Review
Review

Affiliation:
1Immunology Department, Perth Children’s Hospital, Perth 6009, Australia
ORCID: https://orcid.org/0000-0002-2242-3018
Affiliation:
1Immunology Department, Perth Children’s Hospital, Perth 6009, Australia
2Bunbury Hospital, WACHS Southwest, Bunbury 6230, Australia
Affiliation:
1Immunology Department, Perth Children’s Hospital, Perth 6009, Australia
Affiliation:
1Immunology Department, Perth Children’s Hospital, Perth 6009, Australia
3Medical School, University of Western Australia, Perth 6009, Australia
4Immunology Department, PathWest Laboratory Medicine WA, Perth 6009, Australia
5Immunology Department, Sir Charles Gairdner Hospital, Perth 6009, Australia
Email: michaela.lucas@health.wa.gov.au
ORCID: https://orcid.org/0000-0001-8881-9990
Explor Asthma Allergy. 2026;4:1009128 DOI: https://doi.org/10.37349/eaa.2026.1009128
Received: February 27, 2026 Accepted: April 28, 2026 Published: June 07, 2026
Academic Editor: Michele Miraglia Del Giudice, University of Campania, Italy
The article belongs to the special issue Asthma, Allergies, and Respiratory Infections in Pediatric Age
Drug allergies are reported in 10% of children, with non-steroidal anti-inflammatory drugs (NSAIDs) and β-lactam antibiotics being the most frequently implicated; while antibiotic allergy is more commonly reported in early childhood, NSAIDs are the leading cause of confirmed drug hypersensitivity in older children and adolescents. Paracetamol and ibuprofen are widely used in paediatrics for their analgesic, anti-pyretic, and anti-inflammatory effects via their inhibitory action on cyclooxygenase (COX) enzymes. Whilst considered generally safe, hypersensitivity reactions (HSR) to NSAIDs are the leading causes of drug-induced hypersensitivity in children and the most frequent cause of anaphylaxis. NSAID hypersensitivity is classified into immunologic (allergic) and non-immunologic (non-allergic) reactions, typically occurring in selective responders who react to a single NSAID or structurally related group without cross-intolerance. Reactions may be immediate (within one hour with urticaria, angioedema, anaphylaxis), or delayed (hours to days later). Paediatric presentations overlap with adult but pose unique diagnostic and management challenges, compounded by limited paediatric-specific evidence and variable international practice. In 2018, the European Network of Drug Allergy and the European Academy of Allergy and Clinical Immunology published a consensus-based position paper outlining recommendations for diagnosis and management in children and adolescents. A review of 12 recent paediatric studies supports current classification frameworks and reinforces oral provocation testing as the diagnostic gold standard, with prospective study designs and multicentre recruitment that enhance validity and generalisability, highlighting that cutaneous symptoms were the most common presentation and supervised graded drug challenges shown to be safe and clinically informative. Despite these advances, significant global variability persists, and current approaches are still largely guided by expert consensus rather than robust, standardised evidence. This highlights the need for internationally harmonised guidelines, large prospective studies, improved risk stratification, and the development of reliable adjunctive diagnostic tools, particularly given the limited utility and validation of skin testing in this population.
Drug allergies are reported in almost 10% of children, with allergies to non-steroidal anti-inflammatory drugs (NSAIDs) and β-lactam antibiotics being the most common [1]. Whilst antibiotics remain the most frequently reported allergy in very young children, NSAIDs have been reported as the most common drug allergy for children and adolescents combined [2]. Although NSAIDs are widely used, the range of agents approved for paediatric use is relatively limited compared with adults—for example, aspirin (ASA), which is contraindicated in children under 12 due to the risk of Reye’s syndrome. Consequently, paracetamol and ibuprofen remain the most prescribed medications in this population. These drugs exert analgesic, antipyretic, and anti-inflammatory effects through inhibition of cyclooxygenase (COX) enzymes. While generally considered safe, NSAIDs are also recognised as a leading cause of drug-induced anaphylaxis in both children and adults [3].
Non-steroidal anti-inflammatory drug reaction profiles can differ between children of different ages [4]. Younger children are more likely to present with cutaneous reactions, whereas adolescents and adults are more likely to experience anaphylaxis [5]. Hypersensitivity reactions (HSR) typically occur in the paediatric population, where medications like NSAIDs are often recommended in the context of viral or febrile illnesses. Such illnesses can involve similar clinical symptomatology to allergies, such as urticarial rashes, angioedema, wheeze, cough, and coryza [3, 6], which can lead to misdiagnoses of allergies and anaphylaxis. In addition, available diagnostic investigations are often difficult to access, underutilized, or interpreted inconsistently.
NSAIDs can be classified into different chemical groups or pharmacologically by their inhibition of COX enzymes, comprising COX-1 and COX-2 primarily, as well as COX-3 (Table 1). COX enzymes are involved in physiological and regulatory pathways and signalling processes across multiple tissue types, including pro-inflammatory reactions through the production of prostaglandins, prostacyclin, and thromboxane A2 from arachidonic acid. NSAIDs, therefore, have anti-inflammatory effects by inhibiting the activation of COX enzymes, and therefore the activation of the arachidonic acid pathway [7].
NSAID action on cyclooxygenase (COX) enzymes.
| Type of action | Type of NSAID |
|---|---|
| Full COX-1 and COX-2 inhibition (non-selective) | Aspirin (ASA), diclofenac, naproxen, ketoprofen, indomethacin, piroxicam, sulindac, ibuprofen, ketorolac |
| Preferential COX-2, partial COX-1 inhibition | Etodolac, meloxicam, nimesulide, nabumetone, tolmetin |
| Selective COX-2, weak COX-1 inhibition | Rofecoxib, etoricoxib, valdecoxib, celecoxib, lumiracoxib |
| Weak COX-1, weak COX-2 inhibition | 5-ASA, paracetamol, diflunisal, sulfasalazine |
NSAID: non-steroidal anti-inflammatory drug.
