Review
Review

Affiliation:
Department of Clinical Psychology, Kashan University of Medical Sciences, Kashan 8713783976, Iran
Email: behrooz.afshari71@gmail.com
ORCID: https://orcid.org/0000-0002-1705-6698
Explor Neurosci. 2023;2:331–349 DOI: https://doi.org/10.37349/en.2023.00032
Received: June 09, 2023 Accepted: October 11, 2023 Published: December 29, 2023
Academic Editor: Dirk M. Hermann, University of Duisburg-Essen, Germany
The article belongs to the special issue Novel Therapeutic Approaches for the Treatment of Depression
Bipolar disorder (BD) is a debilitating psychiatric disorder characterized by recurrent depression, mania, and hypomania episodes. The interaction of psychological, neuropsychological, and neurobiological factors (cognitive, behavioral, and emotional) is implicated in the development and persistence of BD. Accordingly, almost all investigators confirm that BD is the outcome of psychological and genetic interactions. Therefore, researchers should consider various factors in the psychopathology and psychotherapy of BD. This selective review first reviews research on these factors, then points to a variety of therapeutic methods for BD [interpersonal and social rhythm therapy (IPSRT), cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), mindfulness-based cognitive therapy (MBCT), and family-focused therapy (FFT)], and finally suggested a new comprehensive integrated model for the assessment and therapy of BD.
Nowadays, almost all researchers agree that bipolar disorder (BD) is the result of many genetic and psychological interactions [1]. French psychiatrist Jean-Pierre Falret published an article in 1854 describing what he called “la folie circulaire”, which translated to circular insanity [2]. The article details individuals switching through severe depression and mania and is considered to be the first documented diagnosis of BD [2, 3].
The definitions and distinctions of BD in the field of mental health are a continuing issue and have been frequently revised by the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD) [4, 5]. The conceptualization of the BD has changed since the first description of mania-depressive illness. Although depression and mania episodes are defined by symptoms that have changed over the years, hypomania episodes have been described with fewer changes and their location is less clear than other episodes. Mania and hypomania episodes are considered dimensional as hypomania is a mild episode of mania [6]. When Dunner [7] and Dunner et al. [8] described BD II, the concept of hypomania was dismissed as a milder form of BD.
Despite in the past, there are some specific psychological models for BD today. The cognitive model focuses on schemas [9], negative self-thoughts [10], self-concepts [11], and dysfunctional attitudes [12]. The interpersonal model emphasizes marital contrasts, problems at work, transition from adolescence to adulthood, retirement, and on the whole, building and maintaining relationships [11]. The emotional model emphasizes abnormal processing of emotion and poor emotional retention in BD [13]. In this model, emotion is considered as a whole system reaction because it not only includes emotions, memories, and desires but also a way to think [14]. Behavioral activation and behavioral inhibition models are included in the behavioral models of BD, in which behavioral activation is related to the mania episode of BD, and behavioral inhibition is related to the depression episode of BD [15]. Over the past decades, researchers have also pointed to many life events that have been implicated in BD. Symptoms of BD are predictable by emotional expression, self-esteem, social support, cognitive styles, sleep problems, and many other factors [16]. Some other studies have also addressed the psychological aspects of BD such as cognitive vulnerability and coping skills, for example, pathology may be related to the duration of BD and the number of its episodes [17].
In this selective review, neurobiological, neuropsychological, and psychological models will be referred (behavioral, cognitive, emotional, and personality), then review past and present interventions for BD, and finally, a specific intervention for BD will be addressed that may be useful in improving the efficacy of treatment for the BD and may be an introduction to further researches and design of future therapies.
The BD is diagnosed for patients who are experiencing both types of depression and mania episodes or hypomania or who only experience mania episodes. BD I is defined as having at least one mania episode or mixed episodes, and sometimes a major depression episode in the clinical course. The mixed episode is a period of at least one week in which both mania and major depression are found almost daily. A type of BD characterized by major depression and hypomania (and not mania) episodes is called BD II [18]. The ratio of males to females in BD is approximately equal. The combined prevalence of BD I, BD II, and indeterminate BD in the USA in the DSM-5 was estimated at 1.8% and slightly higher (2.7%) in samples of local community youth 12 years and older. The most common disorders associated with BD include alcohol abuse or dependence, panic disorder, obsessive-compulsive disorder, and social anxiety disorder. In BD, men are more likely to present with substance-related disorders and women are more likely to have concurrent anxiety and eating disorders [19].
