 Original Article
Original Article

Affiliation:
1Northwell, Manhasset, NY 11030, United States
2Institute of Health System Science, Feinstein Institutes for Medical Research, Manhasset, NY 11030, United States
Email: markbutler@northwell.edu
ORCID: https://orcid.org/0000-0003-4359-2897
Affiliation:
1Northwell, Manhasset, NY 11030, United States
2Institute of Health System Science, Feinstein Institutes for Medical Research, Manhasset, NY 11030, United States
Affiliation:
1Northwell, Manhasset, NY 11030, United States
2Institute of Health System Science, Feinstein Institutes for Medical Research, Manhasset, NY 11030, United States
ORCID: https://orcid.org/0000-0002-0102-1263
Affiliation:
3Department of Orthopedics, Johns Hopkins School of Medicine, Baltimore, MD 21205, United States
ORCID: https://orcid.org/0000-0001-8645-2363
Affiliation:
4Mailman School of Public Health, Columbia University, New York, NY 10032, United States
ORCID: https://orcid.org/0000-0001-8530-035X
Affiliation:
1Northwell, Manhasset, NY 11030, United States
2Institute of Health System Science, Feinstein Institutes for Medical Research, Manhasset, NY 11030, United States
ORCID: https://orcid.org/0000-0003-4206-0979
Explor Med. 2026;7:1001402 DOI: https://doi.org/10.37349/emed.2026.1001402
Received: January 30, 2026 Accepted: March 26, 2026 Published: May 11, 2026
Academic Editor: Sverre E. Kjeldsen, University of Oslo, Norway
The article belongs to the special issue Drug Adherence in Hypertension
Aim: Adherence to antihypertensive medication is essential for positive outcomes among patients diagnosed with hypertension. Yet, up to 72% of individuals prescribed antihypertensives do not take medication as prescribed. Understanding mechanisms of behavior change (MoBCs) for antihypertensive adherence provides essential insight for how to change adherence behavior. This study examined the association between 4 potential MoBCs and self-reported antihypertensive adherence.
Methods: This exploratory, cross-sectional study recruited 101 patients prescribed antihypertensive medications to complete self-report questionnaires on adherence and potential mechanisms of nonadherence. Antihypertensive adherence was assessed using the Hill-Bone Compliance to High Blood Pressure Therapy Scale (HB-HBP). The 4 putative MoBCs for nonadherence included self-efficacy, self-regulation, behavioral automaticity, and hypertension knowledge. Associations between self-reported antihypertensive adherence and MoBCs were examined using independent samples t-tests and multivariate median regression with covariate adjustment for participant characteristics.
Results: The sample had a mean age of 61.7 years (SD = 13.1 years), was 59.4% female (n = 60), 66.3% White (n = 67), and 7.9% Hispanic (n = 8). Low adherence was reported by 16.8% of the study sample. Participants who reported low adherence to antihypertensive medications had lower scores on the self-efficacy questionnaire (p < 0.001) and hypertension knowledge (p = 0.045). Self-efficacy and hypertension knowledge remained significantly associated with self-reported adherence in multivariate regression with covariate adjustment.
Conclusions: The current study supports the hypothesis that self-efficacy for adherence and additionally hypertension knowledge are the MoBCs most strongly associated with self-reported adherence behavior. Behavioral interventions to improve medication adherence should consider focusing on self-efficacy and hypertension knowledge as potentially important target MoBCs. The authors recommend that future research should consider tailored intervention approaches that target specific mechanisms of adherence and specific self-reported reasons for nonadherence.
Roughly half of deaths in the United States can be attributed to individual health behaviors, such as low physical activity, smoking, and diet [1, 2]. Of these deaths, nearly a quarter are attributable to hypertension (HTN) or cardiovascular disease (CVD) [3–5]. One of the most important health behaviors for the treatment of HTN and prevention of CVD is adherence to antihypertensive medications [6–8]. Antihypertensive medications lower blood pressure, thereby decreasing the risk of CVD events [9–10]. Individuals who are adherent to antihypertensive medications have a 38% reduction in the hazard of incident CVD [7], while nonadherence (i.e., not taking medication as prescribed) is associated with a 48% increased hazard of all-cause mortality [11]. Despite the importance of antihypertensive medications, between 35% and 72% of individuals with HTN do not take their medication as prescribed [7, 12–15]. Nonadherence is associated with increased rates of CVD, hospitalization, healthcare utilization, and healthcare costs [16–18]. Despite many interventions aimed at improving adherence to antihypertensive medications, the persistence of nonadherence remains a significant and growing public health issue [19]. Meta-analyses examining interventions for antihypertensive medication adherence have found high levels of heterogeneous treatment effects [20–22], suggesting that there is significant variability in how an intervention improves adherence.
