Review
Review

Affiliation:
Division of Surgery and Interventional Science/Pain Management, University College of London, WC1E 6BT London, England
Email: kate.tordoff.22@ucl.ac.uk
ORCID: https://orcid.org/0009-0004-8755-300X
Affiliation:
Division of Surgery and Interventional Science/Pain Management, University College of London, WC1E 6BT London, England
ORCID: https://orcid.org/0000-0002-2859-8548
Affiliation:
Division of Surgery and Interventional Science/Pain Management, University College of London, WC1E 6BT London, England
ORCID: https://orcid.org/0009-0006-8236-6015
Affiliation:
Division of Surgery and Interventional Science/Pain Management, University College of London, WC1E 6BT London, England
ORCID: https://orcid.org/0000-0002-6776-2777
Explor Neurosci. 2026;5:1006129 DOI: https://doi.org/10.37349/en.2026.1006129
Received: September 05, 2025 Accepted: March 02, 2026 Published: March 18, 2026
Academic Editor: Dirk M. Hermann, University of Duisburg-Essen, Germany
Chronic pain, defined as pain persisting beyond 12 weeks, is known to be challenging to manage. Despite increasing opioid prescribing, pain is still an issue for many patients. Patient education has emerged as a key element in supporting self-management and improving pain-related outcomes. This narrative review explores the impact of patient education alongside pain management interventions, with a focus on pain intensity, pain-related beliefs, and pain-related disability. A structured search using PubMed, Medline, EBSCOhost, and UCL Explore identified ten studies (six RCTs, two systematic reviews, two cohort studies) and three national guidelines meeting the inclusion criteria. Inclusion criteria focused on adult patients with chronic non-malignant pain who received some form of education alongside or prior to pain interventions. Pain education was associated with 29% reduction in opioid use, with 7% patients discontinuing opioids entirely in the usual group. Improvements in emotional functioning (41%), pain understanding (75%), and overall functioning (38%) were observed across various trials. Existing research shows promising results; however, the clarity of the type of education needed needs to be established. Short, focused education sessions, especially those incorporating pain neuroscience education (PNE) or cognitive behavioural therapy (CBT) elements, were as effective as longer programs. Further research is required to identify how education improves the outcome of pain management interventions. Integrating targeted patient education into the chronic pain care pathway can significantly reduce disability, improve quality of life, and decrease opioid reliance. These findings support implementing structured education sessions as part of routine pain management services to enhance long-term patient outcomes.
Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage [1]. Acute pain provides a protective role; persistent pain, lasting longer than three months, often has no beneficial function [2]. Persistent pain may arise from various causes but continues beyond normal healing. It can be complex and is often influenced by biological, psychological, and social factors [3].
Pain interventions include both physical and psychological strategies, for example, heat/cold therapy, pharmacology, nerve blocks, cognitive behavioural therapy (CBT), acceptance commitment therapy (ACT), and mindfulness [4, 5]. Psychological interventions may be required if medical interventions have failed or if the patient’s pain is complex. Education plays a critical role in delivering these approaches by improving patient understanding of pain mechanisms and encouraging self-management behaviours.
Pain education aims to explain the neurobiology of pain and improve their understanding of pain and its triggers. Education can be delivered in many ways, including group or one-to-one sessions consisting of flare-up plans, pacing, and coping strategies. A greater understanding of pain can help change an individual’s thoughts about pain and promote self-efficacy and coping [6]. It’s essential that the multidisciplinary team (MDT) highlight education in combination with other interventions. Education is especially important in chronic conditions like fibromyalgia, which present significant challenges [7].
The current National Institute for Health and Care Excellence (NICE) guidelines [3] suggest multiple influences on persistent pain, including health conditions, trauma, stress, substance misuse, lifestyle, housing, income, and social support, see Table 1.
Influential factors of chronic pain.
| Biological | Psychological | Social |
|---|---|---|
| Health conditionComorbiditiesPhysical wellbeing | Stressful life eventsEmotional traumaPhysical traumaCurrent or history of substance misuse | LifestyleDay-to-day activitiesWork patternsHousingIncomeSocial/Family support |
Additionally, these factors shape patients’ experience, interpretation, and coping with chronic pain. Understanding these dimensions is vital to developing personalised pain management plans [3].
