Original Article
Original Article

Affiliation:
1Department of Internal Medicine, General, Emergency and Post-Acute, Diabetic Foot Unit, Ospedale Civile di Baggiovara, Azienda Ospedaliero Universitaria di Modena, 41126 Modena, Italy
2Division of Metabolic Internal Medicine, Ospedale Civile di Baggiovara, Azienda Ospedaliero Universitaria di Modena, 41126 Modena, Italy
Email: maurantonio.mauro@aou.mo.it
ORCID: https://orcid.org/0000-0003-3500-1145
Affiliation:
2Division of Metabolic Internal Medicine, Ospedale Civile di Baggiovara, Azienda Ospedaliero Universitaria di Modena, 41126 Modena, Italy
Affiliation:
2Division of Metabolic Internal Medicine, Ospedale Civile di Baggiovara, Azienda Ospedaliero Universitaria di Modena, 41126 Modena, Italy
Affiliation:
3Department of Surgical and Medical Sciences, University of Modena and Reggio Emilia, 41124 Modena, Italy
Affiliation:
2Division of Metabolic Internal Medicine, Ospedale Civile di Baggiovara, Azienda Ospedaliero Universitaria di Modena, 41126 Modena, Italy
3Department of Surgical and Medical Sciences, University of Modena and Reggio Emilia, 41124 Modena, Italy
ORCID: https://orcid.org/0000-0002-4794-9809
Affiliation:
2Division of Metabolic Internal Medicine, Ospedale Civile di Baggiovara, Azienda Ospedaliero Universitaria di Modena, 41126 Modena, Italy
3Department of Surgical and Medical Sciences, University of Modena and Reggio Emilia, 41124 Modena, Italy
ORCID: https://orcid.org/0000-0002-0410-1760
Explor Med. 2021;2:98–109 DOI: https://doi.org/10.37349/emed.2021.00035
Received: November 04, 2020 Accepted: January 06, 2021 Published: February 28, 2021
Academic Editor: Lindsay A. Farrer, Boston University School of Medicine, USA
The article belongs to the special issue Exploring Type 2 Diabetes Mellitus
Aim: Diabetic foot syndrome (DFS) is a complication of diabetes in which the presence of infections, ulceration and/or destruction of deep tissue associated with neuropathy, peripheral atherosclerosis and comorbidity affect the prognosis, the need for limb amputation and quality of life. Purpose of the present study is to report the features of patients with acute DFS admitted to our Diabetic Foot Unit tertiary Center in 2019.
Methods: In all patients admitted, the approach was performed through a multidisciplinary team (Diabetic Foot Care Team) and described in a specific diagnostic-therapeutic-assistance program. Criteria of inclusion were presence of sepsis and/or suspected osteomyelitis and/or critical limb ischemia. Clinical features and interventions performed were registered. Primary endpoints were mortality and amputation (major, minor). Secondary endpoints were length of hospitalization, type of revascularization and duration of antibiotic therapy.
Results: Among 75 consecutive patients (mean age 70.9 years) enrolled, prevalence of acute DFS was higher among men (M/F 3:1). Poor glycemic control [mean hemoglobin A1c (HbA1c) 67.9 ± 22.3 mmol/mol], long duration of diabetes (mean 19 ± 16.3 years), high low-density lipoprotein-cholesterol (mean 89.5 ± 45.1 mg/ dL) and obesity (mean Body Mass Index 30.2 ± 7.6 kg/m2) were common. Diabetes-related complications as peripheral arterial disease (PAD) (76%), ischemic heart disease (48%), retinopathy (40.5%), hepatic steatosis (50%), heart failure (17.8%) were present. During hospitalization, 21 subjects (28.4%) underwent lower limb amputations (overall rate of major amputation 4%), and 41.3% underwent percutaneous angioplasty. Long period of hospitalization (18.4 ± 7.9 days) and prolonged antibiotic therapy (23.9 ± 15.9 days) were observed. Major amputation was associated with C-reactive protein > 6.5 mg/dL (P = 0.03), osteomyelitis (P = 0.001), prior insulin therapy (P = 0.015).
Conclusions: Male sex, co-morbidity, PAD, systemic inflammation and poor glycemic control are major features of acute hospitalized DFS. An approach through a multidisciplinary team is recommended in order to treat vascular and extra-vascular complications aimed at reducing mortality and at improving quality of life.