Understanding the mechanisms by which an intervention influences health behavior may help to better understand the cause of heterogenous treatment effects [23, 24]. Studying mechanisms of behavior change (MoBCs) provides powerful ways to identify how an intervention works, and not just whether it works. Current recommendations suggest that individually tailored medication adherence intervention approaches are more likely to be successful than ‘one size fits all’ approaches [19]. By identifying the underlying cause of nonadherence to antihypertensive medication (i.e., the MoBC), it is possible to directly act on the most important MoBC for an individual, thereby improving adherence behavior. However, in order to best explore mechanisms, trials must directly test mechanistic pathways [25]. Despite the potential importance of identifying and targeting mechanisms in interventions for medication adherence, only 3% of NIH-funded trials examine potential MoBCs [26]. This shows a critical lack of mechanistic research for behavioral interventions to improve medication adherence.
In this study, we aim to examine the associations between self-reported adherence to antihypertensive medications and potential MoBCs for increasing adherence in a large healthcare system with over 5.5 million patient contacts annually [27]. The goal of this study is to confirm that these hypothesized MoBCs are indeed associated with nonadherence. Further, we will use multivariate regression to examine the association between each MoBC and adherence, adjusting for all other MoBCs as well as patient characteristics. We will also examine self-reported reasons for nonadherence and explore how these are associated with both medication adherence and potential MoBCs. In doing so, we hope to validate and expand the existing research identifying the important mechanisms and correlates of adherence in this exploratory, cross-sectional study.
This is an exploratory, cross-sectional survey designed to explore the associations between self-reported adherence to antihypertensive medications and potential MoBCs for adherence (including self-efficacy, self-regulation, behavioral automaticity, and HTN knowledge). This was a fully remote trial. Participant consent and survey assessments were conducted using REDCap, an approved secure data collection tool [28, 29]. Participants were compensated $50 for participation. The protocol for this trial was approved by the Northwell Health Institutional Review Board in November 2024.
We recruited 101 participants who were prescribed antihypertensive medication. Inclusion criteria can be found in Table 1. Patients were required to be diagnosed with HTN, have a current prescription for antihypertensive medication, and have a recent outpatient contact between December 2023 and January 2025. We excluded non-English speaking individuals to improve the validity and reliability of all study measures (some of which have not been validated in other languages).
Inclusion/exclusion criteria.
| Inclusion criteria | Exclusion criteria |
|---|---|
A participant must meet the following criteria to be included in the study:
| A person who meets the following criteria will be excluded.
|
HTN: hypertension.
With support from the Northwell Health Quantitative Intelligence team, we utilized the electronic health record (EHR) to identify over 3,500 participants who were potentially eligible for the trial. These participants were contacted directly using the contact information provided in the EHR, namely email and phone number. Recruitment for the trial occurred between February and March of 2025. Potentially eligible patients were randomly selected and contacted via a brief email explaining the nature of the study and directing them to a REDCap survey with further information. The REDCap survey contained a more detailed overview of study requirements, a copy of the consent form for review, and contact information for study personnel.
Patients who indicated their interest in this REDCap survey were directed to a brief screening survey to confirm their current HTN diagnosis, that they are currently prescribed a hypertensive medication, and that they had contact with their provider between December 2023 and January 2025.
Individuals deemed ineligible for the study based on their responses to this survey were immediately notified through the REDCap software. Eligible individuals were automatically directed to a digital consent form to review and sign in REDCap.
Adherence to antihypertensive medication was measured using the Hill-Bone Compliance to High Blood Pressure Therapy Scale (HB-HBP) [30]. The HB-HBP is a 14-item survey measure scored on a 4-point Likert scale rated from 4 “None of the time” to 1 “All of the time”. The HB-HBP contains a 9-item subscale used to measure self-reported adherence to antihypertensive/high blood pressure medication. Questions asked “How often do you decide NOT to take your high blood pressure medication?” and “How often do you forget to get your prescriptions filled?” Scores were summed to generate a total score, with higher scores indicating better adherence. For the purposes of this analysis, individuals who scored below the lowest quartile cut-off point on the HB-HBP medication adherence subscale were defined as being nonadherent. The HB-HBP also contains two other scales related to high blood pressure therapy: 1) a 2-item scale measuring adherence to medical appointments and 2) a 3-item scale measuring dietary intake of salty foods. As these two other scales are associated with higher blood pressure levels and have shown good reliability/validity with the medication adherence sub-scale on the HB-HBP [30], these additional scales were also examined in exploratory analyses.
We have identified 4 potential MoBCs for the current study: self-efficacy, treatment self-regulation, behavioral automaticity, and HTN knowledge. Self-efficacy, defined as beliefs about one’s ability to successfully perform a behavior, has been identified as a key MoBC for many behavior change theories [31], and has been found to be integral to medication adherence [32–34], especially to antihypertensive medications [35]. Low medication adherence self-efficacy, defined as a low level of belief in an individual’s ability to consistently take medication as prescribed, is a potential modifiable reason for nonadherence. Self-regulation, defined as the ability of an individual to regulate their own behavior, is also a key MoBC for a variety of health outcomes [36], including medication adherence [37, 38]. Behavioral automaticity, defined as the degree to which an individual engages in a behavior automatically and without thinking [39, 40], has also been found to be associated with adherence to antihypertensives [41]. Behavioral automaticity is also more commonly known as “habit”, i.e., a behavior performed automatically. HTN knowledge is defined as an individual’s awareness of the symptoms of HTN, the potential consequences of HTN, and how HTN can be treated. Low levels of HTN knowledge about medications have previously been associated with nonadherence to antihypertensive medications [21, 42–44].
