 Perspective
Perspective

Affiliation:
1Institute of Clinical Medicine, University of Oslo, 0316 Oslo, Norway
2Department of Cardiology, Oslo University Hospital, 0424 Oslo, Norway
3Department of Nephrology, Oslo University Hospital, 0424 Oslo, Norway
Email: s.e.kjeldsen@medisin.uio.no
ORCID: https://orcid.org/0000-0003-2389-0272
Affiliation:
4Department of General Practice, Institute for Health and Society, University of Oslo, 0316 Oslo, Norway
Affiliation:
5Department of Preventive Cardiology, Oslo University Hospital, Aker, 0586 Oslo, Norway
Explor Med. 2026;7:1001390 DOI: https://doi.org/10.37349/emed.2026.1001390
Received: December 02, 2025 Accepted: March 01, 2026 Published: March 17, 2026
Academic Editor: Carlos M. Ferrario, Atrium Health Baptist Hospital, Wake Forest School of Medicine, USA
The article belongs to the special issue Drug Adherence in Hypertension
New guidelines for high blood pressure (BP) by the European Society of Cardiology (ESC) now consider BP of 120–140/70–90 mmHg to be elevated (“high”) BP and recommend pharmacotherapy for BP > 130/80 mmHg if the estimated 10-year risk of cardiovascular events exceeds 10%, regardless of age. These recommendations are given with reference to two meta-analyses, but the studies included in the referred meta-analyses lack direct relevance, as patients in the first meta-analysis had established hypertension and several cardiovascular risk conditions. Further, the estimation of risk levels in the second meta-analysis was not done a priori with the recommended SCORE2 risk tool, but through a post hoc analysis of cardiovascular death in the placebo group. We argue that no randomized study has provided BP treatment based on such risk algorithms, nor from healthy participants with “elevated BP” (120–139/70–89 mmHg). A further problem is the use of a fixed risk threshold of 10% regardless of age, which will shift treatment to older patients without any major risk factors, while younger individuals with early onset of high BP and other metabolic syndrome characteristics usually will have a 10-year estimated cardiovascular risk far below this threshold, thus treatment may be delayed. This concept of the 2024 ESC hypertension guidelines is not evidence-based and should, in our opinion, not be implemented in Norway or in any other country. Norwegian doctors should follow the National Directorate of Health’s guidelines with age-adjusted intervention thresholds and consult European Society of Hypertension guidelines if they need to consider more extensive patient recommendations.
High blood pressure (BP) is, along with cholesterol and smoking, the dominant modifiable risk factor for cardiovascular disease, kidney failure, and dementia. Diagnosing high BP and treating hypertension is therefore a task of great importance for public health. Over the past 50 years, there has been a positive trend with decreasing levels of BP, cholesterol, and smoking habits in Norway, and there has been a significant reduction in morbidity and mortality from cardiovascular diseases [1]. Health surveys in Norwegian counties, Tromsø [2] and Nord-Trøndelag [3], show that a middle-aged person has almost 10 mmHg lower systolic BP compared to before. The Tromsø study [2] shows that the proportion of individuals aged 40–49 with hypertension (> 140/90 mmHg) has decreased from 46% to 25% for men and from 30% to 14% for women from 1979 to 2015.
BP is epidemiologically associated with increased cardiovascular risk well into what is considered the normal range (BP below 120 mmHg systolic). Data from the Tromsø study [2] in 2015 showed that the average systolic BP for men aged 60–69 years was 136 mmHg, and for those aged 70–79 years it was 140 mmHg, while the corresponding BPs for women were 133 and 144 mmHg.
Although it can be demonstrated in epidemiological studies that there is a lower risk at systolic BP 120 vs. 140 mmHg, like total se-cholesterol of 4 vs. 5 mmol/L, this does not mean that everyone with systolic BP > 120 mmHg or se-cholesterol > 4 mmol/L should be given preventive medication. If attempts to improve lifestyle are insufficient, any recommendation for pharmacological intervention, both in primary and specialist health care, requires a comprehensive analysis of benefits versus drawbacks, resource use (including healthcare personnel and medication costs), and priorities, values, preferences, and shared decision-making among the individuals involved. Central elements in such an assessment are related to the quality of evidence for the intervention and cost/benefit considerations with knowledge of ‘numbers needed to treat’ (NNT), as well as considerations regarding health care costs and necessary workforce. Such trade-offs must underpin recommendations in national and international guidelines. Current Norwegian preventive cardiology guidelines [4] recommend lifestyle advice and possible pharmacological intervention based on a combined assessment of age-adjusted risk and BP levels, if untreated BP > 140/90 mmHg in standard office measurement, or > 130/80 mmHg in 24-hour measurement.
