 Original Article
Original Article

Affiliation:
Department of Preventive Medicine, Aldaitha Healthcare Center, Madinah Health Cluster, Ministry of Health, Madinah 42361, Saudi Arabia
Email: ahmed.a.a11@outlook.com
ORCID: https://orcid.org/0000-0001-8731-5213
Explor Neurosci. 2026;5:1006135 DOI: https://doi.org/10.37349/en.2026.1006135
Received: December 26, 2025 Accepted: March 22, 2026 Published: April 27, 2026
Academic Editor: Sheng-Tao Hou, Southern University of Science and Technology, China
The article belongs to the special issue The Science of Ischemic Stroke
Aim: Stroke represents a leading cause of mortality and disability globally, yet comprehensive epidemiological analyses for Saudi Arabia remain limited. This study aimed to analyze temporal trends in stroke incidence, mortality, and disability-adjusted life years (DALYs) in Saudi Arabia from 1990 to 2021, examine stroke subtype distributions and risk factor attributions, and compare findings with regional and international benchmarks.
Methods: We conducted a comprehensive analysis of the Global Burden of Disease (GBD) 2021 study data for Saudi Arabia, supplemented by systematic review findings and hospital-based registry data. Age-standardized incidence rates (ASIRs), mortality rates (ASMRs), and DALY rates were extracted for ischemic stroke, intracerebral hemorrhage, and subarachnoid hemorrhage. Annual percent change (APC) was calculated using Joinpoint regression. Risk factor attribution was analyzed using comparative risk assessment methodology. Poisson regression models examined sex differences.
Results: The pooled annual stroke incidence in Saudi Arabia was 29 per 100,000 population (95% CI: 15–47). Ischemic stroke predominated, comprising 79–87% of cases. Age-standardized DALYs showed significant yearly decreases of 9.28 per 100,000 (95% CI: 6.31–12.26, p < 0.001). The age-standardized death rate in the Middle East and North Africa (MENA) region was 87.7 per 100,000 [95% uncertainty interval (UI): 78.2–97.6] in 2019, representing a 27.8% regional decrease from 1990. Mean age at first stroke in Saudi Arabia was 63 years—six years younger than Western populations. Hypertension (57.7%), diabetes mellitus (49.4%), and obesity (42.0%) were the major modifiable risk factors. Intravenous thrombolysis utilization remained critically low at 1–3.6%.
Conclusions: Despite declining mortality and DALYs, Saudi Arabia faces a substantial stroke burden characterized by a younger onset age and significant treatment gaps. Achieving Vision 2030 health targets requires accelerated primary prevention addressing metabolic risk factors and expansion of acute stroke treatment capacity nationwide.
Stroke remains a critical global health challenge, ranking as the third leading cause of death worldwide with 7.3 million deaths in 2021 and the fourth leading cause of disability-adjusted life years (DALYs), accounting for 160.5 million DALYs [95% uncertainty interval (UI): 147.8–171.6] [1]. In the Middle East and North Africa (MENA) region, the epidemiological transition has substantially altered disease patterns, with non-communicable diseases (NCDs), including stroke, emerging as predominant causes of mortality and disability [2].
Saudi Arabia, the largest economy in the Gulf Cooperation Council (GCC), has undergone rapid socioeconomic development accompanied by significant lifestyle changes and population aging [3]. Cardiovascular diseases, including stroke, now account for 28% of all deaths in the Kingdom, with stroke specifically identified as the second leading cause of mortality after ischemic heart disease [4]. The unique demographic structure of Saudi Arabia—characterized by a relatively young population with increasing life expectancy—creates distinct epidemiological patterns that differ from Western populations [5].
Previous epidemiological studies have documented considerable variation in stroke incidence across Saudi regions, ranging from 15.9 to 57.6 per 100,000 population [6]. This heterogeneity reflects differences in study methodologies, regional healthcare infrastructure, and population demographics. A systematic review and meta-analysis reported a pooled annual incidence of 29 per 100,000, notably lower than in other high-income countries, though this estimate may understate the true burden given incomplete nationwide surveillance and the absence of a national stroke registry [7].
