Case Report
Case Report

Affiliation:
1Department of Cardiology, Hai’an Hospital of Traditional Chinese Medicine, Nantong 226600, Jiangsu, China
ORCID: https://orcid.org/0009-0005-7889-482X
Affiliation:
2Department of Cardiology, Kunshan Hospital of Traditional Chinese Medicine, Suzhou 215300, Jiangsu, China
ORCID: https://orcid.org/0000-0003-0745-6169
Affiliation:
2Department of Cardiology, Kunshan Hospital of Traditional Chinese Medicine, Suzhou 215300, Jiangsu, China
ORCID: https://orcid.org/0009-0006-1355-5226
Affiliation:
2Department of Cardiology, Kunshan Hospital of Traditional Chinese Medicine, Suzhou 215300, Jiangsu, China
Email: fjhheart@126.com
ORCID: https://orcid.org/0000-0002-3144-9324
Explor Cardiol. 2025;3:101272 DOI: https://doi.org/10.37349/ec.2025.101272
Received: August 13, 2025 Accepted: September 12, 2025 Published: September 22, 2025
Academic Editor: Alireza Ansari-Moghaddam, Zahedan University of Medical Sciences, Iran
Phrenic nerve palsy (PNP) is a recognized complication of cryoballoon ablation (CBA) for atrial fibrillation (AF), particularly during the ablation of the right superior pulmonary vein (RSPV). We report the case of an 80-year-old female with a history of hypertension, who was admitted for CBA of paroxysmal AF. Despite optimal medical treatment with amiodarone, the patient experienced recurrent episodes of AF, prompting the decision to proceed with CBA. During the procedure, while isolating the RSPV, diaphragmatic movement was significantly weakened after 92 seconds of cryoablation at a temperature of –52°C. Immediate cessation of the procedure and intravenous methylprednisolone were administered, resulting in partial recovery of diaphragmatic movement. However, when the procedure resumed, diaphragmatic movement once again diminished, and despite further steroid treatment, the movement did not recover by discharge. The patient remained asymptomatic with stable oxygen saturation, and no respiratory distress was noted. At a six-month follow-up, the patient reported no symptoms of chest tightness or shortness of breath, and her general condition remained stable, although diaphragmatic movement had not fully recovered, indicating partial functional compensation. This case underscores the importance of continuous phrenic nerve monitoring during CBA, early detection of complications, and appropriate management to prevent irreversible injury, highlighting the need for careful procedural planning and postoperative follow-up in elderly patients with comorbidities.
Phrenic nerve palsy (PNP) is a well-recognized complication of cryoballoon ablation (CBA) for atrial fibrillation (AF). We present a case of an 80-year-old woman who developed prolonged PNP following CBA, underscoring the importance of vigilant monitoring and timely management to reduce the risk of permanent dysfunction.
An 80-year-old woman with a history of hypertension was admitted for CBA due to paroxysmal AF. Over the previous three months, she had experienced multiple symptomatic AF episodes lasting several hours despite treatment with amiodarone. Her hypertension was managed with valsartan. Preprocedural transthoracic echocardiography revealed a left ventricular ejection fraction (LVEF) of 62%, normal left ventricular dimensions, and a mildly enlarged left atrium (LA) (diameter 42 mm), without significant valvular disease. Owing to her age and comorbidities, other class I or III antiarrhythmic agents were not considered appropriate. Given her persistent symptoms and limited response to medical therapy, CBA was chosen as the treatment strategy.
After transesophageal echocardiography excluded left atrial thrombus, the procedure was performed under conscious sedation. A ten-polar catheter was positioned in the coronary sinus via the left femoral vein. A single transseptal puncture was made, and a 14-F steerable sheath (FlexCath Advance, Medtronic) was inserted. Based on preprocedural CT imaging of the pulmonary veins, a 28-mm fourth-generation cryoballoon catheter (Arctic Front Advance, Medtronic) was used for pulmonary vein isolation (PVI). Adequate vessel occlusion was confirmed when selective contrast injection demonstrated complete contrast retention without atrial backflow, after which cryothermal energy was applied.