In the UK, chronic pain affects up to 53% of people aged 75 years and older, with notable prevalence in adults aged 16–34 (18%) years, and 30% higher burden observed in women [8]. It is estimated to affect nearly 8 million people in the UK and costs the economy over £10 billion in sickness absence [9]. With a predicted growth of 32% by 2040, persistent pain poses a significant pressure on the health care system [10], with primary care management for persistent pain accounting for 4.6 million appointments [11]. National Pain Audits also show a high level of disability and distress in pain clinic patients [12]. It is worrying that 50% of the patients attending pain clinics in England still lacked understanding or acceptance of their persistent pain 12 months after beginning treatment [13]. The Faculty of Pain Medicine in the UK suggests that people with persistent pain require specialist input [14].
The concept of access to pain management as a human right is arguably being discussed as one of the integral components of the Universal Health Coverage [15]. Interventions like spinal or localised injections are used to reduce pain and enable rehabilitation [14].
Pain is a subjective experience, heavily affected by physical, psychological, and social factors. The use of pharmacological treatments is common in chronic pain management. Pain can derive from inflammation, trauma, injury, disease, or nerve damage; therefore, pharmacology can reduce symptoms associated with pain. The severity and nature of the pain determine the choice of pharmacology. NICE recommends the use of antidepressants after a full discussion of the benefits and harmful risks to the patient. The intended benefits are to improve sleep, psychological distress, pain, and quality of life. NICE advises against most pharmacological treatments due to insufficient evidence of benefit and risk of harm. Long-term opioid use is linked to increased opioid overdose, abuse, and harm, risk of myocardial infarction, sexual dysfunction, and fractures [16].
The International Association for the Study of Pain advises that self-management is the ‘first rung of the ladder in pain care’ and that ‘educational processes of successful self-management programmes are typically grounded in social, cognitive and behavioural theories’ [17]. Providing evidence-based education for chronic pain, it is anticipated that the individual gains:
a better understanding of pain in general,
improved understanding of the function of pain,
understand what options are available for their pain management.
Self-management can reduce the physical and psychological burden of pain; however, the evidence also shows a lack of effect, likely due to facilitator skills. Pain neuroscience education (PNE), mindfulness, distraction techniques, flare-up plans, relaxation, pacing, and pain mechanisms are often delivered through an MDT approach.
NICE recognises the importance of providing advice and education, which should be relevant and individualised. Symptom recurrence, flare-ups, the possibility that pain may not improve and may require ongoing management, and quality of life improvement must be discussed. Shorter education sessions may be more effective as they are easier to implement with staffing, patient uptake, and National Health Service (NHS) costs.
Psychological therapies are recommended as part of pain pathways. Psychology relates directly to the prediction and control of behaviour [18]. In the case of chronic pain, behaviour can be impacted by thoughts and feelings, exacerbating pain. Pain, disability, and distress could be reduced by developing coping skills.
Identifying negative thought patterns is believed to potentially influence behaviour [19]. ‘Explain Pain’ [20] applies the biopsychosocial model to pain and acknowledges that pain is modulated by beliefs and behaviour.
Mindfulness increases awareness of breathing, positive image thoughts, visualisation, and relaxation [21]. By reducing the sensitivity and perception of pain and the associated distress, pain-related disability can support self-care and reduce anxiety and pain intensity.
The British Pain Society proposes that Pain Management Programmes (PMPs), which are psychologically led-based, rehabilitative programmes for patients with unresolved chronic pain, can improve quality of life by teaching physical, practical, and psychological techniques. However, the primary goal is not to improve pain, but improvements have been noted [22].
Chronic pain can have a wider impact on an individual’s mental health. Anxiety, depression, and reduced functional ability may cause frustration and anger, leading to a potential mental health crisis. Up to 18–50% of patients with persistent pain have suicidal ideation [23].