The Saudi Vision 2030 health transformation agenda has established ambitious targets for reducing NCD burden, aiming to decrease the standardized mortality rate from NCDs from 510 to 324 per 100,000 by 2030 [8]. Achieving these targets for stroke specifically requires a comprehensive understanding of temporal trends, risk factor distributions, and treatment gaps.
Despite growing recognition of stroke as a public health priority, knowledge gaps persist regarding long-term temporal trends, comparative burden across stroke subtypes, and progress toward international health targets. This study addresses these gaps by conducting a comprehensive analysis of stroke burden in Saudi Arabia, utilizing Global Burden of Disease (GBD) data spanning three decades, supplemented by regional registry data and systematic review findings. Our objectives were to: (1) analyze temporal trends in stroke incidence, mortality, and DALYs from 1990 to 2021; (2) examine distributions across stroke subtypes; (3) evaluate risk factor attributions; and (4) compare Saudi Arabiaʼs stroke burden with regional and international benchmarks.
This descriptive epidemiological study utilized multiple publicly available data sources. The primary dataset comprised the GBD 2021 study, accessed through the Institute for Health Metrics and Evaluation (IHME) Global Health Data Exchange (GHDx) [9]. The GBD study employs standardized methodology to estimate disease burden across 204 countries and territories using data from vital registration systems, verbal autopsy, surveillance, and published literature.
We extracted Saudi Arabia-specific estimates for three stroke categories defined by ICD-10 codes: ischemic stroke (I63), intracerebral hemorrhage (I61), and subarachnoid hemorrhage (I60). Variables included incident cases, deaths, prevalence, years of life lost (YLLs), years lived with disability (YLDs), and DALYs. All estimates included a 95% UI generated through 1,000 draws from posterior distributions.
Supplementary data were obtained from the World Health Organization Global Health Observatory, the Saudi General Authority for Statistics (GASTAT) mortality databases (2017–2022), and systematic reviews indexed in PubMed and Scopus [10]. Hospital-based data from the Eastern Province Stroke Register and multicenter studies provided validation and additional granularity [11].
The primary outcomes were age-standardized incidence rate (ASIR), age-standardized mortality rate (ASMR), and age-standardized DALY rate per 100,000 population. Secondary outcomes included YLLs, YLDs, and case fatality rates. Age standardization employed the GBD 2019 global standard population. Demographic stratification included sex, age groups (< 50, 50–69, ≥ 70 years), and nationality, where available.
Risk factor attribution utilized GBD comparative risk assessment methodology, which quantifies the population-attributable fraction of stroke burden associated with modifiable risk factors, including hypertension, diabetes, high body mass index (BMI), dietary risks, tobacco use, and ambient air pollution [12].
Temporal trends were analyzed using Joinpoint regression to identify years when significant changes in trend slope occurred and to calculate annual percent change (APC) with 95% confidence intervals (CIs). Poisson regression models with robust standard errors examined associations between demographic factors and stroke metrics, reporting incidence rate ratios (IRRs) with 95% CI.
Autoregressive integrated moving average (ARIMA) models were employed for forecasting 2020–2030 trajectories based on 1990–2019 trends [6]. Regional comparisons utilized World Health Organization regional groupings (MENA, GCC) and Socio-demographic Index (SDI) quintiles.
Heterogeneity in regional incidence estimates was assessed using I2 statistics from meta-analytic frameworks; the systematic review by Alqahtani and colleagues reported substantial heterogeneity (I2 = 98.8%) across included studies [7]. Statistical significance was defined as p < 0.05 (two-sided). Analyses were conducted using R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria) and Stata version 17.0 (StataCorp LLC, College Station, TX).
This study involved secondary analysis of publicly available, de-identified aggregate data and did not require institutional review board approval. The GBD 2021 study has received ethical approval from the University of Washington Institutional Review Board (STUDY00009060). Data from GASTAT are collected under the Statistics Law and are publicly accessible in aggregate form. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [13]. No patient-level data were accessed, ensuring participant confidentiality and data protection.
