20 results in Exploration of Targeted Anti-tumor Therapy
Latest
Sort by :
- Latest
- Most Viewed
- Most Downloaded
- Most Cited
Open Access
Meeting Abstracts
Selected meeting abstracts of 2nd International Conference on Contemporary Oncology
Chouaib Salem
Published: June 28, 2024 Explor Target Antitumor Ther. 2024;5:789–799

Open Access
Case Report
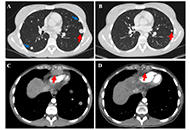
Response to trametinib, hydroxychloroquine, and bevacizumab in a young woman with NRAS-mutated metastatic intrahepatic cholangiocarcinoma: a case report
Aram A. Musaelyan ... Sergey V. Orlov
Published: June 28, 2024 Explor Target Antitumor Ther. 2024;5:780–788
Open Access
Original Article
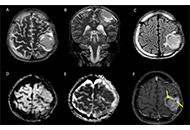
Imaging of supratentorial ependymomas with radio-pathological correlation
Arpita Sahu ... Epari Sridhar
Published: June 27, 2024 Explor Target Antitumor Ther. 2024;5:766–779
This article belongs to the special issue Theranostic Frontiers in Neuro-Oncology
Open Access
Review
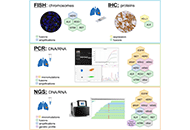
Current status of molecular diagnostics for lung cancer
Evgeny N. Imyanitov ... Sergey V. Orlov
Published: June 27, 2024 Explor Target Antitumor Ther. 2024;5:742–765
This article belongs to the special issue Integrated Approaches for Non-Small-Cell Lung Cancer
Open Access
Review
Antibody-drug conjugates combinations in cancer treatment
Giulia Pretelli ... Anastasios Stathis
Published: June 27, 2024 Explor Target Antitumor Ther. 2024;5:714–741
This article belongs to the special issue Antibody-Drug Conjugates
Open Access
Review
Promising immunotherapeutic approaches for primary effusion lymphoma
Jutatip Panaampon, Seiji Okada
Published: June 26, 2024 Explor Target Antitumor Ther. 2024;5:699–713
This article belongs to the special issue Novel Strategies and Targets for Immunotherapy of Cancer

Open Access
Review
DNA damage targeted therapy for advanced breast cancer
Vanessa Patel ... Luís Costa
Published: June 25, 2024 Explor Target Antitumor Ther. 2024;5:678–698

Open Access
Review
Landscape of targeted therapies for advanced urothelial carcinoma
Shihao Shang ... Zheng Zhu
Published: June 21, 2024 Explor Target Antitumor Ther. 2024;5:641–677
This article belongs to the special issue Emerging Molecular Targets and Therapies of Genitourinary Tumors

Open Access
Review
Clinical relevance of circulating tumor DNA in ovarian cancer: current issues and future opportunities
Elena Trevisi ... Ilaria Colombo
Published: June 19, 2024 Explor Target Antitumor Ther. 2024;5:627–640
This article belongs to the special issue The Implementation of Liquid Biopsy in Clinical Practice for Different Solid Tumor

Open Access
Original Article
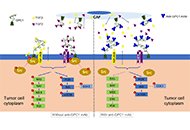
Evaluation of antitumor potential of an anti-glypican-1 monoclonal antibody in preclinical lung cancer models reveals a distinct mechanism of action
Minghua Li ... Qingyu Zhou
Published: June 17, 2024 Explor Target Antitumor Ther. 2024;5:600–626
This article belongs to the special issue Molecular Diagnosis and Personalized Therapy of Cancer
Open Access
Review
Comparison of primary and passaged tumor cell cultures and their application in personalized medicine
Vladislava V. Pipiya ... Valeriya V. Solovyeva
Published: June 17, 2024 Explor Target Antitumor Ther. 2024;5:581–599

Open Access
Meta-Analysis
Anti-PD-1/L1 antibody plus anti-VEGF antibody vs. plus VEGFR-targeted TKI as first-line therapy for unresectable hepatocellular carcinoma: a network meta-analysis
Yiwen Zhou ... Jieer Ying
Published: June 17, 2024 Explor Target Antitumor Ther. 2024;5:568–580
This article belongs to the special issue Novel Insights into Immunotherapy Targeting Tumor Microenvironment in Cancer
Open Access
Original Article
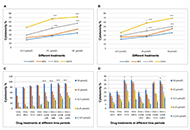
Evaluation of molecular effects associated with apoptosis, tumour progression, angiogenesis and metastasis by a novel combination of drugs with ormeloxifene in triple negative breast cancer cells
Shehna Sharaf ... Lakshmi S
Published: June 11, 2024 Explor Target Antitumor Ther. 2024;5:551–567
This article belongs to the special issue Innovative Strategies to Target Triple-negative Breast Cancer
Open Access
Perspective
Practical implications of androgen receptor inhibitors for prostate cancer treatment
Fabio Campodonico ... Carlo Introini
Published: May 28, 2024 Explor Target Antitumor Ther. 2024;5:543–550
This article belongs to the special issue Molecular Diagnosis and Personalized Therapy of Cancer

Open Access
Original Article
Cadmium nanocluster as a safe nanocarrier: biodistribution in BALB/c mice and application to carry crocin to breast cancer cell lines
Moslem Jafarisani ... S. Zahra Bathaie
Published: May 28, 2024 Explor Target Antitumor Ther. 2024;5:522–542

Open Access
Original Article
Chemotherapy related changes in cfDNA levels in squamous non-small cell lung cancer: correlation with symptom scores and radiological responses
Nithiyanandan Ravi ... Navneet Singh
Published: May 28, 2024 Explor Target Antitumor Ther. 2024;5:508–521
This article belongs to the special issue The Implementation of Liquid Biopsy in Clinical Practice for Different Solid Tumor
Open Access
Perspective
Resistance to immune checkpoint inhibitors in colorectal cancer with deficient mismatch repair/microsatellite instability: misdiagnosis, pseudoprogression and/or tumor heterogeneity?
Nicola Normanno ... Carmine Pinto
Published: May 23, 2024 Explor Target Antitumor Ther. 2024;5:495–507
Open Access
Review
Advancements and recent explorations of anti-cancer activity of chrysin: from molecular targets to therapeutic perspective
Abhilasha Sood ... Manoj Kumar
Published: May 23, 2024 Explor Target Antitumor Ther. 2024;5:477–494

Open Access
Perspective
Immunotherapy in thymic epithelial tumors: tissue predictive biomarkers for immune checkpoint inhibitors
Stefano Lucà ... Renato Franco
Published: May 21, 2024 Explor Target Antitumor Ther. 2024;5:465–476
This article belongs to the special issue Molecular Diagnosis and Personalized Therapy of Cancer
Open Access
Review
Management of oligometastatic and oligoprogressive epidermal growth factor receptor mutated non-small cell lung cancer patients: state of the art of a combined approach
Francesca Di Pressa ... Alessio Bruni
Published: May 17, 2024 Explor Target Antitumor Ther. 2024;5:449–464
This article belongs to the special issue Integrated Approaches for Non-Small-Cell Lung Cancer
