Review
Review

Affiliation:
1Pediatric Allergy Unit, Pediatric Department, Vall d’Hebron University Hospital, Investigadora del Grup d’Investigació “Creixement i Desenvolupament”, Vall d’Hebron Institut de Recerca (VHIR), Vall d’Hebron Hospital Campus, Barcelona, 08035 Catalonia, Spain
Email: teresa.garriga@vallhebron.cat
ORCID: https://orcid.org/0000-0003-1892-9750
Affiliation:
2Allergy Department, Complexo Hospitalario Universitario de Santiago, Santiago, 15405 Galicia, Spain
ORCID: https://orcid.org/0000-0002-8281-2357
Affiliation:
3Allergy Department, Hospital Universitario Central, Oviedo, 33011 Asturias, Spain
ORCID: https://orcid.org/0000-0002-6969-7876
Affiliation:
4Pediatric Allergy Unit, Allergy Department, Gregorio Maranon University Hospital, 28009 Madrid, Spain
ORCID: https://orcid.org/0000-0002-6117-6582
Affiliation:
5Allergy Department, Río Hortega University Hospital, Valladolid, 47012 Castilla y León, Spain
ORCID: https://orcid.org/0000-0002-6931-0176
Affiliation:
5Allergy Department, Río Hortega University Hospital, Valladolid, 47012 Castilla y León, Spain
Affiliation:
6Allergy Department, Hospital Universitario La Paz, Institute for Health Research (IdiPaz), 28046 Madrid, Spain
ORCID: https://orcid.org/0000-0002-6816-3880
Explor Asthma Allergy. 2025;3:100981 DOI: https://doi.org/10.37349/eaa.2025.100981
Received: January 03, 2025 Accepted: April 08, 2025 Published: May 07, 2025
Academic Editor: Désirée Larenas-Linnemann, Hospital Médica Sur, Mexico
The article belongs to the special issue The Global Picture of Asthma after Guideline Changes and the COVID Pandemics
Pediatric and adolescent asthma is a significant health challenge with high prevalence and socioeconomic costs. Telemedicine has emerged as a promising solution for enhancing asthma management, especially in resource-limited settings and in response to the increasing demand for specialized care, particularly after the coronavirus disease 2019 (COVID-19) pandemic. However, its integration into routine clinical practice is hindered by limited evidence and the absence of standardized protocols tailored to younger populations. Telemedicine offers the potential to optimize healthcare delivery, improve access to specialized services, and support continuous patient monitoring. This initiative aims to address current gaps in standardized practices, ensuring equitable, efficient, and personalized care, particularly in underserved regions. A systematic review of literature on telemedicine and asthma was conducted using MEDLINE, EMBASE, Cochrane Library, and PsycINFO databases, up to October 2024. Studies were evaluated for effectiveness, safety, patient satisfaction, and ethical considerations. International guidelines were also reviewed, and recommendations were formulated through a modified Delphi process with a panel of seven experts, adhering to Oxford Evidence-Based Medicine grading. Telemedicine significantly enhances asthma management, improving treatment adherence, quality of life, and patient education while reducing unplanned visits. It is particularly beneficial for regions with limited access to specialized care. However, challenges persist, including insufficient data on cost-effectiveness, gaps in professional training, and technological barriers. Telemedicine is a valuable tool for managing pediatric and adolescent asthma, offering numerous benefits in accessibility and care continuity. Nevertheless, further research is needed to address existing challenges, establish best practices, and ensure its adaptability to diverse clinical settings, ultimately paving the way for more effective and equitable asthma care.
Asthma is the most prevalent chronic respiratory disease among pediatric and adolescent populations, representing a significant socio-health burden due to its rising incidence in recent decades. In Spain, its prevalence is approximately 10%, like rates observed across Europe [1]. The advent of new technologies has profoundly influenced healthcare delivery, introducing concepts such as “eHealth” (electronic health) and the use of “telemedicine” [2]. Telemedicine employs communication tools to provide healthcare services remotely, offering innovative opportunities to improve disease control and treatment adherence for conditions like asthma. Although telemedicine was relatively underutilized before, the SARS-CoV-2 pandemic highlighted its relevance and accelerated its adoption [3, 4].
In response to societal changes and increasing demands for healthcare efficiency, resources have been reallocated toward virtual consultations in specialties such as pulmonology and allergology [5]. Telemedicine enables healthcare professionals to engage with patients in novel ways, including the collection of critical data that was previously challenging to obtain. This capability is particularly relevant for managing chronic diseases like asthma, given the increasing demand for specialized care and the limitations in resource availability [6]. Despite its potential, current evidence regarding the effectiveness and safety of telemedicine in managing asthma in pediatric and adolescent populations remains limited. The lack of standardized protocols further hinders its integration into routine clinical practice for these age groups. Consequently, there is an urgent need to establish specific telemedicine protocols tailored to the unique requirements of pediatric and adolescent patients with asthma [6].
Developing such protocols involves identifying suitable healthcare interventions and addressing sensitive issues, such as information privacy, in accordance with stringent governmental regulations [3, 6]. These protocols aim to systematize medical care while considering the unique developmental and psychosocial needs of this population, including personalized care and active collaboration with parents, guardians, or legal representatives. Moreover, adapting healthcare services to leverage new technologies is essential to achieve equitable, efficient, and patient-centered care [1, 3, 4]. By promoting research and fostering innovation, these efforts seek to improve the management of asthma in pediatric and adolescent populations, ultimately enhancing their quality of life. Implementing a comprehensive telemedicine protocol represents a strategic opportunity to advance pediatric pulmonology and allergology care for allergic asthma, aligning healthcare services with the current and future needs of patients, families, and the healthcare system in Spain.
This protocol not only aims to systematize medical care but also addresses the unique needs of this age group, including personalized care, sensitive information management, and collaboration with parents, legal representatives, or guardians. Developing this protocol is justified by the need to adapt healthcare services to new technologies and provide more equitable, efficient, and personalized care.
The study employs a mixed-methods methodological design, including a systematic review of the literature and consultation with a panel of experts to reach a consensus. It develops a specific protocol for the management of pediatric and adolescent patients with asthma through telemedicine and integrates current available scientific evidence with clinical experience. This combination gives it a hybrid nature while adapting the recommendations to the particularities of the Spanish healthcare system.
A systematic search was conducted in the following electronic databases to identify relevant publications on telemedicine and asthma, including studies on effectiveness, safety, patient satisfaction, and ethical aspects: MEDLINE (via PubMed); EMBASE; Cochrane Library; CINAHL; PsycINFO.
The search was limited to articles published in English and Spanish up to October 31, 2024. The process of developing the article began in January 2021. The following search terms and their combinations were used: “telemedicine”, “telehealth”, “asthma”, “pediatric”, “adolescent”, “protocol”, “guideline”, “management”, and “treatment”. In addition, international clinical practice guidelines on telemedicine and pediatric asthma from the following organizations were reviewed:
European Academy of Allergy and Clinical Immunology (EAACI).
Global Initiative for Asthma (GINA).
American Academy of Allergy, Asthma & Immunology (AAAAI).
American Telemedicine Association (ATA).
Studies evaluating telemedicine interventions in the management of asthma in pediatric and adolescent patients were included. Studies that did not report relevant clinical outcomes or were not available in English or Spanish were excluded. Finally, the methodological quality of the included studies was assessed using the “Cochrane Risk of Bias Tool”.