Mania episodes are defined by abnormally elevated or irritable mood, accompanied by increased activity, decreased need for sleep, increased self-confidence, flight of ideas, rapid speech, and engagement in pleasurable activities without regard to potential negative consequences [20].
Over the past decade, many researchers have suggested that BD patients have deficits in brain structures [21], cognitive function [22], executive function [23], emotion regulation [24], and many other factors.
As mentioned above, a number of theoretical models including cognitive, behavioral, emotional, and interpersonal models have attempted to explain the creation and maintenance of BD. Subsequently, neurobiological, neuropsychological, and psychological models of BD will be examined that attempt to explain this disorder.
Although the diagnosis and treatment of BD are based on psychological and psychiatric models, the neurobiological model has a significant impact on the pathology of this debilitating disorder. The risk of BD in their first-degree relatives is increased [25]. The etiology of BD is not yet clearly defined and involves the interaction between genetic and environmental factors [26]. Also, network connectivity changes may be related to poorer performance in BD patients [21].
Genetic factors, neurobiological abnormalities, and neurotransmitters play a key role in the etiology of BD. Genome-wide association studies (GWAS) were conducted to determine that genes or genetic factors could play an important role in developing BD. Also, many researchers wanted to investigate genes to find out if these genes make a link with BD [27]. They analyzed genes that were associated with neurophysiological processes which contribute to or are also impaired in BD pathologies. Analyzed genes that play a role in circadian rhythms, dopaminergic and serotonergic pathways, brain development, and neurotropism. Moreover, genes that were associated with schizophrenia were also investigated whether the same genes are associated with BD. Some other studies have supported the presence of noradrenergic system abnormalities in BD [28]. Some research has also supported the important role of the serotonergic system in depression episodes in BD, in that reducing 5-hydroxyindoleacetic has been implicated in impulsivity, aggression, and suicide [27]. Another neurotransmitter that plays an important role in BD is dopamine [28]. The decrease in dopamine has been implicated in depression and its increase in mania and hypomania [29, 30]. Depression episodes in BD are also associated with cholinergic [27].
Although the mood swing between depression and mania episodes is the most important feature that distinguishes BD from other psychiatric disorders, the neurobiology of the mood swing is still poorly understood [31]. Swings from depression to mania or hypomania can not only occur spontaneously during the course of the illness but also through stress, sleep deprivation, and standard treatment for depression episodes such as electroconvulsive therapy and medication [32, 33]. Several brain regions have also been implicated in the swing from mania to depression, such as the hypothalamic-pituitary-adrenal axis [31].
Some studies of mental disorders have revealed abnormalities in important parts of the brain such as the frontal cortex [34]. In addition, many patients with frontal lobe injuries have reported deficits in problem-solving and planning their daily activities [35]. Also, there are dysfunctions in the prefrontal cortex and amygdala that are associated with problems in emotion processing [36, 37].
Another area that has been damaged in BD is the anterior singlet cortex [38]. Deficits in this cortex have been associated with emotional and cognitive dysfunction in BD [39, 40]. Another abnormal region in BD is the orbitofrontal cortex [41]. This cortex plays a role in impulse control and mood regulation [42].
Many studies have pointed to neuropsychological deficits in BD [43]. Studies showed that BD has deficits in attention, executive function, cognitive function, cognitive flexibility, and memory [23]. Xu et al. [22] showed that patients with BD have cognitive dysfunction in processing speed and visual memory, which may be a genetic feature of BD patients. BD is also associated with deficits in executive functions such as cognitive flexibility and attention change [44].
In BD patients, higher levels of cognitive deficits are associated with frequent hospitalizations, behavioral, emotional, and cognitive responses as well as the inability to delay rewards [45].
Although the mechanism underlying cognitive deficits in individuals is unclear, many researchers have pointed to the fundamental effects of genes on brain function and cognitive deficits [46–48]. These deficits are associated with psychological dysfunctions in areas such as job performance, communication with family members, and life satisfaction. Also, these functions are associated with the severity of symptoms in mental disorders [49].