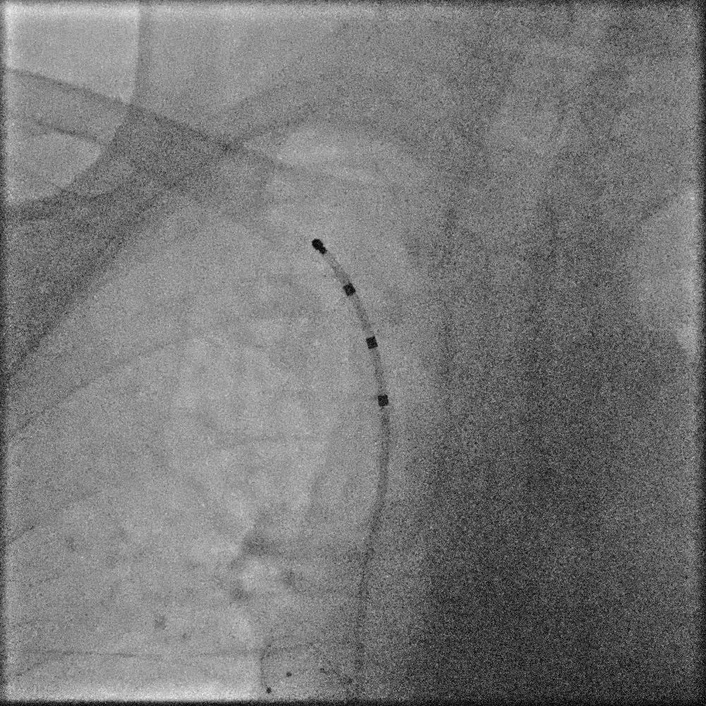
During ablation of the right superior pulmonary vein (RSPV), continuous phrenic nerve monitoring was performed with a decapolar catheter placed in the superior vena cava (Figure 1). High-output pacing (8 V, 2.0 ms pulse width, cycle length 1,500 ms) was delivered between poles 1 and 4 to provide real-time assessment of diaphragmatic movement. After 92 seconds of freezing, with a nadir temperature of –52℃, a marked reduction in diaphragmatic excursion was observed (Movie S1). Ablation was immediately terminated, and intravenous (IV) methylprednisolone sodium succinate (40 mg) was administered. Within minutes, diaphragmatic movement returned (Movie S2).
A second freeze on the RSPV was applied, lasting 112 seconds with a nadir temperature of –53℃. This again resulted in diaphragmatic impairment, which did not recover despite repeated steroid administration (Movie S3). The patient remained asymptomatic, maintaining stable oxygen saturation without dyspnea or chest discomfort. Ablation of the left pulmonary veins was subsequently completed successfully. Radiofrequency ablation (RFA) was performed on the right pulmonary veins, resulting in complete isolation. Postoperatively, the patient received IV methylprednisolone 40 mg daily for three days, but right diaphragmatic function did not recover before discharge. Nevertheless, she remained asymptomatic, with no evidence of respiratory compromise.
At the six-month follow-up, the patient reported no chest tightness, shortness of breath, or functional limitation during a telephone interview. She declined chest radiography, but her stable clinical condition suggested partial functional compensation despite persistent diaphragmatic dysfunction. Table 1 summarizes the timeline of the events.
Timeline of clinical events.