This protocol was developed with the collaboration of a panel of experts comprising seven healthcare professionals from the National Health System (SNS) with experience in managing pediatric and adolescent patients with asthma and the use of telemedicine. All experts were allergologists with specialized training through the Medical Internship and Residency (MIR) program in allergology in Spain, specifically focused on pediatrics. The expert panel participated in a two-round modified Delphi process to:
Validate the results of the systematic review.
Provide consensus on the protocol’s recommendations, considering the available evidence, clinical experience, and the specific needs of the pediatric and adolescent population with asthma. In cases where disagreements arose, they were resolved through a consensus-based approach. Panelists participated in a structured voting process for each contested issue, ensuring that all perspectives were considered. If the predefined consensus threshold (≥ 80% agreement) was not met in the first round, further discussions were conducted, followed by an additional round of voting. This iterative process facilitated a balanced resolution and the development of well-founded recommendations. The Delphi methodology was employed to achieve consensus on the key recommendations derived from the systematic review, ensuring alignment with clinical practice. In the first round, panelists independently reviewed and rated statements related to telemedicine feasibility, effectiveness, safety, adherence, and implementation. Statements were evaluated using a Likert scale (1 = strongly disagree to 5 = strongly agree). Consensus was defined as achieving at least 80% agreement (ratings of 4 or 5). Statements that did not reach this threshold were revised and reassessed in the second round.
The Delphi process addressed the following areas:
Feasibility and implementation—What are the essential requirements for telemedicine in asthma management?
Effectiveness and adherence—How does telemedicine impact symptom control, medication adherence, and quality of life?
Safety and ethical considerations—What are the primary risks, which include data privacy concerns, and legal aspects?
Hybrid models of care—What is the optimal balance between telemedicine and in-person visits?
Recommendations for standardization—What are the key clinical guidelines for integrating telemedicine into routine practice?
Consensus levels achieved: in the first round, 75% of statements reached consensus. Items that did not meet the consensus threshold were revised based on expert feedback. In the second round, after refinement and reevaluation, all remaining statements attained a final consensus level of ≥ 85%, validating the recommendations presented in this study.
The levels of evidence and recommendation grades were based on an adapted approach from the Oxford Centre for Evidence-Based Medicine [7]. This adaptation involved providing a bias risk assessment, based on the “Cochrane Risk of Bias Tool”, of the underlying evidence and highlighting other potentially relevant contextual information. Additionally, the phrasing of recommendations was aligned with their grade (Table 1). The recommendations were formulated according to the following grades: Grade A: “is recommended”; Grade B: “may be recommended”; Grade C: “could be recommended”; Grade D: “may be considered”.
Assignment of levels of evidence and strength of recommendations [9]
| Category | Description |
|---|---|
| Level of evidence | |
| Level I | Systematic reviews, meta-analyses, randomized controlled trials. |
| Level II | Two-group studies, non-randomized (e.g., case-control or cohort studies). |
| Level III | One-group studies, non-randomized (e.g., pre-post studies, before-and-after designs). |
| Level IV | Descriptive studies including variable analysis (e.g., single-subject designs, case series). |
| Level V | Case reports and expert opinions, including narrative reviews, literature reviews, and consensus statements. |
| Grade of recommendation | |
| Grade A | Consistent level I studies. |
| Grade B | Consistent level II or III studies, or extrapolations from level I studies. |
| Grade C | Level IV studies, or extrapolations from level II or III studies. |
| Grade D | Level V evidence or concerningly inconsistent or inconclusive studies at any level. |
| Strength of recommendation | |
| Strong | Evidence from studies with a low risk of bias. |
| Moderate | Evidence from studies with a moderate risk of bias. |
| Weak | Evidence from studies with a high risk of bias. |
Reprinted with permission from [45]. © 2020 EAACI and John Wiley and Sons A/S
A sample size calculation was not required, as this study does not involve empirical data collection or hypothesis testing. As it is based on a systematic review of the literature and expert consultation, calculating a sample size is unnecessary. Moreover, a statistical analysis was not required since the work is not an experimental or observational study that generates its own quantitative data. Instead, it analyzes existing evidence from prior studies, collecting qualitative information and expert recommendations.
In carrying out this work, the authors strictly adhered to the guidelines established by the Spanish Medical Code of Ethics [8], the Tokyo Amendment to the Declaration of Helsinki [9], and the International Directives on Clinical Research. However, it was not necessary to seek approval from an ethics committee because the work consists of a literature review and expert consultation, which do not pose ethical risks to any participant, as it does not involve the collection of original patient data, direct interventions, or the study of clinical variables in human subjects.
A systematic review of the literature was conducted to evaluate the effectiveness, safety, patient satisfaction, and ethical considerations of telemedicine interventions in pediatric and adolescent asthma management. A total of 20 studies (eight randomized clinical trials, seven systematic reviews, and five observational studies) were included in the systematic review based on predefined eligibility criteria. Table 2 summarizes the key characteristics of these studies, including study design, sample size, intervention type, key findings, level of evidence, and risk of bias assessment.
Summary of the studies included in the systematic review