Pain-related disability significantly impacts public health, causing additional pressures on the healthcare system. The fear-avoidance model of pain has been linked to pain-related disability. Zale and Ditre [24] suggest that treatments that reduce pain-related fear are effective at improving pain-related disability. The biopsychosocial model of pain implies that biology, environmental factors, beliefs, understanding, and cognition influence pain disability.
With this in mind, ‘chronic pain patients’ poorer quality of life suggests poor pain management, perhaps due to failure to recognize the multidimensional nature of chronic pain’ [25] perhaps to improve pain management for the patient, and consider the multidimensional aspect of pain, and its impact on the biopsychosocial factors, pain management ‘strategies should focus on improving patients’ quality of life’ [25]. Incorporating self-management approaches could improve overall well-being and improve an individual’s quality of life.
Recommendations by NICE are centred around self-management, including psychological therapies, exercise programmes, advice, and creating flare-up plans. Patient-centred assessments are paramount, and education about what pain is and why it happens may help to change individual perceptions and behaviours.
In recent years, the NICE has updated its guidelines for chronic pain, causing concern across this patient cohort. Specifically, recommending only the use of antidepressants for pharmacological management, acupuncture, psychological therapy, or group-based exercise. Further suggesting that those taking other medications are reviewed as part of ‘shared decision making’, NICE acknowledges that individual chronic pain assessment and management is required [22].
By reviewing its clinical value, this study seeks to highlight opportunities to improve care for patients living with persistent pain. Specifically focusing on the benefit of patient education for chronic pain interventions and management, and its impact on pain-related disability.
Pain is subjective and often influences function, measuring the severity of pain and its impact. Various pain scales are used in acute settings, consisting of numerical, verbal, and visual scoring systems. When measuring chronic pain, it is important to consider the impact the pain is having on an individual’s function and quality of life. The British Pain Society [26] has published a report for pain outcome measures, including outcome measures that not only assess the pain rating but also the impact on interference, such as the Roland and Morris Disability Index, which is only suitable for low back pain and contains sentences that describe different movement and functions. The Brief Pain Inventory (BPI) assesses physical functioning, and the impact pain has on daily living, pain scores, the location of the pain, and the amount of analgesia in the past 24 hours. This outcome tool can be widely used for both chronic and acute pain, and also for cancer pain. The EQ5D5L assessment tool is a patient-reported outcome measure (PROM) capturing five dimensions of quality of life, including mobility, self-care, usual activities, pain/discomfort, and anxiety and depression. The patient global impression of change (PGIC) scale measures improvement or deterioration since a pre-defined point of time, to assess an overall impression of change.
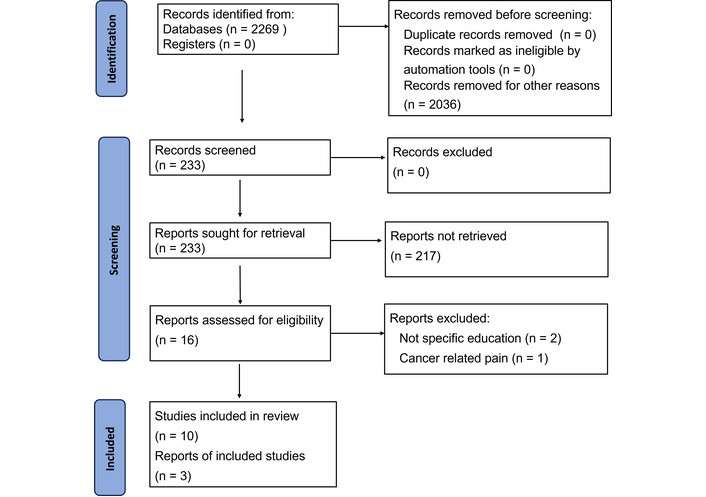
Using the databases PubMed, Medline, EBSCOhost, and UCL Explore, a literature search was conducted using the search terms: ‘education’, ‘patients’, ‘chronic pain’, ‘disability’, ‘intervention’, ‘education session’, ‘improve disability’, ‘education before intervention for chronic pain’, ‘opioids’. Papers were selected from PubMed after an initial search, as the papers were then relevant to medical studies. See Table S1 for full search terms.
