 Review
Review

Affiliation:
Department of Pharmacology, Centre of Natural Products, National Centre for Scientific Research, Havana 11000, Cuba
Email: vivian.molina@cnic.edu.cu
ORCID: https://orcid.org/0000-0003-0706-5547
Affiliation:
Department of Pharmacology, Centre of Natural Products, National Centre for Scientific Research, Havana 11000, Cuba
ORCID: https://orcid.org/0000-0003-3014-5457
Explor Neurosci. 2024;3:65–79 DOI: https://doi.org/10.37349/en.2024.00037
Received: April 06, 2023 Accepted: November 24, 2023 Published: February 26, 2024
Academic Editor: Aurel Popa-Wagner, University of Medicine and Pharmacy Craiova, Romania
The article belongs to the special issue Cerebral Ischemia, Genetics, Comorbidities, Risk Factors and New Therapeutic Options for Neurorestoration
Stroke is among the leading causes of mortality and disability; therefore, it constitutes a relevant health problem. Cuban policosanol presents lipid-lowering, antiplatelet, antioxidant and vascular endothelium protective properties, all of which give it a comprehensive anti-atherosclerotic effect. This review is aimed to show, analyze and discuss the main preclinical and clinical evidence of the effects of Cuban policosanol on ischemic stroke. Preclinical studies evidenced the anti-ischemic effects of preventive and therapeutic oral treatment with Cuban policosanol in Mongolian gerbils with cerebral ischemia induced by unilateral and permanent ligation of a carotid artery, and in global cerebral ischemia induced by bilateral clamping and recirculation of both carotids; being similar or superior to other anti-ischemic agents. Also, combination therapy with aspirin produced greater anti-stroke efficacy compared with aspirin monotherapy, but being similar to policosanol plus atorvastatin combination. This anti-stroke effect was associated to a serum thromboxane A2 (TxA2) concentrations reduction and prostacyclin (PgI2) increase, leading to a favorable TxA2/PgI2 balance, and also to the malondialdehyde (MDA) and sulfhydryl groups (SHG, lipid peroxidation and protein oxidation markers, respectively) reduction. Cuban policosanol combined with aspirin (standard therapy) improved and benefited patients with prior ischemic stroke in terms of functional and neurological outcomes, in open-label studies and in randomized, double-blind, controlled studies. These beneficial effects on stroke patients were associated with antioxidant and antiplatelet effects of policosanol. Also, the combinations of Cuban policosanol plus aspirin and atorvastatin plus aspirin compared in a clinical study significantly and similarly improved the neurological recovery of patients with ischemic stroke. Cuban policosanol was safe and well tolerated, with no serious adverse events occurring during the trials. In conclusion, Cuban policosanol is a safe and effective natural drug for ischemic stroke treatment, which is supported by preclinical and clinical evidences.
Ischemic stroke is a cerebrovascular disease that occurs as a complication of atherosclerosis and consists of a sudden neurological deficit due to disorders in cerebral blood circulation [1]. Stroke is the second cause of death worldwide, being also one of the main causes of dementia, being both of them among the main risk factors for disability [2, 3].
Although ischemic stroke has a multifactorial etiology, its most common cause is the drastic decrease in oxygen and glucose in the brain due to the occlusion of a blood vessel by a thrombus, leading to a neurological deficit associated with ischemic damage to hippocampal cornu ammonis (CA) 1 pyramidal neurons [4, 5]. Furthermore, the release or activation of free radicals, as well as eicosanoids, inflammation, immune response, and lipid degradation products, are involved in its pathogenesis, which act after primary ischemic damage, either sequentially or in parallel, to cause cell death [6, 7].
Taking into account that according to epidemiological data each year 16.9 million people have an ischemic stroke and that the size and aging of the world population is growing progressively, the stroke global burden is increasing intensely [8]. For this reason, primary prevention (adoption of preventive measures in the adult population with risk factors) is the principal strategies to relieve this substantial burden. In this sense, the control of arterial hypertension, diabetes, hypercholesterolemia and obesity, the cessation of smoking, the reduction of alcohol consumption and the practice of systematic physical activity are key aspects [9].
Nevertheless, when an ischemic stroke or transient ischemic attack (TIA) occurs, patients have a high risk of having another stroke. Then, secondary stroke prevention is very important to prevent stroke recurrence and improve the neurological recovery of the patient. An adequate secondary stroke prevention strategy includes use of pharmacological therapy, in which antiplatelet agents constitute the first-line options, being aspirin, clopidogrel, or a combination of aspirin with dipyridamole the most widely used. However, to date, this type of agent has only achieved a moderate reduction in the recurrence of ischemic strokes and they produce adverse events associated with bleeding of greater or lesser amounts [10].