Ibuprofen and paracetamol are both classified as NSAIDs based on their chemical structure and inhibition of COX enzymes. Ibuprofen is a propionic acid derivative, along with other NSAIDs such as naproxen and ketoprofen, and acts as a non-selective inhibitor of COX-1 and COX-2 enzymes [4]. It has particularly strong COX-1 inhibition. Paracetamol is of the para-aminophenol group, with preferential action on COX-2 at low doses. At high doses, it may exert weak partial inhibition of COX-1 [8].
NSAID hypersensitivity can be characterised into two types, allergic (immunologic) and non-allergic (non-immunologic), depending on the underlying mechanism [9]. Immunologic reactions occur primarily in the setting of selective responders (SR), where patients react to a single NSAID or a single chemical group of NSAIDs. These are regarded as non-cross-intolerant reactions and may be immediate or non-immediate. Immediate reactions present as urticaria, angioedema, and/or anaphylaxis, occurring within minutes up to one hour post-ingestion of the NSAID. Non-immediate delayed reactions such as toxic epidermal necrolysis and Stevens-Johnson syndrome (SJS/TEN), drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, and acute generalised exanthematous pustulosis (AGEP) occur more than 24 h post exposure (Tables 2 and 3). Both these processes reflect IgE-mediated (Figure 1), and T-cell-mediated hypersensitivity, and therefore, non-chemically related NSAIDs are usually well tolerated [4, 9].
Classification of non-allergic vs. allergic non-steroidal anti-inflammatory hypersensitivity—paediatric population < 10 years.
| Characteristic | Reaction type | ||
|---|---|---|---|
| Non-immunological NSAID hypersensitivity (NERD/NECD/NIUA) | Selective immediate NSAID allergy [selective NSAID-induced urticaria, angioedema, or anaphylaxis (SNIUAA)] | Selective delayed NSAID hypersensitivity (SNIDR) | |
| Clinical features | Cutaneous (urticaria/angioedema), respiratory, ocular, or systemic symptoms, including anaphylaxis | Acute urticaria, angioedema, or anaphylaxis to a single agent | Heterogeneous, including fixed drug eruptions and severe cutaneous reactions (e.g., SJS/TEN) |
| Onset | Typically, within minutes to a few hours | Usually within 1 h | Delayed onset, generally beyond 24 h |
| Mechanism | Non-allergic mechanism due to COX-1 inhibition | IgE-mediated hypersensitivity | T-cell-driven immune response |
| Cross-reactivity | Present across structurally unrelated NSAIDs | Absent | Absent |
| Associated factors | Patients with asthma, chronic rhinosinusitis, or chronic urticaria | Unknown | Unknown |
COX: cyclooxygenase; NECD: NSAID-exacerbated cutaneous disease; NERD: NSAID-exacerbated respiratory disease; NIUA: NSAID-induced urticaria/angioedema; SJS: Stevens-Johnson syndrome; SNIDR: selective NSAID-induced delayed reactions; TEN: toxic epidermal necrolysis; NSAID: non-steroidal anti-inflammatory drug.
Classification of non-allergic vs. allergic non-steroidal anti-inflammatory hypersensitivity—adolescent population > 10 years.
| Characteristic | Reaction type | ||||
|---|---|---|---|---|---|
| Non-allergic NSAID-exacerbated respiratory disease (NERD) | NSAID-exacerbated cutaneous disease (NECD) | NSAID-induced urticaria/angioedema/anaphylaxis (NIUAA) | Allergic selective NSAID-induced urticaria, angioedema, or anaphylaxis (SNIUAA) | Allergic selective NSAID-induced delayed reactions (SNIDR) | |
| Clinical features | Respiratory (bronchospasm, dyspnoea, nasal congestion, rhinorrhoea) | Cutaneous (urticaria and/or angioedema) | Urticaria and/or angioedema ± respiratory symptoms | Urticaria, angioedema, anaphylaxis | Cutaneous and mucosal eruptions (maculo-papular, fixed drug eruption); severe cutaneous reactions (AGEP, DRESS, SJS/TEN); organ-specific manifestations (hepatitis, nephritis) |
| Onset | Immediate (minutes–hours) | Immediate (minutes–hours) | Immediate (minutes–hours) | Immediate (< 1 h) | Delayed (> 24 h) |
| Mechanism | Non-allergic mechanism due to COX-1 inhibition | Non-allergic mechanism due to COX-1 inhibition | Non-allergic mechanism due to COX-1 inhibition | IgE-mediated | T-cell mediated |
| Cross-reactivity | Present across structurally unrelated NSAIDs | Present across structurally unrelated NSAIDs | Present across structurally unrelated NSAIDs | Absent | Absent |
| Associated factors | Patients with asthma, chronic rhinosinusitis, or chronic urticaria | Chronic urticaria | Unknown | Unknown | Unknown |
COX: cyclooxygenase; SJS: Stevens-Johnson syndrome; TEN: toxic epidermal necrolysis; AGEP: acute generalised exanthematous pustulosis; DRESS: drug reaction with eosinophilia and systemic symptoms; NSAID: non-steroidal anti-inflammatory drug.
