Review
Review

Affiliation:
Department of Nutrition and Dietetics, Faculty of Health Sciences, Lokman Hekim University, Ankara 06510, Turkey
Email: dyt.mervesbah@gmail.com
ORCID: https://orcid.org/0009-0001-1045-3834
Affiliation:
Department of Nutrition and Dietetics, Faculty of Health Sciences, Lokman Hekim University, Ankara 06510, Turkey
ORCID: https://orcid.org/0009-0005-2605-4837
Affiliation:
Department of Nutrition and Dietetics, Faculty of Health Sciences, Lokman Hekim University, Ankara 06510, Turkey
ORCID: https://orcid.org/0000-0001-8690-1341
Explor Foods Foodomics. 2026;4:1010151 DOI: https://doi.org/10.37349/eff.2026.1010151
Received: March 16, 2026 Accepted: April 22, 2026 Published: May 21, 2026
Academic Editor: Marcello Iriti, Milan State University, Italy
Cardiovascular diseases remain a major global health burden, representing one of the leading causes of mortality and morbidity worldwide. A wide spectrum of conditions—such as coronary artery disease, hypertension, stroke, heart failure, and peripheral vascular disorders—is influenced not only by genetic predisposition, lifestyle behaviors, and environmental factors, but also by disturbances in redox balance. Oxidative stress occurs when the production of reactive oxygen species exceeds the capacity of antioxidant defense mechanisms. This imbalance plays a critical role in the pathogenesis of endothelial dysfunction, inflammatory processes, and atherosclerotic progression. In this regard, antioxidants contribute to cardiovascular protection by limiting oxidative damage and preserving cellular integrity. The detoxification of reactive oxygen species is mediated through complex biochemical pathways involving endogenous antioxidant systems, including enzymes such as superoxide dismutase, catalase, and glutathione peroxidase. In addition, exogenous antioxidants derived from the diet—such as vitamins A, C, and E, selenium, zinc, flavonoids, resveratrol, and lycopene—support these defense mechanisms. These compounds have also been associated with enhanced nitric oxide availability, improved vascular function, attenuation of inflammatory responses, and favorable modulation of lipid metabolism. Although these compounds have been associated with beneficial effects on cardiovascular health, the evidence is not entirely consistent, and some studies have reported non-significant findings. This review aims to evaluate both the biochemical mechanisms and clinical implications of antioxidants in cardiovascular disease, with a particular emphasis on nutrition-based preventive and therapeutic approaches.
Cardiovascular diseases (CVDs) constitute a major group of disorders, including conditions such as ischemic heart disease and stroke, and represent a leading cause of death worldwide, placing a considerable burden on public health [1]. Recent estimates from the World Health Organization indicate that nearly 19.8 million people died due to CVD in 2022, accounting for approximately one-third of all global deaths [2]. A comparable trend is also evident in Turkey. According to the 2024 mortality and cause-of-death data published by the Turkish Statistical Institute (TURKSTAT), circulatory system diseases rank as the leading cause of mortality, comprising 36.0% of all deaths [3].
Lifestyle-related factors characteristic of modern living—including chronic stress, sedentary behavior, poor dietary patterns, and environmental exposures—are closely associated with the rising prevalence of CVDs [4]. Many of these factors influence cardiovascular health by enhancing oxidative processes and stimulating inflammatory pathways. In this framework, oxidative stress is widely recognized as a key contributor to CVD development. It reflects a disruption in the balance between reactive oxygen species (ROS) generation and the body’s antioxidant defense capacity. Excessive oxidative load leads to endothelial injury, which in turn initiates inflammatory cascades and promotes the formation of atherosclerotic lesions [5]. Furthermore, oxidative stress is implicated not only in atherosclerotic progression but also in the emergence of cardiovascular conditions, including hypertension, myocardial infarction, and heart failure [6].
Accordingly, approaches targeting the reduction of oxidative stress have become increasingly important in both the prevention and clinical management of CVDs. Antioxidant compounds encompass a broad range of nutrients and bioactive substances, including vitamins (A, C, and E), trace elements such as selenium and zinc, polyphenolic compounds like flavonoids and resveratrol, as well as coenzyme Q10 and omega-3 fatty acids. These agents help mitigate oxidative damage primarily through free radical scavenging mechanisms. In addition, recent research has increasingly focused on their potential roles in preserving endothelial integrity, modulating inflammation, and reducing overall cardiovascular risk [7].
The antioxidant compounds addressed in this review were selected from among those that have been frequently investigated in the literature in the context of oxidative stress and inflammatory mechanisms associated with CVD and whose biological effects have been well characterized. Although numerous compounds exhibiting antioxidant activity are present in the diet, this review focuses on antioxidants that are supported by stronger clinical and epidemiological evidence and whose relationship with cardiovascular health has been more clearly established. However, beyond the traditional view of oxidative stress and antioxidants, it has become evident that this process involves more complex mechanisms at the cellular level. In recent years, the understanding of oxidative stress has moved beyond the simple balance model between oxidants and antioxidants toward a more integrative perspective that emphasizes the critical role of redox signaling in cellular communication [8, 9]. ROS are recognized not only as byproducts that cause cellular damage but also as key molecules involved in intracellular signaling, regulating fundamental physiological processes such as proliferation, differentiation, and apoptosis [10]. Mitochondria, which are an important source of ROS, are considered to play a central role not only in energy production but also in redox-based cellular signaling [8, 9].
This paper explores the contribution of oxidative stress to the development of CVDs and examines how antioxidant compounds influence endothelial integrity, inflammatory pathways, and atherosclerotic progression based on current evidence. Furthermore, it highlights the potential of nutrition-oriented antioxidant approaches in supporting both the prevention and clinical management of CVDs from a comprehensive perspective.
This study is based on a narrative review design and relies on a comprehensive evaluation of the existing scientific evidence regarding the role of antioxidants in CVD. Relevant studies were identified through searches conducted in the PubMed and Google Scholar databases. Only studies published up to March 2026 and written in English were included.
In the search strategy, the keywords “antioxidants in cardiovascular disease”, “oxidative stress and cardiovascular disease”, “dietary antioxidants”, “polyphenols”, “vitamins and cardiovascular disease”, and “antioxidants in CVD” were searched either individually or in combination using Boolean operators (AND, OR). In addition, the reference lists of the selected studies were manually examined to identify additional sources.
As this review is narrative in nature, a systematic selection protocol was not applied, and it is not intended to represent the entirety of the available literature. The selected studies were critically evaluated and synthesized in light of current scientific evidence.
Studies were initially screened based on their titles and abstracts, followed by a detailed full-text evaluation of those considered eligible.
Inclusion criteria:
(i) studies examining the relationship between CVD and antioxidants,
(ii) studies addressing the association between oxidative stress and cardiovascular pathophysiology,
(iii) human-based studies (clinical studies, randomized controlled trials, meta-analyses, and recent reviews),
(iv) studies published in peer-reviewed journals with sufficient scientific rigor.