Additionally, the secondary prevention strategy includes the use of hydroxymethyl glutaryl coenzyme A reductase inhibitors [11], as well as neuroprotectants [12], and antioxidants [13], although these last two with less evidence of their benefits in clinical practice. Likewise, the use of hypotensive drugs in patients with blood pressure higher than 140/90 mmHg (× 0.13332 as conversion factor to kPa) is recommended, within which angiotensin-converting enzyme inhibitors, calcium channel blockers, and diuretics are the choice drugs [14].
Broadly, pharmacological therapies used in the secondary stroke prevention have not achieved clinical efficacy relevant, to the time they present adverse effects that limit their consumption [15, 16]. Therefore, the development of new substances to prevent and/or treat ischemic stroke continues to be a current line of research.
Cuban policosanol is obtained and purified from sugarcane wax (Saccharum officinarum L.), being constituted by a natural mixture of eight high molecular weight aliphatic alcohols where 1-octacosanol is its major component (60–70%), followed by 1-hexacosanol (3–10%), 1-triacontanol (10–15%) and 1-dotriacontanol (5–10%). Other alcohols are also important minor components of the product, such as: 1-tetracosanol, 1-heptacosanol, 1-nonacosanol and 1-tetratriacontanol [17]. It has lipid-lowering [18–22], antiplatelet [23], antioxidant [24] and vascular endothelium protective [25] properties, all of which give it a comprehensive anti-atherosclerotic effect (Figure 1). In addition, policosanol didn’t affect coagulation process neither bleeding time [26], presenting at the same time a good safety and tolerability profile [27–30].
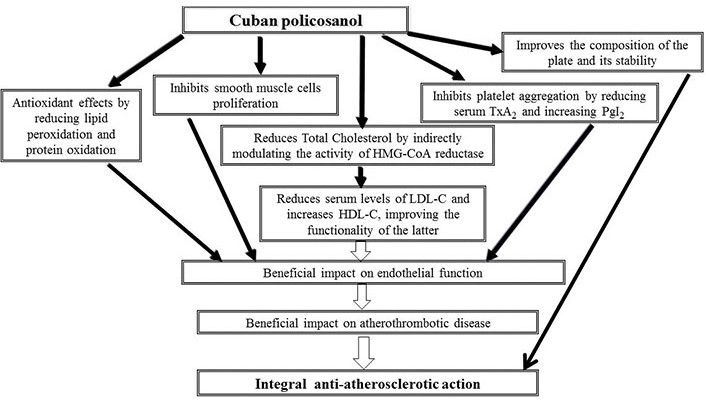
Multifactorial mechanism of action of Cuban policosanol. TxA2: thromboxane A2; PgI2: prostacyclin; HMG-CoA: 3-hydroxy-3-methylglutaryl-CoA; LDL-C: low density lipoprotein-cholesterol; HDL-C: high density lipoprotein-cholesterol
It is worth highlighting that the good safety and tolerability of Cuban policosanol constitutes an advantage demonstrated in the different clinical trials carried out in both young adults and middle-aged and elderly subjects. To this end, phase I clinical trials were first conducted in healthy volunteers, where Cuban policosanol did not modify the clinical or biochemical safety variables, nor was its administration related to the occurrence of adverse events [27, 28]. Likewise, the subsequent trials carried out in patients (phases II and III) did not show adverse effects associated with treatment with Cuban policosanol, nor did they modify the clinical or biochemical safety indicators [20–23, 29, 30]. Thus, as a whole, all clinical trials demonstrated that Cuban policosanol has a very good safety and tolerability profile.
Since anti-platelets drugs are useful for treating stroke it was logical expect that policosanol with proven anti-platelets effects could present protective effects on cerebral ischemia. For this reason, different experimental studies were carried out to evaluate the effects of policosanol in different experimental models of stroke and subsequently policosanol was evaluated in patients with stroke in clinical trials. For that, the objective of this review is to show, analyze and discuss the main preclinical and clinical evidence of the effects of Cuban policosanol on ischemic stroke.
The evaluation of Cuban policosanol on different experimental models of ischemic stroke was carried out in adult Mongolian gerbils (Meriones unguiculatus), since it is a very sensitive species, given by the fact that it lacks of the posterior communicating arteries in the Willis’s polygon in 60% of the animals [31], which justifies its use as a classical experimental model, widely used for the evaluation of new therapeutic candidates for ischemic stroke [32]. The main findings regarding the effects of Cuban policosanol in different experimental models of ischemic stroke are shown here and then summarized in Table 1.