All data analyzed in this study are publicly available. GBD 2021 data are available from the IHME GHDx (https://ghdx.healthdata.org/gbd-results-tool). GASTAT mortality data are available at https://www.stats.gov.sa. WHO Global Health Observatory data are available at https://www.who.int/data/gho.
The pooled annual stroke incidence in Saudi Arabia was 29 per 100,000 population (95% CI: 15–47), derived from a meta-analysis of five eligible population-based studies [7]. Regional variation was substantial, ranging from 13.89 per 100,000 in Al-Madinah to 57.64 per 100,000 (95% CI: 57.3–57.9) in the Aseer region (Table 1). The high heterogeneity (I2 = 98.8%) across regional estimates reflects differences in study methodology, case ascertainment practices, and population demographics rather than uniform geographic distribution of disease [7].
Regional stroke incidence rates in Saudi Arabia.
| Region | Incidence per 100,000/year (95% CI) | Study period | Sample description |
|---|---|---|---|
| Aseer | 57.64 (57.3–57.9) | 2016 | Population = 2,166,983; n = 1,249 cases |
| Riyadh | 43.8 (not reported) | 1982–1992 | Hospital-based; n = 500 cases |
| Eastern Province | 29.8 (not reported) | 1994–1998 | Registry-based; first-ever strokes |
| Pooled national estimate | 29 (15–47) | 1982–2016 | Meta-analysis of 5 studies; I2 = 98.8% |
| Al-Madinah | 13.89 (not reported) | 2014 | Hospital-based registry |
Notes: CIs not reported for all studies. Very high heterogeneity (I2 = 98.8%) indicates that variation largely reflects differences in methodology and case ascertainment. The pooled estimate from Alqahtani et al. (2020) [7] represents the most robust national estimate. CI: confidence interval.
Temporal trend analysis revealed that ASIRs increased from 1990 to 2014, followed by a plateau through 2019. This pattern varied by stroke subtype: ischemic stroke showed a sustained increase from 1990 to 2014 before stabilizing; intracerebral hemorrhage increased from 2000 to 2012, then decreased through 2016; subarachnoid hemorrhage decreased from 1990 to 2002, remained stable until 2015, then showed a slight increase [6].
Sex-stratified analysis using Poisson regression demonstrated significantly higher ischemic stroke incidence in females compared to males (IRR: 1.21, 95% CI: 1.16–1.26, p < 0.001). Subarachnoid hemorrhage similarly showed female predominance (IRR: 1.35, 95% CI: 1.15–1.58, p < 0.001). No significant sex difference was observed for intracerebral hemorrhage (IRR: 1.01, 95% CI: 0.94–1.09, p = 0.800) [6].
Intracerebral hemorrhage accounted for 10.6–21.4% of cases in the majority of published Saudi series, while subarachnoid hemorrhage was notably rare at 1.4–2.4% [7, 14]. The Eastern Province Registry documented ischemic stroke at 69%, intracerebral hemorrhage at 29.6%, and subarachnoid hemorrhage at 1.4% [11]. The higher ICH proportion reported in the Eastern Province Registry (29.6%) likely reflects referral bias toward neurosurgical intervention at that center.
Among ischemic stroke subtypes classified by TOAST criteria, large vessel disease (52%) and lacunar infarctions (21–24.2%) predominated. In young stroke patients (< 50 years), small vessel occlusion was most frequent (31.7%), followed by cardioembolism (19%) and cryptogenic stroke (19%) [15].
The age-standardized death rate from stroke in the MENA region was 87.7 per 100,000 (95% UI: 78.2–97.6) in 2019, with Saudi Arabia positioned among higher-burden countries within its SDI subgroup [2]. Stroke accounted for approximately 11.7% of total deaths in Saudi Arabia, representing the second leading cause after ischemic heart disease [4].
Temporal analysis demonstrated a 27.8% decrease in the MENA regionʼs age-standardized mortality from 1990 to 2019, while total stroke deaths in Saudi Arabia increased by 193.33% over the same period (from 480 to 1,408 deaths), reflecting population growth despite improving age-standardized rates (Table 2) [2]. The overall stroke case fatality rate in Saudi hospital-based studies was 27%, exceeding rates reported in other Middle Eastern countries [6]. Case fatality rates varied by setting: 30-day mortality ranged from 11.1–15%, while one-year mortality reached 26.9% [7].
