Original Article
Original Article

Affiliation:
1Department of Nursing, School of Nursing and Midwifery, Birjand University of Medical Science, Birjand 9717853577, Iran
ORCID: https://orcid.org/0000-0003-4404-960X
Affiliation:
1Department of Nursing, School of Nursing and Midwifery, Birjand University of Medical Science, Birjand 9717853577, Iran
Email: soleimanitoktam1374@gmail.com
ORCID: https://orcid.org/0009-0003-7777-387X
Affiliation:
2Department of Epidemiology and Biostatistics, School of Health, Social Determinants of Health Research Center, Birjand University of Medical Sciences, Birjand 32048321, Iran
Email: alesaleh70@yahoo.com
ORCID: https://orcid.org/0000-0001-7642-5214
Affiliation:
3Department of Cardiology, Dey 9th Hospital, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh 9516915169, Iran
Affiliation:
4Department of Complementary and Chinese Medicine, Persian and Complementary Medicine Faculty, Mashhad University of Medical Sciences, Mashhad 9177899191, Iran
ORCID: https://orcid.org/0000-0002-5756-0952
Explor Med. 2025;6:1001319 DOI: https://doi.org/10.37349/emed.2025.1001319
Received: December 23, 2024 Accepted: March 17, 2025 Published: May 21, 2025
Academic Editor: Yingyong Zhao, Northwest University, China
Aim: The present study determined the effect of acupressure on anxiety, fatigue, and blood pressure in hemodialysis patients.
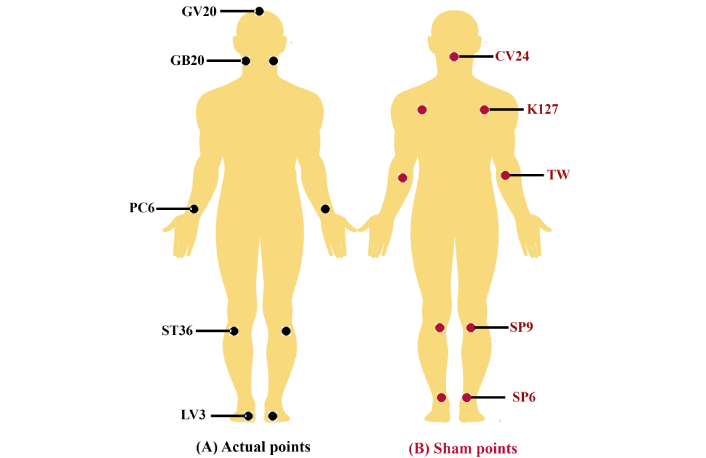
Methods: This randomized controlled clinical trial study was conducted on hemodialysis patients referred to the Dey 9th Hospital in Torbet Haydarieh. Data were collected through Spielberger’s State-Trait Anxiety (STAI) and Piper’s fatigue questionnaires. The intervention group received acupressure massage at the rate of 3 to 4 kg for 10 minutes, three times a week and for 4 weeks at 9 real points [PC6 or Nei guan, GV20 and ST36 (both feet)] and the sham group at the false points [SP9 (2 points), CV24, SP6, KI27 and TW6] were received by the thumb pulp of the therapist’s hand and before the start of dialysis. No intervention was performed in the control group. Blood pressure was measured for 8 weeks [one session per week and three times per session (before dialysis, one hour after the start of dialysis, and at the end of dialysis)]. Data analysis was done with SPSS 21 software and one-way analysis of variance, repeated measures ANOVA, and chi-square statistical tests at a significance level of p-value < 0.05.
Results: There was no statistically significant difference between the studied groups in demographic characteristics. Changes in the mean score of anxiety, fatigue, and mean systolic and diastolic blood pressure in the intervention group decreased significantly more than the sham and control groups one month after the end of the intervention (p-value < 0.05). Also, performing acupressure in real points effectively reduces hemodialysis patients’ anxiety, fatigue, and systolic and diastolic blood pressure in the long term (p-value < 0.05).
Conclusions: Acupressure, as a non-pharmacological intervention of traditional medicine, which is a simple, easy, cheap, and non-invasive method, has a significant effect on reducing anxiety, fatigue, and blood pressure in hemodialysis patients [registered in the Iranian Registry of Clinical Trials (IRCT) at https://irct.behdasht.gov.ir/ with the code IRCT20221223056899N1].
Chronic renal disease, especially end-stage renal disease (ESRD), is one of the leading causes of death and disability worldwide [1, 2]. During the last ten years, the mortality related to renal disease has increased by 31.7% [3], and more than one million people in the world die annually due to ESRD [4]. More than 20 to 27 million Americans suffer from renal failure, of which about 600,000 people are treated, which costs about 35 billion dollars per year [5, 6].
The prevalence of chronic renal failure in the Iranian adult population is estimated at 27.5%, which is reported to be 24% in men and more than 30% in women [7].
Chronic renal failure occurs when the function of the kidney is reduced to less than 15% of the normal limit [8] or glomerular filtration is reduced to less than 15 mL/min/1.73 m2 [9] which causes a disturbance in the metabolism of water and electrolytes in the body due to uremia [10]. Among the alternative treatment methods for renal disorders, renal transplantation, hemodialysis, and peritoneal dialysis are the most common methods to remove waste materials and products from the body when the kidneys are underworked and severely disabled [11, 12].
Hypertension is not only one of the most important causes of end-stage chronic renal failure, but it remains a significant prevalence in dialysis patients, as if not properly treated, leads to cardiovascular diseases (the most common cause of death in renal failure patients) and ultimately leads to death among dialysis patients. The prevalence of hypertension in hemodialysis patients is about 80–100% [13].
Controlling hemodynamic status, especially blood pressure, is a routine and vital procedure in dialysis departments that provides immediate and accessible information about the patient’s cardiovascular function and enables immediate response and treatment for acute and potential problems of the disease [14].