| Author (Year) | Study type | Sample size (number of patients or studies) | Intervention | Key findings | Level of evidence | Biase evaluation |
|---|---|---|---|---|---|---|
| Xu et al. [34] (2010) | Randomized clinical trial | 121 patients | Interactive voice response system versus specialist nurse support versus usual care. | Lower healthcare costs in digital intervention groups, with interactive voice response being the most cost-effective. | I A | Low |
| Beerthuizen et al. [35] (2016) | Randomized clinical trial | 272 patients | Web-based asthma monitoring. | No significant differences in costs. Web-based monitoring was most cost-effective from a healthcare perspective. | I A | Moderate |
| van den Wijngaart et al. [14] (2017) | Randomized clinical trial | 210 patients | Virtual asthma clinic (VAC) versus usual care. | Asthma control and symptom-free days improved significantly more in the VAC group, reducing outpatient visits by 50%. | I A | Low |
| van den Wijngaart et al. [33] (2017) | Randomized clinical trial | 210 patients | Virtual asthma clinic versus usual care for asthma management. | Virtual visits reduced outpatient visits by 50% while maintaining asthma control. | I A | Low |
| Morton et al. [13] (2017) | Randomized clinical trial | 77 patients | Electronic adherence monitoring. | Improved adherence with reminder devices. | I A | Moderate |
| Perry et al. [30] (2017) | Randomized clinical trial | 34 patients | Smartphone-based versus paper-based asthma action plans for self-management. | Improved asthma control test scores and reported high satisfaction with smartphone. | I A | Moderate |
| Halterman et al. [17] (2018) | Randomized clinical trial | 400 patients | School-based telemedicine program versus enhanced usual care. | Telemedicine increased symptom-free days and reduced emergency visits/hospitalizations. | I A | Moderate |
| Perry et al. [18] (2018) | Randomized clinical trial | 393 patients | School-based asthma education via telemedicine versus usual care. | Increased use of peak flow meters and improved medication adherence. | I A | Moderate |
| Belisario et al. [41] (2013) | Systematic review (Cochrane review) | 2 studies | Smartphone and tablet-based asthma self-management apps versus traditional paper-based methods. | Findings were inconclusive; one study showed no impact on symptoms or healthcare use, while another reported improved quality of life, lung function, and fewer emergency visits. | I A | High |
| Vazquez-Ortiz et al. [43] (2020) | Systematic review | 108 studies | Analysis of challenges faced by adolescents and young adults with asthma and allergic conditions. | The review identified five key challenges: quality of life impairment, psychological factors, adherence issues, self-management facilitators, and supportive relationships. Most studies focused on asthma, with limited data on other allergic conditions. | I A | Moderate |
| Knibb et al. [40] (2020) | Systematic review | 30 studies | Psychological, e-health, educational, peer-led, and breathing retraining interventions for asthma self-management. | All interventions improved self-management, quality of life, and adherence, but most were feasibility or pilot studies. No studies included allergic conditions beyond asthma. | I A | Moderate |
| Kim et al. [6] (2020) | Systematic review | 7 studies | School-based interventions. | Benefits of school-based telemedicine. | I A | Moderate |
| Culmer et al. [31] (2020) | Systematic review | 5 studies | Telemedical asthma education for school-age children. | Telemedicine-based asthma education showed mixed results but improved caregiver quality of life and self-management. | I B | Moderate |
| Snoswell et al. [36] (2021) | Systematic review and meta-analysis | 16 studies | Interactive telehealth interventions for asthma management. | Telehealth interventions slightly improved quality of life, with web portals being the most effective, followed by smartphone apps and remote monitoring. | I A | Low |
| Shah & Badawy [15] (2021) | Systematic review | 11 studies | Telemedicine in pediatric asthma. | Benefits in adherence and symptom control. | I A | Low |
| Jochmann et al. [46] (2017) | Observational study | 93 patients | Electronic monitoring of inhaled corticosteroids (Smartinhaler) to assess adherence. | Electronic monitoring identified four patient groups by adherence and asthma control. 58% showed suboptimal adherence. | III C | High |
| Khaleva et al. [44] (2020) | Observational study | 1,179 patients | Survey on current transition management for adolescents and young adults with allergy and asthma. | Most healthcare professionals reported lacking transition guidelines and structured processes. Nearly half noted poor communication between pediatric and adult services. | III C | High |
| Jácome et al. [39] (2021) | Observational study | 107 patients | InspirerMundi app for monitoring asthma medication adherence through gamification, symptom tracking, and social support. | The app was feasible and well-accepted for monitoring medication adherence. | III C | High |
| Haynes et al. [47] (2022) | Observational study | 502 patients | Assessment of telemedicine use for pediatric asthma care. | Families valued better access but reported challenges with measurements and scheduling. | III C | Moderate |
| Radhakrishnan et al. [32] (2022) | Observational study | 100 patients | Comparison of in-person versus virtual asthma education. | Virtual and in-person asthma education were equally effective, with 65.2% preferring virtual education for its safety, convenience, and accessibility. | III C | High |
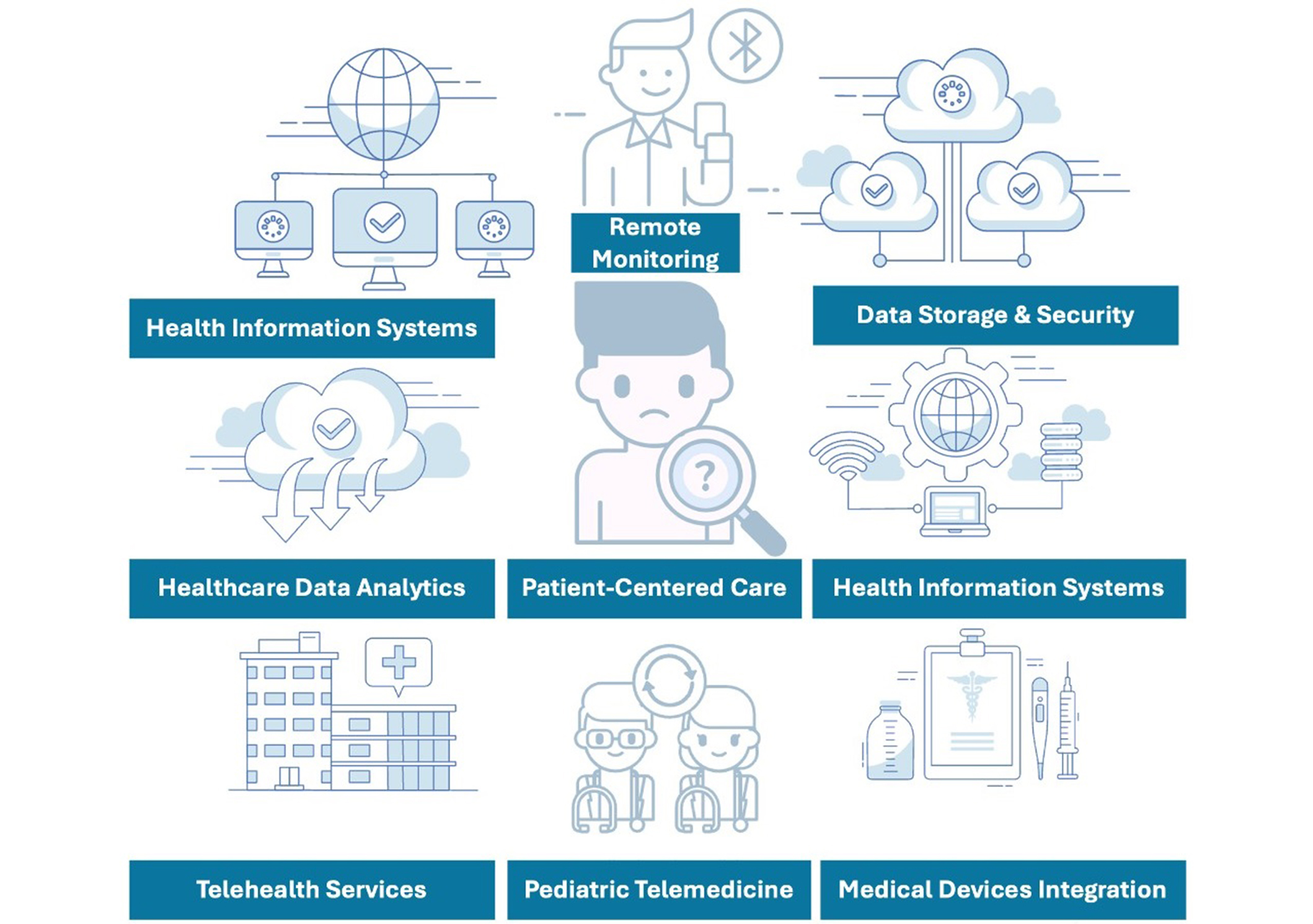
Patients and healthcare professionals must have access to adequate technical resources, not have disabilities that prevent them from using these systems, and, above all, be willing to use them [3–5]. Additionally, unlike adults, pediatric and adolescent asthmatic patients still require the presence of their parents, guardians, legal representatives, or caregivers during virtual consultations. Therefore, potential additional costs, as well as the ethical, cultural, and legal implications of large-scale telemedicine use, must be considered [3]. Figure 1 details possible actions to be carried out during an asthma telemedicine consultation [5]. Nevertheless, it is also important to emphasize that telemedicine should never exclude the possibility of an in-person follow-up visit if deemed necessary by the specialist [4, 5].