It should also be noted that these MoBCs are operationalized in particular manners, which may capture some aspects of the larger mechanistic theory and ignore others. For example, self-efficacy has multiple facets and can be operationalized in a variety of ways [45, 46]. The same is true of all potential MoBCs. How adherence and MoBCs will influence all potential interpretations of findings.
We measured self-efficacy using the Medication Adherence Self-Efficacy Scale Revised (MASES-R), a 13-item measure of medication adherence self-efficacy, previously used in a variety of populations to measure self-efficacy for adherence to antihypertensive medications [34, 47]. The MASES-R assesses individuals’ confidence in their ability to take their antihypertensive medication in a variety of situations, including when they are busy at home or not experiencing any symptoms. The final question assesses confidence in making medication-taking a part of the patient’s routine. Each item is scored from 1, “Not at all sure,” to 4, “Extremely sure.” Participants’ scores across the 13 items were averaged into a total score, with lower values (closer to 1) representing low self-efficacy, and higher values (closer to 4) representing high self-efficacy.
We assessed self-regulation using the Treatment Self-Regulation Questionnaire (TRSQ), a 15-item scale [48]. The questionnaire assesses different sources of motivation for disease self-management, with each potential reason scored on a 7-point Likert scale rated from “Not true at all” to “Completely true”. Each potential motivator was sorted into one of three categories: amotivation (defined as the absence of intention to act), controlled regulation (defined as internal or external pressure to engage in a behavior), and autonomous regulation (defined as feelings of volitional choice for engaging in the behavior) [48, 49]. An average score out of 7 for each of the three categories was calculated for each participant, with low scores corresponding to low levels of motivation in that category, and high scores corresponding to high motivation in that category.
We assessed behavioral automaticity, using the Self-Report Behavioral Automaticity Index (SRBAI) [40], a 4-item measure of the perceived automaticity of health behaviors, previously used for trials examining medication adherence. Questions on the SRBAI ask whether taking hypertensive medication is done automatically, done without consciously remembering, done without thinking, and started without realizing. Each of the items is assessed on a 7-point Likert scale from “Strongly disagree” to “Strongly agree”. Participants’ scores for each of the four questions were summed for a maximum of 28 points, with low scores corresponding to low levels of automaticity and high scores corresponding to high levels of automaticity.
We measured HTN knowledge, using a 10-item HTN knowledge scale [50], previously used in several trials to increase medication adherence and lower blood pressure. The survey asks questions assessing knowledge of what HTN is, ideal health behaviors for those diagnosed with HTN, and the medical consequences of HTN in a brief survey accessible to those with limited literacy. Each question was scored either one point for a correct answer or zero points for an incorrect answer, and each participant was then given a total score out of a total of 10 points, with higher scores indicating greater levels of HTN knowledge.
We also wanted to identify potential barriers to adherence to examine how these were associated with self-report adherence and potential MoBCs. Reasons for nonadherence were assessed using the Medication Adherence Reasons Scale Revised (MAR-revised) [51]. This 20-item scale first asks how many days out of the past 7 days the participant was able to take their medication exactly as prescribed. The other questions provide 19 different potential reasons for nonadherence and ask how many days out of the past 7 were each reason a cause of nonadherence. Each question is rated on a scale from “0 days” to “7 days”.
Potential reasons for nonadherence were grouped into five established categories: nonadherence due to beliefs and perceptions about their condition or medication, nonadherence due to side effects and concerns regarding the medication, nonadherence due to practical and access barriers to taking medication, forgetfulness or unintentional nonadherence, and intentional or contextual nonadherence. The average number of days that each category was responsible for a participant’s nonadherence was calculated. The categorical averages for participants in the high adherence group and the low adherence group were also compared in order to test for the association between adherence level and different nonadherence reasons.
A standardized demographics survey was administered that collected information on participant age, gender, race, ethnicity, primary language, and insurance status.
Analysis for the primary aim outcome: The primary aim for this study is to examine the associations between medication adherence measured using the HB-HBP and four potential MoBCs: Self-efficacy, treatment self-regulation, behavioral automaticity, and HTN knowledge. First, we compared scores on these measures between individuals with low adherence and high adherence using independent samples t-tests. Participant characteristics were also compared between low and high adherence groups using an independent samples t-test for continuous variables and Pearson Chi-squared tests for categorical variables. We then examined the association between MoBC scores and continuous HB-HBP adherence scores using median regression analysis. A median regression model was utilized to provide a more robust comparison due to the small sample size and potentially non-linear distribution of medication adherence. We utilized participant characteristics as covariates in these regression analyses. Finally, we conducted a multivariate median regression model with all MoBCs and covariates included to identify if any MoBCs are associated with self-reported antihypertensive adherence, controlling for all other MoBCs.