Major findings of the preclinical evidences of Cuban policosanol on stroke
| Author | Year | Animal model | Dosing mode | Major findings |
|---|---|---|---|---|
| Arruzazabala et al. [33] | 1993 | Permanent ligature of a carotid in Mongolian gerbils | Preventive single oral doses (25 mg/kg, 50 mg/kg, and 200 mg/kg) | Cuban policosanol reduced clinical symptoms and mortality, associated to a TxA2 reduction and PgI2 increase |
| Preventive single oral doses of policosanol (25 mg/kg) plus aspirin (30 mg/kg) | This combination was more effective than the respective monotherapies on clinical symptoms and mortality, showing a synergism between them | |||
| Molina et al. [35] | 1999 | Permanent ligature of a carotid in Mongolian gerbils | Therapeutic single oral doses (100 mg/kg and 200 mg/kg) | Cuban policosanol (200 mg/kg) reduced clinical symptoms and mortality; and also it protected against brain histological damage |
| Bilateral ischemia and reperfusion in Mongolian gerbils | Therapeutic single oral doses (200 mg/kg) | Cuban policosanol reduced edema and restored AMPc levels in cerebral tissue | ||
| Molina et al. [40] | 2013 | Bilateral ischemia and reperfusion in Mongolian gerbils | Preventive single oral doses of Cuban policosanol and GSE (100 mg/kg and 200 mg/kg) | Both treatments inhibited similarly the hyper-locomotion, brain histological damage and plasma oxidative markers |
| Molina et al. [43] | 2015 | Bilateral ischemia and reperfusion in Mongolian gerbils | Preventive oral doses of Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) during 4 weeks | Both treatments prevented global cerebral ischemia with similar efficacy on hyper-locomotion and plasma oxidative markers, but being policosanol more effective on histological damage score |
| Molina et al. [44] | 2017 | Bilateral ischemia and reperfusion in Mongolian gerbils | Therapeutic oral doses of Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) during 7 days | Both treatments reduced global cerebral ischemia with similar efficacy on neurological symptoms score and plasma oxidative markers, but being policosanol more effective on brain histological damage score |
| Molina et al. [45] | 2013 | Bilateral ischemia and reperfusion in Mongolian gerbils | Therapeutic single oral doses of Cuban policosanol (100 mg/kg and 200 mg/kg) and atorvastatin (10 mg/kg and 20 mg/kg) | Both treatments reduced global cerebral ischemia with similar efficacy on neurological symptoms score, hyper-locomotion and brain histological damage score. Cuban policosanol produced antioxidant effects, unlike atorvastatin that did not modify it |
| Molina et al. [46] | 2018 | Bilateral ischemia and reperfusion in Mongolian gerbils | Single therapeutic doses of Cuban policosanol (100 mg/kg) plus aspirin (60 mg/kg), Cuban policosanol (100 mg/kg) plus atorvastatin (20 mg/kg) and aspirin (60 mg/kg) | Both combinations reduced similarly clinical symptoms, hyper-locomotion and histological damage, but with a major efficacy respect to aspirin monotherapy |
Focal cerebral ischemia was induced by permanent ligature of a carotid in Mongolian gerbils, producing clinical symptoms characterized by circling behavior and rolling fits. Two hours before stroke induction, single oral doses of Cuban policosanol (25 mg/kg, 50 mg/kg and 200 mg/kg) were administrated to the animals. Here, the gerbils of the control group, that only received the vehicle orally, presented clinical symptoms in 55% of the total number of their animals, while mortality was 33%. Although policosanol reduced clinical symptoms by up to 22% (vs. 55%), the comparison with the control group did not reach statistical significance. Indeed, a highlighted result here obtained was that the highest dose of policosanol tested (200 mg/kg) significantly and totally reduced mortality to 0 [33].
These findings were accompanied by a reduction in TxA2 concentrations in animals treated with Cuban policosanol at all doses tested, and by an increase in serum PgI2 with the doses of 200 mg/kg dose [33].
TxA2 and PgI2 are arachidonic acid metabolites with opposite effects. TxA2 is a potent vasoconstrictor and platelet pro-aggregator, while PgI2 is a vasodilator and antiplatelet agent. Thus, an adequate TxA2/PgI2 balance is very important for the maintenance of vascular hemostasis. In fact, an imbalance in PgI2 or TxA2 production is associated with the pathophysiology of atherosclerosis and their complications as ischemic stroke, being recently considered that high concentration of TxA2 may be a risk factor for ischemic stroke [34]. Therefore, the fact that Cuban policosanol exerted a favorable effect on this TxA2/PgI2 ratio represents an advantage in maintaining adequate hemostasis and in preventing a higher risk of ischemic stroke occurrence.
The possible interaction of the Cuban policosanol with aspirin was investigated in a second experimental series, since the last one constitutes the first line of treatment for ischemic stroke.
The results of the joint administration of policosanol and aspirin at ineffective doses (25 mg/kg and 30 mg/kg, respectively) showed a synergism between the two, since this combination significantly reduced the clinical symptoms and mortality, not only compared with the control group but also with each monotherapy separately [33].