Also, numerous executive dysfunctions in BD have been identified, notably that executive deficits have widespread and significant impacts on the lives of bipolar patients, indicating severe problems in controlling and regulating their behaviors [50]. The impact of executive function is so great that researchers refer to it as the basis of almost all of the disorders in the DSM [51]. The neuropsychological structure of executive function and its evaluation methods are different from the neurological disorders present in DSM-5. The major flaw in the diagnostic criteria for neurological disorders present in the DSM-5 is a misunderstanding of clinical neuroscience assessment, especially executive functioning assessment [52]. However, performance-related deficits are associated with the number of mood swings in BD [53]. Some studies showed that the range of cognitive and executive dysfunction in BD patients is related to the course of illness and length of hospitalization, and deficits in the mania episode are more extensive than the other episodes [45].
Psychological factors in BD are very important both clinically and theoretically. Understanding the role of psychological factors in BD can help in understanding the pathology of this disorder and its underlying mechanisms and developing interventions for these patients [54]. Many studies have linked psychological abnormalities associated with depression to unstable self-esteem [55], rumination [56], and distorted attitudes toward self-evaluation [57]. Also, many other studies have linked psychological abnormalities associated with mania to behaviors related to goal achievement and reward [58]. Here research related to behavioral, cognitive, emotional, and personality factors in BD is reviewed.
In BD, hypersexuality is also considered a diagnostic criterion [59]. Hypersexuality may be influenced by psychological factors such as psychosocial factors, psychodynamic factors, aggression, and disordered behaviors [60, 61]. Studies show that in bipolar patients who are disturbed in their sexual responses, there is more difficulty in desire, arousal, and the ability to reach orgasm [62].
During the mania period, patients show impulsive behavior, hyperactivity, thought jumping, and motor hyperactivity, which are considered as an inability to inhibit behavior and thought [63]. These symptoms in BD lead to the destruction of social, occupational, and family functioning [64].
In children whose parents have BD, the risk of behavioral, emotional, and adjustment problems is higher [65]. Some studies have found that bipolar patients received less warmth and acceptance but more psychological control from their parents in childhood [66].
One of the dysfunctional aspects of BD is social cognition. Social cognition is defined as the ability to encode, store, retrieve, and apply social information in a social context [67]. Research shows that cognitive deficits are among the main abnormalities in BD [20].
Although some studies suggest that cognitive processes affect emotional processes, other studies support that emotional processing affects cognition [20]. Overall, researchers emphasize the mutual influence of cognition and emotion on each other [20]. Some researchers have argued that language processing, processing speed, memory, and attention are related to emotional understanding in BD [68].
The inability to regulate emotion is one of the first abnormalities of BD, and the two areas that are most important in emotion regulation are the amygdala and the prefrontal cortex [69]. Bipolar patients have problems in emotional processing, emotional perception, emotional learning, emotional memory, and facial expression, which are associated with the dysfunction of the prefrontal cortex and amygdala [36, 37]. Moreover, many studies have suggested that mixed episodes of BD are associated with suicide [70].
Emotional perception is considered as the first stage of responding to the emotions [67]. Some researchers have reported low accuracy and slow response to emotions such as fear and hatred in BD [71]. Emotional perception ability can predict quality of life in BD [67]. In BD, facial emotion recognition is also related to parenting style [36]. Some research has supported that the deficits in facial emotion recognition may be related to mood state in BD [72]. For example, researchers have found that the ability to recognize negative facial emotion is intact during euthymia while impaired during mania [73]. Research shows that positive or negative effects remain in bipolar patients even after remission [20, 74]. Studies also show that bipolar patients are less able to use emotion regulation strategies but use abnormal strategies instead [75, 76]. Bipolar patients show more problems in controlling speech and behavior than healthy people [77].
Some studies have supported that emotion dysregulation is observed early in BD in patients [78]. Some other studies show that negative emotion regulation is related to the severity of depression symptoms [79, 80]. Emotions related to impulsivity in BD are also related to aggression and suicide [81]. Also, the ability to regulate positive and negative emotions has an important impact on the consequences of BD [20].