Exclusion criteria:
(i) studies not directly related to CVD,
(ii) studies with methodological limitations,
(iii) studies with limited scientific contribution or not supported by current evidence,
(iv) studies conducted solely at the animal or in vitro level without clinical relevance.
Although a systematic selection protocol was not applied, care was taken to include studies reporting both positive and negative findings in order to minimize potential bias.
The findings are presented under the following thematic headings:
The role of oxidative stress in CVDs.
Oxidative stress-related endothelial dysfunction.
Classification and general characteristics of antioxidants.
Effects of antioxidants on cardiovascular health and clinical evidence.
Oxidative stress refers to a pathological state resulting from an imbalance between the production of ROS and the organism’s antioxidant defense capacity [11]. This disequilibrium causes damage at both cellular and tissue levels and contributes significantly to the onset and progression of CVDs, particularly atherosclerosis [12]. A key mechanism underlying cardiovascular injury involves the overproduction and accumulation of free radicals, especially ROS. These reactive species originate from multiple sources, including mitochondrial respiratory activity and enzymatic systems such as NADPH oxidase (NOX), xanthine oxidase, and uncoupled endothelial nitric oxide synthase (eNOS). In addition, processes like immune cell activation and various environmental influences further enhance ROS generation [13, 14].
At physiological and tightly regulated levels, ROS act as key signaling molecules that participate in the regulation of cellular defense systems, primarily through activation of the Nuclear factor erythroid 2-related factor 2 (Nrf2) signaling pathway [15]. Under basal conditions, Nrf2 exists in association with Keap1; however, increased ROS levels trigger its dissociation, followed by translocation into the nucleus, where it interacts with antioxidant response element (ARE) regions [16]. This mechanism supports cellular homeostasis by upregulating the expression of genes responsible for antioxidant enzyme production, including superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) [17].
The biological effects of ROS depend not only on their levels but also on their intracellular localization. This phenomenon is explained by the concept of “compartmentalized redox signaling” [18, 19]. In particular, mitochondria-derived ROS have been reported to act as regulatory molecules involved in intracellular signaling and to play a role in the regulation of vascular functions [20].
When ROS levels rise beyond physiological thresholds and antioxidant defenses fail to adequately compensate, these molecules begin to exert detrimental effects. Under these circumstances, the oxidative load increases, resulting in both structural and functional impairment of critical cellular components, including lipids, proteins, and nucleic acids [21]. Concurrently, redox-sensitive signaling pathways such as nuclear factor kappa B (NF-κB) and mitogen-activated protein kinase (MAPK) become activated, accompanied by an upregulation of adhesion molecule expression. Consequently, the production of proinflammatory cytokines, adhesion molecules, and chemokines is intensified, facilitating the recruitment of monocytes and T lymphocytes into the vascular wall and thereby promoting the progression of inflammation [13, 22].
Moreover, the upregulation of intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) in endothelial cells promotes monocyte attachment to the endothelial surface and facilitates their migration into the vascular wall, thereby sustaining the inflammatory milieu and contributing to atherosclerotic lesion formation [23].
Beyond these mechanisms, oxidative stress plays a prominent role in atherogenesis through lipid peroxidation processes. Elevated ROS levels induce the oxidative modification of low-density lipoproteins, resulting in the generation of oxidized low-density lipoproteins (ox-LDL). The subsequent uptake of these modified lipoproteins by macrophages leads to foam cell formation, while the amplified inflammatory response further drives plaque progression and destabilization [24].
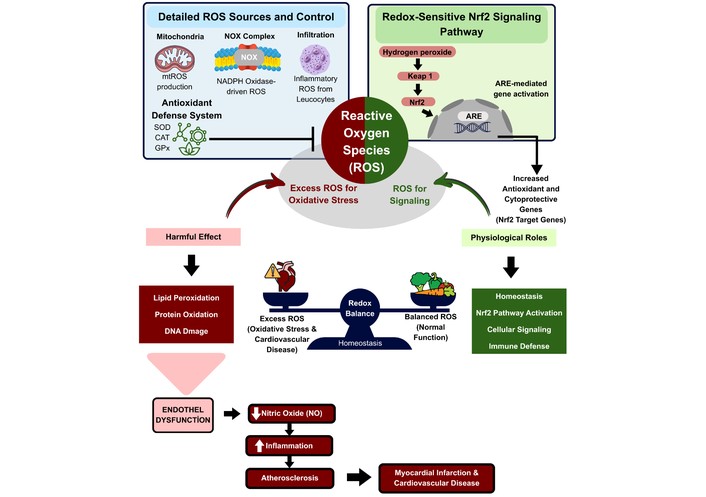
Throughout these processes, antioxidants reduce oxidative stress and the associated cellular damage by neutralizing free radicals [23]. The protective role of antioxidants and the dual mechanism of ROS are illustrated in Figure 1.
ROS originate from multiple sources, such as mitochondrial respiratory activity, NOX function, and the presence of inflammatory cells. Under physiological conditions, tightly regulated ROS levels act as signaling mediators and support vascular homeostasis via redox-dependent pathways, including Nrf2 signaling. During this process, Nrf2 separates from Keap1, subsequently translocates into the nucleus, and interacts with AREs, leading to enhanced expression of antioxidant and cytoprotective genes. Conversely, excessive ROS generation promotes oxidative stress, which induces lipid peroxidation, protein modification, and DNA damage. These alterations are closely linked to endothelial dysfunction, decreased nitric oxide (NO) availability, and heightened inflammatory activity, thereby contributing to the onset and progression of cardiovascular disorders, including atherosclerosis and myocardial infarction.
Oxidative stress impairs the functional integrity of vascular endothelial cells and contributes to the development of endothelial dysfunction. The endothelium is a highly metabolically active cellular layer lining the inner surface of blood vessels, acts as a selective interface between circulating blood and the vascular wall, and is essential for the regulation of vascular homeostasis [25]. By modulating vascular tone, regulating platelet activity, influencing inflammatory responses, and inhibiting vascular smooth muscle cell proliferation, the endothelium serves as a key regulator in maintaining the physiological balance of the cardiovascular system [26].
Under physiological conditions, vascular tone is regulated by vasodilatory mediators such as NO, prostacyclin, and endothelium-derived hyperpolarizing factors, while vasoconstrictive responses are mediated by factors including endothelin-1 (ET-1), angiotensin II, and thromboxane A2 [25]. However, increased ROS production leads to the reaction of NO with superoxide, resulting in the formation of peroxynitrite and thereby reducing NO bioavailability [27].
This decrease in NO levels triggers processes such as enhanced vasoconstriction, increased expression of endothelial adhesion molecules, elevated inflammatory cell infiltration, and stimulation of vascular smooth muscle cell proliferation, thereby contributing to the early stages of atherosclerosis. Therefore, endothelial dysfunction is considered an early and potentially reversible stage of atherosclerosis and is regarded as a critical step in the pathogenesis of CVD [28].
Antioxidants are defined as compounds that slow down or inhibit oxidative reactions in order to limit the damage caused by oxidative stress in cells [29].