Temporal trends in stroke burden metrics, Saudi Arabia and MENA region (1990–2019/2021).
| Metric | 1990 value | 2019/2021 value | Percent change |
|---|---|---|---|
| Age-standardized death rate (MENA) | 121.5/100,000 | 87.7/100,000 | –27.8% |
| Age-standardized DALYs (MENA) | — | — | –32.0% |
| Smoking-attributable DALYs (KSA) | 219.06/100,000 | 170.02/100,000 | –22.4% |
| Smoking-attributable YLLs (KSA) | 207.44/100,000 | 157.81/100,000 | –24.15% |
| Smoking-attributable deaths (KSA) | 7.69/100,000 | 5.53/100,000 | –28.48% |
| Total stroke deaths (KSA) | 480 | 1,408 | +193.33% |
Sources: Shahbandi et al. (2022) [2] for MENA data; Alqahtani et al. (2025) [17] for smoking-attributable Saudi Arabia data. MENA and KSA figures are distinct and not directly comparable. Increase in total deaths reflects population growth despite declining age-standardized rates. The 95% UI for age-standardized death rate in 2019 was 78.2–97.6 per 100,000. —: data not available for the specified time point. MENA: Middle East and North Africa.
In-hospital mortality in the Aseer region was 9.7% (121 of 1,249 hospitalized patients) [16]. The population-level in-hospital stroke mortality rate for that study catchment area was 5.58 per 100,000 per year.
Saudi Arabia-specific age-standardized DALY rates showed a consistent decline over the study period. Analysis demonstrated that each passing year was associated with a decrease of 9.28 DALYs per 100,000 (95% CI: 6.31–12.26, p < 0.001) [6]. At the MENA regional level, the percentage change in age-standardized DALYs from 1990 to 2019 was –32.0% (95% UI: –39.1 to –23.3) [2].
YLLs contributed the majority of stroke DALYs, representing approximately 93% of the total burden in 2021. Analysis of smoking-attributable stroke burden in Saudi Arabia revealed that age-standardized DALYs decreased by 22.4% from 1990 to 2021, with an average APC of –0.85 (95% CI: –0.88 to –0.83) [17].
Despite improvements in age-standardized rates, Saudi Arabia demonstrated higher-than-expected stroke DALYs relative to its SDI level, suggesting an opportunity for improvement compared to countries with similar levels of socioeconomic development [2]. ARIMA forecasting models predicted a continued gradual increase in age-standardized incidence through 2030, while DALYs were projected to show a sustained decrease [6].
Analysis of modifiable risk factors in Saudi stroke patients revealed a high prevalence of metabolic risk factors (Table 3). In the largest multicenter case-control study (n = 2,498), hypertension was present in 57.7% of stroke cases versus 31.8% of controls (adjusted OR: 2.12, 95% CI: 1.74–2.57). Diabetes mellitus affected 49.4% of cases versus 25.9% of controls (adjusted OR: 1.73, 95% CI: 1.41–2.21). Obesity (BMI ≥ 30) was documented in 42.0% of cases (adjusted OR: 1.95, 95% CI: 1.61–2.28), and hypercholesterolemia in 29.4% (adjusted OR: 1.64, 95% CI: 1.28–2.10) [18].
Risk factor prevalence in Saudi stroke patients compared with controls [18].
| Risk factor | Cases n (%) | Controls n (%) | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|---|---|
| Hypertension | 721 (57.7%) | 397 (31.8%) | 2.93 (2.48–3.45) | 2.12 (1.74–2.57) |
| Diabetes mellitus | 617 (49.4%) | 323 (25.9%) | 2.80 (2.36–3.31) | 1.73 (1.41–2.21) |
| Obesity (BMI ≥ 30) | 525 (42.0%) | 385 (30.8%) | 1.63 (1.38–1.92) | 1.95 (1.61–2.28) |
| Hypercholesterolemia | 367 (29.4%) | 151 (12.1%) | 3.30 (2.45–3.73) | 1.64 (1.28–2.10) |
| Current smoking | 128 (10.3%) | 113 (9.0%) | 1.15 (0.88–1.50) | NS |
| Physical inactivity | 1,085 (86.9%) | 875 (70.1%) | Ref | Ref |
| Regular exercise | 164 (13.1%) | 374 (29.9%) | 0.35 (0.29–0.43) | 0.12 (0.05–0.26)† |
Multicenter case-control study, Aseer region, n = 2,498 (1,249 first-time stroke cases and 1,249 matched controls). †The magnitude of this association should be interpreted cautiously; see Discussion. BMI: body mass index; OR: odds ratio; CI: confidence interval; NS: not significant; Ref: reference category (physical inactivity used as the comparator group for the physical activity analysis).
