 Short Communication
Short Communication

Affiliation:
1UOSD Allergologia e Immunologia Clinica, Dipartimento Scienze Mediche e Chirurgiche Addominali ed Endocrino Metaboliche, Fondazione Policlinico A. Gemelli, IRCCS, 00168 Rome, Italy
†These authors contributed equally to this work.
ORCID: https://orcid.org/0000-0001-7631-029X
Affiliation:
1UOSD Allergologia e Immunologia Clinica, Dipartimento Scienze Mediche e Chirurgiche Addominali ed Endocrino Metaboliche, Fondazione Policlinico A. Gemelli, IRCCS, 00168 Rome, Italy
†These authors contributed equally to this work.
Email: ilaria.baglivo@guest.policlinicogemelli.it
ORCID: https://orcid.org/0000-0003-4041-5182
Affiliation:
2UOSD DH Internal Medicine and Digestive Disease, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, 00168 Rome, Italy
ORCID: https://orcid.org/0000-0002-8207-9837
Affiliation:
3UOC CEMAD Centro Malattie dellʼApparato Digerente, Dipartimento di Scienze Mediche e Chirurgiche, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, 00168 Rome, Italy
Affiliation:
4Scuola di Specializzazione in Allergologia e Immunologia Clinica Università Cattolica del Sacro Cuore, 00168 Roma, Italy
ORCID: https://orcid.org/0000-0001-9039-838X
Affiliation:
4Scuola di Specializzazione in Allergologia e Immunologia Clinica Università Cattolica del Sacro Cuore, 00168 Roma, Italy
ORCID: https://orcid.org/0009-0003-4844-7805
Affiliation:
4Scuola di Specializzazione in Allergologia e Immunologia Clinica Università Cattolica del Sacro Cuore, 00168 Roma, Italy
ORCID: https://orcid.org/0000-0003-4703-2088
Affiliation:
4Scuola di Specializzazione in Allergologia e Immunologia Clinica Università Cattolica del Sacro Cuore, 00168 Roma, Italy
Affiliation:
4Scuola di Specializzazione in Allergologia e Immunologia Clinica Università Cattolica del Sacro Cuore, 00168 Roma, Italy
Affiliation:
5Cardio-CARE, Medizincampus Davos, 7265 Davos, Switzerland
ORCID: https://orcid.org/0000-0002-5618-1141
Affiliation:
6Dipartimento di Neuroscienze, Sezione di Fisica, Università Cattolica del Sacro Cuore, 00168 Rome, Italy
7Fondazione Policlinico Universitario “A. Gemelli” IRCCS, 00168 Rome, Italy
ORCID: https://orcid.org/0000-0002-3694-8229
Affiliation:
8Dipartimento di Patologia clinica, Ospedale Santa Maria Goretti, AUSL Latina, 04100 Latina, Italy
ORCID: https://orcid.org/0000-0002-8328-2570
Affiliation:
6Dipartimento di Neuroscienze, Sezione di Fisica, Università Cattolica del Sacro Cuore, 00168 Rome, Italy
7Fondazione Policlinico Universitario “A. Gemelli” IRCCS, 00168 Rome, Italy
ORCID: https://orcid.org/0000-0002-3233-1897
Affiliation:
9Unit of Otorhinolaryngology, “A. Gemelli” University Hospital Foundation IRCCS, 00168 Rome, Italy
Affiliation:
9Unit of Otorhinolaryngology, “A. Gemelli” University Hospital Foundation IRCCS, 00168 Rome, Italy
ORCID: https://orcid.org/0000-0001-5761-7018
Affiliation:
10Department of Translational Medicine and Surgery, Università Cattolica del Sacro Cuore, 00168 Rome, Italy
11Department of Medical and Surgical Sciences, UOC Gastroenterologia, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Rome, Italy
ORCID: https://orcid.org/0000-0003-4863-6924
Affiliation:
12UOC Pronto Soccorso, Medicina d’Urgenza e Medicina Interna, Ospedale Isola Tiberina Gemelli Isola, 00186 Rome, Italy
Affiliation:
12UOC Pronto Soccorso, Medicina d’Urgenza e Medicina Interna, Ospedale Isola Tiberina Gemelli Isola, 00186 Rome, Italy
Affiliation:
13Department of Internal Medicine and Clinical Complexity, Azienda Ospedaliera Universitaria Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0000-0002-3692-1384
Affiliation:
14UOC Reumatologia, Dipartimento di Medicina dei Sistemi, Università di Roma “Tor Vergata”, 00133 Roma, Italy
Affiliation:
15Allergy and Respiratory Diseases, IRCCS Policlinico San Martino, University of Genoa, 16132 Genova, Italy
ORCID: https://orcid.org/0009-0005-5754-4636
Affiliation:
16Division of Allergy and Clinical Immunology, Department of Medicine, ʻSanta Maria della Speranzaʼ Hospital, 84061 Battipaglia, Salerno, Italy
ORCID: https://orcid.org/0000-0001-5640-6446