Thus, both high-dose of Cuban policosanol (200 mg/kg) and combination of low-doses of policosanol (25 mg/kg) and aspirin (30 mg/kg), were effective in protecting against a cerebral ischemia in Mongolian gerbils induced by carotid artery ligation. This result constituted the first preclinical evidence of the anti-stroke efficacy of policosanol and its combination with aspirin, being the starting point for subsequent investigations related to the evaluation of policosanol on ischemic stroke.
Given these results, it was interesting to evaluate the effects of policosanol in this same model, but being administered after induction of ischemia, by determining not only clinical symptoms and mortality but also the histological analysis of brain.
For this, Cuban policosanol (100 mg/kg and 200 mg/kg) was administered orally and immediately after unilateral carotid ligation, each 12 h or 24 h intervals thereafter during 48 h. Here, only the highest tested dose of 200 mg/kg was effective for significantly reducing both clinical symptoms and mortality in both intervals of regimen of administration. The results of the histological study corresponded to those of the aforementioned behavioral study. In this regard, the highest dose of policosanol tested (200 mg/kg) significantly reduced swelling (tissue vacuolation) and necrosis of neurons in all brain areas studied (frontal cortex, hippocampus, striatum, and olfactory tubercle) compared to the control group [35].
Therefore, preventive and therapeutic oral treatment with policosanol at 200 mg/kg presents anti-ischemic effects in Mongolian gerbils with cerebral ischemia induced by unilateral and permanent ligation of a carotid artery.
Bilateral clamping and recirculation of both common carotid arteries in Mongolian gerbils constitutes another classical experimental model of ischemic stroke, characterized by hypoxia or blood flow disruption periods to the brain, which provokes behavioral and neuronal function disorders, supported by cerebral edema, wherein cyclic nucleotides [cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate play (cGMP)] play an important role [36].
After 15 min of carotids clamping and 4 h of recirculation, the control animals presented edema and cAMP levels drop in brain, unlike sham-operated or healthy animals. Orally administered Cuban policosanol (200 mg/kg) immediately after recirculation significantly reduced edema and restored cAMP levels in cerebral tissue compared to control group [35].
It has been described that during the blood recirculation process what follows ischemia there is a considerable increase in the free radical’s and reactive oxygen species generation, which contributes to the blood-brain barrier breakdown, and this in turn leads to impaired adenylate cyclase activity [36], and in correspondence with it, antioxidant substances prevent ischemic stroke and adenylate cyclase damage [37].
In previous studies Cuban policosanol exhibited antioxidant effects by inhibiting lipid peroxidation in different experimental models [38, 39]. So, the protective effect of Cuban policosanol in models of experimentally induced ischemic stroke was associated with its antiplatelet and antioxidant effects, which in turn were related to the observed decrease in the formation of TxA2 and malondialdehyde (MDA), respectively.
Taking into account the efficacy of policosanol in preventing cerebral ischemia induced by bilateral occlusion of both carotids and its reperfusion (ischemia-reperfusion), it was interesting to compare such effects with other anti-ischemic agents.
The effects of Cuban policosanol on global cerebral ischemia were compared with grape seed extract (GSE) in Mongolian gerbils, for what the two carotids of the animals were closed for 5 min, after which recirculation was restored for 24 h [40].
This experimental model is characterized by locomotor hyperactivity several hours after reperfusion, with a peak 24 h after the insult, so hyper-locomotion represents a predictive indicator of hippocampal damage, while CA1 region selective hippocampal injury occurs [41].
Both single oral doses of Cuban policosanol and GSE (100 mg/kg and 200 mg/kg), administered to gerbils 2 h before ischemia induction, prevented cerebral ischemia induced by 5 min of occlusion of both carotids and 24 h of recirculation, by significantly inhibiting hyper-locomotion (– 100% of inhibition) and the histological scores (– 60% of inhibition) with a similar efficacy [40].
In addition, the reoxygenation process that occurs during the reperfusion after ischemia, generates an excess in the production of reactive oxygen species with the consequent lipid peroxidation and protein oxidation, whose extension can be evaluated by the quantification in brain tissue of its corresponding markers such as MDA and sulfhydryl groups (SHG) associated with protein, respectively [42].
Cuban policosanol and GSE significant and similarly lowered MDA and SHG plasma levels in Mongolian gerbils with global cerebral ischemia induced by bilateral ischemia/reperfusion injury [40].
This study concluded that pre-treatment with single oral doses of Cuban policosanol and GSE similarly attenuated the ischemia/reperfusion-induced neurological injury and hyperlocomotion, and also reduced increased levels of plasma oxidative markers in gerbils with global cerebral ischemia [40].