Considering our national Norwegian preventive guidelines [4] discussed above, in the present perspective article, we aim to make a critical review of the novel European hypertension guidelines recently published [5, 6]. The main reason for expressing a critical review would be that one of the new hypertension guidelines [6], if implemented in Norway, would imply a huge expansion of the population to be assessed for pharmacological antihypertensive treatment on the basis of no trial evidence.
European guidelines for the treatment of hypertension were published in 2003 by the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC). ESH and ESC also published joint guidelines in collaboration with other societies, including World Organization of National Colleges, Academies and Associations of General Practitioners/Family Physicians (WONCA, representing General Practitioners in Europe) in 2007, 2013, and 2018. ESH later published guidelines in 2023 without changes to definitions or main principles [5]. In all these guidelines, a BP of > 140/90 mmHg is required before recommending drug treatment in individuals without concomitant cardiovascular/renal conditions or diabetes.
However, ESC published guidelines in 2024 [6] with major changes compared to the previous joint guidelines. ESC has now classified what was previously considered ‘normal BP’ (120–129/70–79 mmHg) or ‘high normal BP’ (130–139/80–89 mmHg) at repeated regular office measurements as ‘elevated BP’ (120–139/70–89 mmHg) [6]. The new ESC guidelines [6] recommend treatment, first non-pharmacological for 3 months and then pharmacological, for everyone up to age high 80s with BP 130–139/80–89 mmHg if the 10-year cardiovascular risk exceeds 10%. The risk level is recommended to be assessed [5, 6] based on hypertension-mediated organ damage and the SCORE2 algorithms, including SCORE2 for individuals aged 40–69 years [7] and Systematic Coronary Risk Evaluation-2 Older People (SCORE2-OP), an algorithm to assess total risk in older people based on Norwegian population data and validated in other European countries for ages 70–89 years [8].
The recommendation from ESC [6] concerning the treatment of “elevated BP” is referenced to two meta-analyses [9, 10] and given as a class 1 recommendation with evidence level A. However, these two meta-analyses do not provide evidence for such a recommendation. The patients in the first meta-analysis [9] had established hypertension and several cardiovascular risk conditions. In the second meta-analysis [10], the risk level was estimated through a post hoc analysis of cardiovascular death in the placebo group and not with SCORE2/SCORE2-OP, and the analyses showed clinical effectiveness of pharmacological treatment only in secondary prevention—i.e., in patients with already established cardiovascular disease [10]. No randomized study has provided BP treatment based on such risk algorithms, nor from healthy participants with “elevated BP” (120–139/70–89 mmHg). This ESC recommendation [6] does not meet the criteria for class IA classification.
The ESC’s new recommendations [6] for “elevated BP” (120–139/70–89 mmHg) are mainly based on SCORE2 [7] and SCORE2-OP [8]. With these risk tools, so-called global risk (10-year risk for cardiovascular events or death) is assessed based on age, gender, smoking, cholesterol, and BP. Although the tools are extensively validated, age and gender have a dominant significance for the absolute risk of cardiovascular events. Therefore, in Norway, we have recommended that primary preventive pharmacological treatment must consider age-specific intervention thresholds. In our current guidelines [4], a risk > 5% for ages 45–54 years, > 10% for ages 55–64 years, and > 15% for ages 65–74 years is defined as advisory decision thresholds for drug treatment that provides a reasonable balance between sensitivity and specificity and acceptable levels for NNT [11]. Very similar conclusions regarding the need for age- and sex-adjusted thresholds have been published in a recent American analysis concerning sensitivity and specificity for the initiation of statins in primary prevention [12]. The ESC’s general preventive guidelines [13], supported by ESH [5], have similarly recommended intervention at risk > 7.5% for ages < 50 years, risk > 10% for ages 50–69 years, and risk > 15% for ages > 70 years. In the new 2024 BP guidelines [6], however, the ESC has unexpectedly abandoned the age-specific risk assessment and instead suggested a 10% risk threshold for all ages, thus significantly lowering the threshold for pharmacological antihypertensive treatment for individuals over 70 years.