Actions to be carried out during a telemedicine consultation for pediatric and adolescent asthmatic patients
It is crucial to define strategies that include disease monitoring and treatment adherence for pediatric and adolescent asthmatic patients, which are currently limited when telemedicine is not employed. Digital technologies and telemedicine are promising tools to overcome these barriers in healthcare delivery [10–12]. Moreover, tele-self-help groups and peer asthma groups can be valuable strategies to enhance adherence and provide emotional support for patients. These initiatives offer a sense of community and shared experiences, which can positively impact treatment commitment and disease management [3, 5, 10, 11]. Figure 2 outlines telemedicine self-management strategies that contribute to monitoring and improving adherence in pediatric and adolescent asthma patients.
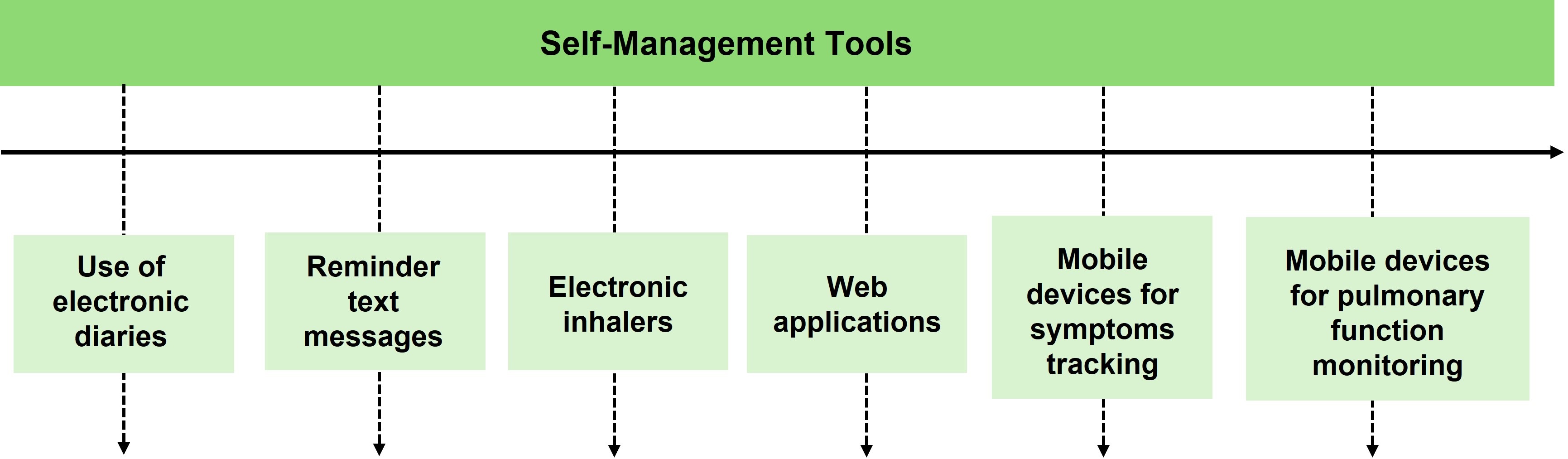
Self-management strategies that contribute to monitoring and improving adherence to telemedicine
The primary tool for evaluating asthma control has traditionally been the follow-up medical visit. However, the pandemic created an unprecedented situation in which in-person visits were not possible, prompting the implementation of previously underutilized interventions to ensure the management of asthma patients. Current studies [2, 5, 6, 10–15] on telemedicine demonstrate improvements in quality of life and symptom management, indicating that virtual education indeed offers benefits. Moreover, current evidence shows that the control of pediatric and adolescent asthma patients through telemedicine-based interventions is comparable to that achieved through in-person visits [15–17]. Table 3 describe tools that can enhance the control and quality of life of pediatric and adolescent asthma patients using telemedicine.
Tools to improve the control and quality of life of pediatric and adolescent patients with asthma through telemedicine
| Tool | General description/Use | Benefits and limitations | Level of evidence |
|---|---|---|---|
| Pulmonary function tests | Useful at home to ensure proper follow-up [11]. | Performing spirometry or peak flow meters without the presence of a physician does not imply a decrease in the quality of the tests. | II B weak. |
| Remote spirometry or peak flow meters emerge as a promising tool for long-term asthma management [12]. |
| II B moderate. | |
| Smart inhalers | Smart inhalers, devices are useful for asthma management [13, 14]. | Reduced use of rescue medication; improved asthma control; reduced exacerbations; reduced hospital admissions.
| III C moderate. |
| Questionnaires | Completed via email, video call, or phone contact. |
| I B moderate. |
There are software programs, typically in the form of mobile applications, that allow users to log when they use their device, report symptoms, record the need for rescue medication, and even provide information about atmospheric conditions such as temperature, environmental humidity levels, and pollen counts, among others, to help avoid crisis-triggering factors [14].
Education for pediatric and adolescent asthmatic patients and their families increases their quality of life, reduces the risk of exacerbations, and lowers the healthcare costs associated with the disease, making it one of the fundamental pillars of treatment [1–3, 17, 18]. The goal is to enable the patient to lead a normal life for their age, including physical and sports activities. Education is necessary to improve treatment adherence and achieve disease control, so patients and their families must be equipped with the necessary skills for self-care and therapeutic compliance, considering their needs, prior knowledge, age, asthma severity, the level of involvement required for self-management and treatment, as well as their beliefs [1, 3, 17, 18, 19]. In this regard, tele-self-help groups and peer asthma groups can be valuable strategies to support education for pediatric and adolescent patients and their families. These initiatives can help families gain a better understanding of the disease, reinforce key educational aspects, and strengthen the asthma patient community [3, 17, 18, 19]. By promoting interaction among patients and caregivers, these groups encourage knowledge exchange and shared decision-making, ultimately leading to improved self-management [3, 17, 18, 19]. Figure 3 summarizes the main interventions necessary for educating pediatric and adolescent asthma patients. Additionally, telemedicine extends beyond traditional medical care and encompasses diverse applications, including tele-education [9, 15, 16, 18], teleconsultation [5, 9, 16], tele-practice [9, 16], and tele-research [1, 9, 15, 16]. These applications leverage technology to enhance medical services and improve patient outcomes in various ways:
Tele-education [9, 15, 16, 18]. Interactive audiovisual links create virtual classrooms for doctors, patients, and families (level of evidence III C strong).
Live video streaming.
Access to stored educational materials.
Use of mobile phones.
Wearable devices, such as smartwatches for emails, calls, or payments, and fitness trackers for monitoring respiratory rate, oxygen saturation, heart rate, or physical activity.
Body sensors track vital signs, brain activity, or sleep quality, including tattoo-like skin sensors and electronic subdermal sensors.
Sports insoles for gait monitoring and injury prevention.
Baby wearables like socks or clothing clips monitor respiration, temperature, position, and activity levels via mobile apps.
Teleconsultation [5, 9, 16]. Strengthens the doctor-patient-family connection by enabling consultations regardless of location (level of evidence II B, moderate).
Addresses daily concerns and updates action plans as needed.
Tele-practice [9, 16]. Enhances patient and family engagement (level of evidence II B, moderate).
Webinars for peer or doctor-patient interactions.
Websites offer accessible and reliable information about illnesses.
Social media platforms for medical education and scientifically validated information.
Online self-care programs.
Tele-research [1, 9, 15, 16]. Gathers asthma-related data remotely via video calls, mobile apps, and remote monitoring systems (level of evidence II B, moderate).
Collects data from large patient groups to better understand diseases and identify patterns.