The diabetic foot syndrome (DFS) defines a cluster of diabetes-related morbid conditions including sensory neuropathy, immunopathy, arthropathy and peripheral arterial disease (PAD), with a global prevalence of 6.3% and in which unrecognized tissue injury can lead to foot ulceration, infection and risk of limb amputation. Diabetic foot prevalence is higher in men (4.5%) than in women (3.5%) and in type-2 diabetes (T2D) (6.4%) than in type-1 diabetes (T1D) (5.5%) [1].
In diabetics with foot ulcer, neuropathy, ischemia, infection and the presence of multi-morbidity affect the prognosis, the need for limb amputation and the quality of life [2]. Further risk factors are age, prolonged duration of diabetes, smoking, poor glycemic control, peripheral neuropathy and/or PAD, anatomical abnormalities, retinopathy, past history of foot ulcer or distal amputation [3–6]. Conversely, the role of sex, a major modifier of disease and nonalcoholic fatty liver disease (NAFLD), a relatively novel cardiovascular risk factor in T2D, remain incompletely characterized [7–11].
The treatment of diabetic foot is the most expensive complication of diabetes [12, 13] and DFS exposes to high morbidity and mortality [14–15]. In DFS, the management of complexity through a global bio-psycho-social approach able to plan personalized assistance and an integrated multidisciplinary team significantly reduce mortality and the risk of infections and major amputation, improving outcomes and quality of life [1, 16–19]. In 2019, in the University Hospital of Modena a multidisciplinary multi-professional team (Diabetic Foot Care Team) was set up, led by an Internist, and including physicians from other medical disciplines, integrated by technical nursing skills. The Diabetic Foot Care Team is described in a specific diagnostic-therapeutic assistance program (DTAP) issued and approved by the local health care system, and it is in charge to serve as a referral center systematically taking care of all patients presenting with both T2D and signs/symptoms related to lower limbs in the Province of Modena, Northern Italy.
In the present study, we addressed some relevant research questions relating to clinical presentation, co-morbidity and other factors such sex differences, prevalence rates of NAFLD and other features associated with DFS and their association with limb amputation.
This is a retrospective observational study performed using a registration system on a cohort of 75 consecutive patients admitted to the Diabetic Foot Unit of Modena since January 1 through December 31, 2019, namely the first year of activity of our center. The Diabetic Foot Care Team composed by specialists in Internal Medicine (team leader), Endocrinology and Diabetology, Vascular Surgery, Orthopedics, Dermatology, Radiology, Microbiology, Infectious Disease, Clinical Nutrition, Physiatry and Clinical Psychology, integrated by technical nursing skills is described in detail in a specific DTAP.
Criteria of inclusion were: presence of signs/symptoms of sepsis, suspicion of osteomyelitis and/or critical limb ischemia. Criteria of exclusion: individuals who were unable or refuse to provide consent to participate in the study and subjects under 18 years. Demographic and anthropometric data such as age, sex, weight, height, body-mass-index (BMI) were registered. Historical data relating to the presence of co-morbidities, previous revascularization, current therapy were recorded at admission, along with all diagnostic-therapeutic interventions performed during hospitalization. The average length of hospitalization and clinical outcomes were also recorded. “PAD” was defined as obstructive atherosclerotic vascular disease with clinical symptoms, signs or abnormalities on non-invasive vascular assessment, resulting in disturbed or impaired circulation in one or more extremities; “osteomyelitis” was defined as infection of the bone, with radiological signs of involvement of the bone marrow; “major amputation” was defined as any resection proximal to the ankle; “minor amputation” was defined as any resection through or distal to the ankle, according to the International Working Group on Diabetic Foot (IWGDF) criteria [2]. “Ischemic heart disease” was defined as history of non-fatal myocardial infarction or coronary revascularization; “chronic kidney disease (CKD)” was defined as presence of progressive renal function decline; “retinopathy” was defined as presence/history of vitreous hemorrhage, blindness or requirement for intra-vitreal agent or photocoagulation. Despite the limitations, especially in obese [20, 21], liver steatosis was defined through ultrasound-based criteria as mild, moderate, severe. Primary endpoints of the study were mortality, major and minor amputations. Secondary endpoints were length of hospitalization, type of revascularization, transfer to intensive care and duration of antibiotic therapy.