Using these search terms, literature was collected and ascertained as to whether they fit into the inclusion criteria. Expanding the database for future research would enhance comprehensiveness.
Figure 1 identifies the data search process undertaken to identify relevant papers that met the inclusion criteria. Table 2 consists of the inclusion criteria and exclusion criteria used during the search process. The risk of bias was not assessed during the study selection because the aim was to provide a broad overview of existing literature; additionally, the aim was not to critically analyse the subject.
Inclusion and exclusion criteria for data search.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Papers between 2003 and 2023 | Non-chronic pain |
| Adult patients over the age of 18 | Papers from before 2003 |
| Full text available | Non-English text papers |
| English language text | Pain related to the child |
| Human studies | Cancer-related pain |
| Including systematic reviews, policies, and guidelines |
Further guidelines were also included in the review from the NICE, the Faculty of Pain Medicine, and the British Pain Society. Including additional guidelines broadened the evidence regarding pain management and education, and reflects current practice and advice.
Education varied in style and form. Explain Pain [27] education showed significant differences (P < 0.001) in pain neurophysiology knowledge with pain physiology education, compared to pacing education and self-management. ‘Explain Pain’ education also helped to reduce catastrophising amongst participants. Reduced pain thresholds were observed with pain physiology and self-management education over time [28].
Additional education (pain physiology) showed an increased understanding of pain and less reported ruminating. Reports suggest that those who catastrophise struggle with concentration and memory problems, and comprehension is not guaranteed.
The pain stage of change questionnaire (PSOCQ) is a validated self-report tool that identifies the willingness to adopt a self-management approach. This was used in one study [29] to identify if pain outcomes, including pain knowledge, catastrophising, and disability, changed. In-depth PNE-based education significantly improved pain-related outcomes, which included self-perceived disability and catastrophising, and improved pain knowledge. There were weakly positive (but significant) correlations found between the changes in PSOCQ and changes in catastrophising (P = 0.01), suggesting that higher reductions in pre-contemplation levels have larger reductions in catastrophism. Patients with longer-term pain had more negative experiences, demonstrating smaller changes in disability.
Empowered relief education, consisting of pain relief skills, showed no inferiority compared with 16 hours of CBT for catastrophising 3 months after education. But it was superior to health-education (nutrition, medication education) at 3 months (P < 0.001). CBT was proven to be more effective for reducing catastrophising than health education [30]. Pain intensity and interference at 3 months, empowered relief (pain-relief education) was non-inferior to CBT, and also non-inferior for sleep, depression, anxiety, and pain behaviour, suggesting no specific type of education improves pain-related outcomes if offered prior to other intervention [30].
Education after an initial intervention for pain had positive results. Education, including a self-help booklet about pain, opioids, and opioid tapering, led by nurses and an opioid experienced lay person, was effective at reducing opioid use. Group education on mindfulness-oriented and medication-cognitive behavioural approaches was effective at opioid reduction [31]. Additionally, 1:1 support improved mental health (Hospital Anxiety and Depression Scale) and quality of life (EQ5D5L).
Intensive education added to initial treatment to improve pain outcomes after injury had positive long-term results. Explain Pain [27], concentrating on the biopsychosocial element of pain, or placebo education, which provided no additional information or education, had no impact initially on pain intensity. However, results suggested that at 3 months and 12 months after ‘Explain Pain’ education, pain intensity reduced [32].
Results by Meeus et al. [28] were comparable to a randomised controlled trial (RCT) by Moseley et al. [33], which investigated neurophysiology education for chronic low back pain (CLBP). Three hours of intensive neurophysiology education and workbooks were provided. Patients had an increased understanding of pain and reported less catastrophising with education on pain physiology compared to only self-management education. Pamphlet-based education to improve coping, positive thinking, and back pain resources had no significant improvement for pain experiences (P < 0.05). CBT had the same results [34]. There were some in-group improvements related to pain-free days, but there was no significance between group differences.