Affiliation:
17Department of Medical Sciences and Public Health, University of Cagliari, 09124 Cagliari, Italy
ORCID: https://orcid.org/0000-0002-4517-1749
Explor Asthma Allergy. 2026;4:1009127 DOI: https://doi.org/10.37349/eaa.2026.1009127
Received: February 18, 2026 Accepted: April 16, 2026 Published: May 27, 2026
Academic Editor: Uday Kishore, University of Oxford, England
The article belongs to the special issue Environment, Infectious Diseases, and Allergy
Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare systemic vasculitis with heterogeneous clinical manifestations. Identifying reliable biomarkers is crucial to predicting disease evolution and guiding therapy. We analyzed clinical, biological, and functional data from 33 patients with EGPA in the vasculitic phase. Blood eosinophil count (BEC), eosinophilic cationic protein (ECP), antineutrophil cytoplasmic antibodies (ANCAs), specific IgE to staphylococcal enterotoxins (SE-IgE), and serum free light chains (FLCs) were evaluated. Severe eosinophilic asthma (SEA) and chronic rhinosinusitis with nasal polyps (CRSwNPs) were present in 100% and 88.5% of patients, respectively. Median BEC was 1950 cells/mm3, with elevated ECP (60.0 µg/L). SE-IgE was detected in 54.2% of patients. A significant negative correlation emerged between λ FLCs and oral corticosteroid (OCS) dose (r = –0.58, p = 0.009). Forced expiratory volume in 1 second (FEV1) was significantly lower in C-ANCA+ patients (p = 0.006). ECP and SE-IgE may serve as markers of eosinophilic activity and epithelial barrier damage in EGPA. λ FLCs might be a useful indicator of OCS exposure and treatment response. These biomarkers could support the evaluation of disease evolution and treatment response.
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAV) are a group of systemic diseases affecting small vessels. AAV includes three main forms: granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic GPA (EGPA).
EGPA is a necrotizing vasculitis affecting small- and medium-sized systemic blood vessels. It is considered a rare disease, with a prevalence of 1–3 cases per million adults worldwide, generally affecting women more than men; the median age at diagnosis is 40 years.
Although eosinophils play a central role in EGPA pathophysiology, other immune cells—including mast cells and neutrophils—are also implicated in the inflammatory process. The disease typically progresses through three overlapping phases:
A prodromal phase of variable duration characterized by high type 2 (T2) inflammation, eosinophilic asthma, and chronic rhinosinusitis with or without nasal polyposis. These are the major clinical features of this phase;
A phase of blood hypereosinophilia;
A vasculitic phase characterized by systemic involvement, in which the inflammation of small vessels leads to organ involvement and damage, such as mononeuritis multiplex in peripheral neurological involvement [1].
Importantly, these phases may overlap or not appear sequentially or in all patients, and some individuals may never develop vasculitic complications, reflecting the clinical heterogeneity of EGPA.
The range of organ systems potentially involved in EGPA and the relapsing-remitting nature of this disease exert a very impactful burden on both patients and health care systems.
The ANCAs are detected in 40% of EGPA patients. Indirect immunofluorescence reveals either cytoplasmic ANCA (C-ANCA) or perinuclear ANCA (P-ANCA), whereas immunoassays reveal antibodies specific for proteinase-3 (PR3-ANCA) and myeloperoxidase (MPO-ANCA). MPO-ANCA are more common and specific for EGPA than PR3-ANCA [2]. Although clinical and genetic evidence support the use of ANCA testing to define two distinct subsets of EGPA, vasculitic manifestations such as glomerulonephritis or peripheral neuropathy can be observed in both patients with ANCA-negative EGPA and those with ANCA-positive EGPA. The pathogenic role of MPO-ANCA is known; however, manifestations such as peripheral neuropathy or cardiomyopathy could be due to both vasculitis and eosinophilic infiltration [3].