Most research shows that BD is more related to negative emotions and maybe less related to positive emotions [20]. These patients are less confident in using emotion regulation strategies. Also, emotional variables have prominent effects on the consequences of BD. Incorrect and negative emotion regulation strategies are related to dysfunction in BD [20].
High levels of emotion may also be involved in executive functioning [82]. In fact, better skills in regulating emotions have a great impact on improving executive functioning [83], especially working memory [84], cognitive flexibility [85], and cognitive inhibition [86].
Personality has been implicated in the etiology, development, and continuation of BD. Kraepelin [87] suggested that there are several specific temperaments in mania-depressive disorder. The most important of which can be the moody “depressive” temperament, the impulsive “mania” temperament, and the hot-tempered “irritable” temperament. Then, many studies have examined personality in BD [88, 89].
Recent investigations have assessed the relevance of various theories of personality for BD [88]. For example, psychosocial personality dimensions, such as extraversion, inhibition, and impulsivity, are higher in BD patients than in normal individuals [89]. Also, Cloninger’s personality theory has been used for mood disorders, and in BD, higher scores have been reported for novelty seeking, reward dependence, and self-transcendence [90].
More studies have been conducted on the behavior activation system in BD [88] with the general finding that activity in this system is significantly stronger than in normal people. Also, it has been reported that BD patients expend more effort when striving towards their goals, further supporting the role of the behavior activation system [89]. In addition, the higher levels of behavior activation system activity in BD patients are associated with high rates of behavioral and cognitive responses, as well as a weakened inability to postpone rewards [15]. Also, Meyer et al. [91] showed that behavior activation system scores related to mania and behavior inhibition system scores are related to depression. Also, an increasing behavior activation system in BD is consistent with increased dopamine levels and more dopaminergic activity [92]. The behavior activation system is controlled by the dopaminergic route as well as the limbic system and its components such as the amygdala [93]. Individuals with strong behavioral activation systems are reward-sensitive, are more likely to use high-risk behaviors, and show more impulsive behaviors [15].
Bipolar patients have higher scores on neuroticism, extraversion, and disinhibition than healthy individuals. Neuroticism predicts depression episodes and suicidal behaviors [94].
Barnet et al. [95] found that increasing neuroticism along with a decrease in extraversion may indicate a person prone to depression, while not predicting a specific characteristic of a mania episode. Overall, many studies have investigated the personality traits of BD and have shown that these patients have many differences from healthy individuals.
Over the past few decades, many preventive interventions have been suggested for BD. BD is a debilitating and costly condition, and for this reason, special treatments are now available for it [96]. The main treatment for BD is medication, and a few researches have been done on the psychotherapy of these patients, of which much less have been approved [54, 83].
Medication is the cornerstone and the main treatment for BD. Although success has been achieved in the treatment of BD [97], this treatment alone is not effective and is associated with approximately 40–60% recurrence [98]. Also, none of the mood stabilizers have had a significant effect on the treatment of BD [99]. The therapeutic response of BD patients to medication is only 50% [97]. However, mood stabilizers can lead to problems such as metabolic and cardiovascular diseases. In addition, 50% of BD patients have at least one non-adherence to medication [100]. In BD, polypharmacy is a rule, not an exception [98]. Finally, it is better to point out that medication alone cannot improve cognitive deficits such as memory as well as executive deficits such as problem-solving [17].
One of the psychotherapies used for BD is cognitive behavioral therapy (CBT). This treatment deals with the cognitive and behavioral patterns of BD [101]. In several randomized controlled trials (RCTs), CBT has been shown to decrease the severity of depression and improve some of the functions of BD [102], but CBT may be less effective with high severity of BD or those with multiple episodes. Some findings indicate that CBT is an effective treatment for depression episodes in BD, but its effectiveness for mania episodes is questionable [98]. Also, Scott [101] showed that CBT may be more useful for BD patients who are in the early stages of their disorder (see Table 1 for more information) [103–119].