Statistical analyses were carried out with the SPSS 21 software (IBM, Armonk, NY, USA) for Windows® operating system. All continuous numerical variables were reported as mean ± SD; nominal variables were reported as absolute frequency and % of the total. Mean differences were compared using Student’s t-test, frequency differences with χ2 test. Differences between means, and associations between variables were considered statistically significant when the probability of chance differences and associations were below 5% (P < 0.05). Variables statistically significant in univariate analyses were used in multivariate models in order to find the ones independently related to osteomyelitis and amputation. The present study was approved by the local Ethics Committee.
We evaluated 75 patients (73.3% men and 26.7% women), mean age 70.9 years (range 47–93), with a mean time of hospitalization of 18.4 ± 7.9 days (Table 1). In our series, the mean duration of T2D was 19 ± 16.3 years, and the mean BMI was 30.2 ± 7.6 kg/m2. At admission, poorly compensated T2D was reported in most cases: median glycated haemoglobin (HbA1c) was 67.9 ± 22.3 mmol/mol whereas blood glucose was 196.9 ± 105.9 mg/dL. In half of the subjects hepatic steatosis was absent (Table 2). Most patients revealed micro and macrovascular complications of diabetes: PAD (76% of cases), ischemic heart disease (50%), CKD (48%), and retinopathy (40.5%).
Main demographic, diseases and therapeutic characteristics, and diagnostic and surgical interventions in the study population with DFS
| Characteristics | Mean value ± SD |
|---|---|
| Sex Males (%) | 73.3 |
| Age (years) | 70.9 ± 10.35 |
| Age of onset of T2D (years) | 49.2 ± 15.5 |
| Duration of diabetes (years) | 19.2 ± 16.3 |
| BMI (Kg/m2) | 30.2 ± 7.6 |
| Systolic Blood Pressure (mmHg) | 143.7 ± 20.5 |
| Diastolic Blood Pressure (mmHg) | 75.5 ± 10.9 |
| Heart Rate (bpm) | 80.4 ± 14.4 |
| Glasgow Come Scale (0–15) | 14.9 ± 0.3 |
| Pain scale (NRS 0–10) | 2.6 ± 3.4 |
| Body Temperature (°C) | 36.5 ± 0.7 |
| Co-morbidity at admission | Frequency (%) |
| Heart failure | 17.8 |
| Soft tissue inflammation | 82.7 |
| Osteomyelitis | 56 |
| PAD | 76 |
| Retinopathy | 40.5 |
| CKD (no. of patients) | 48 |
| Stage IIIa (eGFR 59-45 mL/min) | 20 |
| Stage IIIb (eGFR 44-30 mL/min) | 12 |
| Stage IV (eGFR 29-15 mL/min) | 12 |
| Stage V (eGFR < 15 mL/min) | 4 |
| Ischemic Heart Disease | 50 |
| Atrial Fibrillation | 14.7 |
| Previous Stroke | 13.3 |
| Active cancer | 5.4 |
| Dementia | 4 |
| Hepatic Steatosis | 16 |
| COPD | 6.7 |
| Smokers | 12.3 |
| Therapy at admission | Frequency (%) |
| Anti-hypertensive | 74.7 |
| Oral antidiabetics | 56.8 |
| Insulin | 54.1 |
| Antiplatelet agents | 64.4 |
| Statins | 54.1 |
| Primary Endpoints | Frequency (%) |
| Lower limb amputation (total 21 patients) | 28.4% |
| Major: 4.1% | |
| Minor/Curative: 24.3% | |
| Mortality in Diabetic Foot Unit (no patient) | 0% |
| Secondary Endpoints | Mean value ± SD |
| In-hospital duration of antibiotic therapy (days) | 18 ± 9.8 |
| Total duration of antibiotic therapy (days) | 23.9 ± 15.9 |
| Time of hospital stay (days) | 18.4 ± 7.9 |
| Others | Frequency (%) |
| Percutaneous angioplasty | 41.3% |
| Transfer to Intensive Care Unit (total 4 patients) | 5.3% |
Biochemical assays of the 75 patients admitted in the Diabetic Foot Unit