The treatment of EGPA is focused on reducing inflammation, suppressing the immune response, reducing complications, preventing relapses, and increasing the duration of remission time. Preceding the biologics employment, the standard of care for EGPA involved treatment with corticosteroids alone or in combination with immunosuppressants [4], with a significant burden of side effects due to long-term use. In recent years, the availability of monoclonal antibodies (mepolizumab and benralizumab) has revolutionized the therapeutic approach to EGPA.
In the last decades, the concept of clinical remission has been widely explored in asthmatic patients [5]. In EGPA, remission remains difficult to assess due to the disease’s complexity and the lack of validated biomarkers to monitor disease progression or predict vasculitic involvement.
Preceding the remission assessment, a critical unmet need is predicting the transition from an airway-predominant T2 inflammation phenotype characterized by severe eosinophilic asthma (SEA) and chronic rhinosinusitis with nasal polyps (CRSwNPs) to systemic vasculitis.
Hypereosinophilia, asthma, and CRwNPs are present in 90% of patients during the prodromal phase; however, not all hypereosinophilia-asthma-CRwNPs patients will develop vascular damage.
In this context, the identification of early and reliable biomarkers is essential to enable prompt diagnosis, risk stratification, and individualized treatment approaches. Understanding the inflammatory profile—including epithelial barrier dysfunction and immune dysregulation—may improve disease characterization and guide therapeutic decisions.
The aim of this study is to evaluate the demographic, clinical, and biological features of patients with EGPA in the vasculitic phase. Exploration of the potential role of selected blood biomarkers—including eosinophilic cationic protein (ECP), specific IgE to staphylococcal enterotoxins (SE-IgE), and free light chains (FLCs)—in disease characterization, treatment response, and potentially early detection of vasculitic evolution is also included in the study.
This pilot, prospective, single-center cohort study included 33 patients diagnosed with EGPA according to the 2022 ACR/EULAR classification criteria [2]. Patients were consecutively enrolled at the Allergy and Clinical Immunology Unit of our hospital between January 2023 and December 2024. Only patients in the vasculitic phase were included, and assessments were performed before any treatment modification.
Beyond a comprehensive evaluation including demographic and biological characteristics, all patients underwent:
Pulmonary function tests were performed according to ATS/ERS guidelines [6], and spirometric parameters, particularly forced expiratory volume in 1 second (FEV1), were recorded.
Urinary sediment to detect the eventual renal involvement.
Electrophysiological studies were conducted in patients with suspected peripheral nervous system involvement. Nerve conduction studies assessed the median, ulnar, radial, tibial, fibular, and sural nerves. A reduction or absence of compound muscle action potentials or sensory nerve action potentials was considered diagnostic for neuropathy.
Peripheral blood samples were collected to assess:
Blood eosinophil count (BEC).
ANCAs: C-ANCA and P-ANCA were detected via indirect immunofluorescence on ethanol-fixed neutrophils and confirmed by antigen-specific ELISA [7].
ECP: measured using the Phadia ImmunoCAP system (Thermo Fisher Scientific, Uppsala, Sweden) according to the manufacturer’s instructions. The laboratory reference range was 2.0–18.0 µg/L [8].
Complement fractions (C3, C4).
Total IgE and SE-IgE were measured using ImmunoCAP (Thermo Fisher Scientific, Uppsala, Sweden).
Serum FLCs kappa and lambda: samples were centrifuged at 2,500 g for 10 min, aliquoted, and stored at −80°C until analysis. FLCs were measured using the OPTILITE analyzer (The Binding Site, Birmingham, UK) [9]. Reference ranges: κ: 3.3–19.4 mg/L; λ: 5.7–26.3 mg/L. A κ/λ ratio < 0.26 or > 1.65 was considered abnormal. All analyses were performed blinded to the patients’ clinical status.