CBT for BD
| Study | Mean age | Sample size | Female | Intervention type | Outcomes | Follow-up |
|---|---|---|---|---|---|---|
| Nielssen et al. [103] | 44 | 83 | 55 | 10 weekly group sessions | Reductions in symptoms of depression and mania | 6 months |
| Henken et al. [104] | 46 | 23 | 18 | 10 weekly group sessions | Variation in mood states diminished; there was a change from depressive states to more euthymic states; there was an increase in overall psychosocial functioning and self-reported psychological health | 2 months and 12 months |
| Weinstein et al. [105] | 9.19 | 69 | 29 | 12 weekly group child- and family-focused CBT | Higher self-esteem; decreases in depression and mania symptoms, suicidal ideation, and anxiety; improving mental health in children and parents | 6 months |
| Steinan et al. [106] | 32.4 | 40 | 24 | 8 weekly individual sessions | Improvement in sleep quality; lower scores in mania and depression | 6 months |
| West et al. [107] | 9.15 | 69 | 28 | 12 weekly group child- and family-focused CBT | Reducing mania and depression symptoms; improvement in global functioning | 6 months |
| Costa et al. [108] | 41.5 | 41 | 27 | 14 weekly group sessions | Lower scores for mania (not statistically significant) and depression (statistically significant) as well as a reduction in the frequency and duration of mood episodes; significant improvement in mental health | 6 months |
| González-Isasi et al. [109] | 41.30 | 40 | 19 | 20 weekly individual sessions | Fewer hospitalizations corresponded to better progression, and higher self-esteem corresponded to better prognosis | 6 months and 12 months |
| Parikh and Scott [110] | 40.9 | 204 | 118 | 20 weekly individual sessions | Significantly lower scores in mania and depression | 18 months |
| Gomes et al. [111] | 38.5 | 50 | 27 | 18 weekly group sessions | Significant decreases in the number of depression and mania episodes, and managing mania symptoms | 12 months |
| da Costa et al. [112] | 40.5 | 37 | 25 | 14 weekly group sessions | Fewer symptoms of mania, depression, and anxiety, as well as fewer and shorter mood change episodes | 6 months |
| West et al. [113] | 9.45 | 26 | 11 | 12 weekly group child- and family-focused CBT | Significant improvement in mania symptoms; parents reported an increased ability to cope with their child’s illness | None |
| Zaretsky et al. [114] | 40.7 | 79 | 46 | 14 weekly individual sessions | Lower levels of affective symptoms and higher psychosocial functioning; fifty percent fewer days of depressed mood over the course of one year | 12 months |
| Reilly-Harrington et al. [115] | 38.4 | 10 | 6 | 20 weekly individual sessions | Significant decreases in depressive mood; decreases in mania; significant decreases in anxiety | 2 months |
| Scott et al. [116] | 41 | 253 | 130 | 22 weekly individual sessions | Significant decreases in depression, mania, and hypomania | 6 months, 12 months, and 18 months |
| Feeny et al. [117] | 14 | 16 | 9 | 12 weekly individual sessions | Significantly lower scores in depression and mania | 2 months |
| Pavuluri et al. [118] | 11.33 | 34 | 10 | 12 weekly group child- and family-focused CBT | Significant reductions in ADHD, depression, mania, psychosis, aggression, and sleep disturbance; high levels of treatment integrity, adherence, and satisfaction | None |
| Patelis-Siotis et al. [119] | 39.8 | 49 | 28 | 14 weekly group sessions | Lower scores in symptom severity, and significant improvement in mental health | None |
ADHD: attention deficit/hyperactivity disorder
Interpersonal and social rhythm therapy (IPSRT) is a psychotherapy specifically designed for BD and includes two sections of social rhythm therapy and interpersonal psychotherapy [118]. Other studies showed that IPSRT may reduce the severity of depression in BD [120]. Swartz et al. [121] have shown that IPSRT may be an effective treatment for depression episodes of BD. They also showed that IPSRT helps to reduce depression episodes of BD better than medication. Furthermore, it was reported that IPSRT improved mood disorders (see Table 2 for more information) [122–127].