Education reduced patient-reported use of opioids by 29% with educational interventions compared with 7% without the additional education, which shows group-based education significantly reduced opioid use [31]. Educational interventions were also beneficial, with 48% outcomes with medications by utilising video educational tools and counselling, although they were most unsuccessful for chronic pain [35]. Meditation-CBT education had no significant reduction in opioid use [36] for patients treated with high-dose opioids, suggesting a lack of efficacy of opioids for chronic pain.
Varied results were noted for education and quality of life improvements [31]. Significant improvements with mental health (Hospital Anxiety and Depression Scale), health-related quality of life (EQ5D5L), and visual analogue scale were noted at 4 months after CBT-mindfulness education, but there was no statistical significance with sleep quality. However, education did not reduce depressive symptoms of global impression of change, but did help reduce catastrophising and unhelpful beliefs [32]. However, education is offered for acute pain, suggesting the timing of education could impact quality-of-life improvements.
Pain experience improved with CBT and pamphlet education (P < 0.05), but there was no decrease when comparing education type [34]. Pain-free days improved (P < 0.005) with CBT, coping skills, and maintaining good posture, but no significant difference between group data. Pamphlet-based education significantly improved catastrophising, and fear avoidance decreased with education. Further studies could identify which form of education is superior at improving the quality of life.
CBT was found to reduce catastrophising more than health education [30]. Sleep, depression, anxiety, and pain behaviour were not worse with CBT. This shows CBT and pain relief education are better at reducing catastrophising than health education; however, pain interference and intensity were non-inferior for CBT and empowered relief [30]. Pain severity did not reduce with education [37] after 2 weeks or 3 months, and catastrophising did not improve significantly with PNE or other education. Additionally, depression scores did not change post-intervention, with further studies required to validate these findings.
Pain disability was significantly better with PNE [37] than with other education. Pain acceptance reportedly improved at 26 weeks with meditation-CBT. Pain ratings decreased with regular meditation [37]. The inconsistent mediators showed a transient improvement in pain ratings. A reduced disability correlated with reduced perceived stress with CBT. Results show mindfulness-oriented recovery enhancement decreases pain severity, suggesting long-term opioid use may worsen disability. Catastrophising was linked to exercise capacity [28]; decreased catastrophising may increase activity levels, potentially changing pain tolerance, suggesting that dysfunctional beliefs could be alleviated.
Adaptive coping strategies, rather than maladaptive styles, nearly reached significance; changes in cognition are linked to disability and perception [28]. Disability reduced after education (CI 95%) at 1 week and 3 months [32]. Recurrence and healthcare seeking were lower with CBT (P < 0.001), and long-term disability decreased (P < 0.009) with CBT [32].
PNE improved pain-related outcomes [29], also improving readiness to change. Pain interference and disability decreased [38], suggesting knowledge can reduce pain and increase functioning [29]. PNE also altered a patient’s readiness to change. The 38% reported better functioning, reduced pain interference (P = 0.002), on the Global Impression of Change Scale (GICS) 35% felt a positive change, 75% better understanding [39]. The roland morris disability questionnaire (RMDQ) scores showed PNE was superior to other education [36] and was more effective at reducing disability.
Table 3 presents the key findings reported in the cited studies.
Results and findings.