Disease burden and clinical control were evaluated using standardized patient-reported outcome measures:
Current treatments were recorded, including inhaled corticosteroids (ICS), long-acting beta-agonists (LABA), and long-acting muscarinic antagonists (LAMA) combinations; oral corticosteroid (OCS) dose (daily prednisone equivalent); and the use of biologics and immunosuppressive agents. The ICS doses were classified as low/medium/high as per GINA 2024 guidelines [13].
Descriptive statistics are reported as medians with interquartile ranges (IQRs) or percentages, as appropriate.
Pearson’s correlation coefficients and point-biserial correlation coefficients were calculated with their corresponding 95% confidence intervals. Statistical analyses were performed using R version 4.4.2.
Patients’ informed consent was obtained for data collection, analysis, and publication. The local ethics board approval was obtained for this study (Comitato Etico Territoriale Lazio Area 3, ID 6154).
A total of 33 patients were included. The median age was 60.0 years [IQR 53.0–66.0], with 48.5% males and 51.5% females. The majority were never-smokers (72.7%), while 9.1% were current smokers and 18.2% were former smokers.
All patients had SEA, and 87.8% had CRSwNP. Peripheral neuropathy was present in 60.6% of patients. The median FEV1 was 74.0% predicted [IQR 65.5–86.0]. No renal involvement emerged from urinary sediment results.
The median BEC was 1,950 cells/mm3 [IQR 1,390–2,560] (Figure 1).
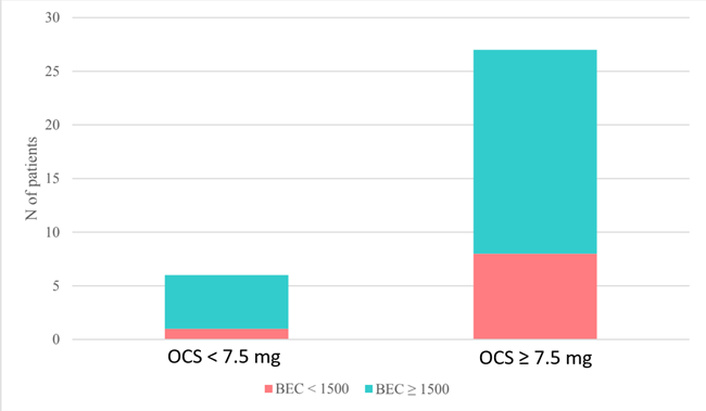
Distribution of patients stratified by OCS dose (< 7.5 mg vs. ≥ 7.5 mg) and BEC (< 1,500 cells/mm3 vs. ≥ 1,500 cells/mm3). Bars represent the number of patients in each subgroup. OCS: oral corticosteroid; BEC: blood eosinophil count.
P-ANCAs were positive in 24.2% of patients, and C-ANCAs in 9.1%. Median serum ECP was 60.0 µg/L [IQR 36.0–109.0].
Total IgE median value was 201.5 kU/L (reference range 0.35–100 kU/L); 54.5% of patients had detectable SE-IgE (Figure 2).
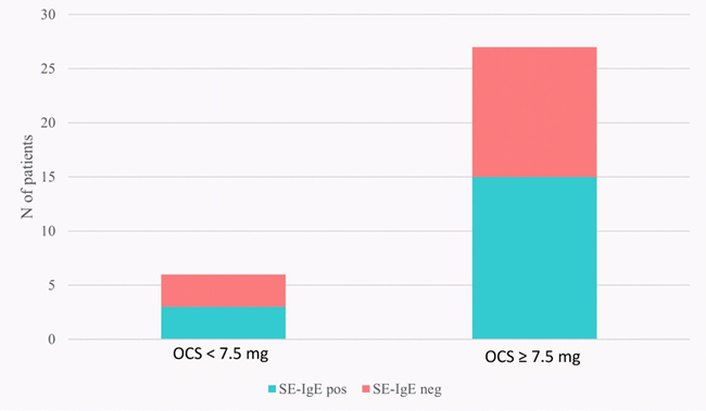
Distribution of patients stratified by OCS dose (< 7.5 mg vs. ≥ 7.5 mg) and SE-IgE. Bars represent the number of patients in each subgroup. OCS: oral corticosteroid; SE-IgE: specific IgE to staphylococcal enterotoxins; pos: positive; neg: negative.
