Standard Control Organization) ought to work with academic and industry stakeholders to establish approval routes for AI-formulated medicine and decision support systems [110]. Cross-validation across global healthcare settings will be necessary to establish generalizability. Moreover, AI outputs should be benchmarked against expert clinician decisions to assess real-world utility.
Third, most ML models are trained on data representing narrow geographic or institutional populations and, therefore, may exhibit performance differences when implemented in diverse real-world environments [111]. The existing models of software as a medical device (SaMD) need to be broadened to encompass more hybrid platforms with formulation modeling, therapeutic monitoring, and self-adjusting doses. Oral therapeutics with AI augmentation may also benefit from evaluation within controlled regulatory frameworks before broader clinical implementation [112].
Fourth, the digital infrastructure needs to be improved so that it can enable real-time monitoring and the implementation of AI in psychiatry. It entails the combination of wearable sensors, ingestible devices, and digital twin models with the hospital EHRs. The presence of interoperability standards must be created to make data exchange between devices and AI platforms seamless [113, 114]. Simultaneously, clinicians would have to be trained in the fields of AI interpretation and digital literacy, preferably via continuing medical education coursework and curricula in psychiatry and pharmacy studies.
Lastly, ethical management should become a part of the research and implementation process. The use of AI tools should be tested in terms of biasness, transparency, and patient safety by independent ethics boards prior to their widespread use. It is also important that there is engagement with the people. Caregivers and patients must co-design AI systems to make sure that their worries on privacy, agency, and trust are appropriately taken into consideration at the initial stage [114]. Figure 4 presents a strategic roadmap of AI-integrated schizophrenia therapeutics to help inform the future direction of translation. It charts the milestones that are crucial such as standardization of data and federation of learning up to regulatory validation and clinical deployment that are necessary in the adoption of the systems.
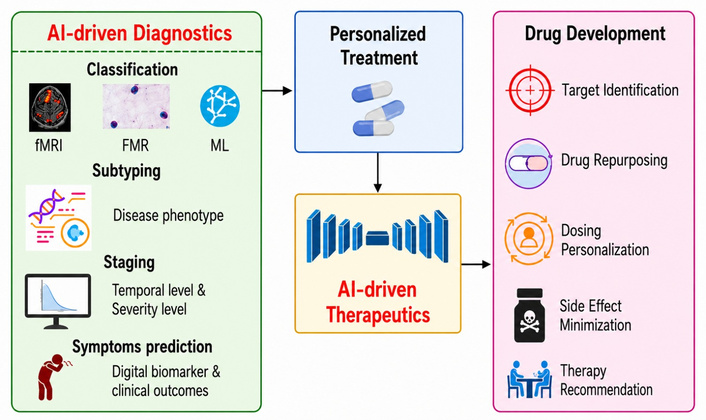
Roadmap for AI-driven diagnostics and therapeutics in schizophrenia. AI: artificial intelligence; fMRI: functional magnetic resonance imaging; FMR: facial morphology recognition; ML: machine learning.
Even though the integration of AI with nanodelivery systems represents an excellent solution for delivering antipsychotic drugs through precision oral delivery, its translational capacity is contingent upon the extent to which the computational algorithmic models represent the actual release behavior of nanocarrier systems. One important drawback in terms of the predictive power of such computational models is the possibility that some of the data on the release patterns are derived from in vitro setups that are not standardized. The problem is that release experiments in nanocarrier studies often vary greatly in their design and can include dialysis bag technique, modified Franz diffusion cell setup, USP (United States Pharmacopeia) dissolution method, or custom-made agitation systems. The parameters influencing the release pattern can involve the composition of the dissolving medium, pH regimen, number of enzymes, surfactant amount, speed of agitation, membrane type, frequency of sampling, and temperature [111].
A related limitation involves potential discrepancies between in vitro release characteristics and in vivo pharmacokinetic properties. With oral nanocarriers, the in vivo behavior of the drug does not solely depend on its release rate from the carrier, but is further affected by gastric retention, intestinal transit time, interaction with bile salts, diffusion across mucus layers, enzymatic degradation, absorption through the enterocytes, lymphatic delivery, penetration through the BBB, and first pass effect [97]. As such, formulations with an optimal in vitro release profile will not always deliver the desired profile of either plasma or brain concentrations over time. Using AI-generated dose recommendations that consider solely in vitro release kinetics without pharmacokinetic assessment could either over- or under-estimate exposure to therapy or dose dumping, among other things.