| Results | Findings | Reference(s) |
|---|---|---|
Double-blinded RCT 48 participants assessing whether pain physiology education was capable of changing pain cognitions and pain thresholds in 48 patients with widespread pain and chronic fatigue syndrome. Education:
|
| Butler and Moseley [27]; Meeus et al. [28] |
Preliminary pragmatic study: 65 participants using a convenience sample, establishing whether readiness to change influences pain-related outcomes after receiving an education intervention for people with chronic pain. Outcomes of pain catastrophizing, kinesiophobia, disability, and pain neuroscience knowledge are being assessed. Education:
|
| Fletcher et al. [29] |
Compared a single-session pain management skills intervention with a single-session health education intervention and 8 sessions of CBT for adults with chronic low back pain (CLBP). 3-armed RCT 263 adult participants. Education:
|
| Darnall et al. [30] |
Multicenter RCT 608 participants with chronic pain to assess opioid reduction. Education:
|
| Sandhu et al. [31] |
RCT 202 participants with acute pain to assess the effect of the education on improving pain outcomes after their initial injury or cause of pain. Education:
|
| Butler and Moseley [27]; Traeger et al. [32] |
RCT 272 participants aimed at preventing fear avoidance and promoting coping. Education:
|
| Linton and Andersson [34] |
Parallel-arm pilot RCT 35 participants assessing mindfulness and CBT for opioid-treated CLBP. All were prescribed > 30 mg/day of morphine equivalent dose for at least 3 months. Education:
|
| Zgierska et al. [36] |
| Systematic review of the literature on video education tools for chronic illness, including pain; 59 studies; 14 measured medication use (24%). |
| Deshpande et al. [35] |
| Systematic review with meta-analysis assessing the effects of education to facilitate knowledge about chronic pain. Comparing PNE with other forms of education. |
| Geneen et al. [37] |
Study ‘fast school’ 88 participants. Education:
|
| Trouvin et al. [39] |
RCT: randomised controlled trial; PNE: pain neuroscience education; PSOCQ: pain stage of change questionnaire; CBT: cognitive behavioural therapy; RMDQ: roland morris disability questionnaire; GICS: Global Impression of Change Scale.
Six papers were RCTs, 2 systematic reviews, one preliminary study, and one further study. All are central to the purpose of the review, whether patient education before and after intervention reduces pain-related disability in chronic pain patients. Education was discussed in various forms, including opioid use for chronic pain. Three guidelines were included to ensure the review encompassed evidence-based and reliable sources.
‘Drug reduction could potentially improve outcomes. Decreased reliance on opioids by chronic pain patients could lessen the societal problem of opioid abuse’ (Zgierska et al. [36]), implying that developing CBT is critical to safely improve outcomes. The 29% participants reduced or discontinued opioids with education, Sandhu et al. [31], a 21.7% difference from the non-education group. Pain intensity reduced significantly with CBT-meditation [36]. Results correlated with another RCT looking at mindfulness-oriented opioid recovery, which also found reduced pain severity and interference, and improved pain acceptance. Sandhu et al. [31] showed that education in both formats significantly reduced patient-reported use of opioids. Encouragingly, reducing opioids was statistically significant with improvements in the patients’ mental health, including anxiety, depression, and quality of life. These findings, which focus on opioid use for chronic pain, could support the need for medication education sessions for patients with chronic pain. A retrospective cohort study [38] found 14% of patients with non-cancer pain became long-term opioid users in a year. There is no good evidence for the use of high-dose opioids for long-term pain [40].
Opioid use can be reduced with various forms of education. If pain intensity and acceptance of pain can be improved with CBT or formal education, the potential long-term opioid use could also decrease, reducing prescription costs, healthcare visits, and long-term risks due to opioids. Considering the worldwide epidemic of opioid use, it would be justified to incorporate medication/opioid management, ensuring patients’ understanding and awareness of the drugs/side effects are optimised. Three guidelines reiterated the limitations of long-term opioid use, advising caution, citing the lack of evidence for long-term opioid use.
‘A CBT preventative intervention may be valuable in the early stages’ [28, 34], aiming to benefit long-term disability. Education may be critical and could reduce disability and healthcare use, which may address the economic burden of chronic pain. Shorter sessions were as effective as education over 2 weeks [28], which would be easier to implement into practice due to staffing pressures and patient commitment. Education was found to be effective in increasing patients’ knowledge and understanding of pain, potentially improving outcomes, and reducing further healthcare visits. If shorter sessions are as effective as a longer course, it would be sensible to consider this when planning education. The results can be generalised to a wider pain population; however, pain education should be patient-centred and available in various forms to improve pain-related disability with a greater impact.