Regarding the FLCs, median κ FLCs was 21.1 mg/L [IQR 15.2–27.4]; median λ FLCs was 15.7 mg/L [IQR 12.8–22.3] with a median κ/λ ratio: 1.26 [IQR 1.19–1.44]. The median C3 and C4 were 90 mg/dL and 24 mg/dL, respectively.
Patient-Reported Outcomes showed: ACQ-5 median: 0.5 [IQR 0.2–0.6]; ACT median: 18.0 [IQR 12.0–23.0]; SNOT-22 median: 80.0 [IQR 52.5–80.0].
All patients were on ICS/LABA therapy; 24.2% were also receiving LAMA therapy. The ICS daily dose was high in 33.3%, medium in 60.6%, and low in 6.1% of patients. 81.8% were receiving OCS ≥ 7.5 mg/day (prednisone or equivalent). 48.5% were treated with biologic therapy (mepolizumab) and 27.3% with immunosuppressants.
A summary of demographic, clinical, and treatment data is shown in Table 1.
Demographics and clinical features of EGPA patients.
| Items | Sample |
|---|---|
| Overall, n | 33 |
| Age (years), median [IQR] | 60.0 [53.0, 66.0] |
| Sex, n (%) | |
| MaleFemale | 16 (48.5)17 (51.5) |
| Weight (kg), median [IQR] | 70.5 [59.0, 81.5] |
| Height (cm), median [IQR] | 169.0 [164.0, 178.0] |
| Smokers, n (%) | |
| FormersNeverCurrent | 6 (18.2)24 (72.7)3 (9.1) |
| FEV1 (%), median [IQR] | 74.0 [65.5, 86.0] |
| BEC (cells/mm3), median [IQR] | 1,950.0 [1,390.0, 2,560.0] |
| C-ANCA, n (%) | 3 (9.1) |
| P-ANCA, n (%) | 8 (24.2) |
| ECP (μg/L), median [IQR] | 60.0 [36.0, 109.0] |
| SE-IgE, n (%) | 18 (54.5) |
| FLCs (mg/L) | |
| Kappa, median [IQR]Lambda, median [IQR]RATIO κ/λ, median [IQR] | 21.1 [15.2, 27.4]15.7 [12.8, 22.3]1.26 [1.19, 1.44] |
| SEA, n (%) | 33 (100) |
| CRSwNP, n (%) | 29 (87.8) |
| CRSwNP number of surgery, median [IQR] | 1.0 [0.0, 1.0] |
| Inhalation therapy, n (%) | |
| ICS/LABAICS/LABA/LAMAHigh ICS doseMedium ICS doseLow ICS dose | 25 (75.8)8 (24.2)11 (33.3)20 (60.6) 2 (6.1) |
| OCS therapy, n (%) | |
| Prednisone (or equivalent) ≥ 7.5 mg | 27 (81.8) |
| Biologics, n (%) | 16 (48.5) |
| Immunosuppressant, n (%) | 9 (27.3) |
| ACQ-5, median [IQR] | 0.5 [0.2, 0.6] |
| ACT, median [IQR] | 18.0 [12.0, 23.0] |
| SNOT-22, median [IQR] | 80.0 [52.5, 80.0] |
| Peripheric neuropathy, n (%) | 20 (60.6) |
ACQ-5: 5-item Asthma Control Questionnaire; ACT: Asthma Control Test; BEC: blood eosinophil count; C-ANCA: cytoplasmic antineutrophil cytoplasmic antibody; CRSwNP: chronic rhinosinusitis with nasal polyp; ECP: eosinophilic cationic protein; EGPA: eosinophilic granulomatosis with polyangiitis; FEV1: forced expiratory volume in 1 second; FLCs: free light chains; ICS: inhaled corticosteroids; IQR: interquartile range; LABA: long-acting beta-agonists; LAMA: long-acting muscarinic antagonists; OCS: oral corticosteroid; P-ANCA: perinuclear antineutrophil cytoplasmic antibody; PR3: proteinase-3; SEA: severe eosinophilic asthma; SE-IgE: specific IgE to staphylococcal enterotoxins; SNOT-22: 22-item Sino-Nasal Outcome Test.
A significant inverse correlation was found between OCS dose and serum λ FLC levels (r = –0.58, 95% CI [–0.82, –0.17], p = 0.009) (Figure 3).