The GBD comparative risk assessment identified Saudi Arabia as having the highest proportion globally (6.89%) of stroke DALYs attributable to high fasting plasma glucose, reflecting the exceptionally high diabetes prevalence in the Kingdom [2]. High BMI emerged as the most important attributable risk factor in Saudi Arabia, Qatar, and the United Arab Emirates (UAE) among GCC nations.
Physical inactivity was highly prevalent (86.9%) among stroke cases. Regular exercise was associated with substantially lower stroke odds (adjusted OR: 0.12, 95% CI: 0.05–0.26) [18]. While this finding is directionally consistent with the broader literature on the protective role of physical activity in stroke prevention, the magnitude of this association and its wide CIs should be interpreted with caution, given that it derives from a single regional case-control study and may be subject to residual confounding or recall bias. Current smoking was prevalent at 10.3% among stroke cases but did not reach statistical significance as an independent risk factor (OR: 1.15, 95% CI: 0.88–1.50).
Critical gaps in acute stroke treatment were identified (Table 4). Intravenous thrombolysis (IV tPA) utilization remained extremely low at 1–3.6% of eligible ischemic stroke patients in urban Saudi centers [19]. By comparison, US national IV tPA utilization rates improved from approximately 6.5% in the mid-2000s to 8–10% nationally by 2013, with comprehensive stroke centers exceeding this threshold [19, 20]. The treatment gap between Saudi Arabia and international benchmarks is therefore wider than historical comparisons suggest.
Stroke treatment patterns and outcomes in Saudi Arabia.
| Treatment metric | Value | Study details |
|---|---|---|
| IV thrombolysis utilization (urban) | 1–3.6% | National estimates; US national rate ~8–10% [20] |
| Thrombolysis/thrombectomy (PCS) | 22.4% | n = 160 patients; PCS |
| EVT successful recanalization | 84.8% | n = 369 patients; anterior circulation |
| EVT good outcome (mRS 0–2 at 90 days) | 41% | Single-center experience, 2015–2022 |
| EVT mortality | 22.4% | Same cohort as above |
| Barrier: Late ED arrival | 77% | Analysis of thrombolysis exclusions |
| Barrier: Recent anticoagulation | 34% | Same cohort |
| 30-day case fatality rate | 11.1–15% | Hospital-based studies |
| 1-year mortality | 26.9% | Tertiary center data |
| In-hospital mortality | 9.7% | n = 1,249 cases, Aseer region |
| Stroke unit admission rate | ~5% | National estimate |
| Active stroke centers (thrombolysis) | 7 | Out of > 350 hospitals nationally |
Treatment gaps represent a major opportunity for outcome improvement. IV: intravenous; PCS: posterior circulation stroke; EVT: endovascular thrombectomy; mRS: modified Rankin Scale; ED: emergency department.
Analysis of barriers to thrombolysis revealed that 77% of exclusions were attributable to delayed emergency department arrival beyond the treatment window. Anticoagulant use within 48 hours accounted for 34% of exclusions, while recent prior stroke (7%) and uncontrolled hypertension (6%) represented additional contraindications (Figure 1) [21].