Video education tools have also been proven to improve patients’ knowledge; however, the evidence does not show an improvement in quality of life. Pain self-efficacy scores and health behaviours can improve with video-based education tools [35]. Age-related factors, education status, cognitive ability, and culture contribute to inaccessibility. A varied approach to education tools needs to be considered to gain optimal benefit. NICE [3] guidelines propose that patients’ understanding of their pain should be discussed, along with expectations and potential causes. Additionally, flare-ups and the impact pain has on one’s quality of life should be identified. Increasing knowledge and understanding and providing patients with self-management strategies have been shown to improve pain intensity and self-perceived disability, and reduce catastrophizing [29, 30, 34, 35, 37, 38]. Education, when offered and combined with other pain management interventions, optimises outcomes and reduces pain-related disability.
Strengths
Good generalisability.
Easily applied to wider pain conditions.
Indicates treatment could be influenced by education.
Early evidence suggests education may efficiently improve symptom management [30].
Weaknesses
Limited search to a single database, and narrowed the findings of relevant articles.
May not be generalised to the wider population.
Pain is implicated by various factors, limiting the generalisability of the results.
RCTs did not assess the diversity of the population, including education and socio-economic status, narrowing the results with a potential for bias; further research would be required.
Education and follow-ups were needed over a longer period to expose the participants to more interventions to gain a better effect.
There were several methodological weaknesses in the studies, such as self-reported data rather than objective measures, such as observation [30, 31]. Additionally, the lack of blinding in some of the studies [29–32] and the limited generalizability due to the ethnicity of the participants [30] cause weakness to the findings and therefore reduce the validity of the results. The results may not be valid in heterogeneous populations due to their limited generalizability. To avoid such weaknesses for future research, the inclusion criteria should include papers from various countries to ensure good generalizability, and also, blinding is sufficient to avoid bias.
In addition to the aforementioned review-level limitations, several methodological weaknesses within the reviewed studies could influence the strength of inference and should be considered when interpreting the findings. For instance, across multiple papers, there was an overreliance on self-reported outcomes rather than objective measures such as structured observation or biochemical confirmation of opioid use [30, 31]. While self-report is an accepted and often necessary approach in pain research, it is vulnerable to recall bias and socially desirable responses. This may have led to over-estimation of educational benefit, particularly in outcomes such as medication use, disability, and psychological improvement. Moreover, the lack of blinding in several trials further increases the risk of bias [29–32]. Educational interventions are particularly susceptible to anticipatory effects due to participants’ beliefs about treatment benefit potentially influencing symptom reporting independently. Consequently, some reported improvements may reflect altered perception rather than true functional change. Hence, the importance of this limitation when interpreting outcomes related to pain severity, catastrophising, and quality of life.
Notably, generalisation of findings is also controlled by limitations in population diversity. As observed in one trial conducted in a predominantly white cohort [30], restricting applicability to more ethnically and socioeconomically diverse populations. Given the established inequalities in pain prevalence, access to care, and treatment response, findings derived from homogenous samples may not translate reliably to routine clinical practice. This is particularly relevant where education is proposed as a universal component of pain management pathways.
Inconsistencies in study design further reduce comparability across the evidence. As indicated in Table 3, educational interventions differed significantly in duration, theoretical framework, delivery style, and intensity. Similarly, outcome measures ranged from opioid use and pain-related disability to emotional functioning and pain beliefs. While this reflects the diversity of educational approaches in practice, it limits synthesis and prevents firm conclusions regarding optimal content, format, or timing.
Another limitation to consider is publication bias. Reassuringly, several studies reported neutral or negative findings, including no improvement in pain severity, catastrophising, or opioid use following education [32, 36, 37]. The inclusion of such results suggests selective reporting was not practiced; however, the predominance of favourable outcomes across the literature indicates that studies demonstrating benefit may still be more likely to get published, which may increase the perceived effectiveness of education interventions and requires caution when interpreting these results.
Despite these limitations, it is important to acknowledge that most included studies were RCTs or systematic reviews, providing a credible evidence base. However, methodological weaknesses such as small sample sizes [29, 36], absence of control groups [29], attrition [34, 39], missing data [35], and procedural variability [32] all reduce confidence in the precision of effect and limit replicability.