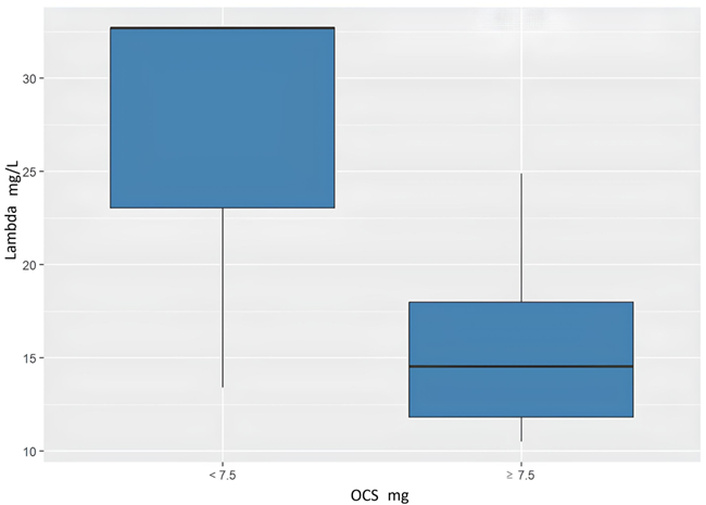
Association between oral corticosteroid (OCS) dose and serum free light chain λ (λ FLCs) levels. Patients were stratified into two groups based on OCS dose (< 7.5 mg vs. ≥ 7.5 mg). Boxplots show that individuals receiving lower OCS doses (< 7.5 mg) exhibit higher serum λ FLCs levels compared to those receiving higher doses (≥ 7.5 mg), suggesting a potential inverse relationship between OCS dose and λ concentrations. In each boxplot, the central line represents the median, the box indicates the interquartile range (IQR, 25th–75th percentile); statistical significance is defined as p < 0.05.
In addition, FEV1 values were significantly lower in C-ANCA-positive patients compared to C-ANCA-negative ones (mean difference: –0.5, 95% CI [–0.74, –0.17], p = 0.006) (Figure 4).
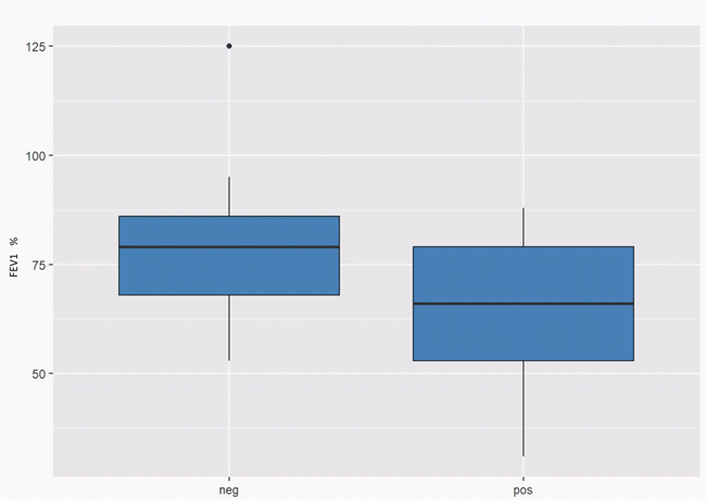
Association between cytoplasmic antineutrophil cytoplasmic antibody (C-ANCA) status and forced expiratory volume in 1 second (FEV1). Patients were stratified according to C-ANCA status (negative vs. positive). Boxplot analysis shows lower FEV1 values in C-ANCA-positive patients compared to C-ANCA-negative individuals, suggesting a potential association between C-ANCA positivity and reduced lung function. In each boxplot, the central line represents the median, and the box indicates the interquartile range (IQR, 25th–75th percentile); statistical significance is defined as p < 0.05. pos: positive; neg: negative.
EGPA is a complex inflammatory disorder with a 5-year survival rate of approximately 90% when correctly diagnosed and treated. However, the prognosis may worsen due to frequent disease relapses, organ involvement, and cumulative chronic damage. In rare diseases such as EGPA, identifying distinct patient clusters and stratifying risk through the use of reliable biomarkers remains a crucial challenge.