| Characteristics | Mean value ± standard deviation |
|---|---|
| HbA1c (mmol/mol) | 67.9 ± 22.3 |
| Blood Glucose (mg/dL) | 196.9 ± 105.9 |
| White blood cells (109/L) | 10.8 ± 4.9 |
| Neutrophils white-blood cells (109/L) | 9.3 ± 8.9 |
| Hb (g/dL) | 11.5 ± 1.8 |
| Sideremia (μg/dL) | 38.1 ± 22.1 |
| Transferrin (mg/dL) | 189.7 ± 52.1 |
| Transferrin saturation (%) | 15.2 ± 10.0 |
| Ferritin (ng/mL) | 301.6 ± 479.9 |
| CRP (mg/dL) | 9.4 ± 8.6 |
| Procalcitonin (ng/mL) | 2.7 ± 8.4 |
| Blood Urea (mg/dL) | 60.3 ± 40.6 |
| Creatinin (mg/dL) | 1.4 ± 0.9 |
| Total cholesterol (mg/dL) | 144.4 ± 55.7 |
| HDL (mg/dL) | 32.4 ± 10.7 |
| LDL (mg/dL) | 89.5 ± 45.1 |
| TG (mg/dL) | 146.6 ± 56.2 |
| Uric acid (mg/dL) | 5.6 ± 2.2 |
| Total Bilirubinemia (mg/dL) | 0.7 ± 0.4 |
| Direct Bilirubinemia (mg/dL) | 0.2 ± 0.1 |
| AST (U/L) | 21.0 ± 15.3 |
| ALT (U/L) | 20.3 ± 24.2 |
| GGT (U/L) | 63.9 ± 74.9 |
| ALK-P (U/L) | 113.6 ± 56.7 |
| B12 vitamin (ng/L) | 345.9 ± 228.7 |
| D-vitamin (ng/mL) | 16.4 ± 17.5 |
| Folic acid (ng/mL) | 9.1 ± 9.7 |
| BNP (ng/L) | 728.9 ± 1083.7 |
| Albumin (g/dL) | 3.1 ± 0.5 |
Co-morbidities: chronic atrial fibrillation (14.7%), previous stroke (13.3%), cancer (5.4%), smoking habit (12.3%), chronic obstructive pulmonary disease (COPD) (6.7%) were observed. Thirteen patients (17.8%) had heart failure.
Drug treatment: drug therapy at home included angiotensin converting enzyme (ACE)-inhibitors or sartans (27% and 11.3% of patients respectively), beta-blockers (47.3%), other vasodilators (5.5%). Antiplatelet agents, i.e., acetylsalicylic acid (74.5%) or the association clopidogrel + acetylsalicylic acid (14.9%) were reported in 64.4% of patients. Oral antidiabetics were used by 56.8% of patients, whereas insulin alone by 54.1%. Statins were taken by 54.1% of patients.
Physical, laboratory and imaging findings: at admission, mean systolic blood pressure was 143.7 ± 20.5 mmHg (1 mmHg = 0.133 kPa) and mean diastolic blood pressure was 75 ± 10.9 mmHg; mean heart rate was 80.4 ± 14.4 beats per minute (bpm) and average body temperature was 36.5 ± 0.7°C. Hospitalized patients showed an increase in indices of systemic inflammation: neutrophilic leukocytosis (white blood cells 10.8 ± 4.9 × 109/L, N = 9.3 ± 8.9 × 109/L), procalcitonin (2.7 ± 8.4 ng/mL) and C-reactive protein (CRP) (9.4 ± 8.6 mg/ dL). In the 82% of patients clinical signs of skin and soft tissues inflammation was identified; in 42 patients (56%) osteomyelitis was diagnosed through radiological imaging (X-ray, computerized tomography or magnetic resonance). In 57 patients (76% of total) PAD was present; in 73.6% of them (42 subjects) vascular obstruction was revealed through angiography while in 26.3% of them (15 subjects) the diagnosis of PAD was based on anamnestic findings. In 82.7% of patients extensive microbiological evaluation was carried out; 10.7% of patients underwent bone biopsy, while debridement or surgical evacuation of phlegmon was performed in 33.8% and 23% respectively (Table 3). In 8.2% of patients blood cultures were positive, and positivity of blood cultures was significantly associated with osteomyelitis (P = 0.026). In multivariate analysis, only insulin therapy appeared to be an independent factor for osteomyelitis, but not for total amputation.