In addition, we compared scores on the MAR-revised between individuals with low adherence and high adherence using independent samples t-tests. We examined scores on the 5 different subscales for the MAR-revised: beliefs/perceptions, side effects, practical/access barriers, forgetfulness/unintentional nonadherence, and intentional/contextual nonadherence.
We also conducted Pearson correlation analyses between continuous HB-HBP scale scores (including medication adherence, appointment attendance, and sodium intake), MoBC measures, and MAR sub-scales. This was an exploratory analysis examining associations for future study. All analyses were conducted with R version 4.6.0 [52].
The sample of 101 participants had a mean age of 61.7 years (SD = 13.1 years), was 59.4% female (n = 60), 66.3% White (n = 67), 7.9% Hispanic (n = 8), and 99.0% insured (n = 100). Full sample characteristics can be found in Table 2. In the sample, there were 17 participants (16.8%) who self-reported low levels of adherence, defined by scoring ≤ 33 on the 9-item medication adherence scale of the HB-HBP (below the lowest cut-point for the lowest quartile). This score corresponds to either reporting taking medication “None of the time” on a single item or “Most of the time” on three items for the HB-HBP. Participants who self-reported low levels of adherence were younger, more likely to be female, and less likely to identify as White than those with high adherence (Table 2).
Participant characteristics by self-reported adherence status.
| Variable | Total sample (N = 101) | High adherence (N = 84) | Low adherence (N = 17) | p-Value | |
|---|---|---|---|---|---|
| Age: mean (SD) | 61.7 (13.1) | 63.2 (12.7) | 55.1 (13.8) | 0.034 | |
| Gender | Male | 40 (39.6%) | 38 (45.2%) | 2 (11.8%) | 0.004 |
| Female | 60 (59.4%) | 46 (54.8%) | 14 (82.4%) | ||
| Other | 1 (1.0%) | 0 (0.0%) | 1 (5.8%) | ||
| Hispanic | 8 (7.9%) | 8 (9.5%) | 0 (0.0%) | 0.405 | |
| Race | White | 67 (66.3%) | 62 (73.8%) | 5 (29.4%) | 0.001 |
| Black | 16 (15.8%) | 10 (11.9%) | 6 (35.2%) | ||
| American Indian | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| Asian | 13 (12.9%) | 9 (10.7%) | 4 (23.5%) | ||
| Pacific Islander | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| More than 1 | 2 (1.9%) | 1 (1.2%) | 1 (5.8%) | ||
| Other | 2 (1.9%) | 2 (2.4%) | 0 (0.0%) | ||
| Declined | 1 (0.9%) | 0 (0.0%) | 1 (5.8%) | ||
| Spanish primary language | 1 (0.9%) | 1 (1.2%) | 0 (0.0%) | 0.999 | |
| Insured | 100 (99.0%) | 84 (100.0%) | 16 (94.1%) | 0.373 | |
| Potential MoBC measures | |||||
| MASES | 3.19 (0.40) | 3.28 (0.28) | 2.68 (0.53) | < 0.001 | |
| TSRQ autonomous | 6.41 (1.20) | 6.48 (1.20) | 6.03 (1.17) | 0.176 | |
| TSRQ controlled | 3.50 (1.59) | 3.42 (1.66) | 3.91 (1.18) | 0.172 | |
| TSRQ amotivation | 3.02 (1.60) | 3.03 (1.60) | 3.00 (1.64) | 0.951 | |
| SRBAI | 22.08 (6.56) | 22.30 (6.74) | 20.80 (5.48) | 0.319 | |
| Hypertension knowledge | 7.98 (1.06) | 8.06 (1.09) | 7.56 (0.81) | 0.045 | |
| Barriers to adherence | |||||
| Medication Adherence Reasons | 6.64 (1.03) | 6.87 (0.37) | 5.44 (2.10) | 0.016 | |
p-Values generated using independent samples t-tests for continuous variables and Chi-squared tests for categorical variables; MASES: Medication Adherence Self-Efficacy Scale; TSRQ: Treatment Self-Regulation Questionnaire; SRBAI: Self-Report Behavioral Automaticity Index.
Comparisons of MoBC by adherence groups showed that individuals who self-reported low levels of adherence also reported lower scores on the MASES [mean (SD) = 2.68 (0.53)] relative to individuals with high levels of adherence [mean (SD) = 3.28 (0.28); independent sample t-test p < 0.001; Table 2]. Individuals with self-reported low levels of adherence also had lower scores on HTN knowledge than [mean (SD) = 7.56 (0.81)] relative to individuals with high levels of adherence [mean (SD) = 8.06 (1.09); independent sample t-test p = 0.045; Table 2]. The distribution of MoBC scores by adherence group can be found in Figure 1.