Anxiety, as one of the most common health problems and the second most important cause of disability around the world [15], is very common (22–53%) in dialysis patients and is associated with adverse clinical symptoms [16]. In addition to it, fatigue and lack of energy are other common and distressing symptoms among these patients, which it’s chronic and debilitating nature results in a reduction in self-care activities, a limitation in playing a role, and a decline in a person’s ability to perform daily life activities [17] and functional impairment [1]. These issues may lead to job loss, elevated healthcare dependency, and increased mortality [18]. In Iran, between 60% and 97% of hemodialysis patients suffer from severe fatigue [19].
The treatment of anxiety, fatigue, and blood pressure is done in two methods: pharmacological and non-pharmacological. The former is the most effective means available to nurses to reduce patients’ anxiety, fatigue, and blood pressure, but due to side effects and differences in their responses, it is important to use non-pharmacological methods to reduce these problems [20]. Due to their lower cost, fewer complications, and ease of implementation in clinical settings, nonpharmacological methods are more widely used than pharmaceutical methods [21, 22]. Non-pharmacological methods of controlling anxiety, fatigue, and blood pressure include the use of complementary medicine, including acupuncture, acupressure, therapeutic massage, aromatherapy, yoga, energy therapy, etc. [23]. The general goal of acupressure is to raise the body’s energy. Based on this, certain points in the body are known as acupuncture points. These points are highly capable of directing energy [24, 25]. In general, the use of acupressure is known as an easy, cheap, fast, safe, and non-drug technique in the treatment of disease [15].
Although the results of various studies indicate the effect of acupressure on patients’ anxiety, fatigue, and blood pressure [26, 27], some studies have also cited that there is a lack of impact of acupressure on patients’ anxiety and depression [28]. Therefore, considering these contradictions in the findings and the limitations of the studies conducted in hemodialysis patients, as well as the high cost and side effects of pharmacological treatments [29], the present study aims to determine the effect of acupressure on anxiety, fatigue, and blood pressure of the treated patients with hemodialysis.
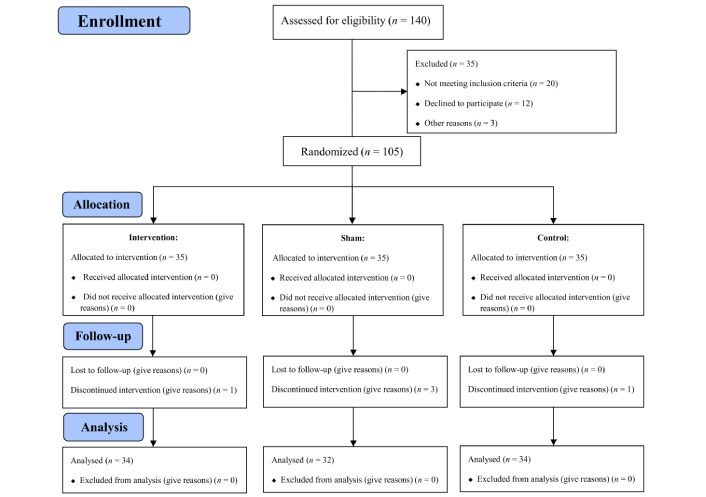
In this randomized controlled clinical trial study with a pre- and post-design, which was conducted based on the CONSORT 2010 checklist, the statistical population included all 140 hemodialysis patients referred to the dialysis department of the Dey 9th Hospital in Torbet Haydarieh in 2022, who met the inclusion criteria.
All patients with the following criteria were included in the study:
At least 18 years old
Dialysis treatment for at least 6 months
Perform dialysis at least 2 times a week, and each time for 3–4 hours
Absence of contraindications to acupressure, such as wounds, fractures, blisters, and other irritating skin lesions at the acupressure points
No limb amputation or wound at the massage site
Absence of physical disability or clear mental disorder that makes the patient unable to take care of himself
Inability to communicate verbally
Having full consciousness
Ability to listen and speak
Not taking sedatives such as benzodiazepines
Willingness to cooperate in the study
Patients who had one of the following conditions during the study were excluded from the study:
Performing a kidney transplant or peritoneal dialysis during research
Suffering from hemodynamic complications in most dialysis sessions
Hospitalization of the patient during intervention
The occurrence of a severely stressful event, such as the death of a first-degree relative
Travel or death of the patient
Unwillingness to continue cooperation in the study
Considering the average effect size equal to 0.32, 95% confidence limit, and 80% power, the sample size was estimated to be 99 people, and taking into account the drop in the final sample size, it was considered as 105 people, with 35 people in each group. A total of 105 participants were selected by the available sampling method and randomly divided into three acupressure groups (35 people), sham points (35 people), and control (35 people).
To balance the number of samples allocated to each of the study groups, the eligible participants were divided into three groups in the randomized block sampling method.
According to the sample size, by using Excel software, 17 blocks of 6 and one block of 3 were created with different and random combinations in terms of the order of letters A, B, and C. Blocks of 6 included two letters A, two letters B, two letters C, and blocks of three included one of these three letters. Letter A corresponds to the intervention group, letter B corresponds to the sham group, and letter C corresponds to the control group. Then, at each stage, based on the table of random numbers, a block was randomly selected, and based on it, participants were assigned to one of the three intervention, sham, and control groups. This process continued until the sample size was completed.
In this study, the required data were collected through a demographic information questionnaire, Spielberger’s State-Trait Anxiety (STAI) questionnaire, and Piper’s fatigue questionnaire. Demographic information included gender, age, education level, marital status, and occupation.