Preventive and therapeutics effects of Cuban policosanol on global cerebral ischemia were compared with omega-3 fish oil in Mongolian gerbils with 5 min of bilateral carotids clamping (ischemia) and 24 h of reperfusion [43, 44].
The study with the preventive administration scheme compared the effects of 4 weeks’ oral daily administration of Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) on global cerebral ischemia, which was induced 1 h after the last administration. The results showed that clinical symptoms score, hyper-locomotion, and hippocampus histological damage were significantly reduced in animals treated with Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (2.5 g/kg) [43].
The comparative analysis between policosanol and omega-3 fish oil on the behavioral variables did not show significant differences, although policosanol was effective from the lowest dose tested of 100 mg/kg, unlike omega-3 fish oil, which only reached statistical significance to reduce clinical symptoms score and hyper-locomotion at the highest dose tested of 2.5 g/kg, which indicates a greater potency of policosanol [43].
The comparative analysis between policosanol and omega-3 fish oil on the histological score of brain damage showed significant differences between both treatments, obtaining greater potency and efficacy with policosanol on this histological variable [43]. Moreover, policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) markedly and significantly reduced MDA and SHG plasma levels, with a similar efficacy [43].
So, the conclusions of this prevention comparative study showed that both Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) orally administered during 4 weeks prevented global cerebral ischemia in Mongolian gerbils, with greater potency of policosanol and similar efficacy on neurological and oxidative stress variables, but being policosanol more effective on cerebral histological damage [43].
Taking into account the results of this preventive study, it was interesting to carry out a comparative study of its therapeutic effects [44]. For that, Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) were orally administered to Mongolian gerbils with global cerebral ischemia, starting at an hour of starting the reperfusion and continuing its administration during 7 days [44].
Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg) significantly and similarly reduced neurological symptoms score measured at 1 day, 3 days and 7 days after bilateral ischemia induction. However, the efficacy achieved with the therapeutic treatment of policosanol to protect against histological damage in brain was greater to that of omega-3 fish oil, since the first one at 100 mg/kg and 200 mg/kg significantly decreased the histological score (35.9% and 43.9% of inhibition, respectively), lowering cell depletion and picnosis of the cells, while omega-3 fish oil only was effective at 2.5 g/kg producing a modest and significant reduction (19.9%). Moreover, policosanol and omega-3 fish oil at doses assayed significantly and markedly reduced MDA and SHG plasma concentrations with a similar efficacy, although the inhibition percentages achieved with policosanol were slightly higher [44].
As it could be observed, the study that evaluated the therapeutic dose scheme demonstrated greater efficacy with the treatment with Cuban policosanol compared to omega-3 fish oil to protect against global cerebral ischemia induced in Mongolian gerbils. This result was similar to that obtained in the comparative study of both substances with the preventive dose scheme, in such a way that it confers a potential value to Cuban policosanol for its preventive and therapeutic use in the treatment of ischemic stroke.
So, the conclusions of this therapeutic comparative study showed that both Cuban policosanol (100 mg/kg and 200 mg/kg) and omega-3 fish oil (1.25 g/kg and 2.5 g/kg), orally administered during 7 days, protected from global cerebral ischemia in Mongolian gerbils, showing a greater efficacy with the Cuban policosanol [44].
A comparative study of the therapeutics effects of the Cuban policosanol vs. atorvastatin was performed in Mongolian gerbils with global cerebral ischemia [45], for which both carotids were clamped during 5 min and after that the recirculation was reestablished 24 h. The treatments with Cuban policosanol (100 mg/kg and 200 mg/kg) and atorvastatin (10 mg/kg and 20 mg/kg) were given as single oral doses at 4 h after the start of reperfusion [45].
Both treatments were similarly effective to lower clinical symptom score, and hyper-locomotion, although only policosanol reduced the frequency of animals that presented such symptoms [45].
All doses assayed of the Cuban policosanol and atorvastatin significantly decreased the histological scores, being mild-to-moderate (< 50%), excepting the highest dose of policosanol (66% reduction of the neuronal damage) [45].
According to previous results, Cuban policosanol produced antioxidant effects by significantly reducing serum concentrations of MDA and SHG in Mongolian gerbils with global cerebral ischemia, unlike atorvastatin that did not modify these oxidative variables [45].
In conclusion, this study demonstrated that therapeutic single oral doses of Cuban policosanol were effective in protecting against global cerebral ischemia in Mongolian gerbils comparable to atorvastatin, improving behavioral parameters such as reducing neurological score and hyperlocomotion, and also reducing histological brain damage. However, Cuban policosanol presented an advantage over atorvastatin, due to its effectiveness in reducing lipid peroxidation and protein oxidation [45].