IPSRT for BD
| Study | Mean age | Sample size | Female | Intervention type | Outcomes | Follow-up |
|---|---|---|---|---|---|---|
| Steardo et al. [122] | 49.1 | 22 | 14 | 12 weekly individual sessions | Improvement in anxious, depressive, mania symptomatology, and global functioning | 3 months and 6 months |
| Frank et al. [123] | 24.3 | 34 | 22 | 12 weekly individual sessions | Decreases in mood symptoms and improvement in psychological functioning | 6 months |
| Goldstein et al. [52] | 15.2 | 13 | 6 | 12 weekly individual sessions | Decreases in mood symptoms and improvement in psychological functioning | 6 months |
| Bouwkamp et al. [124] | 41.4 | 22 | 10 | 24 weekly group sessions | Decreases in depressive symptoms and number of hospital admissions; increased stability of the social rhythm | None |
| Hlastala et al. [125] | 16.5 | 12 | 6 | 18 weekly individual sessions | Significant decreases in mania, depressive, and general psychiatric symptoms; increased global functioning | 12 months |
| Frank et al. [126] | 34.5 | 125 | 74 | 24 weekly group sessions | More rapid improvement in occupational functioning | None |
| Orhan et al. [127] | 34 | 175 | 92 | 12 weekly individual sessions | Ability to increase regularity of social rhythm; significant decreases in symptom severity | 24 months |
Another type of psychotherapy for BD is dialectical behavior therapy (DBT). DBT developed by Linehan et al. [128] is a type of psychotherapy initially used to treat patients with borderline personality disorder, suicidal behaviors, and self-harm. This method was later used to treat other mental disorders such as BD [128]. The effectiveness of DBT in reducing depression severity, emotion regulation, and suicide reduction suggests that DBT can be effective in the treatment of BD [98]. DBT has been found to be effective in reducing suicidal behaviors, emotion dysregulation, and depression severity in BD [129–131]. Effective in impaired dysfunction, Steardo et al. [122], showed that DBT for 12 months resulted in decreased amygdala activity and improved mood and emotion regulation in patients with BD. They also showed that DBT intervention for 3 months decreased amygdala activity and improved emotion regulation (see Table 3 for more information) [122, 130, 132, 133].
DBT for BD
| Study | Mean age | Sample size | Female | Intervention type | Outcomes | Follow-up |
|---|---|---|---|---|---|---|
| Samadi et al. [131] | 16.2 | 40 | 20 | 8 weekly group sessions | Reduces aggression, self-criticism, and self-injurious behaviors | None |
| Afshari et al. [132] | 36.5 | 60 | 34 | 12 weekly individual sessions | Lower scores in mania, depression, and emotion dysregulation; higher scores in mindfulness, planning, problem-solving, and cognitive flexibility | 3 months |
| Eisner et al. [133] | 41.3 | 37 | 27 | 12-week DBT group skills training | Skill acquisition in the areas of mindfulness, emotion regulation, and distress tolerance; improved psychological well-being and decreased emotion reactivity | 6 months |
| Goldstein et al. [130] | 16.3 | 20 | 15 | 36 weekly individual sessions | Acceptability of the intervention was high, with less severe depressive symptoms and suicidal ideation, a significant improvement from pre- to post-treatment in mania symptoms, and emotional dysregulation | 12 months |
| Van Dijk et al. [98] | 43.2 | 24 | 18 | 12 weekly group sessions | A trend toward reduced depressive symptoms, significant improvement in mindful awareness, and less fear toward and more control of emotional states; group attendees had reduced emergency room visits and mental health related admissions in the six-month follow-up | 6 months |
Family-focused therapy (FFT) has also been shown to be effective in treating BD. The FFT was initially formulated for families of people at risk for schizophrenia and targeted high levels of emotion. FFT was then adapted to treat BD [118]. Several studies have shown that FFT significantly reduces the duration of depression in BD [134, 135]. The FFT can also be effective in reducing the rates of depression in adolescents. Researchers have hypothesized that the effects of FFT on BD may be due to family support for patients. It can also be effective in reducing family problems and poor social functioning (see Table 4 for more information) [105, 118, 136–142].