The STAI has 40 self-report options that measure the first 20 options of state anxiety and the next 20 options of trait anxiety. The state form of this questionnaire is based on a 4-point Likert scale from very low (score 1) to very high (score 4), and the adjective form is scored based on a 4-point Likert scale from never (score 1) to always (score 4). The minimum score for each of the mood and adjective forms is 20, and the maximum score is 80. In a concurrent criterion validity research of this questionnaire, it has been reviewed and confirmed [30]. In a study by Salari et al. (2013) [31], the reliability of this questionnaire was reported as 0.89 using the Cronbach’s alpha method. Piper’s fatigue questionnaire has 27 questions in four domains: behavioral/intensity, emotional, sensory, and cognitive/mood. Questions 2 to 23 of the questionnaire are scored based on the 11-point Likert scale from 0 to 10, and the average total score of this scale is between 0 and 10. A higher score indicates a higher level of fatigue. The other 5 questions of this questionnaire are qualitative data only to enrich the scale and are not calculated in scoring. The validity and reliability of this questionnaire have been confirmed in international and national studies in different patients [30, 31]. In which the reliability of this questionnaire was reported as 0.98 using the Cronbach’s alpha method [32].
Objectives of the study were explained to the patients, and after that, the patients agreed to cooperate in the study, they completed the demographic profile form and STAI questionnaires, Piper’s fatigue, and their blood pressure was recorded. Consequently, for the patients of the acupressure group, massage was performed on PC6 or Nei guan points, GV20, and ST36 (both legs) in total (9 points). Sham points group patients received acupressure on false points on which applying pressure has no soothing effect, in the form of massage on two points SP9, which is inside the leg at the junction of the tibial shaft and the tibial condyle in a depression (to instead of ST36) and the CV24 point, which is exactly between the chin and the lower lip on the front midline of the body in the middle of the lip-chin distance (instead of GV20), also the SP6 point (instead of LV3), the KI27 point (instead of GB20) and the TW6 point (instead of PC6) was done (Figure 1).
For both the intervention and sham groups, massage was performed by the therapist’s thumb pulp (nurse with a certified course) with a pressure of 3 to 4 kg for 10 minutes three times a week for 4 weeks, while in the control group, no intervention was performed on the patients. The patient would feel heaviness, numbness, and warmth at the pressure point if it was performed correctly [32]. All three groups of patients received routine ward care. After the end of the intervention and one month after the end of the intervention, the examined questionnaires were completed again by the patients of all three groups.
The blood pressure of patients was measured on five occasions (first, second, third, fourth, and eighth week) and three times each occasion (before dialysis, one hour after the start of dialysis, and end of dialysis).
In this study, the patients were not aware of the exact location of the points. In this study, the research assistant was used to help complete all questionnaires to blind and prevent bias in the results. In this way, the research assistant would not be aware of the groupings and the type of interventions performed by each group and individual.
Data analysis was done using SPSS 21 software and according to the normality of distribution of variables, with chi-square statistical tests, one-way analysis of variance, and one-way repeated measures ANOVA for comparing the repeated measures in the first, second, third, fourth, and eighth weeks. A significance level of p-value < 0.05 was considered.
Obtaining permission from the research ethics committee of Birjand University of Medical Sciences was approved with the code of IR.BUMS.REC.1400.443 and was registered in the Iranian Registry of Clinical Trials (IRCT) at https://irct.behdasht.gov.ir/ with the code IRCT20221223056899N1. In addition, informed consent was obtained from the participants before the implementation of the study, and during the implementation of the study, the patients could not continue their cooperation with the project if they were not willing to participate anymore.
Among the 105 patients who agreed to participate in the study, 100 completed post-tests 1 and 2, including 34 people in the intervention group (acupressure of real points), 32 people in the sham group (acupressure of unreal points), and 34 people in the control group (Figure 2). The mean age of the participants was 54.66 ± 15.04 years, and each patient underwent dialysis for an average time of 4.23 ± 3.12 hours per month. A total of 55% of the participants were male. The results of the statistical analysis showed that there was no significant difference in the demographic variables of the participants in the study. The demographic information of the participants according to the study groups is presented in Table 1.
Distribution of demographic characteristics of participants by intervention, sham, and control groups
| Item | Group | p-value | |||
|---|---|---|---|---|---|
| Intervention (N = 34) (%) | Sham (N = 32) (%) | Control (N = 34) (%) | |||
| Sex | Male | 15 (44.1) | 22 (68.7) | 18 (52.9) | 0.127* |
| Female | 19 (55.9) | 10 (31.3) | 16 (47.1) | ||
| Job | Unemployed | 16 (47.1) | 11 (34.4) | 16 (47.1) | 0.642* |
| Freelance job | 6 (17.6) | 7 (21.9) | 7 (20.6) | ||
| Employed | 5 (14.7) | 6 (18.8) | 8 (23.5) | ||
| Pensioner | 7 (20.6) | 8 (25.0) | 3 (8.8) | ||
| Marriage status | Married | 29 (85.3) | 25 (78.1) | 26 (76.5) | 0.212* |
| Single | 3 (8.8) | 3 (9.4) | 4 (11.8) | ||
| Divorced | 2 (5.9) | 3 (9.4) | 0 (0.0) | ||
| Widow | 0 (0.0) | 1 (3.1) | 4 (11.8) | ||
| Education | Illiterate | 3 (8.8) | 7 (21.9) | 6 (17.6) | 0.387* |
| Primary | 8 (23.5) | 7 (21.9) | 4 (11.8) | ||
| Guidance | 1 (2.9) | 1 (3.1) | 2 (5.9) | ||
| High school | 12 (35.3) | 7 (21.9) | 4 (11.8) | ||
| University | 10 (29.4) | 10 (31.3) | 18 (52.9) | ||
| Age (Mean ± SD) | 52.91 ± 15.38 | 54.62 ± 14.37 | 56.44 ± 15.54 | 0.631** | |
| Average time of hemodialysis per month (hours) | 5.03 ± 4.28 | 3.38 ± 2.14 | 4.24 ± 2.30 | 0.098** | |
SD: standard deviation; * chi-square; ** one-way ANOVA
The results showed that the average anxiety score in dialysis patients in the intervention group decreased from 129.82 ± 21.95 to 125.35 ± 20.44 in one month after the end of the intervention, and this change was statistically significant (p-value < 0.0001). However, in the same period, the average anxiety score increased in the dialysis patients of the sham and control groups, but this trend was not statistically significant (p-value = 0.580 and p-value = 0.325, respectively) (Table 2).