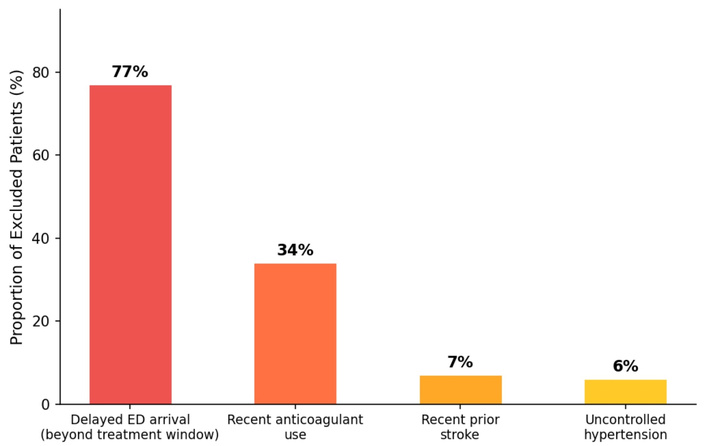
Barriers to intravenous thrombolysis among acute ischemic stroke patients in Saudi Arabia [21]. Categories represent the proportion of thrombolysis-excluded patients with each documented barrier; categories are not mutually exclusive. Delayed emergency department arrival—beyond the therapeutic window—accounts for 77% of exclusions, underscoring the need for population-level awareness campaigns on stroke symptom recognition and rapid response. ED: emergency department.
In a study of posterior circulation stroke, only 22.4% of patients received thrombolysis and/or thrombectomy [22]. Endovascular thrombectomy experience from a single center (n = 369 patients) demonstrated successful recanalization in 84.8% of anterior circulation strokes, with good functional outcome (modified Rankin Scale 0–2 at 90 days) achieved in 41% and mortality of 22.4% [23]. SITS-MENA Registry data showed that Saudi stroke patients were younger (median age 55 vs. 73 years globally) but presented with more severe strokes (NIHSS 12 vs. 9) and higher diabetes prevalence [24].
Saudi Arabia showed distinct patterns compared with GCC neighbors and international benchmarks. Mean age at first stroke in Saudi Arabia was 63 years, compared to 69 years in the United States and approximately 70 years in the United Kingdom, reflecting premature disease onset in the Saudi population [1, 5].
Among GCC countries from 1990 to 2021, Qatar achieved a 59.9% decrease and the UAE a 50% decrease in age-standardized stroke death rate (best performers), while Kuwait showed a 14.4% increase and Saudi Arabia a modest decrease of only 0.59% (Figure 2) [25]. Saudi Arabia contributed approximately 45% of GCC stroke deaths, 49% of years of potential life lost, and 60% of the regionʼs NCD-related economic losses—estimated at USD 50 billion annually, equivalent to 3.3% of GCC GDP [25].
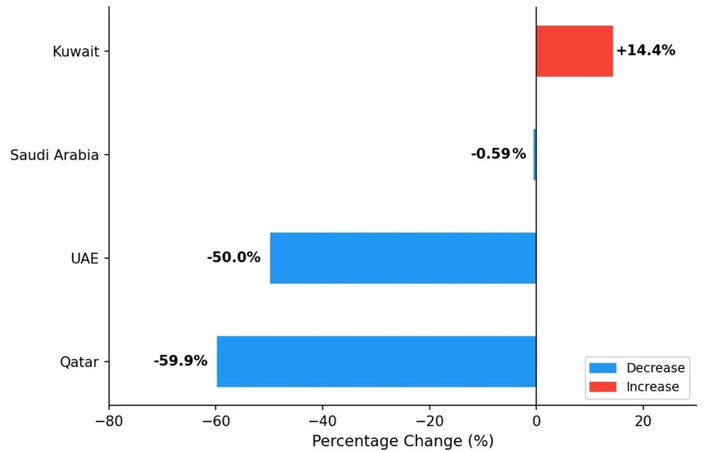
Percentage change in age-standardized stroke death rate among selected GCC countries, 1990–2021 [25]. Blue bars indicate countries with decreasing rates; the red bar indicates Kuwait with an increasing rate. Saudi Arabiaʼs –0.59% change contrasts markedly with Qatar (–59.9%) and the UAE (–50%), highlighting comparatively limited progress in stroke mortality reduction. GCC: Gulf Cooperation Council; UAE: United Arab Emirates.