Contributes valuable data for “Big Data” systems, enabling advanced analyses like phenotyping and exposome evaluation.
Necessary interventions in the education of pediatric and/or adolescent asthmatic patients
Table 4 outlines the inclusion and exclusion criteria, necessary resources, and ethical and legal considerations for implementing a telemedicine protocol for pediatric and adolescent asthmatic patients [17, 20, 21]. These elements are essential to ensure proper patient selection, efficient use of human resources, and adherence to ethical and legal standards in the use of information and communication technologies (ICT) in clinical processes. It is also important to note that depending on the methods used for telemedicine, the material resources required for its implementation may vary [17–22]. Below are the resources required for telemedicine based on the method used:
General requirements
Device access: A reliable phone, smartphone (Android or iOS), or computer with a phone line and internet connection.
Electronic health records (EHR): Secure access to a General Data Protection Regulation (GDPR) compliant system for storing and retrieving patient data.
Electronic prescription system: Integration with dispensing capabilities for prescriptions.
Email: Professional email accounts for healthcare providers and personal email for guardians to facilitate communication and material sharing.
Method-specific requirements
Phone call [22]. (i) Suitable for quick consultations and follow-ups; (ii) Requires the setup of secure channels for recording activities in EHR systems.
Video call [23–25]. (i) Additional needs: Quiet, well-lit, and distraction-free environment; Stable internet connection to ensure uninterrupted audio and video; Headphones for improved sound quality and privacy; Video platforms must be secure, encrypted, and compliant with clinical standards (for example UPmédica, HealthTap, Zoom for Healthcare); (ii) Clear protocols must guide how data is integrated into the EHR or handled otherwise; (iii) Informed consent is mandatory, with documentation detailing the service’s features and limitations.
Material resources [1, 3, 5, 26–31]
Smartphone applications: For symptom tracking, medication reminders, self-care, and educational support (for example Asthma Forum App).
Educational materials: Questionnaires (for example asthma control tests or inhaler adherence tests) and validated digital educational content.
Home monitoring devices: Peak Flow Meter for respiratory monitoring; Mobile spirometry devices with data-sharing capabilities (for example AirNext® spirometer with Nuvoair® platform).
Pulmonary function tests: Advanced options are available at health centers for detailed evaluations.
Telemonitoring platforms: Facilitate real-time data collection (for example peak flow, questionnaires) and sharing with healthcare teams. Enable remote evaluation of clinical conditions, track variability, and customize intervention thresholds.
Considerations for the implementation of a telemedicine protocol in pediatric and adolescent patients with asthma
| Category | Description/Requirements |
|---|---|
| Inclusion criteria | A legal guardian who consents and is willing to participate and adhere to the teleassistance protocol. |
| Familiarization of the patient and guardian with the use of mobile phones, tablets, computers, and software applications. | |
| Availability of a mobile phone, tablet, computer, and internet connection (if the patient does not have a mobile phone, it may be necessary to provide a device for use during the follow-up period). | |
| Evaluation of asthma stratification criteria that may be considered inclusive: poorly controlled asthma, telematic follow-up after admission to the Pediatric Intensive Care Unit, asthma in adolescent patients, among others. | |
| Exclusion criteria | Patients or families who are hypo-perceptive or hyper-perceptive of the disease. |
| Physical, cognitive, or linguistic barriers affecting the legal guardian or the minor that prevent teleassistance. | |
| Other conditions determined by the team responsible for the teleassistance program. | |
| Human resources | Medical healthcare professionals: pediatric allergist/pulmonologist or physicians responsible for asthma units. |
| Non-medical healthcare professionals: nursing staff (with specific training in asthma)/nursing assistants. | |
| Non-healthcare personnel: administrative staff (scheduling appointments, managing agendas, and patient communication). | |
| Evaluation and follow-up | It is essential to monitor teleconsultation activities, which requires the development of appropriate indicators. |
| Ethical and legal aspects of using teleconsultation | We must understand the ethical aspects linked to the use of information and communication technologies in clinical processes, ensuring elements such as equity in access to services and the availability of appropriate technology to access these services. |
Access to telemedicine with bidirectional communication between parents and healthcare providers reduces unplanned visits to hospitals or primary care centers (Figure 4). Additionally, parents who receive asthma education via telemedicine, compared to those who receive it in person, prefer this type of education as a safer option that reduces exposure to infections [17, 18, 31, 32]. One of the main reasons identified for parents/caregivers’ preference for telemedicine is the greater convenience and accessibility in terms of time and cost, which translates into increased flexibility and adaptability to family lifestyles, greater participation by more family members, and the avoidance of school and work absenteeism [1, 3, 18, 19, 29–32].
Most existing studies on telemedicine and asthma in children and adolescents focus on its acceptability and technical feasibility [1, 3, 5, 6, 29–32]. Few studies evaluate its clinical efficacy, and even fewer assess the cost-efficiency of telemedicine for pediatric asthma. Table 5 describes the main studies on cost-effectiveness and efficiency published to date [14, 33–35].
Summary of studies on cost-effectiveness and cost-efficiency of telemedicine in pediatric and adolescent asthmatic patients
| Author | Number of patients (follow-up) | Study groups | Results | Scientific evidence |
|---|---|---|---|---|
| van den Wijngaart et al. [14, 33], Netherlands | 210 patients (6–16 years) follow-up: 16 months. |
|
| I A weak |
| Xu et al. [34], Australia | 121 patients (3–16 years) follow-up: 6 months. |
| The total healthcare cost was significantly lower for patients who received nursing phone calls and in the group with automated telephone assistance compared to the control group (cost reduction of A$225 and A$451 per patient, respectively) [36]. | I A moderate |
| Beerthuizen et al. [35], Netherlands | 272 pediatric patients (4–18 years) follow-up: 12 months. |
| No differences were found in costs or cost-effectiveness. | I A moderate |
The use of digital technology in pediatric and adolescent asthmatic patients offers significant strengths in managing asthma among pediatric and adolescent patients by addressing key objectives in disease management [36, 37]. It facilitates the identification of the disease, monitors its progression, and recognizes factors contributing to exacerbations and reduced quality of life. These are achieved through remote patient monitoring using electronic devices, recording inhaler usage, collecting objective data, and obtaining quantitative information. Additionally, telemedicine aids in identifying the exposome after recognizing different phenotypes and endotypes by providing access to quantitative data, integrating exposome-related information, refining phenotype definitions, and improving the understanding of varied therapeutic responses. These capabilities collectively enhance personalized and effective asthma management. However, telemedicine also presents factors that represent weaknesses [38, 39] as a tool for routine management and follow-up in asthmatic patients as described in Table 6.