Comparison of mean anxiety among the study groups (before, at the end of the intervention, and one month after the end of the intervention)
| Time | Intervention (Mean ± SD) | Sham (Mean ± SD) | Control (Mean ± SD) | Test result* | ||
|---|---|---|---|---|---|---|
| Test statistics | p-value | |||||
| Before intervention (Time 1) | 129.82 ± 21.95 | 126.81 ± 20.66 | 133.00 ± 14.59 | 0.847 | 0.432 | |
| End of the intervention (Time 2) | 120.53 ± 19.75 | 126.34 ± 21.48 | 132.94 ± 14.71 | 3.705 | 0.028 | |
| One month after the end of the intervention (Time 3) | 125.35 ± 20.44 | 127.06 ± 21.13 | 133.12 ± 14.38 | 1.587 | 0.210 | |
| p-value | < 0.0001 | 0.580 | 0.325 | - | - | |
| Score differences during intervention times | Time 2 – Time 1 | –9.29 ± 6.31 | –0.47 ± 3.88 | –0.06 ± 0.34 | 49.866 | < 0.0001 |
| Time 3 – Time 1 | –4.47 ± 4.31 | 0.25 ± 2.53 | 0.12 ± 0.69 | 28.536 | < 0.0001 | |
| Results of variance analysis of one-way repeated measures | Group and time interaction | - | - | - | 28.536 | < 0.0001 |
| Group effect | - | - | - | 1.617 | 0.204 | |
| Time effect | - | - | - | 21.948 | < 0.0001 | |
SD: standard deviation; -: not applicable; * one-way repeated measures ANOVA
Also, the average anxiety score in the intervention group at the end of the intervention is significantly lower than the sham and control groups (p-value = 0.028), but one month after the intervention, this difference is not significant (p-value = 0.210). The average changes in the anxiety score at the end of the intervention and a month after the end of the intervention, compared to before the intervention, are significantly higher in the intervention group than in the sham and control groups (p-value < 0.0001). The results of the analysis of the variance test with repeated measurements also revealed that the effect of time (p-value < 0.0001) and the interaction effect of group and time (p-value < 0.0001) are significant in raising the anxiety score, which means that performing acupressure on real points. In addition, the time interval between performing acupressure and measuring anxiety in patients is effective in reducing the anxiety score in dialysis patients (Table 2).
Comparison of fatigue in intervention, sham, and control group patients before and after the intervention.
Based on the findings of the study, the average fatigue score of dialysis patients in the intervention group decreased from 141.06 ± 39.54 to 131.94 ± 37.04 one month after the end of the intervention, which was statistically significant (p-value < 0.0001). There is a decline in the average score of fatigue in the sham group dialysis patients, which was also statistically significant one month after the end of the intervention (p-value = 0.031). However, in the control group, this change was not statistically significant (p-value = 0.459) (Table 3).
Comparison of the average fatigue among the study groups (before, at the end of the intervention, and one month after the end of the intervention)
| Time | Intervention (Mean ± SD) | Sham (Mean ± SD) | Control (Mean ± SD) | Test result* | ||
|---|---|---|---|---|---|---|
| Test statistics | p-value | |||||
| Before intervention (Time 1) | 141.06 ± 39.54 | 138.59 ± 33.25 | 151.44 ± 24.79 | 1.420 | 0.247 | |
| End of the intervention (Time 2) | 124.29 ± 38.36 | 135.16 ± 38.74 | 149.67 ± 23.16 | 4.741 | 0.011 | |
| One month after the end of the intervention (Time 3) | 131.94 ± 37.04 | 137.28 ± 35.03 | 150.09 ± 23.04 | 2.838 | 0.063 | |
| p-value | < 0.0001 | 0.031 | 0.459 | - | - | |
| Score differences during intervention times | Time 2 – Time 1 | –16.76 ± 7.76 | –3.44 ± 7.24 | –1.76 ± 10.29 | 31.140 | < 0.0001 |
| Time 3 – Time 1 | –9.12 ± 6.23 | –1.31 ± 3.29 | –1.35 ± 10.59 | 12.519 | < 0.0001 | |
| Results of variance analysis of one-way repeated measures | Group and time interaction | - | - | - | 12.519 | < 0.0001 |
| Group effect | - | - | - | 2.729 | 0.070 | |
| Time effect | - | - | - | 28.381 | < 0.0001 | |
SD: standard deviation; -: not applicable; * one-way repeated measures ANOVA
Therefore, it can be said that performing acupressure at real and unreal points is effective in reducing anxiety, fatigue, and blood pressure in dialysis patients.
Also, the results of the study demonstrated that the average fatigue score in the intervention group at the end of the intervention is significantly lower than the sham and control groups (p-value = 0.011), but one month after the intervention, this difference is not significant (p-value = 0.063). The average changes in the fatigue score at the end of the intervention and one month after the end of the intervention, compared to before the intervention, are significantly higher in the intervention and sham groups than in the control group (p-value < 0.0001 and p-value = 0.031, respectively).
Also, the results of the analysis of variance with repeated measurements show that the effect of time (p-value < 0.0001) and the interaction effect of group and time (p-value < 0.0001) are significant in reducing the fatigue score, which means that doing acupressure in real points and unreal and the time interval between doing acupressure and measuring fatigue in patients is effective in diminishing fatigue in dialysis patients (Table 3).