According to their mechanisms of action, antioxidants are classified as primary (chain-breaking) and secondary (preventive) antioxidants. Primary antioxidants directly neutralize free radicals and terminate oxidative chain reactions, whereas secondary antioxidants exert their effects through indirect mechanisms such as chelating metal ions, reducing ROS formation, and converting hydroperoxides into less reactive compounds [30].
According to their sources, antioxidants are examined in two main groups: endogenous and exogenous antioxidants [31]. Endogenous antioxidants refer to the defense system synthesized by the organism, consisting of enzymatic and non-enzymatic components, whereas exogenous antioxidants include compounds obtained through diet or supplementation [32, 33]. Both groups of antioxidants function in a complementary and synergistic manner in maintaining cellular homeostasis and protecting against oxidative stress [31]. The classification of endogenous antioxidants is presented in Table 1, while the classification of exogenous antioxidants is presented in Table 2.
However, the biological effects of antioxidants depend not only on their chemical structures but are also shaped by pharmacokinetic processes such as bioavailability and metabolism [34]. The bioavailability of antioxidant compounds is particularly influenced by intestinal absorption and metabolic processes [35]. In addition, metabolic transformations carried out by the gut microbiota play an important role in determining the biological effects of dietary antioxidants, especially polyphenols [36].
Furthermore, many antioxidant compounds are metabolized by the gut microbiota into biologically active metabolites, and these metabolites have been reported to exert various biological effects in circulation [37]. Accordingly, it is suggested that classification of antioxidants based solely on chemical properties or source-based approaches is not sufficient; for a more comprehensive evaluation, mechanistic, pharmacokinetic, and systems biology-based approaches should also be taken into consideration.
Endogenous antioxidants [38].
| Enzymatic antioxidants | Non-enzymatic antioxidants | |
|---|---|---|
| Superoxide dismutaseCatalaseGlutathione reductaseGlutathione peroxidaseGlucose-6-phosphate dehydrogenase | GlutathioneUric acidBilirubinAlbuminMelatonin | Lipoic acidCeruloplasminCoenzyme Q10 |
| Antioxidants used as pharmacological agents | Vitamin- and mineral-derived antioxidants | Polyphenols | Other natural bioactive compounds |
|---|---|---|---|
| Xanthine oxidase inhibitorsTrolox-C (vitamin E analog)NADPH oxidase inhibitors (e.g., nonsteroidal anti-inflammatory agents) | Ascorbic acid (vitamin C)Tocopherols (vitamin E)Folic acidβ-Carotene (provitamin A)SeleniumZinc | FlavonoidsPhenolic acids ResveratrolLignansTannins | Omega-3 fatty acids |
The enzymatic antioxidant defense system is primarily composed of three major enzymes: SOD, CAT, and GPx. SOD catalyzes the conversion of superoxide radicals into hydrogen peroxide, thereby reducing the potentially harmful effects of ROS and playing a crucial role in the initial phase of cellular antioxidant defense. Following this step, CAT facilitates the breakdown of hydrogen peroxide into water and oxygen, limiting its intracellular accumulation. In addition, GPx is responsible for reducing hydrogen peroxide as well as other peroxide derivatives, thereby helping to minimize oxidative damage at the cellular level [40].
Enzymes such as glutathione reductase and glucose-6-phosphate dehydrogenase are among the supportive components of the antioxidant defense system. Rather than directly neutralizing free radicals, these enzymes enhance the effectiveness of other antioxidant mechanisms by maintaining the continuity of the glutathione cycle and preserving cellular redox balance. Through these processes, they contribute to reducing ROS-related oxidative damage in cells [7, 40].
Vitamin A is a fat-soluble micronutrient that participates in a wide range of physiological and metabolic functions. Its biologically active forms include retinol, retinal, and retinoic acid, whereas carotenoids—most notably β-carotene—serve as precursors that can be converted into vitamin A within the body [41]. Preformed vitamin A (retinoids) is predominantly obtained from animal-based sources, including liver, fish oil, egg yolk, and dairy products. In contrast, plant-derived carotenoids can be metabolically converted into retinol, with colorful fruits and vegetables such as carrots, sweet potatoes, spinach, kale, red peppers, and mango representing major dietary sources of provitamin A carotenoids [42].
It has critical importance in maintaining endothelial function, preserving vascular elasticity, and regulating blood pressure. In this context, experimental and mechanistic studies suggest that carotenoids, through their antioxidant properties, may contribute to the preservation of endothelial function and thereby support the maintenance of vascular integrity [43]. Epidemiological evidence indicates that the relationship between vitamin A and cardiometabolic health is complex and heterogeneous. Analyses based on large population datasets have reported that higher dietary vitamin A intake is inversely associated with the prevalence of cardiometabolic diseases, with retinol intake making this relationship more pronounced [44]. Similarly, in a study conducted using NHANES data [45], higher vitamin A intake was found to be inversely associated with the prevalence of coronary artery disease, and this association was shown to be particularly more pronounced in women.
However, observational evidence suggests a non-linear association between serum vitamin A concentrations and cardiovascular mortality, with both deficient and elevated levels corresponding to less favorable outcomes [46]. In addition, high vitamin A intake has not shown a consistent protective effect on cardiovascular risk factors such as hypertension and, in some cases, has been associated with adverse outcomes [47]. In a prospective cohort study, an L-shaped relationship was identified between dietary vitamin A intake and the risk of hypertension; while an increased risk was observed at low intake levels, the additional protective effect appeared limited beyond a certain threshold [48]. These differences are thought to arise from variability in dose, bioavailability, study duration, and population characteristics.
When all findings are considered together, it becomes evident that the relationship between vitamin A and CVD is not linear or consistent, and observational studies should be interpreted with caution in terms of causality.
Vitamin C is a water-soluble micronutrient characterized by a strong antioxidant capacity and is abundantly present in a variety of foods, including citrus fruits, kiwi, strawberries, red peppers, broccoli, and leafy green vegetables. It helps limit oxidative damage induced by ROS and other free radicals, while also contributing to the preservation of other antioxidants, such as glutathione and α-tocopherol (vitamin E), in their reduced and biologically active states [49].
In contrast to certain other mammals, humans are unable to produce vitamin C (ascorbic acid) endogenously. This limitation arises from the absence of a functional L-gulono-γ-lactone oxidase (GULO), an enzyme responsible for the final step in ascorbic acid biosynthesis [50]. Therefore, vitamin C must be obtained through the diet, and maintaining adequate intake is essential for the proper functioning of physiological processes [51].
In light of these biological characteristics, the influence of vitamin C on cardiovascular health has been examined in both epidemiological and clinical settings. Observational evidence indicates that greater vitamin C intake tends to correspond to a lower likelihood of CVD. For instance, the SUN (Seguimiento Universidad de Navarra) cohort study conducted among university graduates in Spain reported an inverse pattern between vitamin C intake and cardiovascular mortality [52].
In a systematic review evaluating the effects of vitamin C intake from diet and supplementation on plasma levels, it was reported that vitamin C obtained from both sources increased plasma concentrations; however, this increase was more pronounced with supplementation. Additionally, the increase was found to be greater in individuals with CVD, while it remained more limited in healthy individuals [53].