Amputation, osteomyelitis and risk factors in 75 patients with DFS enrolled in the study
| Total Amputations (major and minor) | Risk Factor | Amputation NO | Amputation YES | P value |
| CRP > 65mg/L | 6 | 15 | 0.03 | |
| Osteomyelitis | 3 | 18 | 0.001 | |
| Insulin therapy | 5 | 16 | 0.015 | |
| Duration of diabetes (≥ 20 years) | 9 | 13 | 0.055 | |
| HbA1c > 55 mmol/mol | 4 | 17 | 0.165 | |
| Previous revascularization | 6 | 15 | 0.089 | |
| Osteomyelitis | Risk Factor | Osteomyelitis NO | Osteomyelitis YES | P value |
| CRP > 65 mg/L | 13 | 29 | 0.001 | |
| Total Amputations | 24 | 18 | 0.001 | |
| White blood cells > 12 × 109/L | 24 | 18 | 0.003 | |
| Insulin therapy | 13 | 29 | 0.003 | |
Treatment: during hospitalization, antibiotic therapy was administered to 98.7% of patients, in 77.3% via injective route; the mean duration of antibiotic therapy was 23.9 ± 11.59 days. 41.3% of patients were submitted to percutaneous angioplasty; the most affected vessels were the posterior tibial artery (47.6%) and the anterior tibial artery (45.2%). In the whole cohort of patients admitted to the Diabetic Foot Unit, the Multidisciplinary Team, coordinated by an Internal Medicine doctor, involved more than 20 specialists, mainly Vascular Surgeons (94.7%) and Infectious Disease specialists. During hospitalization, 21 patients (28.4%) were submitted to lower limb amputations: only in 3 of them a major amputation was performed while 18 patients (24.3%) underwent curative minor amputation for either osteomyelitis or gangrene. Four patients were transferred to an Intensive Care Unit, while no death was observed in the Unit.
This study was conducted on a cohort of 75 consecutive patients admitted to our Diabetic Foot Unit, as part of a DTAP for the management of T2D with DFS. The four main findings of the study were the followings: DFS appeared to be a sexually dimorphic disease; patients have deranged cardio-metabolic parameters; markers of inflammation seemed to be associated with amputation; DFS had a high rate of co-morbidities that reflect severity of diabetes.
Male sex seemed to be associated with DFS complications, with a male/female ratio of 3:1 (73.3% vs. 26.7% respectively). Similar results were observed in a recent meta-analysis [22]. Other observational studies have confirmed the male prevalence of complicated diabetic foot disease, in which the female sex, however, would be burdened by worse outcomes [23, 24]. Poor foot self-care, characterized by not regularly checking feet, poor hygiene and unhealthy habits were more frequent in a cross-sectional study conducted in a sample of 1,515 patients with T2D aged 40 year-old or older [25]. In previous observational studies, women with PAD, when compared to men, seem to have a more pronounced pro-inflammatory profile [26, 27]. However, our preliminary study does not enable us to draw any firm conclusions as to the potential association of sex and outcomes, because this was not a population-based study.