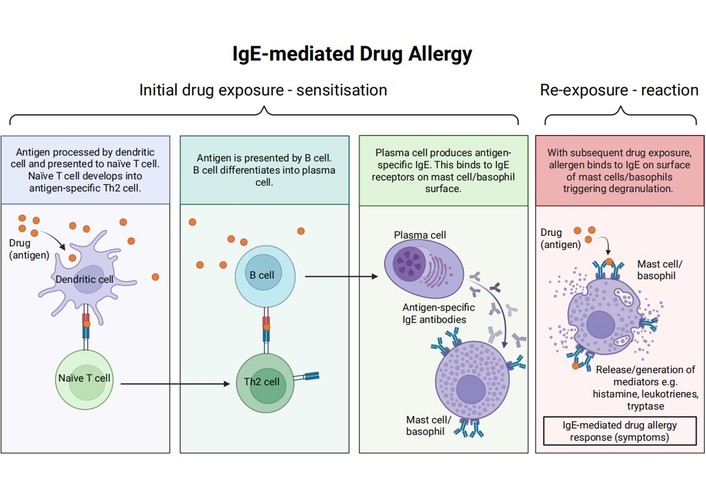
IgE-mediated allergic response. Created in BioRender. Lucas, M. (2026) https://BioRender.com/almimaw.
Non-immunologic reactions are usually characterised by the presence of cross-intolerance (CI) across different NSAID classes. These processes are caused physiologically by COX-1 inhibition and reduced prostaglandin E2 (PGE2) production, leading to an increased release of leukotrienes (Figure 2). Clinical features include urticaria, angioedema, and respiratory complications (Tables 2 and 3) [4, 5].
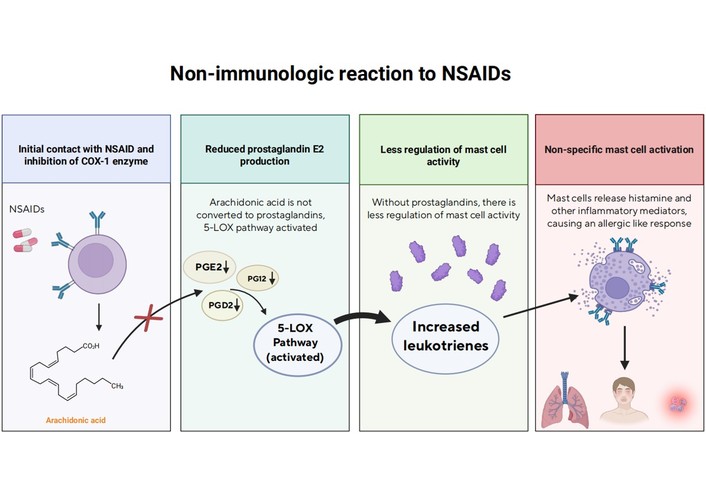
Non-immunologic response. Created in BioRender. Lucas, M. (2026) https://BioRender.com/k7vlxlu.
Both non-allergic and allergic reactions are classified according to the European Network of Drug Allergy (ENDA) as follows: NSAID-induced urticaria, angioedema, or anaphylaxis (NIUAA); NSAID-exacerbated respiratory disease (NERD); NSAID-exacerbated cutaneous disease (NECD); selective NIUAA (SNIUAA); and selective NSAID-induced delayed reactions (SNIDR) [2]. However, it is reported that this classification alone is not well adapted for children [10], and a modified version is presented in Tables 2 and 3.
There is a lack of knowledge on HSR to NSAIDs in children with regard to epidemiology, clinical spectrum, and appropriate diagnostic methods [11]. Therefore, a more extensive investigation into the safety and efficacy of drug provocation testing (DPT) in children is needed. In particular, specific testing protocols and use of alternative medications such as ASA and celecoxib, as well as defined management options for those confirmed to have NSAID-induced HSRs, are warranted [3].
Despite the widespread use of NSAIDs in children, there remains limited knowledge regarding NSAID-induced HSR in this age group. While broadly comparable to those seen in adults, NSAID-induced HSR in children presents distinct diagnostic and management challenges and has historically lacked international consensus. In 2018, the ENDA, in collaboration with the European Academy of Allergy and Clinical Immunology (EAACI), published a position paper outlining the diagnosis and management of NSAID hypersensitivity in children and adolescents, based on available evidence and expert opinion [2].
Classifying drug hypersensitivity as either selective reactions to a specific NSAID (potentially immune-mediated) or CI reactions to multiple NSAIDs via non-immunologic mechanisms (e.g., COX-1 inhibition) is a critical step for appropriate patient testing and management. In the paediatric population, however, this process is further complicated by co-factors such as intercurrent infection, exercise, and age-related differences in drug metabolism. To address these challenges, a more detailed age-stratified classification was developed for children under ten years and adolescents aged 10–19 years (Tables 2 and 3). A simplified classification was applied to younger children, while a more detailed framework, adapted from adult recommendations, was used for older children and adolescents. This approach reflects the predominance of non-immunologic, cross-intolerant reactions with significant co-factors in younger children, whereas reactions in older children and adolescents increasingly resemble adult patterns, albeit with a sufficiently high frequency of anaphylaxis to warrant modification of existing adult classifications. This revised framework aims to support more accurate diagnosis and optimal management of NSAID hypersensitivity in children [2].
The EAACI/ENDA position paper highlights that diagnosis of NSAID hypersensitivity in children is primarily based on a detailed clinical history, including the culprit drug(s), timing and nature of symptoms, involvement of single or multiple NSAIDs, prior tolerance, and relevant co-factors such as intercurrent infection, exercise, and fever. Because these co-factors frequently confound diagnosis in children, accurate classification into selective NSAID hypersensitivity or CI reactions is essential to guide appropriate investigation and management.