However, it appears that improvements observed in biochemical markers do not always translate to clinical outcomes to the same extent. In an umbrella review assessing the effects of dietary vitamin C on cardiometabolic risk factors, higher intake was reported to be associated with favorable changes in blood pressure, lipid profile, and certain cardiometabolic indicators; nevertheless, it was noted that the consistency of findings and the level of evidence varied across studies [54].
These differences become more apparent when the study design is taken into account. While observational studies often indicate a protective association [55], findings from randomized controlled trials do not consistently support this effect [56]. In particular, vitamin C supplementation appears to have limited or no significant effect on cardiovascular events [57]. This may be related to the fact that the synergistic effects observed when vitamin C is consumed through the diet together with other bioactive compounds are not replicated when it is administered alone in supplement form.
Overall, although the effects of vitamin C on cardiovascular health are supported by strong mechanistic evidence, the clinical findings remain inconsistent, and there is a need for better-designed intervention studies in this area.
Vitamin E refers to a group of fat-soluble compounds comprising eight structurally related forms, namely four tocopherols (α, β, γ, and δ) and four tocotrienols (α, β, γ, and δ) [58]. These compounds are widely found in foods such as vegetable oils (particularly sunflower and wheat germ oil), as well as nuts like hazelnuts and almonds, and green leafy vegetables [59]. As a fat-soluble vitamin, the bioavailability of dietary vitamin E is influenced by the fat content of the diet, and it has been reported that absorption may be reduced in diets with insufficient fat [60].
Vitamin E compounds exhibit strong antioxidant properties that support the stability of cell membranes and lipoproteins against oxidative modifications caused by free radicals. Among these isomers, α-tocopherol is considered the form with the highest biological activity and the most prevalent in human tissues [58]. Acting in the lipid phase, α-tocopherol interrupts the lipid peroxidation process, thereby contributing to the preservation of the structural integrity of cell membranes and lipoproteins [61]. Additionally, vitamin C has been reported to regenerate oxidized vitamin E, thereby contributing to the maintenance of its antioxidant function [59]. In this context, α-tocopherol is reported to limit LDL oxidation, potentially slowing the progression of atherosclerotic processes, and to exert anti-inflammatory effects through the modulation of cellular signaling pathways [62].
In light of these mechanistic characteristics, vitamin E has been proposed to play a role in the prevention of CVD, and this relationship has been widely explored in epidemiological research. Current evidence suggests that greater dietary intake of vitamin E tends to align with lower levels of cardiovascular risk. In this regard, a large prospective cohort analysis based on NHANES (2003–2018) data reported that higher vitamin E intake corresponded to reduced incidence of CVD, as well as lower risks of both cardiovascular and all-cause mortality [63].
In contrast, evidence derived from randomized controlled trials evaluating vitamin E supplementation does not consistently corroborate this relationship. For instance, the HOPE (Heart Outcomes Prevention Evaluation) trial reported no significant protective effect of vitamin E use on major cardiovascular events [64]. Similarly, findings from the Vitamin E Atherosclerosis Prevention Study (VEAPS) indicate that daily administration of 400 IU DL-α-tocopherol in individuals without clinical evidence of CVD resulted in a significant reduction in oxidized LDL levels. However, after a follow-up period of approximately three years, no significant difference was observed in carotid intima-media thickness progression compared with the placebo group [65]. These findings suggest that improvements observed at the biochemical level do not always translate into clinical outcomes. In this context, recent guideline-based evaluations indicate that vitamin E supplementation does not provide a clear benefit in the prevention of CVD and is therefore not recommended for routine use [66]. These inconsistencies in clinical findings may be associated with various factors, including interindividual genetic differences, dietary patterns, synergistic interactions among antioxidants, and baseline antioxidant levels.
Overall, although the biochemical effects of vitamin E on the cardiovascular system are evident, current clinical evidence does not support that these effects translate into a strong and consistent benefit in preventing cardiovascular events. The mechanisms of vitamin E in the atherosclerotic process, its biological effects, and the related clinical findings are presented in Figure 2.
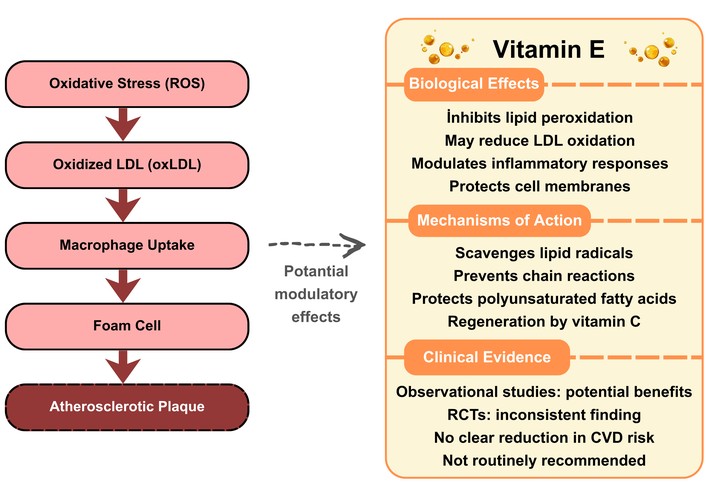
Potential role of vitamin E in atherosclerosis: mechanisms, biological effects, and clinical evidence.
The atherosclerotic process progresses through a series of sequential events, including LDL oxidation triggered by increased oxidative stress, macrophage uptake, foam cell formation, and plaque development. Vitamin E may influence this process through various biological effects, such as limiting lipid peroxidation, supporting the stability of cell membranes, and regulating inflammatory responses. From a mechanistic perspective, it interrupts chain reactions by scavenging lipid radicals and protects polyunsaturated fatty acids against oxidative damage. However, while observational studies suggest a possible association between vitamin E intake and cardiovascular risk, findings from randomized controlled trials are inconsistent and do not support a clear benefit in preventing cardiovascular events. Therefore, the role of vitamin E in the prevention of CVDs remains unclear, and the evidence regarding its routine use is limited.
Selenium is an essential trace element required for human health. After dietary intake, it is primarily metabolized in the liver and incorporated into the structure of selenoproteins found in various tissues. These proteins are involved in maintaining redox balance, supporting antioxidant defense mechanisms, and regulating inflammatory responses [67]. Selenium is present in foods such as cereals, as well as animal-derived products, including meat, fish, milk, and dairy products, and is also found in nuts. However, the selenium content of plant-based foods can vary considerably depending on the selenium levels of the soil in which they are grown [68].
Selenium contributes to the maintenance of cellular redox balance and the antioxidant defense system through its incorporation into the structure of selenoproteins. In particular, selenium-dependent enzymes such as GPx and thioredoxin reductase support the reduction of oxidative stress by enabling the detoxification of ROS [69]. Through these mechanisms, selenium is suggested to exert regulatory effects on the pathophysiological processes involved in the development of CVD [70].