Weaknesses of telemedicine in pediatric and adolescent asthmatic patients
| Challenge | Description of the barrier |
| Key challenges in telemedicine implementation | Detailed barriers to effective telemedicine adoption. |
| Preference for personal interaction | Doctor-patient interaction is highly valued*. Many patients feel more reassured when physically examined by their doctor, despite clinical history being the primary tool in allergy diagnosis. |
| Disconnect between telemedicine results and daily practice integration | A real gap exists in incorporating telemedicine outcomes into routine medical records#. |
| Concerns about privacy and confidentiality | Limited trust in the ability of telemedicine tools to ensure privacy and confidentiality. |
| Challenges in data transfer | Significant difficulty transferring information from telemedicine platforms to standard healthcare management programs. |
| Inequitable technology use | Lack of uniformity in technology usage among the population, where errors in responses may lead to misinterpretation of results. |
| Lack of evidence | Currently, there are no systematic reviews to support outcomes or clarify cost-benefit (profitability, standardization, among others). |
*Despite the increase (> 70%) in the use of telemedicine during the first lockdown in 2020, the numbers dropped drastically after in-person interaction resumed, with usage rates in subsequent waves falling to 5–10% [38]. #A project related to the use of an asthma app demonstrated low patient interest, with participation rates below 5% [39]
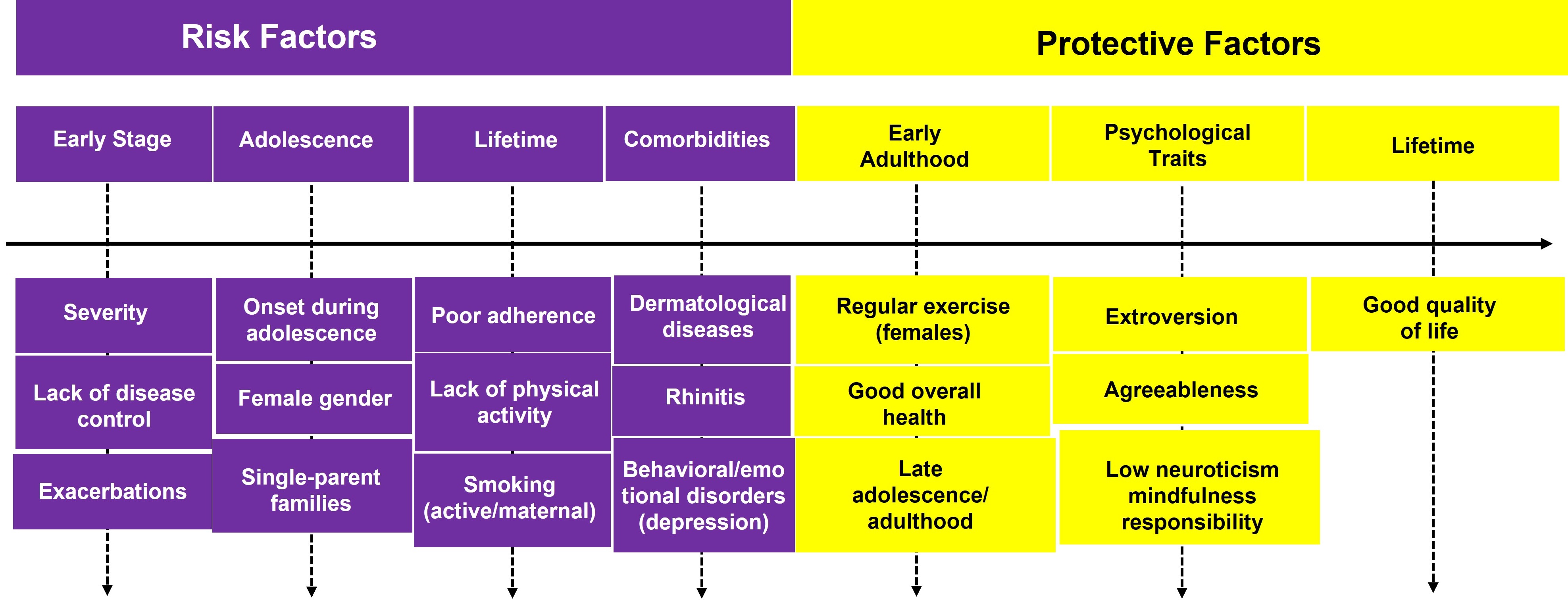
It is now known that all digital health-based interventions are significantly associated with improved asthma control (Figure 5), especially in adolescents and young adults (AYAs) with moderate or severe uncontrolled asthma [40, 41]. In Spain, AYAs value psychological support and digital technology the most [42]. In this context, online platforms, mobile applications, and video calls become tools that empower adolescents, allowing them to take an active role in managing their asthma, including personalized education, continuous monitoring, emotional support, and smooth communication with healthcare professionals, thus improving their quality of life [43–45]. Furthermore, telemedicine can facilitate the transition of adolescent asthma patients to adult healthcare systems, promoting the continuity of specialized medical care [44, 45].
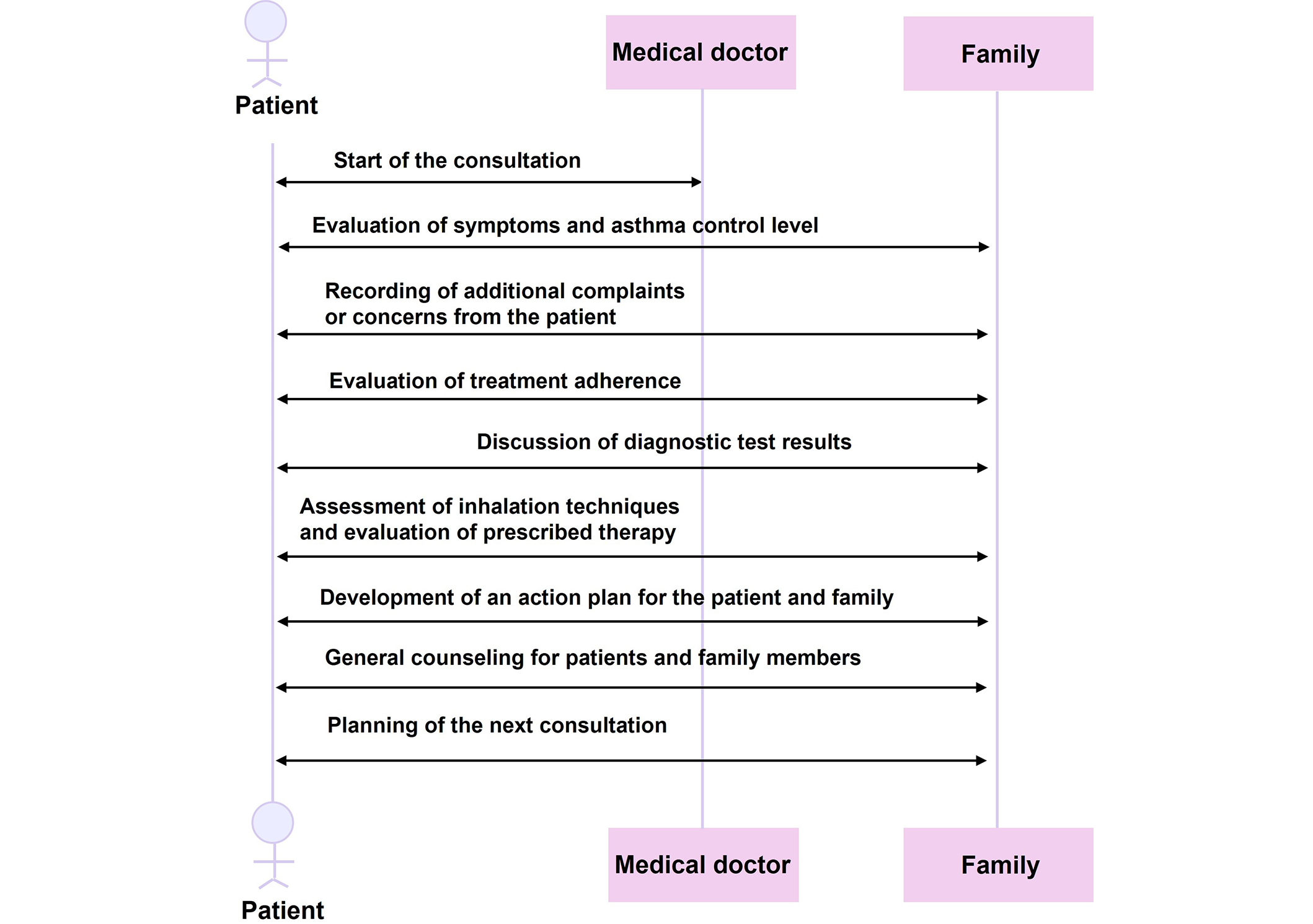
Based on the results of the systematic review and expert consultation, recommendations for the use of telemedicine in pediatric and adolescent asthma patients were established. Table 7 details each recommendation along with its level of scientific evidence, providing a clear and well-supported protocol for clinical practice [6, 13–15, 17, 18, 30–32, 34–36, 39–41, 43, 44, 46, 47]. Moreover, Figure 6 illustrates the structured asthma consultation process, detailing the key stages from pre-consultation to follow-up visits. It provides a visual representation of the step-by-step approach, highlighting essential components such as patient assessment, treatment planning, and post-consultation monitoring. This structured framework ensures a comprehensive and effective management of asthma care.