Combinations of Cuban policosanol plus aspirin and Cuban policosanol plus atorvastatin were compared with each other and with respect to aspirin monotherapy in the global cerebral ischemia model in Mongolian gerbils [46]. For this, Mongolian gerbils underwent bilateral carotid ligation for 5 min and 24 h reperfusion, which were orally administered with single doses of Cuban policosanol (100 mg/kg) plus aspirin (60 mg/kg), Cuban policosanol (100 mg/kg) plus atorvastatin (20 mg/kg) and aspirin (60 mg/kg) at 4 h after reperfusion started [46].
Both combinations reduced clinical symptoms, hyper-locomotion and CA1-pyramidal cells region histological damage in Mongolian gerbils with ischemia/reperfusion-induced global cerebral ischemia, with a similar efficacy between them, but with advantage compared to aspirin monotherapy. The study on oxidative variables demonstrated the efficacy of the two combinations in markedly and significantly reducing MDA and SHG serum concentrations, unlike aspirin therapy, the which did not change these variables [46].
Thus, the conclusions of this study exposed the similar efficacy of the combinations Cuban policosanol plus aspirin and Cuban policosanol plus atorvastatin to protect against global cerebral ischemia in Mongolian gerbils, being both combinations slightly more effective than aspirin monotherapy. Added to this is the fact that the two combinations had antioxidant effects, unlike aspirin alone, which represents an additional benefit [46].
In order to corroborate the anti-ischemic stroke effects of Cuban policosanol obtained from preclinical studies different clinical trials were done. The main findings of the clinical studies evaluating the effects of Cuban policosanol on stroke are shown here and then summarized in Table 2.
Major findings of the clinical evidences of Cuban policosanol on stroke
| Author | Year | Study population | Dose | Major findings |
|---|---|---|---|---|
| Ortega et al. [47] | 2006 | Fifty patients who have suffered ischemic stroke | Cuban policosanol (20 mg/day) was administered during the acute phase and 5 years after the ischemic stroke | Cuban policosanol improved neurological recovery and prevented the recurrence of new vascular events. Treatment was well tolerated |
| Sánchez et al. [48] | 2010 | Fifty-five patients with previous TIA | Cuban policosanol (20 mg/day) plus aspirin (125 mg/day) during 5 years | Combination therapy improved neurological recovery and reduced recurrence of vascular events. Treatment was well tolerated |
| Sánchez et al. [49] | 2012 | Ninety-two patients who had suffered a recent moderate to severe ischemic stroke | Cuban policosanol (20 mg/day) plus aspirin (125 mg/day) compared to placebo plus aspirin 125 mg/day during 24 weeks | Combination therapy significantly improved the neurological score and reduced platelet aggregation with more efficacy than aspirin monotherapy. Unlike aspirin the combination produced antioxidant effect. Treatments were well tolerated |
| Sánchez et al. [52] | 2016 | Sixty patients that recently suffered an ischemic stroke 30 days after stroke onset | Cuban policosanol (20 mg/day) plus aspirin (125 mg/day) and atorvastatin (20 mg/day) plus aspirin (125 mg/day) for 12 weeks | Both combinations therapies improved similarly neurological recovery and prevented recurrent cerebrovascular events. Both combinations reduced cholesterol, with atorvastatin being more effective, unlike which policosanol increased HDL-C |
The first study where the effects of Cuban policosanol in patients with ischemic stroke were evaluated was carried out in a population of fifty patients. The trial was an observational pilot open study that investigated the effects of Cuban policosanol administration (20 mg/day) on neurological recovery during the acute phase and the 5 years after the ischemic stroke [47]. Cuban policosanol treatment improved the neurological score [assessed through the Canadian Neurological Scale (CNS)], no patient died, and 80% of patients did not experience new vascular events; only one (2.0%) suffered a new stroke, and two (4.0%) suffered more than one TIA. Policosanol also lowered serum total cholesterol (TC), while triglycerides (TG) were unchanged, and treatment being well tolerated [47].
This study demonstrated that concomitant administration of policosanol with aspirin and vitamins improves neurological outcomes and recurrent events in patients who have suffered ischemic stroke [47].
Given this result, a 60 months follow-up study was designed for 55 patients who suffered an ischemic stroke with a prior history of TIA, after hospital discharge. In this study, the neurological evolution of the patients was evaluated with the aim of demonstrating the usefulness of treatment with policosanol (20 mg/day) plus aspirin (125 mg/day) [48].
The results of this study were encouraging as the CNS neurological score improved significantly and progressively over the 5 years study period of all the patients involved in the study, only one suffered a new stroke (1.8%), four (7.3%) experienced a new TIA, and fifty patients (90.9%) did not experience a new vascular event. No patient died during the trial and no other serious adverse effects occurred [48].