The average size of systolic blood pressure in dialysis patients in the intervention group before dialysis decreased from 131.03 ± 22.59 to 120.29 ± 17.79 mmHg in one month after the end of the intervention, which was statistically significant (p-value < 0.0001). This measure at the end of dialysis reduced from 120.15 ± 24.29 to 109.41 ± 17.40 mmHg in one month after the end of the intervention, which was statistically significant (p-value < 0.0001).
The average size of systolic blood pressure in dialysis patients in the sham and control groups before dialysis increased one month after the end of the intervention, which was not statistically significant (p-value = 0.752 and p-value = 0.118, respectively). This measure decreased at the end of dialysis, one month after the end of the intervention in the sham group, which was not statistically significant (p-value = 0.452), but it increased significantly in the control group (p-value = 0.022).
As demonstrated in Table 4, the mean systolic blood pressure in the patients of the intervention group before dialysis, one hour after the start of dialysis and at the end of dialysis, one month after the end of the intervention, was significantly different from the sham and control groups (p-value = 0.040, p-value = 0.042, and p-value = 0.024, respectively). At other times [first, second, third, and fourth week (end of intervention)], no significant difference was observed.
Comparison of the before, one hour after starting dialysis, and end of dialysis systolic blood pressure (mmHg) mean in the studied groups in the before, during, end, and one month after intervention
| Times during the hemodialysis sessions | First week | Second week | Third week | Fourth week | Eighth week | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | |
| Before starting dialysis | 131.03 ± 22.59 | 129.53 ± 22.44 | 130.88 ± 22.44 | 127.79 ± 23.16 | 126.09 ± 22.81 | 127.50 ± 22.87 | 133.09 ± 23.84 | 131.72 ± 23.91 | 132.35 ± 23.33 | 128.68 ± 24.16 | 126.72 ± 23.54 | 128.38 ± 23.82 | 120.29 ± 17.79 | 130.78 ± 20.48 | 132.35 ± 23.84 |
| p-value | 0.957 | 0.950 | 0.973 | 0.938 | 0.040 | ||||||||||
| One hour after starting dialysis | 123.68 ± 23.81 | 122.97 ± 22.43 | 123.38 ± 23.54 | 123.09 ± 23.29 | 122.34 ± 23.07 | 123.09 ± 22.59 | 122.64 ± 21.78 | 124.06 ± 23.12 | 125.14 ± 22.91 | 121.62 ± 24.55 | 122.66 ± 25.90 | 123.82 ± 25.23 | 114.85 ± 18.69 | 125.47 ± 21.30 | 126.00 ± 20.58 |
| p-value | 0.992 | 0.989 | 0.901 | 0.937 | 0.042 | ||||||||||
| End of dialysis | 120.15 ± 24.29 | 118.59 ± 24.20 | 119.12 ± 23.69 | 120.59 ± 22.18 | 118.75 ± 21.51 | 120.29 ± 22.19 | 123.82 ± 22.16 | 122.81 ± 22.47 | 123.09 ± 22.29 | 121.76 ± 24.43 | 120.00 ± 24.10 | 121.03 ± 23.86 | 109.12 ± 17.47 | 115.47 ± 21.57 | 123.09 ± 22.86 |
| p-value | 0.965 | 0.936 | 0.982 | 0.957 | 0.024 | ||||||||||
| p-value | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 |
SD: standard deviation
The results of a one-way analysis of variance with repeated data showed that the effect of time (p-value = 0.007) and the interaction effect of time and group (p-value < 0.0001) in reducing the systolic blood pressure of patients before dialysis are significant. The interaction effect of time and group (p-value = 0.011) is significant in declining the systolic blood pressure of patients, one hour after dialysis. Also, the effect of time (p-value = 0.045) and the interaction effect of time and group (p-value < 0.0001) in reducing the systolic blood pressure of patients at the end of dialysis were significant (Table 5).
Comparing means of systolic blood pressure (mmHg) in the study groups (before, at the end of the intervention, and one month after the end of the intervention) (results of repeated measures ANOVA analysis)
| Time | Group effect | Time effect | Group and time interaction |
|---|---|---|---|
| Before intervention (Time 1) | 0.923 | 0.007 | < 0.0001 |
| End of the intervention (Time 2) | 0.836 | 0.279 | 0.011 |
| One month after the end of the intervention (Time 3) | 0.890 | 0.045 | < 0.0001 |
The average changes in systolic blood pressure in the intervention group at all three times before dialysis (p-value = 0.001), one hour after dialysis (p-value < 0.0001) and at the end of dialysis (p-value < 0.0001), one month after the end of the intervention, was significantly different from sham and control groups (Table 6 and Figure 3).