Overall, the available evidence suggests education is a promising addition to chronic pain management. Nevertheless, variability in methodological quality, reliance on subjective outcomes, demographic restriction, and design heterogeneity mean conclusions should be regarded as suggestive rather than definitive. Further research should prioritise larger and more diverse trial populations, objective outcome measures alongside self-report, standardised intervention frameworks, and longer follow-up periods, as without methodological consolidation, education risks being implemented on theoretical appeal rather than robust observed validation.
Table 4 presents the main limitations of the papers reviewed.
Limitations of evidence.
| Article | Limitations |
|---|---|
| Meeus et al. [28] |
|
| Fletcher et al. [29] |
|
| Darnall et al. [30] |
|
| Sandhu et al. [31] |
|
| Traeger et al. [32] |
|
| Linton and Andersson [34] |
|
| Zgierska et al. [36] |
|
| Deshpande et al. [35] |
|
| Geneen et al. [37] |
|
| Trouvin et al. [39] |
|
Some results were conflicting in their findings. Some results showed there was no reduction in pain severity or depression following education as an intervention. Some results [30, 32, 37] showed that education in the form of CBT or 2 hours of PNE and mindfulness was no better at reducing depression or pain intensity. CBT was shown not to improve pain experience or intensity, indicating that perhaps this form of education, when used separately, does not help with the overall pain experience. Perhaps education for a longer period was required, as some results showed an improvement at 3 and 6 months.
Education for chronic pain, including the mechanics of pain, methods of alleviating and minimising pain, can improve pain-related disability and help patients manage and cope with their pain. Education can increase the patient’s understanding of the neurophysiology of pain, further stating that ‘it may be clear that pain physiology education is a useful modality’, suggesting that dysfunctional beliefs could be alleviated [28]. Shortened PNE has shown greater increases in neurophysiology [29], suggesting brief interventions of pain education may be more effective. The findings prove shortened education sessions, inclusive of CBT and PNE, could improve pain-related disability. Further research may be beneficial to prove the best way of educating patients about their chronic pain; evidence already supports the need for pain education for patients.
Long-term opioid use is ineffective for chronic pain management, and guidelines by NICE, core standards by the British Pain Society, and evidence from the Faculty of Pain Medicine advise against opioids. Currently, only antidepressants are offered to patients with chronic pain, due to their potential benefit of improving sleep, quality of life, and psychological distress. The safety of the patient must be considered, and regular reviews with a healthcare professional should be undertaken.
Interventions and chronic pain management options use evidence-based best practice treatment plans, which include person-centred assessments, including self-management, which could include education [3, 8]. Education, pre-medical intervention, including coping techniques, flare-up plans, self-management, and PNE, could be offered at an earlier stage to improve the patient’s expectations of further interventions that may help with pain-related disability.
Chronic pain can have profound effects on patients’ mental health and quality of life. Education has proven benefits and can enable self-management of the chronic pain condition. Current evidence, including NHS guidelines, strongly encourages self-management and patient education. The findings of this review have proven that education for pain management is effective in reducing pain catastrophising, increasing functioning and mental health, and improving quality of life. These results alone should influence healthcare practitioners to incorporate education as a prominent part of chronic pain management, specifically by developing policies and pathways to respond to and learn from the data. Despite promising results for education and chronic pain outcomes, further research is required to prove that patient education alongside other strategies for managing long-term pain is more effective at improving chronic pain management.
CBT: cognitive behavioural therapy
MDT: multidisciplinary team
NHS: National Health Service
NICE: National Institute for Health and Care Excellence
PNE: pain neuroscience education
PSOCQ: pain stage of change questionnaire
RCT: randomised controlled trial
The supplementary table for this article is available at: https://www.explorationpub.com/uploads/Article/file/1006129_sup_1.pdf.
The authors would like to express their deepest gratitude to their families for their unwavering support throughout this research journey.
KET: Conceptualization, Writing—original draft, Writing—review & editing. RC: Writing—review & editing, Supervision. AG: Writing—review & editing. MH: Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 949
Download: 14
Times Cited: 0