| Date/Time | Event | Details/Findings | Management/Outcome |
|---|---|---|---|
| Baseline (pre-procedure) | Admission | 80-year-old female, history of hypertension, recurrent paroxysmal AF despite amiodarone. LVEF 62%, LA 42 mm, no thrombus on TEE | Planned for CBA |
| Day 0—procedure | CBA initiated | 28-mm fourth-generation cryoballoon, transseptal puncture, PV angiography performed | Start of PVI |
| Day 0—during RSPV ablation (92 s, –52°C) | First PNP episode | Diaphragmatic movement weakened, detected by phrenic nerve pacing | CBA stopped, IV methylprednisolone 40 mg; partial recovery observed |
| Day 0—second RSPV ablation (112 s, –53°C) | Recurrent PNP | Persistent reduction of diaphragmatic movement | CBA stopped, methylprednisolone repeated; no recovery |
| Day 0—completion | Remaining veins ablated | Left PVs isolated by CBA; right PVs completed by RFA | Successful PVI achieved |
| Post-procedure (hospital stay) | Persistent right PNP | No dyspnea, SpO2 stable; treated with IV methylprednisolone for 3 days | No diaphragmatic recovery at discharge |
| 6-month follow-up | Telephone consultation | Patient asymptomatic, no chest tightness or dyspnea; declined chest X-ray | Stable condition, functional compensation suspected |
AF: atrial fibrillation; CBA: cryoballoon ablation; IV: intravenous; LA: left atrium; LVEF: left ventricular ejection fraction; PNP: phrenic nerve palsy; PV: pulmonary vein; PVI: pulmonary vein isolation; RFA: radiofrequency ablation; RSPV: right superior pulmonary vein; TEE: transesophageal echocardiography.
The risks of CBA, including potential phrenic nerve injury (PNI), were thoroughly explained preoperatively, and informed consent was obtained. When PNP occurred, the patient was promptly informed of its nature, management strategies (including corticosteroids), and the possibility of delayed recovery. Shared decision-making was emphasized, and the patient agreed to continued follow-up and supportive management, trusting the multidisciplinary team’s recommendations.
PNP is a recognized complication associated with CBA for AF, with an incidence ranging from 1.14% to 11.2% in published series [1–3]. Patient-specific anatomical factors may include the proximity of the RSPV to the phrenic nerve, as studies show that 32% of the anterior walls of the RSPV are less than 2 mm away from the phrenic nerve [4]. Therefore, the phrenic nerve is prone to injury during CBA of the RSPV. In comparison with other ablation techniques, CBA is associated with a relatively higher risk of PNP due to its circumferential energy delivery and the proximity of the RSPV to the phrenic nerve. RFA, by contrast, allows for point-by-point lesion creation and greater flexibility, which may reduce the risk of PNI but requires longer procedure times and carries risks of collateral tissue damage, such as esophageal injury. Pulsed field ablation (PFA) has recently emerged as a promising modality with myocardial selectivity and a favorable safety profile, including a lower incidence of PNI. However, long-term safety and efficacy data on PFA remain limited, and further studies are warranted.
Management of PNP typically involves immediate cessation of the procedure, administration of corticosteroids, and monitoring for spontaneous recovery. In most cases, PNP is transient and resolves within 3 to 12 months, although some cases may require further interventions such as physical therapy if recovery is incomplete. There is no reliable method for predicting PNI before the procedure. Based on the preoperative CTA results of the PVs, a 28-mm fourth-generation cryoballoon catheter is selected to improve thermal distribution and reduce the risk of PNP. This approach ensures that the phrenic nerve is closely monitored during ablation to prevent potential damage. The selection of the cryoballoon size and monitoring of the phrenic nerve are crucial steps to enhance the safety and effectiveness of the procedure.
Although the overall incidence of PNP is low and most cases are transient [5], the present case underscores the vulnerability of the phrenic nerve during CBA. When weakened diaphragmatic movement was first detected, ablation was immediately halted, and 40 mg of methylprednisolone sodium succinate was administered intravenously. After several minutes of observation, diaphragmatic movement resumed. Methylprednisolone, a corticosteroid with potent anti-inflammatory effects, was used to reduce nerve inflammation and facilitate recovery. Histopathological studies of cryoballoon-induced PNI have demonstrated axonal damage consistent with Wallerian degeneration, with the extent of injury correlating with functional impairment of diaphragmatic motion [6]. Nevertheless, PNP recurred after resumption of ablation at the RSPV. Despite continued postoperative administration of methylprednisolone, diaphragmatic movement had not recovered at the time of hospital discharge, suggesting that the nerve injury was more severe than initially anticipated.