Comparison of the before, one hour after starting dialysis, and end of dialysis systolic blood pressure (mmHg) mean in the studied groups in the before, during, end, and one month after intervention
| Times during the hemodialysis sessions | Comparison time | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | p-value |
|---|---|---|---|---|---|
| Before starting dialysis | First and second week | –3.23 ± 6.26 | –3.43 ± 6.40 | –3.38 ± 6.24 | 0.991 |
| First and third week | 2.05 ± 8.71 | 2.19 ± 8.97 | 1.47 ± 9.34 | 0.942 | |
| First and fourth week | –2.35 ± 7.90 | –2.81 ± 7.92 | –2.50 ± 7.81 | 0.971 | |
| First and eighth week | –10.73 ± 7.79 | 1.25 ± 9.33 | 1.47 ± 5.44 | 0.001 | |
| One hour after starting dialysis | First and second week | –0.59 ± 6.12 | –0.62 ± 6.12 | 0.29 ± 5.76 | 0.970 |
| First and third week | –1.03 ± 8.24 | 1.09 ± 7.27 | 1.76 ± 6.26 | 0.263 | |
| First and fourth week | –2.06 ± 8.36 | –0.31 ± 9.15 | 0.44 ± 7.52 | 0.453 | |
| First and eighth week | –8.82 ± 10.66 | 2.50 ± 7.40 | 2.62 ± 10.56 | < 0.0001 | |
| End of dialysis | First and second week | 0.44 ± 7.22 | 0.16 ± 7.46 | 1.18 ± 7.18 | 0.841 |
| First and third week | 3.67 ± 6.99 | 4.22 ± 6.85 | 3.97 ± 7.05 | 0.951 | |
| First and fourth week | 1.62 ± 7.55 | 1.41 ± 7.75 | 1.91 ± 7.39 | 0.963 | |
| First and eighth week | –11.03 ± 12.84 | –3.12 ± 18.69 | 3.97 ± 10.28 | < 0.0001 |
SD: standard deviation
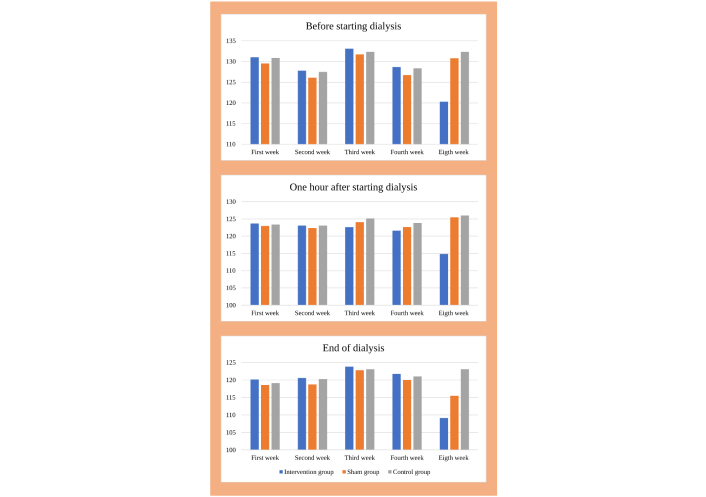
Comparison of the before, one hour after starting dialysis, and end of dialysis systolic blood pressure (mmHg) mean in the studied groups in the before, during, end, and one month after intervention
Therefore, it can be concluded that performing acupressure in real points is effective in reducing the systolic blood pressure of dialysis patients in the long term.
The average size of diastolic blood pressure in dialysis patients in the intervention group before dialysis decreased from 82.94 ± 13.09 to 76.47 ± 8.47 mmHg in one month after the end of the intervention, which was statistically significant (p-value < 0.0001). At the end of dialysis, this measure reduced from 74.70 ± 10.36 to 63.23 ± 6.38 mmHg in one month after the end of the intervention, which was statistically significant (p-value < 0.0001).
However, the observed decrease in the average size of diastolic blood pressure in sham group dialysis patients before dialysis and at the end of dialysis, one month after the end of the intervention, was not statistically significant (p-value = 0.931 and p-value = 0.081, respectively). Also, the average size of diastolic blood pressure before dialysis and at the end of dialysis in dialysis patients of the control group increased one month after the end of the intervention, which was not statistically significant (p-value = 0.110 and p-value = 0.943, respectively). More details are given in Table 7.
Comparison of the before, one hour after starting dialysis, and end of dialysis diastolic blood pressure (mmHg) mean in the studied groups in the before, during, end, and one month after intervention
| Times during the hemodialysis sessions | First week | Second week | Third week | Fourth week | Eighth week | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | |
| Before starting dialysis | 82.94 ± 13.09 | 82.19 ± 13.13 | 82.65 ± 12.81 | 79.1 ± 12.64 | 78.44 ± 12.01 | 78.82 ± 12.37 | 77.06± 11.68 | 77.34 ± 12.82 | 77.79 ± 13.38 | 75.5 ± 10.57 | 80.93 ± 10.71 | 81.47 ± 12.22 | 76.47 ± 8.47 | 80.78 ± 10.71 | 83.09 ± 10.87 |
| p-value | 0.972 | 0.975 | 0.985 | 0.076 | 0.026 | ||||||||||
| One hour after starting dialysis | 76.47 ± 12.70 | 75.62 ± 12.62 | 76.32 ± 12.57 | 75.44 ± 12.45 | 74.53 ± 12.27 | 75.29 ± 12.30 | 71.56 ± 11.07 | 71.25 ± 11.12 | 71.62 ± 11.26 | 67.94 ± 7.70 | 67.81 ± 7.92 | 70.14 ± 8.48 | 69.71 ± 9.29 | 74.37 ± 10.30 | 77.65 ± 11.09 |
| p-value | 0.959 | 0.950 | 0.982 | 0.412 | 0.007 | ||||||||||
| End of dialysis | 74.71 ± 10.37 | 74.70 ± 10.35 | 74.56 ± 10.25 | 74.71 ± 11.61 | 73.75 ± 11.29 | 74.71 ± 11.41 | 71.32 ± 10.61 | 70.78 ± 10.71 | 71.62 ± 10.99 | 69.12 ± 7.53 | 71.25 ± 11.29 | 74.11 ± 11.51 | 63.23 ± 6.38 | 72.81 ± 10.15 | 75.00 ± 11.87 |
| p-value | 0.965 | 0.927 | 0.950 | 0.136 | < 0.0001 | ||||||||||
| p-value | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 | < 0.0001 |
SD: standard deviation
Therefore, it can be said that performing acupressure on real points is effective in reducing the anxiety, fatigue, and blood pressure of dialysis patients.
Based on the results of the study (Table 7), the average diastolic blood pressure in the patients of the intervention group before dialysis, one hour after the start of dialysis and at the end of dialysis, one month after the end of the intervention was significantly different from the sham and control groups (p-value = 0.026, p-value = 0.007 and p-value < 0.0001, respectively). At other times [first, second, third, and fourth week (end of intervention)], no significant difference was observed.