Within this biological framework, the relationship between selenium and CVD has been extensively investigated in epidemiological studies and meta-analyses. Current evidence suggests that low selenium levels may be associated with an increased risk of CVD, whereas adequate levels may exert potential protective effects [71, 72]. However, this relationship does not appear to be linear and may vary across different populations [73, 74].
Current evidence indicates that the effects of selenium on cardiovascular health are dose-dependent and generally exhibit a U-shaped relationship. It has been reported that increases in selenium levels up to a certain threshold are associated with a reduction in cardiovascular risk; however, at higher levels, this effect may diminish or even reverse [75]. These findings suggest that both insufficient and excessive selenium levels may be associated with adverse health outcomes.
In contrast, data from randomized controlled trials and their meta-analyses indicate that the effect of selenium supplementation on cardiovascular outcomes is limited (RR = 0.91; 95% CI: 0.74–1.10) [76]. Similarly, although observational studies have reported an inverse association between higher selenium levels and lower disease risk, this effect has not been consistently confirmed in intervention studies [77].
When all findings are considered together, it becomes evident that the effects of selenium on cardiovascular health may vary depending on individual selenium status, dosage, population characteristics, and study design. Despite a strong mechanistic biological basis, current clinical evidence does not support a clear and consistent benefit of selenium supplementation in the prevention of CVD.
Zinc is a trace element present in various food groups, including meat, seafood, legumes, nuts, whole grains, and dairy products, and it is essential for the maintenance of physiological functions. As the human body does not have the capacity to produce zinc, maintaining adequate levels depends on regular dietary intake [78].
Zinc plays an active role in numerous physiological processes, including immune function, cell proliferation, wound healing, and protein and DNA synthesis, and contributes to metabolic processes by serving as a structural or catalytic component of many enzymes [79]. In addition, it limits ROS accumulation by supporting the activity of antioxidant systems such as SOD and metallothionein [80].
Furthermore, zinc has been reported to suppress NF-κB signaling through A20 and peroxisome proliferator-activated receptor-α/γ (PPAR-α/γ), and to inhibit NF-κB activation by reducing inhibitor κB kinase (IKK) activity [81]. Through these effects, zinc may influence processes involved in the pathogenesis of CVD by alleviating oxidative stress and modulating inflammatory responses. The regulatory effects of zinc on the ROS-mediated NF-κB signaling pathway are summarized in Figure 3.
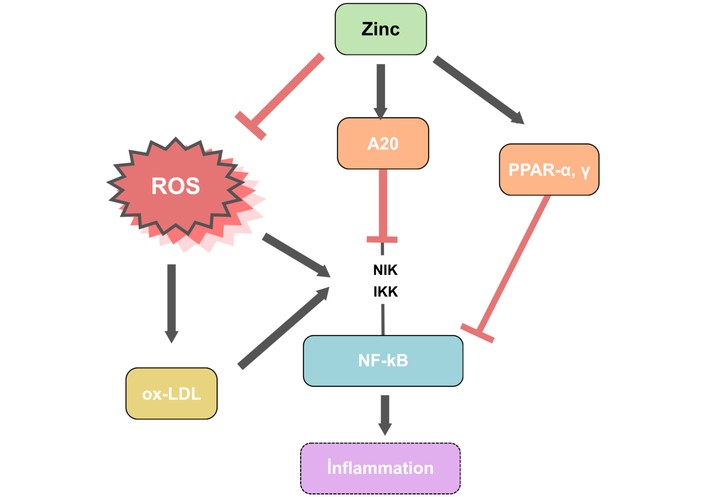
Schematic representation summarizing the effects of zinc on ROS formation and NF-κB signaling. Created by the author based on [81]. NF-κB: nuclear factor kappa B; PPAR: peroxisome proliferator-activated receptor; ROS: reactive oxygen species.
ROS promote the formation of ox-LDL by elevating oxidative burden, thereby facilitating the progression of atherosclerosis. They also amplify inflammatory responses through activation of NF-κB signaling via the NIK/IKK pathway. In contrast, zinc counteracts this process by inducing A20, a negative regulator of NF-κB signaling, which suppresses NIK/IKK activation. Additionally, zinc modulates inflammation by restricting NF-κB activity through PPAR-α/γ-mediated pathways.
In line with these biological effects, the potential contribution of zinc to the prevention of CVD has increasingly become a subject of research in recent years. Epidemiological evidence generally suggests that low zinc levels may be associated with more adverse cardiovascular outcomes. For instance, a study conducted in patients with myocardial infarction reported that low serum zinc levels were associated with an increased likelihood of rehospitalization due to heart failure [82]. Similarly, in individuals with diabetes, adequate dietary zinc intake was shown to be associated with a reduced 10-year risk of atherosclerotic CVD (OR = 0.77, 95% CI: 0.61–0.99) [83]. In addition, inadequate zinc intake in middle-aged and older individuals has been reported to be associated with a higher likelihood of cardiovascular mortality [84].
However, the relationship between zinc and health outcomes does not appear to be linear; both insufficient and excessive intake may lead to adverse effects. Indeed, some studies have reported that higher zinc levels are associated with increases in cardiometabolic markers such as HbA1c, triglycerides, and insulin resistance [85]. These findings highlight the importance of maintaining zinc levels within an optimal range.
Experimental evidence also supports this observation, indicating that high zinc levels may contribute to increased ROS production, exacerbation of oxidative stress, mitochondrial dysfunction, and subsequent cellular damage [86, 87]. Within this framework, it becomes evident that effects observed at the biochemical level do not always directly translate into clinical outcomes, and that the impact of zinc on the cardiovascular system may vary depending on factors such as dosage, individual characteristics, and study design.
In conclusion, although zinc may exert potential protective effects on the cardiovascular system through antioxidant and anti-inflammatory mechanisms, current evidence suggests that this effect is not linear and that maintaining appropriate levels is a key determinant.
Flavonoids represent a class of plant-derived polyphenols present across a wide range of foods, particularly fruits and vegetables, as well as beverages such as tea and red wine. Their antioxidant, antithrombotic, anti-inflammatory, and vasodilatory properties have been linked to potential benefits in the prevention and management of CVDs [88]. These effects largely stem from the strong antioxidant capacity of flavonoids. By limiting the accumulation of free radicals and ROS, these compounds help attenuate oxidative burden. Additionally, they support endogenous antioxidant defense systems, thereby promoting the activity of enzymes such as SOD, CAT, and GPx [89].
Furthermore, flavonoids downregulate NF-κB signaling, leading to decreased production of proinflammatory cytokines, including tumor necrosis factor alpha (TNF-α), interleukin-1 beta (IL-1β), and interleukin-6 (IL-6), while also limiting the expression of adhesion molecules such as ICAM-1 and VCAM-1, thereby reducing the attachment of inflammatory cells to the vascular wall [90].
Flavonoids contribute to the regulation of vascular tone and support endothelial function by increasing endothelium-derived NO levels. NO facilitates vasodilation by inducing relaxation in vascular smooth muscle cells, thereby contributing to the reduction of blood pressure and the improvement of tissue perfusion [88].