Recommendations for clinical practice of telemedicine in pediatric and adolescent asthmatic patients
| Recommendation category | Recommendation description | Level of evidence and strength |
|---|---|---|
| Recommendation Grade A (“is recommended”) | ||
| Telemedicine for control and follow-up | The use of telemedicine is recommended for pulmonary function testing, medication, and symptom tracking, as well as for control and quality of life questionnaires in the management and follow-up of pediatric and adolescent asthma patients. | I A moderate |
| Quality of life in patients with severe asthma | The use of telemedicine is recommended to improve the quality of life of pediatric and adolescent asthma patients, especially those with severe asthma. | I A moderate |
| Cost-effectiveness of telemedicine | It is recommended to evaluate the cost-effectiveness of the various tools encompassed by telemedicine separately. | I A moderate |
| It is recommended to analyze the cost-effectiveness of telemedicine for the follow-up of pediatric and adolescent asthma patients and as a complement to conventional visits. | I A moderate | |
| Recommendation Grade B (“may be recommended”) | ||
| Mixed approach | The mixed approach, alternating telemedicine with in-person visits, may be recommended for the appropriate management of asthma in pediatric and adolescent patients. | I B moderate |
| Adolescent patient with asthma | Telemedicine may be recommended as an essential tool in the management of asthma in adolescent patients. | I B moderate |
| Telemedicine may be recommended to overcome barriers of distance and accessibility and to provide a personalized approach that improves the quality of life of adolescent patients with asthma. | IV B moderate | |
| Difficult-to-control asthma | Telemedicine may be recommended for patients with difficult-to-control asthma to assess treatment adherence, adjust it, and evaluate the need for in-person visits. | II B strong |
| Research | The need for further studies may be recommended to evaluate optimal strategies that ensure satisfaction for patients, their families, and all healthcare professionals. | II B moderate |
| Recommendation Grade C (“could be recommended”) | ||
| Home-based monitoring | The recording of various parameters could be recommended for asthma management from home to enable the early detection of exacerbations. | III C moderate |
| Quality of care | Telemedicine could be recommended to improve the quality of care for pediatric and adolescent patients with asthma. | III C moderate |
| It could be recommended that telemedicine consultations be scheduled only for patients who do not require a physical examination. | III C moderate | |
| Benefits of telemedicine | Telemedicine could be recommended for its beneficial effects on asthma management and control, as well as for the high level of acceptance and satisfaction reported by patients. | III C moderate |
| Digital interventions | Digital interventions that include educational strategies, behavioral approaches, and interactions with medical professionals could be recommended to improve adherence and asthma control. | IV C moderate |
| Recommendation Grade D (“may be considered”) | ||
| Ethical aspects | Ethical issues, privacy, and information security may be considered major concerns and limitations of telemedicine. | V D moderate |
| Technology | The familiarization of patients and their families with the use of mobile phones, tablets, computers, and network applications may be considered essential for the implementation of a telemedicine program. | V D weak |
| Technological solutions can only be considered opportunities for success if combined with the medical team to achieve maximum benefit. | V D weak | |
Structured asthma consultation process-from pre-consultation to follow-up. *ACT/ACQ: Asthma Control Test/Asthma Control Questionnaire; †TAI: Test Adherence to Inhalers (Spanish adherence test); ‡MiniAQLQ/PAQLQ: Mini Asthma Quality of Life Questionnaire/Pediatric Asthma Quality of Life Questionnaire
Telemedicine has emerged as a valuable tool in the management of asthma in pediatric and adolescent patients, especially in the wake of the SARS-CoV-2 pandemic [3–5]. Its implementation has enabled continuity in medical care, demonstrating its potential to improve both disease control and patients’ quality of life [11–15]. However, the results obtained to date present limitations that must be considered when integrating this modality into routine clinical practice. Currently, various studies have demonstrated that digital interventions, such as treatment reminders and the use of applications for symptom tracking, contribute to greater adherence to treatment, a critical factor in the management of pediatric and adolescent asthmatic populations [10].
Additionally, telemedicine allows for closer and more continuous monitoring of the patient’s health status, facilitating early detection of exacerbations and the adjustment and optimization of treatment [36, 37]. In a study conducted on a pediatric population, where electronic devices were used to measure asthma treatment adherence, it was concluded that electronic monitoring devices help distinguish between patients with severe asthma versus difficult-to-control asthma based on adherence [46]. Severe asthma was classified in pediatric patients with good adherence who still had persistent and poorly controlled symptoms. One of the fundamental aspects of pediatric asthma management is patient and caregiver education, which plays a crucial role in ensuring proper disease control and treatment adherence. In traditional clinical settings, physicians dedicate significant time to explaining asthma triggers, treatment plans, and correct inhaler techniques. However, the increasing patient load, limited consultation time, and restricted hospital access may hinder the effectiveness of in-person education [25].
Telemedicine offers an opportunity to bridge this gap by reinforcing patient education through structured virtual sessions, allowing healthcare professionals to provide step-by-step inhaler technique demonstrations, assess patient competence in inhaler use remotely, and offer interactive guidance for asthma self-management. Additionally, it enables caregivers to receive targeted support and continuous access to educational resources, reducing the risk of treatment errors and enhancing asthma control. Moreover, the implementation of tele-self-help groups and patient support networks through telemedicine could significantly improve the quality of life of children and adolescents with asthma. These platforms facilitate ongoing education, emotional support, and peer engagement, helping patients and their families navigate the challenges of asthma management more effectively. Integrating telemedicine into routine asthma management could improve treatment outcomes, reduce hospital visits due to poor disease control, and empower both patients and caregivers with the necessary knowledge to manage the condition more effectively [17–19, 25, 31]. Further research is warranted to evaluate the long-term impact of telemedicine-based educational interventions on adherence and clinical outcomes in pediatric asthma.