Cuban policosanol (20 mg/day) plus aspirin (125 mg/day) combination therapy after three months significantly lowered serum TC (21.3%) compared with baseline, effect that was maintained and improved throughout the therapy until completing the study. The TC reduction correlated (r = 0.987) with the improvement of the neurological outcome. These results suggested that hypocholesterolemic effect of policosanol could be responsible, at least partially, for the protective effects on stroke. Also, TG lowered significantly compared with baseline after 12 months of therapy. Policosanol was very well tolerated [48].
This study concluded that the combined therapy policosanol 20 mg/day plus aspirin 125 mg/day, for 5 years, in patients who suffered an ischemic stroke and had a previous history of TIA, produced good results in the neurological recovery, recurrence of events and cholesterol control, which remarks its benefit in preventing the high risk of recurrent stroke in these patients after hospital discharge [48].
Nevertheless, in light of these results it could not yet be asserted that the benefits obtained on neurological recovery are entirely attributable to policosanol since the study did not include a control group treated with placebo plus aspirin, being an open and uncontrolled study, where all the patients consumed conventional therapy with aspirin. Therefore, randomized, double-blind, controlled studies were necessary.
The first randomized, double-blind, controlled study evaluating the effects of Cuban policosanol in patients who had suffered a recent ischemic stroke was conducted in ninety-two patients [49]. The evaluation of the improvement of the neurological result was carried out through a modified Rankin scale score (mRSs), in addition the effects on platelet aggregation were determined. The objective of the study was to compare the effects of the combined therapy policosanol 20 mg/day plus aspirin 125 mg/day with respect to placebo plus aspirin 125 mg/day. Cuban policosanol 20 mg/day plus aspirin 125 mg/day treatment significantly improved the neurological score (24.1%) by mRSs at week 6, not only compared with the baseline time but with respect to the placebo plus aspirin 125 mg/day group, and this combined treatment effect did not wear off, but improved significantly and progressively thereafter, at 12 weeks and 24 weeks (31% and 55%, respectively) [49].
Twelve weeks after randomization, policosanol 20 mg/day plus aspirin 125 mg/day, not placebo plus aspirin 125 mg/day, significantly decreased arachidonic acid-induced platelet aggregation (30.3%) compared to baseline value. At the end of the study (24 weeks) the combination therapy significantly reduced platelet aggregation induced by arachidonic acid and (41.0%) and adenosine diphosphate (24.8%) with respect to monotherapy aspirin [49].
The antiplatelet effects observed in this study, therefore, could be responsible, at least partly, for the benefits of policosanol 20 mg/day plus aspirin 125 mg/day therapy on stroke outcomes over the conventional aspirin monotherapy.
The benefits effects of combined therapy policosanol 20 mg/day plus aspirin 125 mg/day, respect to Placebo plus aspirin 125 mg/day, on lipid profile were also evaluated. The combined therapy significantly decreased serum TC and LDL-C levels during 24 weeks’ study, and increased HDL-C values compared to baseline and relative to placebo plus aspirin group [49].
During the study drug compliance was similar in both groups and very good (90%) and no reports of recurrent cerebrovascular event or any other major vascular event patients [49].
These results demonstrate that treatment with Cuban policosanol 20 mg/day plus aspirin 125 mg/day improves neurological recovery compared with placebo plus aspirin 125 mg/day (conventional therapy), while decreasing platelet aggregation in stroke patients with recent ischemic disease, suggesting the utility of concomitant treatment of both drugs as soon as after hospital discharge [49].
However, since it is the first randomized, double-blind, controlled clinical study that demonstrated the greater efficacy of the combination therapy of Cuban policosanol with aspirin on recovery from ischemic stroke, it was necessary to carry out subsequent studies to corroborate such results and allow further study of these effects.
In light of this background, the effects of therapy with Cuban policosanol 20 mg/day plus aspirin 125 mg/day, compared with placebo plus aspirin 125 mg/day, on neurological recovery (assayed by mRSs) and plasma oxidative endpoints in sixty patients who had a recent ischemic stroke were investigated. Thus, after 6 weeks of treatment with Cuban policosanol 20 mg/day plus aspirin 125 mg/day the neurological score measured by mRSs was significantly improved (28.6%) compared to placebo plus aspirin 125 mg/day. This effect did not disappear but continued to improve throughout the study, reaching 39.3% and 59.9% at 12 weeks and 24 weeks, respectively [49].
The evaluation of the oxidative variables showed that the combination policosanol 20 mg/day plus aspirin 125 mg/day significantly reduced the plasma concentrations of MDA and SHG, while increasing the plasma total antioxidant capacity in comparison with the basal values and with the placebo plus aspirin 125 mg/day group. The placebo plus aspirin 125 mg/day treatment did not modify the oxidative variables [49].