The Vasculitis Damage Index (VDI) is a valuable tool for assessing chronic organ damage resulting from both the disease and its treatment and its strongly correlated with mortality and morbidity [14]. While the VDI is useful in patients with established vasculitic involvement, there is currently a lack of biomarkers capable of predicting disease evolution before the vasculitic phase develops.
Our work describes the demographic and clinical features of 33 EGPA patients in the vasculitic phase. According to the currently available data, all EGPA patients were affected by SEA and more than 85% by CRSwNPs, while peripheral neuropathy was present in approximately 60% of the patients.
ANCA positivity was detected in a minority of cases (P-ANCA: 24.2%; C-ANCA: 9.1%), confirming the limited sensitivity of ANCA testing as a standalone biomarker for EGPA, as reported in previous literature [14]. C-ANCA presence is a negative criterion for EGPA definition [2]; however, it can be detected in a minority of EGPA patients. C-ANCA could be involved in pulmonary manifestations in EGPA. Our results suggest a correlation with lower FEV1.
The median BEC in our cohort exceeded 1500 cells/mm3, aligning with current EGPA classification criteria [2]. We observed elevated median serum ECP levels released during eosinophil activation, which directly contributes to tissue damage. ECP may offer valuable insight into disease activity and organ involvement. Although the role of ECP in T2 inflammation remains debated, recent studies have reported higher ECP levels in symptomatic asthmatic patients compared to asymptomatic asthmatic individuals [15], suggesting its potential utility as an active eosinophilic inflammation marker. Furthermore, elevated ECP has been proposed as a predictor of nasal polyp (NP) recurrence after surgery [16], supporting its prognostic relevance in the prodromal phase of EGPA.
Over half of the patients in our study tested positive for SE-IgE. SE-IgE plays an essential role in the pathogenesis of CRSwNP together with IL-5 and other T2 cytokines. SE are known to act as superantigens, inducing a strong Th2 immune response, promoting epithelial barrier dysfunction, and triggering chronic inflammation via activation of IgE-mediated pathways and eosinophil degranulation [17]. These mechanisms may contribute to the progression from localized airway inflammation to systemic disease in susceptible patients.
Similarly, in asthma, SE-IgE detection has been recognized as a marker of epithelial barrier dysfunction and may help to identify more severe patients or a higher risk of progression to systemic involvement.
In our EGPA cohort, only serum levels of κ FLCs were elevated, while λ FLCs remained within the normal reference range. Notably, a significant negative correlation was observed between serum λ FLC levels and OCS dosage, suggesting a potential suppression of FLC λ synthesis by corticosteroid treatment. These findings are consistent with previous observations in SEA, where κ FLCs appeared to reflect early inflammatory responses, while λ FLCs may represent a more delayed or sustained immunological activation, potentially linked to disease severity [18].
The observed κ/λ ratio remained within normal limits; this could support the hypothesis that κ FLCs serve as an early-phase inflammatory marker, whereas λ FLCs, being more sensitive to corticosteroid suppression, may serve as a biomarker of chronic treatment exposure or corticosteroid-related immune modulation [13–18].
FLCs have also been investigated in both ANCA-associated and ANCA-negative vasculitides [19], suggesting a broader role in systemic inflammatory conditions. Based on our findings, serum λ FLCs could be a potential biomarker for OCS exposure and corticosteroid-related tissue damage. Further investigation in larger cohorts is warranted to confirm these preliminary insights and better delineate the role of FLCs in EGPA pathogenesis and management, considering the cross-sectional nature of the study and the small patient cohort.
In EGPA, the hypothesis of an autoimmune trigger involving molecular mimicry and antigenic spread has been proposed as a mechanism by which local eosinophilic inflammation—such as that seen in SEA—may evolve into systemic vasculitis [20]. However, the unpredictable nature of this progression and the variability in clinical presentation underscore the urgent need for tools that allow better risk stratification.