The GCC region overall showed substantially higher obesity prevalence compared to the global average, with over 70% of Saudi adults classified as overweight or obese, particularly among women [25].
This comprehensive analysis of stroke burden in Saudi Arabia reveals important epidemiological patterns with significant public health implications. Despite encouraging declines in the MENA region age-standardized mortality (–27.8%) and DALYs (–32.0%) from 1990 to 2019, several findings warrant urgent attention.
The pooled Saudi incidence of 29 per 100,000—while lower than many high-income countries—likely underestimates the true burden due to incomplete case ascertainment in the absence of a national stroke registry. The very high heterogeneity (I2 = 98.8%) and regional variation from 13.89 to 57.64 per 100,000 partly reflect methodological differences rather than genuine geographic heterogeneity, as documented by Alqahtani and colleagues [7].
The younger age at stroke onset in Saudi Arabia (mean 63 years) compared to Western populations (69–70 years) has profound implications for societal and economic impact. This six-year difference translates to greater years of potential productivity lost and extended disability burden. The high prevalence of diabetes (49.4%) and obesity (42.0%) among stroke patients reflects broader population trends and contributes to premature disease onset [18].
Among MENA region countries within its SDI subgroup, Saudi Arabia demonstrated the highest proportion of stroke DALYs attributable to high fasting plasma glucose (6.89%), reflecting the exceptionally high diabetes prevalence in the Kingdom [2]. The Vision 2030 health transformation agenda appropriately targets metabolic risk factors, but implementation must be accelerated to achieve the NCD mortality reduction target of 324 per 100,000 [8].
The critically low thrombolysis rates (1–3.6%) represent perhaps the most actionable finding. As illustrated in Figure 1, delayed presentation accounts for 77% of thrombolysis exclusions, underscoring the urgent need for public awareness campaigns targeting symptom recognition and emergency response. Saudi Arabia has only seven centers providing thrombolysis among over 350 hospitals, with stroke unit admission rates of approximately 5% [19]. Updated benchmarking against US centers—where IV tPA rates have risen to 8–10% nationally and exceed 10–15% at comprehensive stroke centers—confirms that the Saudi treatment gap is substantial and widening rather than narrowing [20]. The SITS-MENA Registry evidence demonstrates that when patients access treatment, outcomes are comparable to international benchmarks, supporting investment in healthcare system strengthening [24].
The association between regular exercise and reduced stroke risk (adjusted OR: 0.12) observed in the case-control study by Alhazzani and colleagues [18] is directionally consistent with meta-analyses from higher-income settings. However, the unusually strong magnitude of this protective effect—stronger than most published estimates—likely reflects the specific characteristics of this single regional study population, including potential healthy-user bias and recall bias in a case-control design. This finding provides supportive, rather than definitive, evidence for community wellness initiatives and should not be generalized without corroboration from additional Saudi studies or pooled analyses.
Comparison with GCC neighbors provides important context. While Qatar achieved 59.9% and the UAE 50% mortality reduction from 1990 to 2021, Saudi Arabiaʼs more modest progress (–0.59%) highlights considerable opportunity for improvement. These findings demonstrate that substantial reductions in stroke mortality are achievable within the GCC region and underscore the need for accelerated intervention in Saudi Arabia [25].
Regarding the higher-than-expected stroke burden relative to Saudi Arabiaʼs SDI level, it is important to note that this analysis relied on GBD SDI quintile comparisons without performing Saudi-specific SDI adjustment. Future analyses incorporating country-specific development trajectories may provide more precise quantification of this excess burden.
The data from 2020 to 2021 should be interpreted with particular caution given the COVID-19 pandemic, which affected healthcare utilization patterns, emergency presentations, and vital registration completeness across the MENA region during this period. These effects may have introduced bias into GBD estimates for the most recent years.
Strengths of this study include utilization of standardized GBD methodology enabling international comparisons, comprehensive temporal coverage spanning three decades, and synthesis of multiple data sources including registry and systematic review data.