DPT is the gold standard for confirming NSAID hypersensitivity in children and adolescents and for distinguishing between selective and cross-intolerant reactions, as well as identifying safe alternative antipyretic and analgesic options. Skin testing has a very limited role and is recommended only in selected cases of suspected immediate selective hypersensitivity, while in vitro tests are not validated and are not recommended for routine use. DPT should be performed in a specialist setting with appropriate monitoring and emergency preparedness, and ideally when confounding factors such as acute infection have resolved. This approach aims to minimise misdiagnosis, avoid unnecessary NSAID avoidance, and support safe, evidence-based management of children with suspected NSAID hypersensitivity.
HSR to NSAIDs in children remain a complex and clinically significant challenge. Across the reviewed literature detailed in Table 4, there is a consistent emphasis on the heterogeneity of paediatric NSAID reactions and the need for careful, evidence-based evaluation. The EAACI/ENDA 2018 position paper represents the first comprehensive consensus statement specifically tailored to children and adolescents, consolidating prior observational, clinical, and interventional studies into standardised guidance.
Current paediatric literature regarding NSAID hypersensitivity and assessment.
| Author, year, and country | Study design | Sample size/participants/age | Type of reported allergic adverse-drug-like reaction | Key results |
|---|---|---|---|---|
| Arikoglu et al. [25], 2024, Turkey | Prospective observational study of patients with a history of NSAID-H reactions using a standardized diagnostic protocol according to EAACI/ENDA recommendations. Comparison of EAACI 2013 and paediatric EAACI/ENDA 2028 classification | 232 patients (4–11 years). Children with a history of nonsteroidal anti-inflammatory drug HSR | Primarily cutaneous (urticaria, angioedema), some respiratory reactions (mild-moderate), no anaphylaxis. |
|
| Dogan et al. [12], 2024, Turkey | Observational retrospective clinical evaluation using ENDA/EAACI classification and drug provocation testings (DPTs) | 67 children with suspected NSAID hypersensitivity (age categories < 10 and > 10 included) | NSAID-H confirmed HSR: mainly NSAID-induced urticaria/angioedema (NIUA); classification into cross-intolerant and selective responders based on DPT outcomes |
|
| Aytekin Güvenir et al. [16], 2024, Turkey | Retrospective observational study; OPT/DPT with alternative drugs stratified by phenotype | 91 patients underwent testing with 109 alternative drugs, median age 15 years (Jan 2015–Feb 2023) | NSAID-H reactions, primarily cutaneous reactions (urticaria, angioedema), and less commonly GIT reactions (nausea). |
|
| Hadley et al. [19], 2023, United States | Cross-sectional survey-based study | 100 paediatric patients with severe asthma, aged 6–18 years | Reported history of NSAID hypersensitivity based on survey (self-reported reactions to NSAIDs) |
|
| Li et al. [15], 2022, USA | Retrospective observational cohort study of outpatient two-step NSAID challenge procedures | 249 patients with reported NSAID allergy (mean age 51.6 years, range 5–87; 63.5% female) undergoing 262 two-step NSAID challenges; individuals with aspirin-exacerbated respiratory disease were excluded | HSR during challenge: immediate reactions (within ~3 h) and delayed reactions following a two-step NSAID challenge protocol |
|
| Metbulut et al. [20], 2025, Turkey | Multicentre retrospective study | 265 children with 293 drug-related anaphylactic episodes; ages 1 month to 18 years (median 107 months) | Drug-related anaphylaxis (including NSAIDs, antibiotics, others) |
|
| González Moreno et al. [22], 2025, Spain | Mixed retrospective and prospective observational study; retrospective focus on patients < 18 years old with cross-intolerance to NSAIDs through DPT 1999–2019, prospective reassessment in 2021–2022 in visit 2 | 46 children aged 1–17 years with confirmed cross-intolerance | Primarily cutaneous (urticaria, angioedema), some respiratory symptoms (bronchorrhea, bronchospasm) |
|
| Mori et al. [17], 2020; multicentre European (Belgrade, Florence, Geneva, Madrid, Porto, Rome) | Multicentre retrospective study | 693 children with a history of NSAID reactions; ages 0–18 years; 526 drug provocation tests performed | HSR to NSAIDs in paediatric patients |
|
| Podlecka et al. [13], 2023, Poland | Observational clinical diagnostic study with drug challenge tests (oral provocation) in children | 56 children aged 4–18 years referred for suspected drug allergy to NSAIDs; skin prick tests and provocation tests performed | NSAID HSR: acute urticaria and angioedema; immediate (≤ 1 h) and delayed/late reactions (after 1 h) following NSAID |
|
| Tekcan et al. [23], 2025, Turkey | Retrospective, observational study of patients with a history of NSAID and paracetamol hypersensitivity, comparing NPV of single vs. 2-day DPTs for NSAID and paracetamol hypersensitivity | 104 patients—53.8% boys, age 1–18 | Rash, gastrointestinal symptoms, respiratory symptoms with angioedema |
|
| Uluc et al. [24], 2025, Turkey | Prospective study evaluating the development of tolerance in children with a confirmed diagnosis of NSAID-H | 34 cases confirmed NSAID-H, 23 (67.65%) were included in study. Median age 16.5 (last DPT). Tolerance was developed in 12/23 (52.1%). Median duration to tolerance development: 6.16 years. | Urticaria most common symptom at DPT in the tolerant group. In the persistent group, reactions occurred at significantly lower cumulative doses |
|
| Yilmaz Topal et al. [14], 2020, Turkey | Retrospective observational diagnostic study with oral DPT in children | 243 patients with suspected NSAID-H (median age ~84 months; including both < 10 years and older children) were evaluated with 238 provocation tests | HSR to NSAIDs with mainly isolated skin manifestations (e.g., urticaria/angioedema); classified according to the EAACI position paper; classification |
|
HSR: hypersensitivity reactions; NSAID: non-steroidal anti-inflammatory drug.