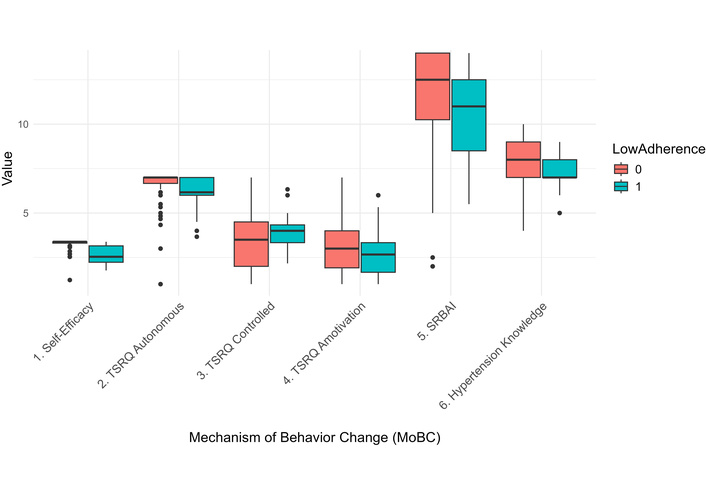
Boxplot of MoBCs by adherence status. TSRQ: Treatment Self-Regulation Questionnaire; SRBAI: Self-Report Behavioral Automaticity Index.
In regression analyses, self-efficacy was associated with continuous self-reported medication adherence scores on the HB-HBP in the unadjusted model [coefficient (95% CI) = 5.20 (4.51 to 7.55)], the covariate adjusted model [coefficient (95% CI) = 4.64 (3.43 to 7.49)], and the model adjusted for all other MoBCs [coefficient (95% CI) = 4.84 (3.30 to 7.37); Table 3]. HTN knowledge was also associated with continuous medication adherence in the unadjusted regression model [coefficient (95% CI) = 0.50 (0.22 to 1.51); Table 3] and remained significant in covariate-adjusted and multivariate models. This suggests that self-efficacy and HTN knowledge are uniquely associated with self-reported adherence after adjustment for covariates and other MoBCs. All other MoBCs were not significantly associated with continuous medication adherence scores at any level of adjustment.
Median regression models predicting self-reported adherence.
| Mechanism | Single predictor analyses without covariate adjustment | Single predictor analyses with covariate adjustment | Multivariable predictor analyses withcovariate adjustment | |
|---|---|---|---|---|
| Coefficient (95% CI) | Coefficient (95% CI) | Coefficient (95% CI) | ||
| Medication Adherence Self-Efficacy Scale (MASES) | 5.20 (4.51 to 7.55) | 4.64 (3.43 to 7.49) | 4.84 (3.30 to 7.37) | |
| Treatment Self-Regulation Questionnaire (TSRQ) | Autonomous | 0.50 (–0.18 to 0.96) | 0.45 (–0.01 to 0.73) | 0.00 (–0.05 to 0.02) |
| Controlled | 0.00 (0.00 to 0.00) | 0.00 (0.00 to 0.03) | 0.01 (–0.12 to 0.05) | |
| Amotivation | 0.00 (0.00 to 0.00) | 0.00 (0.00 to 0.06) | –0.01 (–0.03 to 0.09) | |
| Self-Report Behavioral Automaticity Index (SRBAI) | 0.00 (0.00 to 0.13) | 0.00 (0.00 to 0.07) | –0.00 (–0.03 to 0.01) | |
| Hypertension knowledge | 0.50 (0.22 to 1.51) | 0.21 (0.04 to 0.45) | 0.13 (0.01 to 0.21) | |
Participant characteristics in the single predictor and multiple predictor models included age at recruitment, gender, Hispanic ethnicity, and race.
Analysis of the associations between reasons for medication adherence and self-reported adherence was not statistically significant for independent samples t-tests (Table 4). However, in bivariate correlation analyses examining the association between continuous HB-HBP medication adherence scores and reasons for medication adherence, adherence was associated with participant beliefs (r = –0.20, p = 0.04), participant concerns about side effects (r = –0.31, p = 0.002), practical access barriers (r = –0.21, p = 0.04), and unintentional adherence/forgetfulness (r = –0.36, p < 0.001; Table 5). Only intentional reasons for nonadherence were not significantly associated with continuous HB-HBP scores. In addition, reasons for medication adherence were associated with medication adherence self-efficacy. For example, concerns about side effects were strongly negatively associated with self-efficacy (r = –0.48, p < 0.001; Table 5).