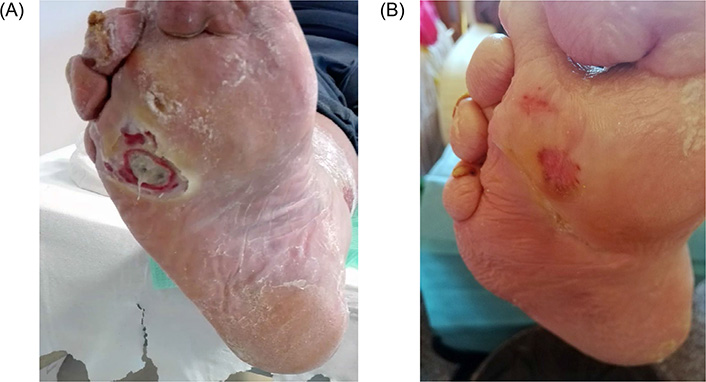
Most patients hospitalized in the acute phase presented with poor metabolic control and had raised indices of systemic inflammation. In our cases, patients hospitalized with DFS had a long disease duration (19 years) and poor glycemic control. Low-density lipoprotein (LDL)-cholesterol was high, too, and 76% of patients had PAD, conditioning an increased cardiovascular risk. Statins improve the lipid profile and exerted pleiotropic effects including plaque stabilization, regression of atheroma and anti-inflammatory effects able to minimizing cardiovascular risk in high risk subjects; however, the role of lipid-lowering drugs in PAD patients requires further studies [28]. Cardiovascular prevention guidelines recommend reaching the LDL-cholesterol target < 70 mg/dL in high-risk subjects and a target of < 55 mg/dL in very high-risk subjects with cardiovascular disease and/or multiple cardiovascular risk factors [29, 30]. Patients with diabetic foot ulcer (DFU), especially if PAD or other relevant co-pathologies such as CKD are present, should be considered at very high risk [31, 32]. In our cohort, only 54.1% of patients used statins and this fact conflicts with recommendations of international guidelines. In our series of patients, a similar deviation from the blood pressure target was observed with median values of 143.7 mmHg, i.e. above those recommended target values (systolic blood pressure < 140 mmHg and diastolic blood pressure < 90 mmHg) that prevent cardiovascular events and micro-vascular complications [33–37]. The American Diabetes Association suggests lower targets if atherosclerotic cardiovascular disease (ASCVD) is present [35]. The finding that hospitalized patients with T2D and acute DFS do not reach the therapeutic targets in primary and secondary prevention suggests that it is necessary to implement therapeutic models and strategies to reduce the incidence of cardiovascular complications and to improve outcomes in patients with DFS. It is known that DFU is a condition of infection and ulceration sometimes accompanied by destruction of deep tissue (Figure 1). Our results therefore, confirm the presence of a sensitive neuropathy in which poor glycemic control plays a major role [38, 39]. In our study there seems to be an association between the use of home insulin therapy and total amputations (P = 0.015), seemingly in contrast with some evidence in recent literature supporting either a neutral or a protective effect of insulin on the cardiovascular outcomes [40–42]. In T2D, insulin treatment is usually started after secondary failure of oral hypoglycemic therapy. However, there is a long duration of illness before this occurs; thus, it is the duration of illness, rather than the use of insulin, that could be the true risk factor associated with amputation. In our study, the association of amputation with median duration of T2D is intriguing, though it did not reach statistical significance (P = 0.055), probably owing to the limited patient population.
The systemic inflammatory state plays a key role in development of vascular complications and in predisposing to hospitalization [43]. In a randomized study carried out on about 18,000 seemingly healthy subjects with low LDL-cholesterol levels but with high C Reactive Protein (CRP), it was found that the administration of statin significantly reduced the incidence of cardiovascular events [44–46]. In our patients, the intensity of painful symptoms linked to ischemia and/or local peripheral inflammation, assessed by the numerical rating scale (NRS), was 2.6 ± 3.4; only in 2–3% of cases it was necessary to implement the analgesic therapy by pain-therapy specialists.
Although the team’s criteria for amputation were clinical and radiological, in our study a CRP > 6.5 mg/dL was found to be associated with total amputations (P = 0.03) and with presence of osteomyelitis (P = 0.001). The same association was also found between osteomyelitis and total amputations (P = 0.001) such as discussed below. Based on these results, CRP may be considered a sensitive test to identify patients with the worst prognosis.
In our patients with acute DFS, PAD is confirmed to be a highly prevalent condition (76% of cases); furthermore, retinopathy (40.5%), CKD (48%), ischemic heart disease (50%) were also found. Half of patients had hepatic steatosis. Patients with NAFLD are at an increased risk for cardiovascular disease [47] and NAFLD is a well-defined risk factor for the future development of T2D and Metabolic Syndrome [48]. Patients with T2D will worsen the course of NAFLD and, conversely, patients with NAFLD were at higher risk for cardiovascular complications of T2D [49]. In a cross-sectional study on 2,646 T2D patients, patients with NAFLD had significantly higher prevalence of PAD compared with those without NAFLD; this association was much stronger among women than among men [50]. Further studies are needed to screen for hepatic steatosis with/without fibrosis even with non-invasive tests [51].