Flavonoids are classified into different subclasses based on their chemical structures, and these subgroups exhibit distinct biological effects on the cardiovascular system [89]. For example, quercetin and kaempferol, which belong to the flavonol group, have been reported to support endothelial function by reducing oxidative burden and thereby contributing to blood pressure control. In particular, quercetin is suggested to exert regulatory effects on the renin-angiotensin-aldosterone system by inhibiting angiotensin-converting enzyme activity, and thus may play a role in blood pressure regulation [91].
In contrast, compounds such as catechin and epicatechin, which belong to the flavan-3-ol group, have been reported to influence hemodynamic balance by supporting vascular relaxation, with this effect being reflected in reductions in blood pressure [92]. In addition, regular consumption of cocoa products rich in epicatechin has been associated with decreases in both systolic and diastolic blood pressure values [93].
Anthocyanins, which are pigment compounds belonging to the flavonoid class and are predominantly found in purple and blue-colored fruits, exhibit pronounced antioxidant and anti-inflammatory properties [88]. These compounds have been reported to limit inflammatory processes in the vascular wall by reducing the adhesion of monocytes to endothelial cells stimulated by TNF-α [94].
These mechanistic observations are consistent with findings from population-based studies. Evidence from systematic reviews and meta-analyses suggests that higher flavonoid intake may be associated with a lower likelihood of hypertension [95, 96]. Similarly, analyses including prospective cohort studies have reported that dietary patterns rich in flavonoids are associated with lower incidence of CVD and related mortality [97, 98]. In addition, evidence from large-scale cohort studies suggests that various flavonoid subclasses tend to correspond to lower levels of CVD risk [99].
However, it is noteworthy that findings regarding the effects of flavonoids on cardiovascular health vary depending on study design. While epidemiological studies generally report protective associations, data from randomized controlled trials do not consistently support this effect, and evidence regarding their direct impact on clinical outcomes remains limited [100]. These discrepancies may be attributed to interindividual variability in the bioavailability, metabolic transformations, and interactions of flavonoids with the gut microbiota [101].
In addition, it has been reported that not only total flavonoid intake but also the diversity of flavonoids in the diet may be a determining factor in health outcomes; dietary patterns characterized by greater flavonoid diversity have been associated with lower risks of chronic diseases [102]. Within this framework, it is suggested that the effects of flavonoids may be more pronounced when consumed through a variety of food sources rather than as isolated compounds.
In conclusion, although flavonoids may provide potential benefits for cardiovascular health through antioxidant and anti-inflammatory mechanisms, these effects are not consistently reflected in clinical outcomes, and their intake through whole foods may be more effective.
Resveratrol is a polyphenolic compound derived from various plant sources, including grape skin, red wine, blueberries, and peanuts [103]. It has been reported in the literature that, beyond its antioxidant and anti-inflammatory properties, this compound may exert protective effects on the cardiovascular system [104]. In this context, it may limit the oxidative modification of low-density lipoproteins by reducing oxidative burden, thereby slowing the progression of the atherosclerotic process [105]. In addition, it has been suggested that it may exert antithrombotic effects by inhibiting platelet activation and aggregation [106, 107].
In line with this mechanistic basis, the effects of resveratrol on cardiovascular health have been evaluated through clinical studies and meta-analyses. Accordingly, resveratrol supplementation has been reported to be associated with significant reductions in C-reactive protein and TNF-α levels in individuals with CVD, whereas no significant change was observed in IL-6 levels [108]. In addition, another meta-analysis reported that resveratrol supplementation was associated with improvements in endothelial function, reflected by increased flow-mediated dilation values, along with reductions in ICAM-1 levels [109].
However, current evidence indicates that these biological effects are not consistently reflected in clinical outcomes. Umbrella reviews have reported that the effects of resveratrol supplementation on body weight and obesity-related indicators remain limited [110], while comprehensive systematic reviews emphasize that the existing evidence is insufficient to support its routine use [111]. On the other hand, findings from some subgroup analyses reporting increases in triglyceride levels suggest that the cardiometabolic effects of resveratrol do not follow a uniform pattern across all parameters [112].
These inconsistent findings may be attributed to factors such as variability in study designs, differences in applied doses and intervention durations, limited sample sizes, and constraints related to bioavailability. Within this framework, the discrepancies observed among observational studies, randomized controlled trials, and meta-analyses suggest that, despite its promising mechanistic effects, the clinical role of resveratrol has not yet been clearly established.
Lycopene is a carotenoid with strong antioxidant capacity, found in high amounts in various foods, particularly tomatoes and tomato-based products [113]. Recent research has increasingly focused on examining the potential contributions of lycopene to the prevention of CVD and the improvement of cardiovascular risk markers [114].
The effects of lycopene on the cardiovascular system are primarily mediated through antioxidant and anti-inflammatory mechanisms. In this context, it contributes to reducing oxidative burden by limiting ROS formation and may slow the progression of the atherosclerotic process by enhancing the resistance of the vascular wall to oxidative damage [113]. In addition, through its anti-inflammatory effects, it reduces the levels of proinflammatory mediators such as TNF-α, IL-6, and IL-1β, and modulates the inflammatory response by suppressing NF-κB signaling [115]. Furthermore, it enhances cellular defense capacity by stimulating the Nrf2-mediated antioxidant response, thereby contributing to the activity of antioxidant enzymes such as SOD, CAT, and GPx [113].
The mechanisms underlying the effects of lycopene on the cardiovascular system are summarized in Figure 4.
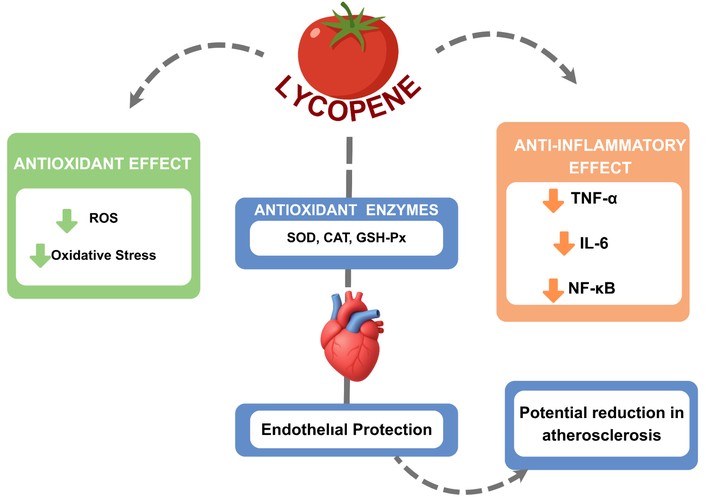
Schematic representation of the antioxidant and anti-inflammatory effects of lycopene on the cardiovascular system.
Lycopene has been shown to reduce cellular oxidative burden by limiting the generation of ROS, while also supporting antioxidant defense systems, including SOD, CAT, and GPx. It may also influence inflammatory responses through regulatory effects on key mediators such as TNF-α, IL-6, and IL-1β, and NF-κB. Within this context, lycopene is thought to help preserve endothelial integrity and may contribute to slowing the progression of atherosclerosis.