Association between adherence and Medication Adherence Reasons (MAR) Scale.
| Variable | High adherence (N = 84) | Low adherence(N = 17) | p-Value |
|---|---|---|---|
| MAR beliefs and perceptions; mean (SD) | 0.33 (2.12) | 1.06 (2.11) | 0.219 |
| MAR side effects and concerns; mean (SD) | 0.75 (2.29) | 2.69 (4.92) | 0.142 |
| MAR practical and access barriers; mean (SD) | 0.70 (4.16) | 2.81 (7.03) | 0.261 |
| MAR forgetfulness/unintentional nonadherence; mean (SD) | 0.67 (2.17) | 2.81 (4.93) | 0.106 |
| MAR intentional/contextual nonadherence; mean (SD) | 0.36 (1.62) | 0.25 (1.00) | 0.729 |
p-Values generated using independent samples t-tests.
Exploratory Pearson correlations between scales with 95% confidence intervals in parentheses.
| Variable | Hill-Bone medication adherence | Hill-Bone sodium | Hill-Bone missed appointments | MASES | TSRQ autonomous | TSRQ controlled | TSRQ amotivation | SRBAI | Hypertension knowledge | MAR beliefs and perceptions | MAR side effects and concerns | MAR practical and access barriers | MAR forgetful |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hill-Bone sodium | 0.32** (0.13 to 0.48) | - | - | - | - | - | - | - | - | - | - | - | - |
| Hill-Bone missed appointments | 0.28** (0.09 to 0.45) | 0.03 (–0.17 to 0.22) | - | - | - | - | - | - | - | - | - | - | - |
| MASES | 0.72*** (0.61 to 0.80) | 0.38*** (0.20 to 0.53) | 0.41*** (0.23 to 0.56) | - | - | - | - | - | - | - | - | - | - |
| TSRQ autonomous | 0.24* (0.05 to 0.41) | 0.12 (–0.08 to 0.31) | 0.17 (–0.03 to 0.35) | 0.39*** (0.21 to 0.54) | - | - | - | - | - | - | - | - | - |
| TSRQ controlled | –0.02 (–0.21 to 0.18) | –0.04 (–0.23 to 0.16) | 0.16 (–0.04 to 0.34) | 0.07 (–0.12 to 0.27) | 0.40*** (0.23 to 0.56) | - | - | - | - | - | - | - | - |
| TSRQ amotivation | 0.05 (–0.14 to 0.25) | –0.02 (–0.23 to 0.16) | 0.11 (–0.09 to 0.30) | 0.10 (–0.10 to 0.29) | 0.03 (–0.17 to 0.22) | 0.62*** (0.48 to 0.72) | - | - | - | - | - | - | - |
| SRBAI | 0.17 (–0.03 to 0.35) | 0.09 (–0.11 to 0.28) | 0.09 (–0.11 to 0.28) | 0.19 (–0.01 to 0.37) | 0.28** (0.09 to 0.45) | 0.37*** (0.19 to 0.53) | 0.23* (0.03 to 0.40) | - | - | - | - | - | - |
| Hypertension knowledge | 0.24* (0.05 to 0.42) | 0.16 (–0.04 to 0.34) | 0.06 (–0.13 to 0.26) | 0.16 (–0.04 to 0.34) | 0.08 (–0.11 to 0.27) | 0.09 (–0.10 to 0.28) | 0.05 (–0.15 to 0.24) | 0.06 (–0.14 to 0.25) | - | - | - | - | - |
| MAR beliefs and perceptions | –0.20* (–0.38 to –0.01) | –0.04 (–0.23 to 0.16) | –0.06 (–0.26 to 0.13) | –0.21* (–0.39 to –0.01) | –0.04 (–0.23 to 0.16) | 0.16 (–0.03 to 0.35) | 0.17 (–0.03 to 0.35) | 0.01 (–0.18 to 0.21) | 0.10 (–0.09 to 0.29) | - | - | - | |
| MAR side effects and concerns | –0.31** (–0.48 to –0.12) | –0.05 (–0.25 to 0.14) | –0.25* (–0.42 to –0.05) | –0.48*** (–0.62 to –0.31) | –0.07 (–0.26 to 0.12) | 0.14 (–0.05 to 0.33) | 0.04 (–0.16 to 0.23) | 0.07 (–0.13 to 0.26) | –0.02 (–0.22 to 0.18) | 0.64*** (0.51 to 0.74) | - | - | - |
| MAR practical and access barriers | –0.21* (–0.39 to –0.01) | –0.02 (–0.22 to 0.17) | 0.01 (–0.18 to 0.21) | –0.25* (–0.42 to –0.05) | –0.04 (–0.23 to 0.16) | 0.12 (–0.08 to 0.31) | 0.10 (–0.10 to 0.29) | –0.05 (–0.25 to 0.14) | 0.02 (–0.17 to 0.22) | 0.88*** (0.83 to 0.92) | 0.67*** (0.55 to 0.76) | - | - |
| MAR forgetfulness/unintentional nonadherence | –0.36*** (–0.52 to –0.18) | –0.22* (–0.40 to –0.02) | –0.09 (–0.28 to 0.10) | –0.30** (–0.47 to –0.11) | –0.14 (–0.33 to 0.05) | 0.08 (–0.12 to 0.27) | 0.10 (–0.10 to 0.29) | –0.12 (–0.31 to 0.08) | 0.00 (–0.19 to 0.20) | 0.67*** (0.54 to 0.76) | 0.54*** (0.38 to 0.66) | 0.68*** (0.56 to 0.77) | - |
| MAR intentional/contextual nonadherence | –0.06 (–0.26 to 0.13) | 0.03 (–0.17 to 0.23) | 0.09 (0.11 to 0.28) | –0.11 (–0.30 to 0.09) | –0.09 (–0.28 to 0.11) | 0.15 (–0.04 to 0.34) | 0.13 (–0.07 to 0.32) | 0.02 (–0.18 to 0.22) | –0.03 (–0.22 to 0.17) | 0.76*** (0.67 to 0.83) | 0.46*** (0.30 to 0.60) | 0.80*** (0.71 to 0.86) | 0.61*** (0.48 to 0.72) |
*p < 0.05; **p < 0.01; ***p < 0.001; MASES: Medication Adherence Self-Efficacy Scale; TSRQ: Treatment Self-Regulation Questionnaire; SRBAI: Self-Report Behavioral Automaticity Index; MAR: Medication Adherence Reasons. This table does not adjust for multiple comparisons and is purely exploratory. No inferences should be drawn from these findings.