This remote monitoring capability not only reduces the need for in-person visits but also decreases the costs associated with asthma management [14, 33, 34]. The cost analysis considered both direct and indirect cost metrics. Direct costs include telemedicine infrastructure, software, and healthcare professional fees, while indirect costs account for patient travel expenses, missed workdays, and caregiver burden reduction. The analysis aimed to provide a holistic assessment of the economic impact of telemedicine compared to traditional in-person consultations. However, although some studies suggest that follow-up through digital means can be as effective as in-person visits with potentially lower costs [14, 33, 34], the evidence is still limited, and more studies encompassing different contexts and populations are needed. High-quality studies are crucial to consider factors such as age, socioeconomic level, and the patient’s study setting (rural/urban), as well as the severity of asthma, to obtain more precise conclusions.
Nonetheless, there are still significant challenges that must be addressed to ensure effective implementation [11, 12]. The clinical accuracy of tests performed at home, such as spirometry, remains a point of contention. Although this test is accessible at home, the variability in the results obtained compared to those performed in hospitals raises questions about its clinical validity and its ability to fully replace in-person evaluations [12]. Therefore, it is crucial to determine in which scenarios and for which patients’ telemedicine can be used effectively without compromising the quality of care for pediatric and adolescent asthmatic patients.
Another relevant aspect is the acceptance and satisfaction of patients and their families. Current data indicate a high degree of acceptance, largely due to the convenience and flexibility this modality offers, particularly in terms of time savings and reduced exposure to potential infections [31, 32]. However, this acceptance may vary depending on the socioeconomic and cultural context of families and their familiarity with technologies. It is essential to consider these variables to avoid exacerbating inequalities in access to healthcare.
Along these lines, ensuring adequate training for patients and caregivers in the use of digital technology, as well as regular follow-up to identify and address difficulties and implement strategies to overcome technological and socioeconomic barriers, is crucial. This protocol acknowledges that socioeconomic and technological disparities may limit access to telemedicine for some patients. To mitigate this issue, several strategies are suggested: (1) providing digital literacy training for patients and caregivers, (2) implementing hybrid care models that combine in-person visits with remote monitoring, (3) integrating telemedicine services into public healthcare programs to ensure equitable access, and (4) offering low-bandwidth solutions, such as phone-based consultations, for patients with limited internet access. Future research should explore policies that support telemedicine adoption among underserved populations. This point is key to ensuring that telemedicine does not exacerbate health inequalities, closes the digital divide, and allows all patients to benefit equitably from telemedicine [6, 46, 47].
Additionally, there are concerns about privacy and data security that must be addressed to ensure patients’ trust in telemedicine services. Ensuring privacy and data security is a fundamental concern in telemedicine. Policymakers can take several steps to mitigate these risks and strengthen the protection of patient information. Key measures include enforcing strict encryption protocols and secure authentication methods to safeguard patient data from unauthorized access, as well as establishing standardized regulations for telemedicine providers regarding data storage, sharing, and patient consent to ensure compliance with privacy laws. Additionally, increasing patient education on their rights concerning digital health records and best practices for secure telemedicine interactions can further enhance data security. Another crucial step is the development of interoperable systems that facilitate secure data exchange between healthcare providers while maintaining confidentiality and preventing breaches [8, 21, 22, 24]. Data protection regulations, such as the GDPR of the European Union [22–25], establish clear standards that must be met. However, integrating these requirements into telemedicine platforms still faces technical and operational challenges [38, 39].
Future research should explore the effectiveness of current privacy frameworks in telemedicine and investigate new strategies to enhance patient trust and regulatory compliance in digital healthcare environments. These efforts will be essential in promoting the sustainable and ethical integration of telemedicine in routine healthcare practice. It is also important to point out that although telemedicine has proven to be an effective tool in many cases, it cannot be considered a complete substitute for in-person consultations. Additionally, to effectively implement telemedicine, it should be highlighted that the cooperation of the patient and/or their caregivers, the absence of additional mental health issues, and access to technological resources are crucial. Therefore, telemedicine may currently be applicable to a limited patient population, and necessary infrastructure conditions must be established for its implementation. Moreover, it might be also worth evaluating not only the short-term but also the long-term patient adherence to telemedicine (for example treatment compliance) and considering that face-to-face communication is always more effective than virtual interactions, particularly in ensuring that the patient takes the disease and treatment seriously [19, 22–25]. Finally, the coronavirus disease 2019 (COVID-19) (SARS-CoV-2) pandemic significantly accelerated the adoption of telemedicine, transforming healthcare delivery worldwide. Several studies have examined the impact of telemedicine during the pandemic, highlighting both its strengths and challenges. Telemedicine was instrumental in ensuring continuity of care, reducing the risk of viral exposure, and optimizing resource allocation in overwhelmed healthcare systems. However, studies also reported limitations, including disparities in access due to technological and socioeconomic barriers, difficulties in conducting physical examinations, and concerns about data security and patient privacy [22–25, 38].
Despite these challenges, the pandemic provided valuable insights into the feasibility of long-term telemedicine implementation. The lessons learned have informed ongoing efforts to integrate telemedicine into routine pediatric asthma care, ensuring a more structured, equitable, and efficient approach to remote healthcare services. Future research should continue evaluating the impact of telemedicine beyond the pandemic to refine best practices and maximize its potential in pediatric allergy and asthma management [19, 23, 24, 38].
Hence, telemedicine should complement and enhance traditional medical care but not completely replace it. Physical visits remain essential for the initial evaluation of the patient, performing complex diagnostic tests, and when a detailed physical examination is required [4, 5]. Therefore, a hybrid approach combining telemedicine with in-person visits is suggested, optimizing the benefits of both modalities [6].
Finally, due to the rapid evolution of telemedicine and digital health tools, it is recommended that this protocol be reviewed every 2 years to incorporate emerging technologies, regulatory changes, and clinical best practices. Additionally, continuous feedback from patients and healthcare providers should be collected to ensure that the protocol remains relevant and effective.
In conclusion, telemedicine offers a promising alternative for the management of pediatric and adolescent asthmatic patients, especially in situations where access to in-person care is limited. However, its widespread implementation requires careful planning that considers current limitations, technological and legal requirements, and the need for a personalized approach for each patient. It is essential to continue researching to validate its clinical effectiveness, cost-effectiveness, and long-term acceptance among pediatric and adolescent asthmatic patients and their families.
AYA: adolescents and young adults
COVID-19: coronavirus disease 2019
EHR: electronic health records
GDPR: General Data Protection Regulation
ICT: information and communication technologies
The authors thank Dr. Carmelo Escudero and Dr. Sonsoles Infante, both coordinators of the Pediatric Allergy Committee of the Spanish Society of Allergology and Clinical Immunology, for their invaluable assistance in the development of this project. We also extend our gratitude to Dr. Silvia Sánchez-García for her collaboration in this project as the coordinator of the Pediatric Respiratory Allergy Working Group of the Pediatric Allergy Committee of the Spanish Society of Allergology and Clinical Immunology.
PMB, OAG, PCF, SFC, MESM, and MTP: Investigation, Writing—original draft, Writing—review & editing, Validation. TGB: Investigation, Writing—original draft, Writing—review & editing, Validation, Conceptualization, Supervision. All authors read and approved the submitted version.
The authors declare no conflicts of interest related to this work.
Not applicable.
Not applicable.
Not applicable.
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 7119
Download: 48
Times Cited: 0
Riyad Allehebi, Hamdan AL-Jahdali
Yasmeen Othman ... Asmaa Ali
Maria Michelle Papamichael, Charis Katsardis
Yuto Hamada ... Peter Gerard Gibson
Andrea Giovanni Ledda ... Stefano Del Giacco