Within this mechanistic framework, the effects of lycopene on cardiovascular risk factors have been examined through clinical studies and meta-analyses. In a systematic review and meta-analysis evaluating the effects of lycopene and tomato consumption on these risk indicators, lycopene intake was found to be associated with favorable changes in blood pressure, lipid profile, and inflammatory markers; however, it was emphasized that these effects were not observed at a similar magnitude across all study types [116]. Similarly, a recent umbrella review indicates that the available evidence demonstrates considerable heterogeneity and that the overall level of evidence remains limited [117]. Data from intervention studies also support this observation, showing that consistent changes in plasma lipid levels and antioxidant capacity are not always observed [118]. Indeed, in a randomized controlled trial involving moderately overweight but otherwise healthy individuals, no significant differences in cardiovascular risk markers were identified despite relatively high lycopene intake [119].
These findings suggest that the cardiovascular effects of lycopene are inconsistent and may not be attributable to a single component alone. In this context, overall evaluations indicate that lycopene intake can be associated with improvements in cardiovascular risk markers [120]; however, it remains unclear whether these effects are directly attributable to lycopene itself or to overall dietary patterns rich in lycopene-containing foods. Indeed, a review comparing tomato consumption with lycopene supplementation reported that tomato-based foods produced more consistent and pronounced effects on cardiovascular risk markers, whereas lycopene supplements were associated with more limited outcomes [121]. This suggests that approaches focusing solely on isolated nutrient components may not be sufficient.
These differences may be associated with factors related to bioavailability and the food matrix. For example, the conversion of lycopene into cis isomers with higher bioavailability during thermal processing contributes to increased absorption [122]. In addition, the consumption of lycopene together with fats such as olive oil enhances its absorption due to its lipophilic nature; this effect has been demonstrated by increases in plasma lycopene levels [123]. Furthermore, randomized controlled trials showing more pronounced effects of tomato products enriched with olive oil on cardiovascular risk markers support these findings [124].
Within this framework, the cardiovascular effects of lycopene appear to vary depending on factors such as bioavailability and the food matrix, suggesting that its intake through whole foods may represent a more effective approach.
Recent literature has increasingly focused on the effects of dietary antioxidants on cardiovascular health. Experimental and clinical findings have reported that antioxidant intake may exert reducing effects on markers associated with vascular calcification and inflammation [125, 126]. In addition, dietary patterns with anti-inflammatory properties have been shown to be associated with reductions in systolic and diastolic blood pressure, LDL and total cholesterol levels, as well as decreases in inflammatory markers [127].
Epidemiological evidence generally supports the relationship between dietary antioxidants and cardiovascular risk. Higher Composite Dietary Antioxidant Index (CDAI) values have been reported to be associated with a lower prevalence of CVD; however, this association did not retain statistical significance in multivariable analyses. In subgroup analyses by sex, a protective trend was observed in men, whereas no similar association was identified in women [128]. These findings suggest that the cardiovascular effects of antioxidants may vary depending on population characteristics.
The effects of antioxidants on cardiovascular health are also addressed in the context of lipid metabolism. It has been reported that the combined use of natural antioxidants may be associated with improvements in lipid profiles [129], and these findings are supported by meta-analyses demonstrating that lipid supplementation is associated with favorable changes, particularly in blood lipid levels and blood pressure. However, it is emphasized that the effects of different lipid fractions on cardiometabolic markers are not uniform and may vary [130].
When evaluated in terms of cardiovascular mortality, higher dietary intake and circulating levels of vitamin C have been reported to be associated with a lower risk of cardiovascular death. For vitamin E and β-carotene, only circulating levels were found to be inversely associated with mortality, whereas dietary intake did not demonstrate a similar protective effect, and these findings were supported by low levels of evidence [131]. These results suggest that the cardiovascular effects of antioxidants may vary depending on the type of compound and the level of intake.
However, there are also studies indicating that antioxidants do not exert protective effects under all conditions. Findings from Mendelian randomization analyses suggest that high intake levels of certain antioxidants, particularly α-tocopherol and retinol, may be associated with an increased risk of specific CVDs [132]. In addition, prospective cohort studies have shown that some dietary antioxidants are associated with CVD risk; in particular, vitamin E intake has been linked to a lower risk, whereas no significant association has been identified for compounds such as vitamins A and C and zinc [133]. These findings suggest that discrepancies may arise between observational studies and approaches aimed at assessing causality.
When the available evidence is considered as a whole, the effects of antioxidants on cardiovascular health appear to be multidimensional and cannot be explained by a single mechanism. The beneficial effects of fruits and vegetables on the cardiovascular system are thought to arise not from a single antioxidant compound but from the synergistic interactions of various bioactive components present in these foods. Accordingly, it is emphasized that obtaining antioxidants through whole foods rather than isolated supplements may represent a more effective approach [134].
Within this framework, current evidence suggests that dietary antioxidant compounds may exert beneficial effects on cardiovascular health; however, these effects are not always consistent and may vary depending on the type of compound, level of intake, and individual characteristics.
The overall effects of dietary antioxidants on cardiovascular pathways are presented in Figure 5. The major dietary antioxidants associated with cardiovascular health, including their food sources, mechanisms of action, and recommended intake levels, are summarized in Table 3.
Major dietary antioxidants affecting cardiovascular health, their mechanisms of action, and recommended daily intake levels.
| Antioxidant | Main dietary sources | Mechanism of action | Cardiovascular effects | Recommended daily intake level |
|---|---|---|---|---|
| Vitamin A | Liver, fish oil, egg yolk, and dairy products; carrots, sweet potatoes, spinach, kale, and red peppers [135] | Regulation of antioxidant defense systems and oxidative stress responses via retinoic acid [136] | Support of endothelial function, maintenance of vascular integrity, and reduction of cardiometabolic risk [43–45] | 700–900 µg RAE/day [135] |
| Vitamin C | Citrus fruits, kiwi, strawberries, red peppers, broccoli, and green leafy vegetables [137] | Neutralization of ROS and reduction of oxidative stress [49] | Support of endothelial function and reduction of cardiovascular disease risk [52–54] | 75–90 mg/day [137] |
| Vitamin E | Vegetable oils, hazelnuts, almonds, and green leafy vegetables [137] | Inhibition of lipid peroxidation and reduction of LDL oxidation [61, 62] | Slowing of atherosclerosis and reduction of platelet aggregation [62, 64, 65] | 15 mg/day [137] |
| Selenium | Cereals, meat, fish, seafood, dairy products, and nuts [137] | Selenoprotein synthesis, antioxidant enzyme activity, and ROS neutralization [67, 71] | Reduction of oxidative stress, regulation of inflammation, and decreased risk and mortality of cardiovascular diseases [67, 71, 72] | 55 µg/day [137] |
| Zinc | Meat, seafood, legumes, nuts, whole grains, and dairy products [135] | Antioxidant enzyme activity (SOD), reduction of ROS, and inhibition of NF-κB [81] | Reduction of oxidative stress and inflammation, and decreased risk of cardiovascular disease [81–84] | 8–11 mg/day [135] |
| Flavonoids | Fruits, vegetables, tea, cocoa, and red wine [88] | Neutralization of ROS; inhibition of NF-κB; increased NO production [88–90] | Improvement of endothelial function, vasodilation; reduction in cardiovascular disease risk [88, 89, 97–99] | - |
| Resveratrol | Grape skins, red wine, blueberries, and peanuts [103] | Neutralization of ROS, inhibition of LDL oxidation, and anti-inflammatory and antithrombotic effects [105, 107, 108] | Improvement of endothelial function [109] | - |
| Lycopene | Tomatoes, watermelon, and pink grapefruit [113] | Neutralization of ROS, inhibition of NF-κB, and activation of antioxidant enzymes [113, 115] | Slowing of atherosclerosis and improvement of cardiovascular disease risk factors [113, 116, 120] | - |
Note. The recommended daily intake levels are based on Dietary Reference Intakes (DRI) reports. There are no established recommended daily intake levels for flavonoids, resveratrol, and lycopene. NF-κB: nuclear factor kappa B; NO: nitric oxide; ROS: reactive oxygen species; SOD: superoxide dismutase.