FFT for BD
| Study | Mean age | Sample size | Female | Intervention type | Outcomes | Follow-up |
|---|---|---|---|---|---|---|
| Tabas et al. [136] | 31.88 | 60 | 16 | 12 weekly group sessions | Improved relapse prevention and promoted social functioning | 3 months |
| Fredman et al. [137] | 35.61 | 108 | 67 | 21 weekly individual sessions | Improvements in mania symptoms; showing appropriate self-sacrifice | None |
| West et al. [107] | 9.15 | 69 | 28 | 12 weekly group child- and family-focused CBT | Reducing mania and depression symptoms; improvement in global functioning | 6 months |
| Miklowitz and Chung [138] | 14.4 | 52 | 33 | 21 weekly individual sessions | Reductions in depressive and mania symptoms | 12 months |
| Solomon et al. [139] | 41 | 53 | 30 | 12 weekly individual sessions | Recovering from mood episodes; changing attitude toward the illness; decreasing feelings of isolation and burden; significantly fewer hospitalizations; increasing the ability to manage symptoms and mood episodes | 6 months |
| Miller [140] | 39 | 92 | 52 | 12 weekly group sessions | Significantly improves recovery from BD I mood episodes | None |
| Reinares et al. [141] | 35.4 | 45 | 22 | 12 weekly group sessions | Increasing caregivers’ knowledge of BD, reduced caregivers’ belief about the link between disruption in life and the patient’s behavior, and reduced the caregivers’ subjective burden | 3 months |
| Weisman et al. [142] | 27.19 | 26 | 26 | 21 weekly individual sessions | Decreases in hospitalization; improvement in problem-solving and management of episodes | 24 months |
Mindfulness-based cognitive therapy (MBCT) is a treatment protocol that includes meditation practices and CBT exercises. This treatment, which was formulated for unipolar depression [143], was later adapted for depression episodes in BD [118]. Some studies have reported positive results of using MBCT for BD I and BD II [144]. The MBCT helps patients to be more able to observe their thoughts and feelings and to experience less depression [144–146]. A study of the use of MBCT for BD showed a significant reduction in anxiety in BD patients [147]. MBCT may also be effective in treating cognitive and emotional problems associated with depression episodes of BD and reduce residual symptoms of BD (see Table 5 for more information) [118, 148–156].
MBCT for BD
| Study | Mean age | Sample size | Female | Intervention type | Outcomes | Follow-up |
|---|---|---|---|---|---|---|
| Hanssen et al. [150] | 46.6 | 72 | 43 | 8 weekly group sessions | Reducing current depressive symptoms; improving mindfulness skills; reducing trait anxiety; positive mental health | 15 months |
| Weber et al. [151] | 48 | 71 | 53 | 12 weekly group sessions | Decreases in depression and anxiety symptoms; improving quality of life, attention, emotion regulation abilities, psychological well-being, psychological functioning, and self-efficacy; greater self-awareness | 3 months |
| Miklowitz et al. [152] | 33.7 | 39 | 39 | 8 weekly group sessions | Increasing mindfulness and improvements in depression | 6 months |
| Lahera et al. [153] | 41 | 140 | 86 | 8 weekly group sessions | Reduced depressive symptoms and improved cognitive performance | 3 months |
| Howells et al. [154] | 37 | 12 | 10 | 8 weekly group sessions | Improved attention readiness; attenuated activation of non-relevant information processing during the attention process | None |
| Stange et al. [155] | 42 | 8 | 6 | 12 weekly group sessions | Improving mindfulness, nonjudgmental observance and awareness of thoughts, feelings, sensations, and executive functioning | 24 months |
| Weber et al. [156] | 48 | 15 | 11 | 8 weekly group sessions | Improving mindfulness and decreasing depression | 12 months |
Although each therapeutic pattern used for BD is based on a specific theoretical orientation, there are several aspects in common. First, each of these therapies targets specific symptoms and has a limited effect on BD, for example, CBT is effective in reducing the severity of depression but does not work for mania. Second, these therapies (except IPSRT) are not initially designed to treat BD. Taken together, these findings suggest that current interventions for BD (both medication and psychotherapy) need to be improved and promote their effectiveness in BD. Therefore, it is imperative to seek more effective treatments that address BD and target the symptoms directly.
As mentioned earlier, in the psychopathology field of BD, it is better to pay attention to behavioral, cognitive, emotional, personality, and neuropsychological factors. In this case, a more comprehensive understanding of BD will be obtained, although this may be relatively time-consuming. Psychopathology is the introduction to the treatment of BD. Therefore, the primary focus should be on the correct recognition of all factors that cause and maintain BD.