When using SCORE2-OP [8], it is evident that almost the entire European population over 70 years old will have a 10-year risk of 10% or more. This means, for example, that healthy 70-year-old men may be recommended antihypertensive treatment with a BP of 131/82 mmHg, and the same would apply to women at 75 years and older. Since the average systolic BP for this age group is > 140 mmHg for both men and women [2], there are very few older people with systolic BP < 130 mmHg. Thus, in practice, almost the entire population above 70 years appears to be candidates for pharmacological BP-lowering treatment if the proposed ESC guidelines [6] are to be implemented in Norway. It should be noted, however, that for old patients with frailty, the ESC guidelines [6] rightfully suggest exceptions and special considerations.
The recommendation in the ESC guidelines from 2024 [6] regarding antihypertensive treatment of large population groups with “elevated BP” mainly relies on one meta-analysis featuring a significant portion of study participants at increased risk [9]. Among individuals categorized as “without cardiovascular disease” and with a systolic BP of 120–139 mmHg, approximately 40% had diabetes, 20% had kidney disease, 10% had peripheral vascular disease, and 6–8% had atrial fibrillation. Furthermore, at the start of the study, 27.5% were using angiotensin-converting enzyme inhibitors, 27% calcium blockers, 21.5% diuretics, 17% beta-blockers, and 11% angiotensin receptor blockers.
The closest we come to studies on the benefits of giving medications to individuals with baseline BP < 140/90 mmHg is the Heart Outcomes Prevention Evaluation-3 (HOPE-3) study with 12,705 randomized individuals [14]. In HOPE-3, candesartan/ hydrochlorothiazide was compared to placebo among categories of patients with different baseline BP, fairly corresponding to the BP levels of 120–129/70–79 mmHg, 130–139/80–89 mmHg, and > 140/90 mmHg highlighted in the 2024 ESC hypertension guidelines [6]. Only the tertile with the highest baseline BP (> 143.5 mmHg and an average of 154.1 mmHg) had clinical benefits from the candesartan/ hydrochlorothiazide BP-lowering treatment in HOPE-3 [14].
Regarding the reason why ESC has changed policy from recommending pharmacological treatment of people with hypertension (BP > 140/90 mmHg) to drug treatment of people with “elevated BP”, previously high normal BP (BP 130–139/80–89 mmHg) we can only speculate. The intention has probably been to enhance CVD risk reduction further, based on indirect evidence from epidemiological studies and studies on different high-risk patients with several comorbidities. However, such indirect evidence cannot replace proper trial outcome data from the population in question, i.e., from a trial on otherwise healthy older men and women with elevated BP and a SCORE risk > 10%—a risk that could be driven primarily by age itself.
The paradox with the 2024 ESC new hypertension guidelines [6] is that when recommendations to treat BP > 130/80 mmHg are linked to a risk of atherosclerotic cardiovascular disease risk > 10% (regardless of age), in practice almost everyone over 70 years qualifies for treatment [8], while younger people with clearly higher risk than their peers do not qualify. If a 45-year-old person with overweight, prediabetes, and dyslipidemia already has a BP of 135/88 mmHg, it is likely that early BP treatment could be an important part of reducing his lifelong, significant excess risk. But the SCORE2 risk [7] will be far below 10%. In fact, no no-smoking individual below the age of 60 will have SCORE2 risk that exceeds 10% in low-risk countries like Norway, not even if systolic BP is > 170 mmHg and non-HDL > 6 mmol/L.
When a young person has a systolic BP of 135 mmHg, he or she is above the average, which signals a significant, lifelong excess risk. When a 70-year-old person has a systolic BP of 135 mmHg, he or she is below the average for his or her peers, and additional risk factors should be present before the risk level creates concern and demands pharmacological intervention.
The distribution of BP according to the traditional ESH/ESC definitions [11] shows a general shift towards the “optimal” and “normal” categories (< 120/80 mmHg and 130–139/85–89 mmHg, respectively) for both women and men in nearly all age groups (Figure 1). The proportion of participants with “normal” BP according to the previous joint ESH and ESC Guidelines (systolic BP below 140 mmHg and diastolic BP below 90 mmHg) [11] increased from 52.8% in HUNT1, via 57.4% in HUNT2, to 71.0% in HUNT3. The improved BP control increased in both sexes and in all age-groups as shown in graphs and tables at the home page of the Norwegian Institute of Public Health (https://www.fhi.no/is/ncd/blodtrykk/blodtrykk/): Average systolic BP (mmHg) in age groups of 10-year ranges in the Norwegian population surveys HUNT1 through HUNT4.