Dietary antioxidant components (vitamins, minerals, polyphenols, and carotenoids) may contribute to the maintenance of cardiovascular health by exerting regulatory effects on key cardiovascular pathways such as endothelial function, inflammatory processes, lipid metabolism, and mitochondrial activity. Through these interactions, potential benefits may include improved endothelial function, attenuation of inflammatory responses, improvements in lipid profiles, and enhanced mitochondrial function.
Although the potential protective effects of antioxidants on CVD have been extensively addressed in the literature, their translation into clinical outcomes does not present a consistent pattern. Findings obtained at the experimental and mechanistic levels suggest that antioxidants may contribute to the reduction of oxidative burden. However, analyses evaluating randomized controlled trials indicate that antioxidant use does not always provide clinically significant benefits [66, 138]. This phenomenon is referred to in the literature as the “antioxidant paradox” and describes the discrepancy between strong findings at the experimental level and inconsistent clinical outcomes [139].
In addition, there are notable differences between obtaining antioxidants naturally through food and consuming them in supplement form. Epidemiological evidence indicates that dietary patterns rich in antioxidants are associated with favorable health outcomes. In contrast, findings derived from isolated antioxidant supplementation tend to be more variable and often limited [134]. Moreover, a large-scale cohort study demonstrated that the intake of vitamins and minerals from foods is inversely associated with mortality, whereas supplement use does not confer a similar benefit [140].
These findings are also supported by large-scale meta-analyses. Notably, a Cochrane Collaboration review including more than 290,000 individuals reported that antioxidant supplementation does not provide a significant benefit in terms of mortality and, in some cases, may be associated with an increased risk of mortality [141].
Within this framework, promoting dietary patterns rich in antioxidants is of particular importance in clinical practice. Diet models that include fruits, vegetables, and plant-based foods may contribute to reducing oxidative burden by increasing antioxidant intake and have been associated with lower all-cause mortality [142]. In this regard, current literature indicates that the beneficial effects on health cannot be attributed solely to individual nutrients; rather, they are determined by the synergistic interactions of nutrients and bioactive compounds within their natural food matrix [134].
CVDs are among the leading determinants of global mortality and disease burden. Disruption of redox balance constitutes a key biological basis in the onset and progression of these diseases. An increase in ROS levels, together with insufficient antioxidant defense mechanisms, promotes cardiovascular pathologies by triggering processes such as endothelial dysfunction, activation of inflammatory responses, and acceleration of atherosclerotic progression. In this context, strategies aimed at controlling oxidative burden have gained increasing importance in the prevention and management of CVD.
Current literature indicates that both endogenous defense mechanisms and exogenous antioxidant components play a role in regulating oxidative burden. While enzymatic systems such as SOD, CAT, and GPx perform essential functions in maintaining cellular redox balance, dietary antioxidants—including vitamins, minerals, and polyphenolic compounds—may influence the cardiovascular system through various biochemical processes, such as neutralizing free radicals, inhibiting inflammatory signaling pathways, and supporting endothelial function. However, it should also be considered that these mechanistic effects are not always consistently reflected in clinical outcomes.
Dietary patterns characterized by high consumption of fruits, vegetables, whole grains, nuts, and other plant-based foods rich in antioxidants are considered to potentially contribute to the prevention of CVD by reducing oxidative burden and attenuating inflammatory processes. However, findings from clinical studies investigating the effects of antioxidant supplementation on cardiovascular outcomes do not consistently present a uniform pattern. These discrepancies may be attributed to multiple factors, including bioavailability, administered dose, interindividual genetic and metabolic variability, overall dietary composition, and interactions among antioxidants. Within this framework, obtaining antioxidants through the regular consumption of antioxidant-rich foods, rather than isolated supplements, appears to be a more appropriate approach for maintaining cardiovascular health.
In order to more comprehensively elucidate the effects of antioxidants on cardiovascular health, future studies should focus on large-scale and long-term clinical investigations that take into account bioavailability, metabolic processes, and interindividual variability in response. In addition, the use of advanced molecular analysis techniques may contribute to a more detailed and mechanistic understanding of the effects of dietary bioactive compounds on the cardiovascular system. Within this framework, current evidence indicates that the clinical effectiveness of antioxidant-based approaches may vary due to interindividual differences and the complex nature of biological systems. Accordingly, in order to enhance the effectiveness of antioxidant strategies, it is important to develop precision nutrition approaches that take individual characteristics into account and to place greater emphasis on interventions targeting redox balance.
Overall, available data indicate that antioxidants may play a supportive role in the prevention and management of CVDs. However, findings from the literature do not uniformly endorse antioxidant supplementation as a reliable strategy for reducing cardiovascular risk. Instead of functioning as an independent intervention, antioxidants appear to exert greater benefits when derived from whole foods within balanced and varied dietary patterns. From a public health perspective, approaches that encourage regular intake of antioxidant-rich foods constitute a key element of integrated strategies targeting CVD prevention. Further well-designed randomized controlled trials remain essential to better define optimal intake levels and long-term outcomes.
ARE: antioxidant response element
CAT: catalase
CVDs: cardiovascular diseases
GPx: glutathione peroxidase
ICAM-1: intercellular adhesion molecule-1
IKK: inhibitor κB kinase
IL-1β: interleukin-1 beta
IL-6: interleukin-6
NF-κB: nuclear factor kappa B
NO: nitric oxide
NOX: NADPH oxidase
Nrf2: Nuclear factor erythroid 2-related factor 2
ox-LDL: oxidized low-density lipoproteins
PPAR-α/γ: peroxisome proliferator-activated receptor-α/γ
ROS: reactive oxygen species
SOD: superoxide dismutase
TNF-α: tumor necrosis factor alpha
VCAM-1: vascular cell adhesion molecule-1
MSE: Conceptualization, Investigation, Visualization, Writing—original draft, Writing—review & editing. FRÖ: Writing—original draft, Conceptualization. GD: Writing—review & editing, Supervision. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
This study received no external funding.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 1667
Download: 40
Times Cited: 0