Comparison of these recent studies with the EAACI/ENDA recommendations reveals common themes as outlined in Table 4. Dogan et al. [12] (2024) and Podlecka et al. [13] (2023) both highlighted the limited reliability of clinical history alone for diagnosis, reinforcing the critical role of oral provocation testing, a principle central to the EAACI/ENDA consensus, which endorses stepwise, controlled drug challenges as the diagnostic gold standard. Similarly, Yilmaz Topal et al. [14] (2020) noted limitations in current paediatric classification systems, with some children exhibiting atypical reactions that do not clearly fit into CI or selective hypersensitivity categories. The EAACI/ENDA framework responds to these challenges by advocating an individualised diagnostic approach, emphasising careful interpretation of provocation test results within the context of paediatric physiology and comorbid conditions.
Evidence supports the safety and utility of structured outpatient NSAID challenge protocols in children. Li et al. [15] (2022) confirmed that graded challenges can be safely conducted under clinical supervision, aligning with EAACI/ENDA recommendations. Observational studies, including Aytekin Güvenir et al. [16] (2024), provide epidemiological context, demonstrating that cutaneous reactions, particularly urticaria and angioedema, are the most frequent manifestations, while respiratory and systemic symptoms, though less common, remain clinically important. These findings reinforce the EAACI/ENDA classification of paediatric NSAID hypersensitivity phenotypes and inform practical risk stratification and individualised management.
Across multiple prospective and retrospective studies (Dogan et al. [12], 2024; Li et al. [15], 2022; Mori et al. [17], 2020), systematic evaluation using detailed histories, oral provocation tests, and risk stratification confirms the feasibility and safety of supervised challenge protocols, supporting the position paper’s recommendation for structured assessment. Graded outpatient challenges, in particular, have proven safe and effective in identifying true hypersensitivity, minimising unnecessary drug avoidance. This is further supported by Aytekin Güvenir et al. [16] (2024), who demonstrated that alternative NSAID and non-NSAID provocation testing can be safely performed in children with confirmed hypersensitivity, reinforcing the importance of structured testing not only for diagnosis but also for guiding safe therapeutic alternatives.
Reaction patterns largely align with EAACI/ENDA phenotypes: cutaneous manifestations, including urticaria and angioedema, predominate, while respiratory and systemic reactions are less frequent but clinically relevant [18–20]. Several studies underscore co-factors influencing reaction presentation, including infections and severe asthma [19]. Whilst the role of NSAIDs as the causal pathogenesis in children remains unclear, it is understood that use in children may lead to asthma exacerbations [21]. In addition, the recognition of NSAID-exacerbated food allergy (NEFA) and NSAID-induced food allergy (NIFA) refines the original EAACI/ENDA classification and highlights that some apparent NSAID reactions may be co-factor-dependent rather than true drug hypersensitivity.
Multicentre data by Mori et al. [17] (2020) and Metbulut et al. [20] (2025) provide epidemiological validation, showing that cross-reactive reactions are more common than selective hypersensitivity and underscoring the importance of precise phenotyping for clinical management. Observational and review studies by Podlecka et al. [13] (2023) and Yilmaz Topal et al. [14] (2020) illustrate challenges in classification due to variable co-factors and atypical presentations, suggesting that misdiagnosis or over-reporting of NSAID allergy remains a concern. Extending this, González Moreno et al. [22] (2025) provided longitudinal evidence suggesting that some children with cross-intolerant NSAID hypersensitivity may develop tolerance over time, highlighting the need for follow-up reassessment and selective re-challenge in clinical practice.
Tekcan et al. [23] (2025) showed that single-day and two-day provocation protocols have comparable diagnostic accuracy in paediatric NSAID hypersensitivity, supporting EAACI/ENDA recommendations for standardised DPT while suggesting that shorter protocols may be suitable in carefully selected low-risk patients. Uluc et al. [24] (2025) further extended these findings by demonstrating that age may influence both reaction phenotype and the development of tolerance, indicating that incorporating age stratification could improve diagnostic precision and risk assessment. In addition, Arikoglu et al. [25] (2024) identified limitations in current classification approaches and proposed that children with underlying allergic disease may represent a distinct subgroup, reinforcing EAACI/ENDA phenotypes while highlighting the need for further refinement of diagnostic pathways in atopic paediatric populations. However, these studies are limited by relatively small sample sizes, heterogeneous patient populations, and predominantly single- or limited-centre designs, which may restrict generalisability. In addition, variability in provocation protocols and outcome definitions limits direct comparison between studies and underscores the need for larger, standardised multicentre prospective research.
Collectively, these studies reinforce the EAACI/ENDA framework while contributing important refinements, as outlined in Table 5:
Comparison of paediatric NSAID hypersensitivity studies to EAACI/ENDA 2018 consensus.