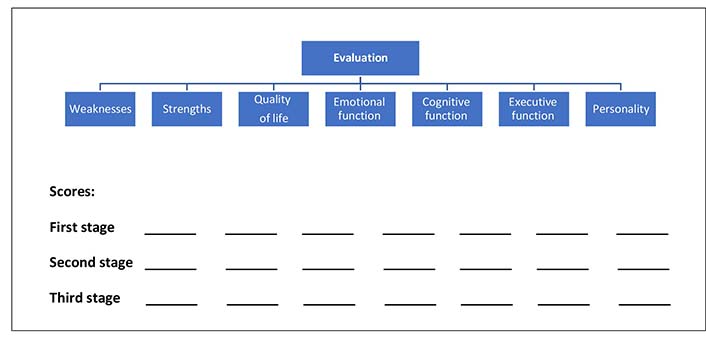
The first stage will be an interview with bipolar patients so that after the diagnosis of BD is confirmed, the symptoms of the disorder and their severity, the patient’s performance (cognitive, executive, and emotional functions), quality of life, coping abilities, and the patient’s weaknesses and strengths are identified. It is better to design a tool to measure all functions together. The proposed tool can combine several questionnaires and neuropsychological tests and examine cognitive, executive, emotional, personality, and neuropsychological functions comprehensively. Considering the scope of the evaluation, it is better to evaluate the clients in several sessions (two or three sessions). Then all the functions of the clients are given a score and all the scores are compared in a graph to determine what the best and worst functions of the clients are. It is suggested that the evaluation be done in three stages: before the treatment, in the middle of the treatment, and after the end of the treatment (Figure 1).
Considering the past and present efforts regarding psychotherapy for bipolar depression, designing a separate treatment for this disorder will bring new perspectives to researchers and therapists. With the help of previous theories about BD, designing a special treatment for BD, directly targets the problems of these patients, and takes steps to reduce the pain caused by this abnormality.
After patients have been comprehensively evaluated, functions improvement therapy can be used. This treatment covers all the functions and symptoms as well as the weak and strong points of the person. The treatment plan is based on the problems identified in the assessment phase. It is better to have short-term treatment in weekly sessions. In all stages, treatment is carried out individually. In each session, the materials of the previous session are reviewed and a review of assignments is also done.
Treatment should teach patients skills to manage their disorder. Treatment should cover both the depressive and mania phases. It is better for researchers and therapists, regardless of their theoretical approach, to evaluate this special type of treatment for BD so that the effectiveness of this treatment can be investigated in numerous studies. It is better to evaluate the effectiveness of this treatment compared to other treatments such as CBT and DBT. It is an eclectic therapy that uses techniques from other therapies in a framework that best fits BD.
According to the passage, the interaction of neurobiological, neuropsychological, and psychological factors (behavioral, cognitive, emotional, and personality) is involved in the development and persistence of BD. Indeed, nowadays, almost all researchers agree that BD is the result of many genetic and psychological interactions. Hence, investigators should consider various factors in the psychopathology and psychotherapy of BD. This selective review first reviewed research on these factors, then pointed to a variety of treatment models for BD (CBT, IPSRT, DBT, FFT, and MBCT), and finally proposed a new comprehensive integrated model for the evaluation and treatment of BD.
BD: bipolar disorder
CBT: cognitive behavioral therapy
DBT: dialectical behavior therapy
DSM: Diagnostic and Statistical Manual of Mental Disorders
FFT: family-focused therapy
IPSRT: interpersonal and social rhythm therapy
MBCT: mindfulness-based cognitive therapy
I would like to thank my colleagues and friends at “Amir Kabir Rehabilitation Center for the Disabled’’ in Kashan as well as “Social Welfare Department of the city of Kashan’’ for their intellectual assistance and thoughtful insights on an earlier draft of this paper.
BA: Conceptualization, Investigation, Methodology, Project administration, Writing—original draft, Writing—review & editing.
The author declares that he has no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Hans-Klaus Goischke
Claudia Vollbracht, Marc Werner
Bobbie Posmontier ... Tony Ma
Eloisa Ruiz-Marquez
Eloisa Ruiz-Marquez
Trevor R. Norman
Ayan Mohamud Yusuf, Dirk M. Hermann