In addition to these correlations, we found many significant associations between MoBC measures. For example, self-efficacy was strongly associated with autonomous self-regulation (r = 0.39, p < 0.001; Table 5). The full correlation matrix for all study measures can be found in Table 5. It should be noted that due to multiple comparisons, any inferences drawn from these correlation analyses should be interpreted cautiously.
The findings in the current study support the idea that MoBCs are associated with adherence to antihypertensive medications. More specifically, self-efficacy for medication adherence is the MoBC most consistently associated with antihypertensive nonadherence in both univariate and multivariate analyses in our cross-sectional, self-report study. In addition, HTN knowledge was also associated with antihypertensive adherence in univariate regression analyses and in regressions with covariate adjustment. This shows that HTN knowledge is also an important mechanism for adherence. However, despite previous research suggesting that behavioral automaticity is a potentially important factor in medication adherence [41], SRBAI scores were not associated with self-reported adherence in either univariate or multivariate analyses. It should be noted that SRBAI scores were in the hypothesized direction and might have reached statistical significance in a much larger sample size or with repeated assessment measures. Collectively, these findings underscore the significant role of multiple distinct MoBCs, particularly self-efficacy and HTN knowledge, in understanding antihypertensive medication adherence. However, it should be noted that all of the above findings are based on self-reported medication adherence, which is potentially subject to biased reporting.
Luckily, future researchers can look to influence any potential target MoBCs using the extensive research showing the linkage between particular behavior change techniques (BCTs) and MoBCs [46, 53–55]. We intend to utilize the current study to identify key MoBCs for action and then utilize existing literature to design interventions targeted specifically for improving MoBCs.
Though scores on the MAR did not significantly differ between the groups with high and low adherence in independent samples t-tests, there were significant associations between continuous HB-HBP scores and MAR in bivariate correlation analyses. In addition, self-reported reasons for adherence, such as forgetfulness and barriers, were also associated with self-efficacy. This potentially shows how self-reported reasons for nonadherence may be associated with particular MoBCs, highlighting a future intervention pathway that can be tailored to reasons for nonadherence.
It should also be noted that a systematic review for nonadherence to antihypertensive medications found larger associations between predictors and adherence when adherence is assessed using objective measures rather than self-report [13]. It is possible that the “noise” and variability introduced by self-report bias may increase confidence intervals and reduce the strength of these associations [13]. Therefore, though the current results only represent a small snapshot of the antihypertensive adherence of a large healthcare system, future research may demonstrate stronger associations utilizing more objective measures of adherence, such as pharmacy refill data or smart pill bottles [56, 57]. It is also possible that the associations between adherence to antihypertensives and self-reported MoBCs may differ from the current findings if adherence were assessed more objectively. Low scores on self-efficacy and low self-reported antihypertensive adherence may reflect a self-critical psychological stance rather than a mechanistic association with behavior. There exists a great deal of nuance in how antihypertensive adherence is measured and operationalized. The authors acknowledge that depending on how adherence is determined and how a particular MoBC is measured, the strength of the associations between antihypertensive adherence and MoBCs may vary greatly.
In addition to our primary findings, exploratory analyses examining bivariate correlations between our study measures have the potential to provide useful estimates of effect size for future trials. Though the number of comparisons used in these analyses makes it difficult to draw strong inferences about the relationships between variables, we fully intend to utilize this information to calculate the sample sizes required for future behavioral interventions to increase antihypertensive medication adherence.