| Study | Study design & population | Alignment with EAACI/ENDA 2018 | Notes/Contributions |
|---|---|---|---|
| Dogan et al. [12], 2024—Assessment of paediatric patients with suspected NSAID hypersensitivity | Prospective assessment of children referred for suspected NSAID reactions: detailed history, skin testing, and oral challenge | Supports EAACI/ENDA recommendation for systematic evaluation and controlled drug challenges; reinforces phenotype classification | Adds recent real-world data on the prevalence of true NSAID hypersensitivity in children |
| Podlecka et al. [13], 2023—Practical approach to NSAID hypersensitivity in children | Narrative review/expert opinion on paediatric NSAID reactions | Directly aligns with EAACI/ENDA guidance for structured assessment | Useful as practical guidance for clinicians; emphasises outpatient safety |
| Yilmaz Topal et al. [14], 2020—Results of NSAID provocation tests and classification challenges | Retrospective cohort of children undergoing oral provocation tests | Highlights limitations noted in EAACI/ENDA 2018 regarding classification and co-factors | Provides data supporting careful interpretation of drug challenges and phenotype assignment |
| Li et al. [15], 2022—Safety, outcomes, and recommendations for two-step outpatient NSAID challenges | Prospective outpatient two-step challenge in children | Reinforces EAACI/ENDA recommendation for supervised graded challenges | Strengthens evidence for outpatient risk stratification and procedural safety |
| Aytekin Güvenir et al. [16], 2024—Alternative drug safety in children with nonsteroidal anti-inflammatory drug hypersensitivity | Observational study; children with confirmed NSAID hypersensitivity undergoing alternative drug provocation | Strong alignment with guideline emphasis on drug provocation testing (DPT) as the gold standard and identification of safe alternatives | Supports safety of paracetamol and selective COX-2 inhibitors; reinforces the need for individualized testing rather than assumption of cross-reactivity |
| Mori et al. [17], 2020—Multicentre retrospective study, ENDA group | Multicentre retrospective European cohort of children | Directly validates EAACI/ENDA classification (cross-reactive vs. selective) | Offers multicentre evidence supporting the international applicability of classification |
| Hadley et al. [19], 2023—NSAID hypersensitivity in severe paediatric asthma | Observational cohort of children with severe asthma | Aligns with EAACI/ENDA risk stratification recommendations; highlights asthma as a co-factor | Supports tailored assessment in high-risk subgroups |
| Metbulut et al. [20], 2025—Evaluation of drug-related anaphylaxis in children | Multicentre retrospective anaphylaxis registry | Reinforces EAACI/ENDA emphasis on severe reaction recognition | Provides data on severe outcomes, informing emergency preparedness and management |
| González Moreno et al. [22], 2025—Natural history of cross intolerance to NSAIDs in the paediatric population | Longitudinal cohort; paediatric patients with CI followed over time | Aligns with the classification of cross-intolerant phenotypes (CI) but extends beyond the guidelines by examining natural history | Demonstrates that some children may outgrow CI, which is not well addressed in EAACI/ENDA 2018; adds prognostic insight |
| Tekcan et al. [23], 2025—Comparison of negative predictive values of single- and two-day provocation tests with suspected nonsteroidal anti-inflammatory drug and paracetamol allergy in children | Diagnostic accuracy study; children undergoing 1-day vs. 2-day DPT for NSAIDs/paracetamol | Strong alignment with the recommendation for DPT to confirm/exclude hypersensitivity | Suggests shorter (1-day) protocols may be sufficient in many cases; contributes to optimizing and standardizing testing protocols |
| Uluc et al. [24], 2025—Evaluation of nonsteroidal anti-inflammatory drug hypersensitivity in children: is age the crucial factor? | Observational cohort; evaluates NSAID tolerance across different paediatric age groups | Partially aligned; supports guideline focus on individual variability, but introduces age as a modifying factor not emphasized in the 2018 paper | Suggests younger children may have higher tolerance or different phenotypes; proposes an age-stratified approach to evaluation |
| Arikoglu et al. [25], 2024—Alternative drug safety in children with nonsteroidal anti-inflammatory drug hypersensitivity. | Comparative study of classification protocols in children with NSAID hypersensitivity | Challenges: strict application of EAACI/ENDA classification; proposes refinement of phenotypes | Highlights that children with underlying atopy/asthma may represent a distinct subgroup; suggests the need to adapt adult-derived classifications for paediatrics |
CI: cross-intolerance; COX: cyclooxygenase; NSAID: non-steroidal anti-inflammatory drug.
Confirmation of the safety and practicality of outpatient graded challenges.
Reinforcement of phenotype-based classification with epidemiological support.
Identification of co-factors (asthma, infection, food) influencing reaction severity and phenotype.
Emphasis on individualised risk stratification and tailored management in paediatric populations.
Therefore, recent literature closely aligns with the EAACI/ENDA 2018 position paper, providing both empirical validation and clinically relevant refinements, particularly regarding co-factor-dependent reactions and high-risk subgroups such as children with severe asthma or multisystem reactions. These insights guide safe diagnostic pathways, rational NSAID use, and precision risk assessment in paediatric practice. Overall, the body of literature preceding 2018 offers robust observational and interventional evidence on prevalence, phenotypes, risk factors, and diagnostic strategies in paediatric NSAID hypersensitivity, which the EAACI/ENDA position paper synthesizes into a standardised, child-specific framework. The alignment between individual study findings and the position paper underscores the critical importance of evidence-informed, age-specific approaches to the evaluation and management of NSAID hypersensitivity in children and adolescents.
Building on the EAACI/ENDA consensus and supported by recent studies, ibuprofen has been identified as the most common cause of HSR among NSAIDs in children. These reactions can be either selective, occurring in response to a single drug, or cross-reactive, mediated through COX-1 inhibition. Accurate diagnosis is therefore critical, particularly because options for alternative treatment, such as selective COX-2 inhibitors, remain limited in younger age groups. At present, definitive diagnosis relies on DPT, which has been shown to reliably confirm true allergy and predict the risk of reactions upon re-exposure. However, DPT is resource-intensive and carries a measurable risk of inducing adverse reactions. To address these challenges, Stehlin et al. [26] (2025) conducted a study to validate a clinical risk stratification tool designed to predict the likelihood of a positive DPT in children with suspected ibuprofen hypersensitivity, potentially allowing for more targeted and safer diagnostic approaches.