In order to mitigate this risk, a validation strategy for the development of future AI-assisted oral nanotherapeutics needs to be created based on a closed loop validation procedure involving AI predictions, standardized release testing in vitro, and pharmacokinetics in vivo. In this approach, the AI system would predict the composition and release pattern of the drug formulation, which would then be validated using standard release methodologies such as relevant USP dissolution apparatus or biorelevant dissolution medium tests [105]. The obtained results from the release experiments would need to be compared against pharmacokinetic parameters, including Cmax, Tmax, AUC, half-life, brain-to-plasma ratio, and individual variation in patients. A discrepancy between the predicted and experimentally observed drug release or pharmacokinetic profile would indicate the need for model refinement and retraining using newly generated experimental data to improve predictive accuracy [84, 113].
The integration of AI with innovative oral drug delivery systems represents a promising direction for improving the diagnosis and treatment of schizophrenia. The review has critically discussed the diagnostic shortcomings of more traditional symptom-based paradigms and how AI-powered tools such as NLP, neuroimaging analytics, electrophysiological modeling, and multi-omics fusion can be used to enable earlier, more precise, and personalized diagnosis. Simultaneously, it has been shown that the nascent nanocarrier platforms and smart oral formulations can enhance CNS targeting, pharmacokinetics, and therapeutic compliance.
These innovations, combined, establish a platform on which precision psychiatry is possible, where diagnosis and treatment are dynamically personalized to the neurobiological and behavioral profile of the patient. Recent preclinical studies, early clinical investigations, and computational reports published between 2022 and 2025 suggest the potential of nanoparticle-enhanced oral formulations, AI-supported dosing approaches, and digital twin-based simulations. However, broader clinical validation is still required before these approaches can be recommended for routine schizophrenia care. Such systems provide not only the pharmacological benefits, but also the possibility of a real-time therapeutic monitoring and adaptive intervention.
The intervention to implement with the clinicians is to start using the AI-enhanced decision-support tools and electronic adherence monitoring in outpatient care. The researchers ought to concentrate on AI model multicenter validation and data integration framework standardization. Regulatory agencies and policymakers should put forward the establishment of transparent avenues that will be used to clear AI-designed therapeutics and hybrid diagnostic systems.
There are several limitations to this review. First, this is a narrative review, and it is not a systematic review or a meta-analysis, meaning that there is no formal risk-of-bias assessment and quantitative pooling in this review. Secondly, there are several studies that still lie in their preliminary stages, preclinical or clinical, making the application difficult. Additionally, pediatric, adolescent, and elderly populations of schizophrenia were not considered separately despite them possibly needing different approaches in diagnosis and treatment. Finally, a meta-analysis was impossible due to too much heterogeneity between studies regarding AI models, datasets, nanosystems, and methodologies used.
Looking ahead, the convergence of neuroscience, ML, and smart delivery science should be supported by structured regulatory sandboxes for AI-nano combination products, where formulation performance, algorithmic reliability, patient safety, and real-world clinical utility can be evaluated before wider clinical implementation.
AI: artificial intelligence
ANNs: artificial neural networks
AUC: area under the curve
BBB: blood-brain barrier
CDSCO: Central Drugs Standard Control Organization
CDSS: clinical decision support system
CHR: clinical high risk
CNN: convolutional neural network
CNS: central nervous system
CQAs: critical quality attributes
DALYs: disability-adjusted life years
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
DTI: diffusion tensor imaging
EEG: electroencephalography
EHRs: electronic health records
EMA: European Medicines Agency
ERP: event-related potential
FDA: U.S. Food and Drug Administration
fMRI: functional magnetic resonance imaging
GI: gastrointestinal
GWAS: genome-wide association studies
ICD-11: International Classification of Diseases, 11th Revision
MEG: magnetoencephalography
ML: machine learning
MRI: magnetic resonance imaging
NLCs: nanostructured lipid carriers
NLP: natural language processing
PBPK: physiologically based pharmacokinetic
PEG: polyethylene glycol
P-gp: P-glycoprotein
PK: pharmacokinetic
PLGA: poly(lactic-co-glycolic acid)
PRS: polygenic risk score
RFs: random forests
SaMD: software as a medical device
SEDDS: self-emulsifying drug delivery system
SHAP: Shapley additive explanations
SLNs: solid lipid nanoparticles
SVMs: support vector machines
WHO: World Health Organization
XAI: explainable artificial intelligence
Declaration of AI and AI-assisted technologies in the writing process: during the preparation of this work, the authors used Grammarly and QuillBot for English language refinement. After using these tools, the authors reviewed and edited the content as needed and take full responsibility for the content of the manuscript.
The authors are thankful to their respective institutions for providing academic support during the preparation of this review article.
YDD: Conceptualization, Data curation, Investigation, Methodology, Resources, Visualization, Writing—original draft, Writing—review & editing. DUK: Conceptualization, Project administration, Resources, Supervision, Validation, Writing—review & editing. RKM: Data curation, Software, Visualization, Writing—review & editing. KS: Formal analysis, Validation, Writing—review & editing. VMN: Formal analysis, Validation, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 400
Download: 15
Times Cited: 0
Rui Yang ... Xuejuan Zhang