The prolonged course of PNP in this case is relatively uncommon but has been described in the literature. While most instances of PNI following AF ablation resolve spontaneously within 12 months regardless of the energy source [7], rare cases of persistent palsy lasting beyond one year—or even permanently—have been reported. Long-term complications may include reduced exercise tolerance, exertional dyspnea, impaired quality of life, and increased susceptibility to pulmonary infections due to impaired diaphragmatic excursion. For patients with prolonged or irreversible PNP, preventive and supportive measures such as pulmonary rehabilitation, respiratory muscle training, and regular pulmonary function assessment are recommended. These considerations emphasize the importance of vigilant intraoperative monitoring, early intervention, and multidisciplinary follow-up to optimize long-term outcomes in affected patients.
Several factors may have contributed to the development of prolonged PNP in this elderly patient. Anatomical factors, particularly the close proximity of the RSPV to the phrenic nerve, likely increased the nerve’s vulnerability during ablation. Advanced age may have further compounded this risk, as age-related tissue rigidity renders older individuals more susceptible to nerve injury [8]. Comorbidities such as hypertension may also have predisposed the patient to procedural complications. Technical factors related to the CBA procedure may have influenced the severity of PNP. The duration and intensity of freezing are key determinants of tissue injury. In this case, freezing times of 92 seconds during the first application and 112 seconds during the second, with nadir temperatures of –52°C and –53°C, respectively, likely increased the risk of thermal injury to adjacent tissues, including the phrenic nerve. Catheter positioning is also critical. Although the cryoballoon was positioned to achieve optimal vessel occlusion with full contrast retention, subtle variations in balloon placement relative to the RSPV and phrenic nerve could have increased the likelihood of injury. Continuous phrenic nerve monitoring with a decapolar catheter in the superior vena cava allowed real-time assessment of diaphragmatic motion, enabling early recognition of PNP and prompt interruption of ablation to limit further damage. Despite this precaution, procedural factors such as balloon size, freezing parameters, and catheter positioning may have contributed to the unfavorable outcome [9].
Although this report primarily describes short-term findings, the long-term recovery of phrenic nerve function is crucial for assessing the full clinical implications of prolonged PNP. At the six-month follow-up, the patient remained clinically stable, without symptoms of chest tightness or dyspnea. Nevertheless, persistent PNP can impair diaphragmatic motion, leading to reduced exercise tolerance and diminished quality of life. Long-term follow-up and rehabilitation strategies—including pulmonary rehabilitation and respiratory muscle training—may be required to promote functional recovery and mitigate complications. Continued monitoring of respiratory function and quality of life is essential in patients with persistent nerve injury.
This case highlights the importance of vigilant phrenic nerve monitoring during cryoablation of the right pulmonary veins. Although the use of fourth-generation cryoballoons and 14-F steerable sheaths may improve procedural efficiency and reduce the risk of nerve injury, PNP can still occur. Upon detecting PNP, ablation should be terminated immediately, and corticosteroids may facilitate nerve recovery. However, repeat cryoablation should be avoided, and switching to alternative ablation modalities may help prevent additional phrenic nerve damage.
AF: atrial fibrillation
CBA: cryoballoon ablation
IV: intravenous
PFA: pulsed field ablation
PNI: phrenic nerve injury
PNP: phrenic nerve palsy
RFA: radiofrequency ablation
RSPV: right superior pulmonary vein
The supplementary movies for this article are available at: https://www.explorationpub.com/uploads/Article/file/101272_sup_1.pdf.
We thank the patient for allowing the publication of this report.
JF: Conceptualization, Writing—review & editing. WY: Investigation, Supervision. HX: Visualization, Writing—original draft. WP: Writing—original draft. All authors read and approved the submitted version.
The authors report no conflicts of interest in this work.
The study complies with the Declaration of Helsinki (2024 version). Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent to participate in the study was obtained from the participant.
The patient provided written informed consent for her case details to be published.
The datasets used are available from the corresponding author on request.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 4878
Download: 189
Times Cited: 0