As current therapies show limited efficacy in reversing systemic damage once the vasculitic phase is established, identifying patient endotypes is increasingly important. Defining distinct inflammatory or immunological clusters may allow for earlier recognition of patients at higher risk of disease progression, facilitating a precision medicine approach. Incorporating potential biomarkers in early screening in EGPA could therefore improve patient stratification and enable earlier intervention—potentially intercepting epithelial barrier damage/immunological dysfunction before the vasculitic phase develops. Study limitations: one key limitation of our study is the lack of stratification based on OCS dosage or type of treatment, which was constrained by the small sample size. Future studies with larger cohorts should explore differences across treatment subgroups, including biologics and immunosuppressants. Recent data from the EGPA Study Group showed no significant differences in clinical characteristics or outcomes between patients treated with different biologics [21], though further subgroup analyses are needed.
The lack of vasculitis activity scores, the treatment heterogeneity, the small monocentric patient cohort, the cross-sectional design of our study, together with the absence of a control cohort, limit the strength of our results, which are preliminary. Another limitation of our study is that only patients in the vasculitic phase were evaluated. Longitudinal studies tracking biomarker profiles across the different phases of EGPA—particularly from the prodromal to vasculitic phase—are crucial for understanding disease evolution. As observed in severe asthma, the phenotypic variability in EGPA remains poorly explained. Identifying why only a subset of SEA and CRSwNP patients progress to systemic vasculitis is a critical unmet need.
Even if certain causality cannot be established, our preliminary findings seem to confirm the limited diagnostic utility of ANCA in EGPA, highlighting the potential role of composite biomarkers in assessing disease activity and progression.
Serum ECP may reflect eosinophilic activation and tissue damage, while SE-IgE could indicate epithelial barrier dysfunction. Considering the mentioned limitations, the inverse correlation between λ FLC levels and corticosteroid exposure could suggest a possible role of λ FLC as a treatment burden marker.
Further studies are needed to validate these biomarkers and explore their role in early disease detection and personalized treatment strategies.
AAV: antineutrophil cytoplasmic antibody-associated vasculitides
ACQ-5: 5-item Asthma Control Questionnaire
ACT: Asthma Control Test
ANCAs: antineutrophil cytoplasmic antibodies
BEC: blood eosinophil count
C-ANCA: cytoplasmic antineutrophil cytoplasmic antibody
CRSwNPs: chronic rhinosinusitis with nasal polyps
ECP: eosinophilic cationic protein
EGPA: eosinophilic granulomatosis with polyangiitis
FEV1: forced expiratory volume in 1 second
FLCs: free light chains
GPA: granulomatosis with polyangiitis
ICS: inhaled corticosteroids
IQRs: interquartile ranges
LABA: long-acting beta-agonists
LAMA: long-acting muscarinic antagonists
MPO: myeloperoxidase
OCS: oral corticosteroid
P-ANCA: perinuclear antineutrophil cytoplasmic antibody
PR3: proteinase-3
SEA: severe eosinophilic asthma
SE-IgE: specific IgE to staphylococcal enterotoxins
SNOT-22: 22-item Sino-Nasal Outcome Test
T2: type 2
VDI: Vasculitis Damage Index
CC: Project administration, Conceptualization, Methodology, Investigation, Writing—original draft, Writing—review & editing, Supervision, Validation, Data curation. IB: Project administration, Conceptualization, Methodology, Investigation, Writing—original draft, Writing—review & editing, Supervision, Validation, Data Curation. SC, MR, E De Corso, GBC, PA, AD, EG, BB, VP, and SDG: Writing—review & editing, Supervision. MAZ, DL, CL, LB, GL, FRS, and GC: Data Curation, Writing—review & editing, Supervision. E Di Carluccio, UB, and BN: Data Curation, Formal analysis. AG: Supervision, Visualization. All authors read and approved the submitted version.
Vincenzo Patella, who is the Editorial Board Member and Guest Editor of Exploration of Asthma & Allergy, had no involvement in the decision-making or the review process of this manuscript. The other authors declare no conflicts of interest.
The study was approved by the Comitato Etico Territoriale Lazio Area 3 Ethics Committee (ID 6154) and complies with the Declaration of Helsinki.
Patientsʼ informed consent was obtained for data collection, analysis, and publication.
Patientsʼ informed consent was obtained for data collection, analysis, and publication.
Data are available upon reasonable request to the corresponding author.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 687
Download: 39
Times Cited: 0
Aurelia S. Monk ... Adam J. Kimple
Maria Concetta D’Ovidio ... Gennaro D’Amato
Aimuanmwosa Frank Eghomwanre, Henrietta Onyinye Ogbebor