The results of a one-way analysis of variance with repeated data showed that the effect of time (p-value < 0.0001) in reducing the diastolic blood pressure of patients before dialysis is significant. The effect of time (p-value < 0.0001) and the interaction effect of time and group (p-value < 0.0001) are significant in reducing the diastolic blood pressure of patients, one hour after dialysis. Also, the effect of time (p-value < 0.0001) and the interaction effect of time and group (p-value < 0.0001) in reducing the diastolic blood pressure of patients at the end of dialysis were significant (Table 8).
Comparing mean diastolic blood pressure (mmHg) in the study groups (before, at the end of the intervention, and one month after the end of the intervention) (results of repeated measures ANOVA analysis)
| Time | Group effect | Time effect | Group and time interaction |
|---|---|---|---|
| Before intervention (Time 1) | 0.949 | < 0.0001 | 0.109 |
| End of the intervention (Time 2) | 0.704 | < 0.0001 | < 0.0001 |
| One month after the end of the intervention (Time 3) | 0.332 | < 0.0001 | < 0.0001 |
The average changes in diastolic blood pressure in the intervention group before dialysis (p-value < 0.0001) and at the end of dialysis (p-value = 0.011) were significantly different from the sham and control groups at the end of the intervention. Also, the average diastolic blood pressure changes in the intervention group at all three times before dialysis (p-value = 0.002), one hour after dialysis (p-value = 0.002), and at the end of dialysis (p-value < 0.0001). One month after the end of the intervention, it was significantly different from the sham and control groups (Table 9 and Figure 4).
Comparison of the before, one hour after starting dialysis, and end of dialysis diastolic blood pressure (mmHg) mean in the studied groups in the before, during, end, and one month after intervention
| Times during the hemodialysis sessions | Comparison time | Intervention (N = 34) (Mean ± SD) | Sham (N = 32) (Mean ± SD) | Control (N = 34) (Mean ± SD) | p-value |
|---|---|---|---|---|---|
| Before starting dialysis | First and second week | –3.82 ± 4.27 | –3.75 ± 4.58 | –3.82 ± 4.27 | 0.997 |
| First and third week | –5.88 ± 5.57 | –4.84 ± 7.56 | –4.85 ± 7.53 | 0.780 | |
| First and fourth week | –7.35 ± 6.99 | –1.25 ± 5.54 | –1.18 ± 5.51 | < 0.0001 | |
| First and eighth week | –6.47 ± 8.12 | –1.42 ± 9.34 | 0.44 ± 5.12 | 0.002 | |
| One hour after starting dialysis | First and second week | –1.03 ± 2.69 | –1.09 ± 2.76 | –1.03 ± 2.93 | 0.994 |
| First and third week | –4.71 ± 5.36 | –4.37 ± 5.35 | –4.70 ± 5.49 | 0.960 | |
| First and fourth week | –8.53 ± 7.74 | –7.81 ± 7.40 | –6.17 ± 7.79 | 0.443 | |
| First and eighth week | –6.76 ± 9.60 | –1.25 ± 11.50 | 1.32 ± 6.43 | 0.002 | |
| End of dialysis | First and second week | 0.00 ± 3.01 | –0.31 ± 2.82 | 0.14 ± 7.23 | 0.926 |
| First and third week | –3.38 ± 4.21 | –3.28 ± 4.33 | –2.94 ± 4.79 | 0.913 | |
| First and fourth week | –5.59 ± 8.42 | –2.81 ± 6.71 | –0.44 ± 5.13 | 0.011 | |
| First and eighth week | –11.47 ± 8.40 | –1.25 ± 5.54 | 0.44 ± 10.90 | < 0.0001 |
SD: standard deviation
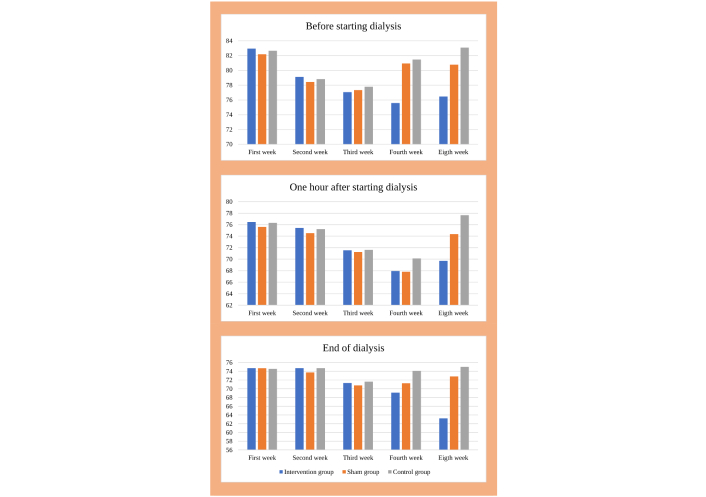
Comparison of the before, one hour after starting dialysis, and end of dialysis diastolic blood pressure (mmHg) mean in the studied groups in the before, during, end, and one month after intervention
Therefore, it can be concluded that performing acupressure in real points can be effective in reducing the diastolic blood pressure of dialysis patients in the short and long term.
The findings of the current study demonstrated that in the intervention group, the average anxiety score decreased significantly one month after the intervention, but in the sham and control groups, there was no significant difference in the anxiety score before and one month after the intervention. Also, the average changes in the anxiety score at the end of the intervention and one month after the end of the intervention, compared to the pre-intervention, were significantly higher in the intervention group than in the sham and control groups. In other words, performing acupressure at real points and the time interval between performing acupressure and measuring anxiety in patients has been effective in reducing anxiety scores in dialysis patients. Siasari et al. (2020) [33] found that the average score of depression and anxiety after the intervention in the acupressure group patients was significantly lower than the control group. In this context, Moradi et al. (2015) [34] concluded that acupressure can reduce anxiety in patients undergoing hemodialysis treatment. Furthermore, Cho et al. (2021) [26] reported that acupressure for 12 minutes and massage for 3 minutes a day, three days a week, for four weeks, reduces anxiety, depression, and fatigue in hemodialysis patients.