Finally, it is interesting to note the characteristics of individuals in our sample who self-reported non-adherence. Participants with self-reported non-adherence were more likely to be younger, female, and have different racial characteristics. This aligns with previous research showing non-adherent individuals have a younger age [58–60] and different racial characteristics [60]. Prior findings regarding self-reported sex and gender are more mixed. Some previous studies found no association between sex and antihypertensive adherence [61] or inconsistent findings based on the study population [62]. Prior work has highlighted that the factors that influence adherence may vary by gender, with female individuals being more likely to have low levels of antihypertensive adherence due to psychological factors [63, 64]. Additional research is needed to identify how best to address the adherence concerns among men and women.
The current study has several strengths. Firstly, we did not solely recruit individuals with problems adhering to antihypertensive medications. Instead, we recruited all individuals prescribed antihypertensive medication. This allows our study to examine MoBC levels in individuals with different self-reported adherence. In addition, we were able to obtain a preliminary, exploratory estimate of the prevalence of antihypertensive nonadherence within our health system, though this estimate may not reflect the full population of our health system. Secondly, we examined multiple potential MoBCs simultaneously. As a result, we can examine the association between each MoBC and adherence individually and in combination.
However, it should also be noted that this study has several limitations. Firstly, we collected data on a relatively small sample of patients who were taking antihypertensive medication. The sample was a majority female, predominantly white, and nearly all patients were insured. It is unlikely that these results will be representative of the full population of patients treated with antihypertensive medication in our health system. It should also be noted that we conducted a remote, digital survey trial. This would likely create a bias towards participants with high levels of digital literacy. We also compensated participants for completing the survey, which could also potentially introduce bias. Secondly, the current study has a cross-sectional design, which precludes longitudinal analyses of the associations between antihypertensive adherence and potential MoBCs. Further, cross-sectional findings prevent the determination of causality. If MoBCs are truly important targets for interventions, then changes in MoBCs should be associated with proportional changes in health behaviors. We cannot demonstrate these causal effects in this study. Though we plan to utilize the findings from the current study to justify future longitudinal clinical trials, we did not have the resources to run such a trial at this time. Finally, the current trial utilizes a self-report measure of medication adherence, which could potentially be subject to bias. However, it should be noted that medication adherence research often relies on self-report adherence measures [13]. It should also be noted that only 17% of the sample were nonadherent to medications, suggesting most individuals participating did not have high levels of nonadherence to antihypertensive medications. Further, non-adherence was classified based on the lowest quartile of responses in this particular sample. Other samples will likely have different cut-offs using the same approach. Therefore, the dichotomous analyses comparing low and high adherence levels should be interpreted cautiously. It is also possible that shared method variance may result from utilizing a self-report adherence measure in conjunction with self-reported MoBCs, though it is uncertain how this might enhance or dilute the associations shown in the current study [65].
The findings of the current exploratory study reinforce previous literature showing that MoBCs are associated with adherence to antihypertensive medications. Further, our study supports prior findings showing that self-efficacy for adherence is strongly associated with self-reported adherence behavior. HTN knowledge was also found to be associated with self-reported adherence. As a result, we believe that interventions targeting self-efficacy for medication adherence and HTN knowledge are potentially useful targets for MoBCs for behavioral interventions to improve antihypertensive adherence. However, we also believe that adherence to antihypertensive medications is a complex behavior that is likely to be influenced by multiple MoBCs simultaneously. We also recognize that the magnitude of the association between a particular MoBC and antihypertensive adherence may differ based on each individual and the potential causes of that individual’s behavior. Future research should examine the benefits of tailored interventions targeting specific mechanisms of adherence and potentially utilize self-reported reasons for nonadherence to guide and tailor the intervention approach.
CVD: cardiovascular disease
EHR: electronic health record
HB-HBP: Hill-Bone Compliance to High Blood Pressure Therapy Scale
HTN: hypertension
MAR-revised: Medication Adherence Reasons Scale Revised
MASES-R: Medication Adherence Self-Efficacy Scale Revised
MoBCs: mechanisms of behavior change
SRBAI: Self-Report Behavioral Automaticity Index
MJB, DL, and YKC: Conceptualization. MJB: Writing—original draft. DL and DM: Data Curation, Investigation, Project Administration. EH and YKC: Methodology. AMG: Supervision. MJB, DL, DM, EH, AMG, and YKC: Writing—review & editing. All authors read and approved the submitted version.
The authors declare no conflicts of interest.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Northwell Health (Protocol version 24-1048-MRB approved 11/20/2024).
Informed consent was obtained from all subjects involved in the study.
Informed consent to publication was obtained from relevant participants.
Access to de-identified data and analysis code is available upon request to the corresponding author.
This work was supported by the Barbara Zucker Emerging Scientist award. This is an internal award to Northwell Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 800
Download: 5
Times Cited: 0
Sameen Abbas ... Sohail Kamran
Claudio Tomasino, Marco Tomasino
Eirik Olsen ... Camilla L. Søraas
Vaia Raikou, Sotiris Gavriil
Shawna D. Nesbitt
Aaron Walsh ... Ranjit Philip
Sverre E. Kjeldsen ... Tor Ole Klemsdal