In consideration of the available evidence, comorbidities reflect severity of diabetes, unhealthy lifestyle habits and failure to achieve cardiovascular prevention targets [6, 30].
Our study shows a statistically significant association between amputations and CRP > 6.5 mg/dL (P = 0.03), osteomyelitis (P = 0.01) and prior therapy with insulin (P = 0.015) (Table 3). With regard to the duration of diabetes (> 20 years), the relationship is interesting although not statistically significant (P = 0.055); the same trend was observed for the previous revascularization data (P = 0.089). In our study, HbA1c levels seem not associated with amputation (P = 0.165). In our sample, osteomyelitis seems strongly associated with: CRP > 6.5 mg/dL (P = 0.001), risk of amputation (P = 0.001), leukocytosis > 12 × 109/L (P = 0.003) and prior therapy with insulin (P = 0.003). High levels of high-sensitivity CRP, a marker of inflammation, are associated to poor cardiovascular prognosis in obesity and in metabolic syndrome [52, 53]. Simple steatosis is no more considered a benign condition and NAFLD is associated to cardio-renal complications [14, 54]. Although evidence suggests an association between NAFLD and T2D, in this study the relationship between BMI, glycemic status and presence of hepatic fibrosis with risk of amputation is unclear.
Size of the sample, retrospective design, and lack of a control group admitted to general hospital wards are points of weakness of the present study, which have prevented more in-depth statistical analyses. Our study is homogeneous with respect to the final patient allocation, which allowed the standardization of diagnoses [according to the International Classification of Diseases, Ninth Edition-Clinical Modification (ICD9-CM) system] and treatment schedules.
Despite these limitations, in this study, conducted in a cohort of 75 consecutive patients admitted in the Diabetic Foot Unit of the Third Level Center of the Modena University Hospital, a prevalence of male sex, poor glycemic control, systemic inflammation, prolonged hospitalization time, presence of PAD and need for invasive interventions in acute presentation of DFS were observed, and confirmed the complexity of DFS. Statins were found to be used by only half of patients, and this fact reinforces the need to tackle patients to adhere to the recommended therapies. Additional studies are needed to evaluate the impact of co-morbidities on the risk of major amputation. Moreover, adequate screening and prevention programs should be further developed among patients with long-standing T2D and particularly among those with ASCVD aimed at achieving the recommended metabolic targets, establishing “scores” allowing the identification of patients at higher risk for complications and amputation, and thus reducing the incidence of acute DFS. Future studies should evaluate, in a larger sample size, the most relevant risk factors linked to DFS risk, in order to reach a more targeted prevention, an earlier diagnosis, and a faster therapy of patients with such a harmful syndrome.
BMI: body-mass-index
CKD: chronic kidney disease
CRP: C-reactive protein
DFS: diabetic foot syndrome
DTAP: diagnostic-therapeutic-assistance program
HbA1c: hemoglobin A1c
NAFLD: nonalcoholic fatty liver disease
PAD: peripheral arterial disease
MM and CC conceived and designed this study. MM, AC, PA and FG designed the statistical analysis and analyzed the data. MM, FG, CC, AC and LR interpreted the results. MM wrote the first draft of manuscript. MM, FG, CC and LR contributed to the writing of the manuscript. All authors have read and confirmed the data in the manuscript and they can take the responsibility for the integrity of the data and the accuracy of the data analysis, read and approved the submitted version.
The authors declare that they have no conflict of interest.
The study was approved by the local Ethics Committee (reference number 855/2019).
Informed consent to participate in the study was obtained from all participants.
Not applicable.
The raw data supporting the conclusions of this manuscript will be made available by the authors to any qualified researcher. The datasets generated and/or analyzed during the current study are not publicly available as they are held by AOU Modena Health Organization as an integral part of their statutory activity. Any request for access should be directly submitted to Principal Investigator/Author.
Not applicable.
© The Author(s) 2021.
Copyright: © The Author(s) 2021. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 5773
Download: 36
Times Cited: 0
Alessandro Mantovani ... Giovanni Targher
Agostino Milluzzo ... Laura Sciacca
Erika Pedone ... Amelia Caretto
Roberta Malaguarnera ... Salvatore Piro