The favorable modification on the oxidative variables exerted by the addition of Cuban policosanol to standard therapy with aspirin constitutes an additional benefit in the recovery from ischemic stroke, based on the evidence that the redox imbalance plays a fundamental role in the early activation of damage at the endothelial level in patients with stroke, leading to even increased risk of recurrent stroke or other vascular events [50].
Consistent with all previous studies policosanol 20 mg/day plus aspirin 125 mg/day produced beneficial effects on the lipid profile, as it significantly reduced LDL-C and TC, while it increased HDL-C [49].
During the study, no patient had a recurrent cerebrovascular event or any other major vascular event, this being a valid result as treatment compliance was 90%. This double-blind, randomized, controlled study confirmed that combination therapy with Cuban policosanol 20 mg/day plus aspirin 125 mg/day significantly improved the functional outcomes of stroke, while demonstrating for the first time the beneficial effects of this combination therapy on plasma oxidative variables in patients who had recently suffered a moderate to severe ischemic stroke.
Considering, considering the usefulness and use of statin therapy to reduce the risk of stroke recurrence in patients who have suffered an ischemic stroke [51], it was of interest to compare the effects of Cuban policosanol with atorvastatin in patients who have suffered an ischemic stroke. With this objective, a comparative study was designed with sixty patients that recently suffered an ischemic stroke, who received Cuban policosanol (20 mg/day) or atorvastatin (20 mg/day) for 12 weeks, all of whom were also treated with aspirin (125 mg/day), in order to compare the effects of both of these treatments on neurological outcome [assessed through mRSs and Barthel Index (BI)] [52].
Combinations of Cuban policosanol (20 mg/day) plus aspirin (125 mg/day) and atorvastatin (20 mg/day) plus aspirin (125 mg/day) improved neurological recovery in ischemic stroke patients, as measured by both mRSs and BI, the stroke functional outcome being similar between both combination therapies [52].
The quantification of the lipid profile showed a significant reduction in the serum concentrations of TC and LDL-C, both with the combination of Cuban policosanol plus aspirin and with that of atorvastatin plus aspirin, although the latter achieved a higher efficacy. However, serum HDL-C concentrations only increased significantly with the Cuban policosanol plus aspirin combination, but not with atorvastatin [52].
Drug compliance was similar between both groups (90%), without any patient presenting recurrent cerebrovascular events or other major vascular events. All treatments were safe and well tolerated [52].
The conclusions of this clinical trial exposed that 12 weeks’ administration of the combinations Cuban policosanol (20 mg/day) plus aspirin (125 mg/day), and atorvastatin (20 mg/day) plus aspirin (125 mg/day) significantly and similarly improved the functional outcome in stroke patients with 30 days after stroke onset [52].
The preclinical evaluation of Cuban policosanol in different experimental models of ischemic stroke in Mongolian gerbils demonstrated its anti-ischemic efficacy both in preventive and therapeutic dose schedules, being similar or superior to other anti-ischemic agents. Also, combination therapy with aspirin produced greater anti-stroke efficacy compared with aspirin monotherapy, but was similar to policosanol plus atorvastatin combination. Clinical evaluation of Cuban policosanol in open studies, and in randomized, double-blind, controlled studies performed in patients with previous ischemic stroke showed that policosanol combined with aspirin (standard therapy) improves and benefits the functional and neurological outcome of these patients. Cuban policosanol was safe and well tolerated, with no serious adverse events occurring during the trials. Therefore, the clinical evidences confirmed the preclinical evidences on the protective and anti-stroke effects of Cuban policosanol.
Preclinical and clinical evidence supports the anti-stroke efficacy of Cuban policosanol, a natural drug with an excellent safety and tolerability profile, with its combination with aspirin being a good alternative for the treatment of patients suffering from ischemic stroke.
cAMP: cyclic adenosine monophosphate
CA: cornu ammonis
GSE: grape seed extract
HDL-C: high density lipoprotein-cholesterol
LDL-C: low density lipoprotein-cholesterol
MDA: malondialdehyde
mRSs: modified Rankin scale score
PgI2: prostacyclin
SHG: sulfhydryl groups
TC: total cholesterol
TIA: transient ischemic attack
TxA2: thromboxane A2
VMC: Conceptualization, Writing—original draft, Writing—review & editing. AOY: Writing—original draft, Writing—review & editing.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 6123
Download: 49
Times Cited: 0
Mihai Andrei Ruscu ... Aurel Popa-Wagner
Chaitanya Sanghadia ... Brandon Lucke-Wold
Divya Sharma, Rahul Kumar
Lorena Dellagnesi Depieri ... Lorena Souza Viana
Ana-Maria Dobri-Nicoară ... Cristiana Tanase