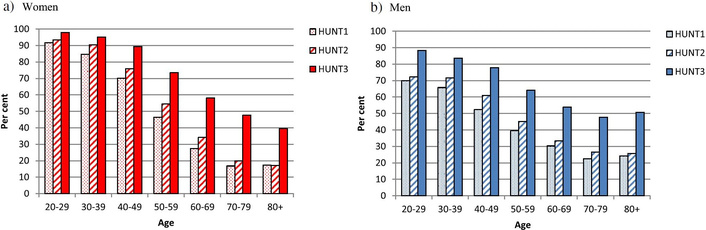
Per cent of participants with SBP < 140 mmHg in the Norwegian Nord-Trøndelag Health Studies, HUNT1, HUNT2, and HUNT3, by age ranges in women (a) and in men (b). Less than 50% of individuals > 70 years have SBP below 140 mmHg in the most recent survey, while approximately 80% of men and 90% of women are below 140 mmHg in the age group 40–49 years. The graphs are reproduced from [3], © 2016 Holmen et al. Distributed under the terms of the Creative Commons Attribution 4.0 International License, with data from the HUNT Research Centre, University of Science and Technology (NTNU). All HUNT data are stored at the HUNT Research Centre and are available from http://www.ntnu.edu/hunt. The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between HUNT Research Centre (Faculty of Medicine, Norwegian University of Science and Technology NTNU), Nord-Trøndelag County Council, Central Norway Health Authority, and the Norwegian Institute of Public Health.
The documentation behind ESC’s new guidelines [6] is insufficient to put many millions of individuals, especially among the older population, on antihypertensive therapy with uncertain clinical benefit and all the side effects that may accompany it. The healthcare system globally, the workforce, and budgets are already struggling to meet the demands of managing hypertension for at-risk patients, where the benefits of therapy are proven. It is estimated that primary care physicians, pharmacists, specialized nurses, and physician assistants must spend more than 20% of their working hours providing 2 hours of annual care for patients with hypertension in the USA [15]. We assume that the demands on primary healthcare in Europe will be similar. Given a rapidly growing population of older individuals at high risk for cardiovascular events, the many unresolved issues will require thoughtful prioritization based on timely and adequately driven clinical studies. Nonetheless, significant proportions of the population have uncontrolled BP assessed as > 140/90 mmHg [2], and the capacity in the healthcare system should be prioritized for better management of these individuals, rather than healthy people with lower BP and risk.
We conclude that Norwegian doctors should continue to follow the guidelines developed by the Norwegian Directorate of Health [16] with age-adjusted intervention thresholds [4] and consult ESH guidelines [5] if they need to consider in-depth recommendations. A novel aspect for the future may also be to consider BP in relation to reproductive health. Recent studies indicate that even high-normal or mildly elevated systolic BP adversely affects live birth rates in women undergoing assisted reproduction [17, 18].
It may appear reasonable that other countries with similar population characteristics also perform independent critical analyses of the ESC 2024 hypertension guidelines before implementation.
BP: blood pressure
ESC: European Society of Cardiology
ESH: European Society of Hypertension
HOPE-3: Heart Outcomes Prevention Evaluation-3
NNT: numbers needed to treat
SCORE2-OP: Systematic Coronary Risk Evaluation-2 Older People
The authors thank Inger Ariansen, MD, PhD, for reviewing and commenting on this article.
SEK: Writing—original draft. BG: Writing—review & editing. TOK: Writing—review & editing. All authors read and approved the submitted version.
Sverre E. Kjeldsen reports lecture honoraria from Emcure, Getz, Hikma, J.B. Pharma, Merck Healthcare KGaA, and Vector-Intas in the past 3 years. Sverre E. Kjeldsen has been a Guest Editor of Exploration of Medicine but was not involved in the decision-making or the review process of this manuscript. The other authors declare that there are no conflicts of interest.
Not applicable.
Not applicable.
The current article is based on a similar review published in the Journal of the Norwegian Medical Association on May 6th, 2025 (reference [19]). The re-publication in English in Exploration of Medicine has been approved by Are Brean, MD, Editor-in-Chief of the Journal of the Norwegian Medical Association. Approval was received by E-mail to first author on November 10, 2025.
Not applicable.
There was no funding for the present article.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 3851
Download: 13
Times Cited: 0
Sameen Abbas ... Sohail Kamran
Claudio Tomasino, Marco Tomasino
Eirik Olsen ... Camilla L. Søraas
Vaia Raikou, Sotiris Gavriil
Shawna D. Nesbitt
Aaron Walsh ... Ranjit Philip