Several limitations must be acknowledged. GBD estimates for Saudi Arabia are modeled based on incomplete vital registration data, potentially affecting precision. The very high heterogeneity across regional studies (I2 = 98.8%) limits the interpretability of the pooled incidence estimate. Regional studies employ heterogeneous methodologies, further limiting direct comparisons. The absence of a national stroke registry prevents precise population-based surveillance. Hospital-based studies may underestimate mild strokes not presenting to healthcare facilities. Expatriate populations (approximately 38% of Saudi Arabiaʼs population) are variably included in surveillance systems, potentially biasing national estimates. No Saudi-specific SDI adjustment was performed, limiting comparative burden analysis. Finally, the COVID-19 pandemic may have influenced GBD estimates for 2020–2021, and post-pandemic data should be analyzed as they become available.
Achieving Vision 2030 stroke-related targets requires a multi-pronged intervention. Primary prevention must address the exceptionally high metabolic risk factor prevalence through population-based dietary interventions, physical activity promotion, and diabetes screening and management programs. Secondary prevention requires expanding stroke treatment capacity through the establishment of additional primary stroke centers, public awareness campaigns emphasizing stroke symptom recognition and urgent presentation, and telemedicine networks connecting rural facilities to expert consultation. The current treatment gap represents preventable deaths and disability.
Tertiary prevention and rehabilitation services require development to address the growing population of stroke survivors. With 93% of DALYs attributable to YLLs rather than YLDs, mortality reduction remains paramount, but disability management will become increasingly important as survival improves.
Establishing a nationwide stroke registry should be prioritized to enable accurate surveillance, quality improvement, and evaluation of intervention effectiveness. The Eastern Province Registry experience demonstrates feasibility in the Saudi context [11].
Stroke burden in Saudi Arabia demonstrates encouraging declining trends in mortality and DALYs, yet substantial challenges persist. The younger onset age, high metabolic risk factor prevalence, and critically low treatment utilization rates represent urgent public health priorities. Saudi Arabiaʼs higher-than-expected burden relative to its socioeconomic development level—compounded by a treatment infrastructure gap that has grown relative to international benchmarks—indicates considerable room for improvement. Achieving Vision 2030 health targets will require accelerated implementation of primary prevention strategies targeting diabetes and obesity, substantial expansion of acute stroke treatment infrastructure, and the establishment of comprehensive national surveillance systems.
APC: annual percent change
ARIMA: autoregressive integrated moving average
ASIR: age-standardized incidence rate
ASMR: age-standardized mortality rate
BMI: body mass index
CIs: confidence intervals
DALYs: disability-adjusted life years
GASTAT: Saudi General Authority for Statistics
GBD: Global Burden of Disease
GCC: Gulf Cooperation Council
GHDx: Global Health Data Exchange
IHME: Institute for Health Metrics and Evaluation
IRRs: incidence rate ratios
IV tPA: intravenous thrombolysis
MENA: Middle East and North Africa
NCDs: non-communicable diseases
SDI: Socio-demographic Index
UAE: United Arab Emirates
UI: uncertainty interval
YLDs: years lived with disability
YLLs: years of life lost
AAA: Conceptualization, Investigation, Formal analysis, Visualization, Writing—original draft, Writing—review & editing. The author read and approved the submitted version.
The author declares that there are no conflicts of interest.
This study involved secondary analysis of publicly available, de-identified aggregate data and did not require institutional review board approval. No individual patient-level data were accessed at any stage of the analysis. All procedures were conducted in accordance with the principles of the Declaration of Helsinki. The Global Burden of Disease Study 2021 data utilized in this study were collected under ethical approval from the University of Washington Institutional Review Board (STUDY00009060). Data from the Saudi General Authority for Statistics are collected under the authority of the Statistics Law and are publicly accessible in aggregate form.
Not applicable. This study utilized only de-identified, publicly available aggregate data with no involvement of individual participants.
Not applicable.
All data analyzed in this study are publicly available. Global Burden of Disease Study 2021 data are available from the Institute for Health Metrics and Evaluation Global Health Data Exchange (https://ghdx.healthdata.org/gbd-results-tool). Saudi General Authority for Statistics mortality data are available at https://www.stats.gov.sa. World Health Organization Global Health Observatory data are available at https://www.who.int/data/gho.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1379
Download: 26
Times Cited: 0