The I3A risk-stratification tool, developed by Stehlin et al. [26] (2025), is a simple clinical scoring system designed to predict the likelihood of a positive DPT in children with suspected ibuprofen hypersensitivity. It assigns points based on three factors from the initial reaction: angioedema (2 points), anaphylaxis (1 point), and age ≥ 10 years (1 point), yielding a maximum score of 4. Children scoring 0–2 are considered low-risk, with a high negative predictive value, while those scoring 3–4 are high-risk, having a markedly increased probability of a positive DPT. By identifying children at higher or lower risk, the tool aims to help clinicians plan DPTs more safely and efficiently. Within their cohort of 82 children, the relative risk of reacting to a challenge in the I3A group scoring 3–4 compared with 0–2 was 11.4 (p < 0.001). Anaphylaxis after DPT was observed in 9/25 (36.0%) in the high-risk group compared with 2/52 (3.8%) in the low-risk group [26]. The tool therefore provides a practical method to improve risk stratification and support safer, more targeted use of DPT in paediatric patients.
Drug HSR are complex, and accurate diagnosis requires thorough evaluation. Current in vitro biomarkers, such as specific IgE, tryptase, and certain HLA-DR genotyping, are often drug-specific and thus are not widely used or consistently reliable for NSAID hypersensitivity. Despite recent advances, available biomarkers remain limited due to challenges in analytical or clinical validation and are often not easily accessible. One study, however, has identified genetic variants in the vitamin D pathway, retinoid receptors, and the high-affinity IgE receptor as being associated with NSAID hypersensitivity risk. Furthermore, correlations between IgE levels and clinical features suggest that IgE may help explain these reactions and could aid in patient stratification [27]. Nonetheless, further multicentre studies are needed to validate these findings and support their clinical application.
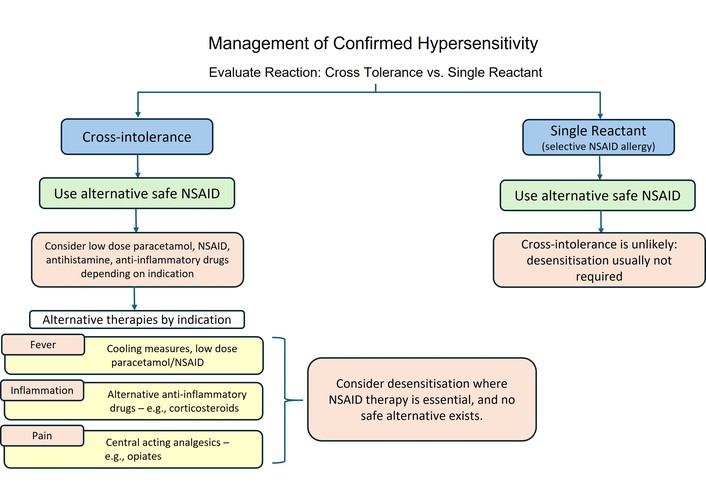
Once NSAID hypersensitivity has been confirmed, it is important to classify the underlying mechanism of the reaction as either a selective reaction or a cross-reactive pattern. This distinction is clinically significant, as patients with selective hypersensitivity may be able to tolerate alternative NSAIDs, and clinicians should follow an algorithm such as the one detailed in Figure 3. Regardless of the classification, patients and caregivers should be provided with both verbal and written guidance outlining medications to avoid and safe alternative options, including specific formulations and appropriate dosing [2]. However, it is important to acknowledge that therapeutic options are more limited in childhood. Consequently, reassessment during adolescence or early adulthood is recommended, with ongoing education essential to explore broader treatment possibilities, appropriate for adulthood, to determine which medications may be safely used or should continue to be avoided.
However, in patients with cross-intolerant NSAID hypersensitivity, safe alternative agents within the NSAID class cannot be reliably identified. Although COX-2 selective inhibitors, such as celecoxib, have been evaluated in adult populations, their use in children remains limited and is not universally approved worldwide [2]. Management must therefore focus on treating individual clinical indications, such as pain, pyrexia, and inflammation, using non-NSAID options. Paracetamol may be considered for analgesia and antipyresis, while corticosteroids represent a suitable alternative for anti-inflammatory purposes. Opiates are approved for use in young children, primarily for the management of moderate to severe pain, particularly in post-operative settings; however, they do not possess antipyretic or anti-inflammatory properties and are associated with a higher risk of adverse effects [2].
Despite clear evidence of NSAID hypersensitivity in children and adolescents, and a predominance of cross-reactive over selective reactions, there are scarce data in relation to desensitisation of NSAIDs such as paracetamol, ibuprofen, and ASA in children. Whilst the need for desensitisation with ASA is rare in young children, it is indicated in cardiac conditions such as Kawasaki disease, with a lack of published data, use of adult protocols that have been adjusted for weight and age are currently indicated [2].
It is widely documented that NSAIDs are the second most common cause of hypersensitivity in children. Although penicillin is generally regarded as the most common culprit for drug allergies in children, confirmed penicillin allergy occurs in less than 10% of cases, whereas confirmed NSAID allergy affects approximately 30% of children labelled with both selective and cross-intolerant NSAID hypersensitivity [12]. This highlights the importance of accurate diagnostic evaluation and careful management of confirmed NSAID hypersensitivity to minimise the risk of future reactions and guide safe therapeutic choices. Studies related to NSAID hypersensitivity in children are limited. Within this review, we have examined 12 recent studies that have addressed this issue and aligned them with the guidelines outlined in the EAACI/ENDA position paper [2]. Collectively, these studies reinforce the evidence base underpinning the 2018 consensus, particularly supporting the central role of oral provocation testing as the diagnostic gold standard. Methodological strengths, including prospective study designs and multicentre cohorts, enhance both the validity and generalisability of findings. Across studies, there is consistent confirmation of the predominance of cutaneous manifestations and the safety of supervised graded drug challenges [12, 15, 17, 20].