In contrast, the results of Mousavi et al.’s (2009) [35] study on the effect of acupressure therapy on students’ anxiety showed that acupressure had no effect on anxiety, which was not consistent with the results of the present study. Also, the results of Kafaei Atrian et al.’s research (2014) [36] showed that acupressure is not effective in reducing the anxiety of patients with dysmenorrhea. Probably, one of the reasons for this inconsistency is the difference in the way of implementing the intervention, its duration and the type of statistical population.
Acupressure can reduce anxiety and depression by regulating the concentration of neurotransmitters and reducing adrenocorticotropic and hydroxytryptophan hormones in neural pathways and improving relaxation [37]. One of the main mechanisms of acupressure in reducing patients’ anxiety and depression is increasing endorphins as a result of reducing pressure points [38]. Among the points of acupressure to relieve anxiety, it is named on the inner side of the forearm and in the cavity between the bones of the forearm, and the size of three finger widths above the fold of the wrist (point P6) [39].
Also, the results of the present study revealed that in the intervention and sham groups, the average fatigue score decreased significantly one month after the intervention compared to before, but in the control group, there was no significant difference in the fatigue score before and a month after the intervention. Also, the average changes in the fatigue score at the end of the intervention and a month after the end of the intervention, compared to before the intervention, were significantly higher in the intervention and sham groups than in the control group. In other words, performing acupressure in real and unreal points and the time interval between performing acupressure and measuring fatigue in patients has been effective in reducing fatigue in dialysis patients.
Eğlence et al. (2013) [40] and Kalani et al. (2019) [41] in 2 studies reported that acupressure is effective in declining fatigue in hemodialysis patients. Suandika et al. (2023) [42] found that in ESRD patients receiving hemodialysis, acupressure had a significant and independent impact on fatigue, depression/anxiety, and sleep quality. Also, Jones et al. (2015) [43] showed in a study that acupressure reduces anxiety, depression, and fatigue in hemodialysis patients. Also, the results of the meta-analysis by Liu et al. (2023) [44] showed that acupressure is effective and safe in treating sleep disorders, fatigue, depression, and pruritus in hemodialysis patients.
According to the theory of acupressure, fatigue is caused by a lack of energy or an imbalance of qi energy, and its recovery is achieved by focusing on adding and activating qi energy in the functioning of the main channels.
Acupressure causes the release of neurotransmitters such as serotonin, which can affect people’s sense of relaxation. Acupressure can also play a role in the treatment of fatigue through the fluctuation of cytokines and hormones [45].
In Valiee et al.’s (2012) [46] study, in the acupressure group, fatigue was significantly reduced in false points, which may be due to the psychological and physiological effects of massage.
The results of the current study revealed that in the intervention group, the average size of systolic and diastolic blood pressure decreased significantly one month after the intervention, but in the sham and control groups, there was a significant difference in the average size of systolic and diastolic blood pressure before and one month after the intervention.
The average changes in systolic and diastolic blood pressure in the intervention group at all three times before dialysis, an hour after dialysis, and at the end of dialysis, one month after the end of the intervention, were significantly different from the sham and control groups. In other words, performing acupressure in real points has been effective in reducing the systolic blood pressure of dialysis patients in the long term and in reducing the diastolic blood pressure of dialysis patients in the short and long term. In the study of Bassampour et al. (2008) [47] in patients undergoing abdominal surgery, a significant difference was observed between the average level of anxiety, average breathing rate, and systolic blood pressure in the before and after intervention and placebo groups.
Also, Barker et al. (2006) [48] in a study concluded that systolic blood pressure and diastolic blood pressure decreased and Chen et al.’s study (2005) [49] indicated a decrease in mean arterial blood pressure after the intervention.
Contrary to these cases, the results of Vasokolaei et al.’s study (2019) [50] titled “Effect of Acupressure on Anxiety and Hemodynamic Parameters in Female Patients with Acute Coronary Syndrome Hospitalized in Cardiac Care Unit: A Randomized Placebo Controlled Clinical Trial” showed that there is no significant difference between the hemodynamic variables in the two groups which are due to the difference in the places where acupressure is performed on the body.
In general, acupuncture and acupressure are among the non-pharmaceutical treatments that are receiving attention today even on the spontaneous rotation of a fetus with breech presentation [51], but considering that traditional acupuncture requires undressing the patient and performing an invasive intervention and is accompanied by an increased risk of acquired immunodeficiency syndrome and hepatitis, the trend of applying acupressure has increased [52].
This study has limitations, and the results should be interpreted with caution. The most important limitations of this study were the small sample size and single-center design. Therefore, future studies with larger sample sizes and multi-center considering the demographic variations are recommended.
In conclusion, according to the results of the present study, the acupressure intervention method, as a non-pharmacological method of traditional Chinese medicine, which is a simple, easy, cheap, and non-invasive method, has a significant effect on reducing anxiety, fatigue, and blood pressure in patients undergoing hemodialysis treatment.
ESRD: end-stage renal disease
STAI: Spielberger’s State-Trait Anxiety
MN: Conceptualization, Supervision, Validation, Writing—review & editing. TS: Conceptualization, Supervision, Data curation, Methodology, Formal analysis, Writing—original draft. HS: Supervision, Validation, Writing—review & editing, Formal analysis. RG and HBT: Supervision, Validation, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The research project, which obtained permission from the research ethics committee of Birjand University of Medical Sciences, was approved with the code of IR.BUMS.REC.1400.443 and was registered in the Iranian Registry of Clinical Trials (IRCT) at https://irct.behdasht.gov.ir/ with the code IRCT20221223056899N1.
Informed consent was obtained from the participants before the implementation of the study, and during the implementation of the study, the patients could not continue their cooperation with the project if they were not willing to participate anymore.
Not applicable.
The data are available on request from the corresponding author.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 9538
Download: 121
Times Cited: 0