Furthermore, recent research has contributed to the refinement of classification, including the identification of co-factor-dependent reactions and recognition of higher-risk subgroups, such as children with severe asthma [19]. However, there is a need for global consensus guidelines to standardise care and reduce uncertainty, which should be based on evidence rather than solely expert opinion. Structured methods such as the Delphi methodology, which uses iterative surveys among experts to achieve a consensus on best practice, or may follow an established framework such as AGREE II (Appraisal of Guidelines for Research and Evaluation), which provides criteria for guidelines ensuring they are transparent, rigorously developed, and clinically useful.
The retrospective studies consistently demonstrate that both detailed clinical history and oral provocation testing are essential for establishing an accurate diagnosis. They further emphasise that NSAID hypersensitivity represents a significant diagnostic challenge in paediatric populations, largely due to the presence of nonspecific and clinically indistinguishable symptoms within patient histories, as well as overlapping clinical features that complicate classification [13, 14, 18]. However, the retrospective design of these studies introduces limitations, including susceptibility to recall and selection bias. Additionally, variability in provocation protocols and differences in population characteristics restrict direct comparability between studies, while important co-factors, such as intercurrent infection or concurrent food exposure, were not consistently assessed.
More recently, the I3A risk-stratification tool provides a practical and evidence-based method to identify children at higher risk of reacting during ibuprofen DPT. Incorporating key clinical features from the initial reaction, it enables improved risk stratification, supports safer challenge planning, and may help prioritise testing in appropriate patients while minimising the risk of severe reactions [26]. In addition, data is emerging that there is evidence to suggest that IgE-mediated NSAID-induced urticaria/angioedema (NIUA) can experience a loss of hypersensitivity over time; there is limited data on non-immunological reactions. One study addressed this issue in adults and found that NIUA patients may develop tolerance over time, but this was also influenced by atopy and the type of clinical reaction [28–30]. Emerging paediatric data suggest that this also occurs in children. Recent evidence indicates that a proportion of children with NSAID hypersensitivity may outgrow their reactivity, although again influenced by atopic history, supporting the concept that the natural history in paediatric populations may parallel, at least in part, that observed in adults. These findings highlight the importance of periodic re-evaluation and consideration of repeat oral provocation testing in selected cases to avoid unnecessary long-term drug avoidance [22].
From a clinical perspective, these findings support a structured and proactive approach to management. Early referral to specialist allergy services is essential for children with suspected NSAID hypersensitivity, given the high rate of misclassification based on clinical history alone. Where appropriate, risk-stratified oral provocation testing should be undertaken to confirm or exclude the diagnosis and to identify safe alternative medications. Management should be individualised, with consideration of tolerated agents such as paracetamol or selective COX-2 inhibitors to minimise unnecessary treatment restriction and improve patient care.
Overall, this review demonstrates that there is currently a global variation in how paediatric NSAID hypersensitivity is classified, diagnosed, and managed across clinical practice. Future research should focus on the development of standardised, paediatric-specific diagnostic and classification frameworks that incorporate factors such as age, atopy, and co-factor-dependent mechanisms. Large, multicentre prospective studies using harmonised protocols are needed to improve comparability and refine risk stratification. Further investigation into the natural history of both selective and cross-intolerant reactions is essential, particularly to identify predictors of tolerance development. In parallel, the identification and validation of reliable in vitro biomarkers or adjunctive diagnostic tools remains a key unmet need. International collaboration will be crucial to develop consensus guidelines using robust methodological frameworks, such as Delphi methodology and AGREE II, ensuring recommendations are transparent, evidence-based, and widely applicable.
Ultimately, improving diagnostic accuracy and standardising management pathways in paediatric NSAID hypersensitivity will reduce unnecessary drug avoidance, optimise treatment options, and enhance patient safety.
AGEP: acute generalised exanthematous pustulosis
ASA: aspirin
CI: cross-intolerance
COX: cyclooxygenase
DPT: drug provocation testing
DRESS: drug reaction with eosinophilia and systemic symptoms
EAACI: European Academy of Allergy and Clinical Immunology
ENDA: European Network of Drug Allergy
HSR: hypersensitivity reactions
NECD: non-steroidal anti-inflammatory drugs-exacerbated cutaneous disease
NERD: non-steroidal anti-inflammatory drugs-exacerbated respiratory disease
NIUA: non-steroidal anti-inflammatory drugs-induced urticaria/angioedema
NIUAA: non-steroidal anti-inflammatory drugs-induced urticaria, angioedema, or anaphylaxis
NSAIDs: non-steroidal anti-inflammatory drugs
SJS: Stevens-Johnson syndrome
SNIDR: selective non-steroidal anti-inflammatory drug-induced delayed reactions
SNIUAA: selective non-steroidal anti-inflammatory drug-induced urticaria, angioedema, or anaphylaxis
TEN: toxic epidermal necrolysis
AA: Conceptualization, Visualization, Data curation, Formal analysis, Methodology, Writing—original draft, Writing—review & editing. CB: Conceptualization, Data curation, Writing—original draft, Writing—review & editing. KD: Writing—review & editing. ML: Conceptualization, Visualization, Writing—review & editing, Methodology, Supervision. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 2304
Download: 60
Times Cited: 0
Cristiana Indolfi ... Michele Miraglia del Giudice
Sonila Borici ... Ilir Akshija
Malik Sallam ... Mohammed Sallam
Alberto Vidal, Pedro Cortez