Case Report
Case Report

Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
Email: christian.ratti@unimi.it
ORCID: https://orcid.org/0009-0000-8824-3717
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0000-0001-8648-0532
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0009-0009-8184-9623
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0000-0001-8028-5453
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0000-0003-4486-5084
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0009-0007-4903-0533
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0009-0007-7588-8680
Affiliation:
Allergy and Clinical Immunology Unit, Sacco Hospital, 20157 Milan, Italy
ORCID: https://orcid.org/0000-0003-1510-9677
Explor Asthma Allergy. 2026;4:1009113 DOI: https://doi.org/10.37349/eaa.2026.1009113
Received: December 19, 2025 Accepted: February 13, 2026 Published: March 02, 2026
Academic Editor: Umit Murat Sahiner, Hacettepe University Faculty of Medicine, Turkey
Scombroid syndrome is a frequent cause of fish poisoning and typically presents with mild, self-limiting symptoms. Severe anaphylaxis-like reactions are uncommon, and a biphasic clinical course has not previously been reported. We describe the case of a 19-year-old woman who developed flushing, headache, generalized urticaria, facial edema, dyspnea, and hypotension approximately 30 minutes after ingesting raw amberjack tartare. Emergency treatment with adrenaline, antihistamines, corticosteroids, and intravenous fluids led to initial clinical improvement; however, three hours later, she experienced a recurrence of cutaneous, respiratory, and gastrointestinal symptoms, consistent with a biphasic reaction. The patient subsequently developed chest pain associated with transient electrocardiographic changes and mild troponin elevation, prompting further evaluation for suspected Kounis syndrome. Allergy assessment, including specific IgE testing and skin-prick testing with fresh fish, was negative, supporting a toxic rather than IgE-mediated mechanism. This case expands the clinical spectrum of scombroid syndrome by documenting a biphasic anaphylaxis-like presentation and underscores the importance of considering histamine fish poisoning in the differential diagnosis of severe food-related reactions. Careful evaluation is essential to prevent misdiagnosis and unnecessary long-term dietary restrictions.
Scombroid syndrome is the most common cause of ichthyotoxicosis worldwide and results from the ingestion of improperly stored fish containing high concentrations of histamine [1]. Histamine is produced through bacterial decarboxylation of the amino acid histidine, which occurs when the fish is not adequately refrigerated soon after death. Bacterial decarboxylation of other amino acids generates additional biogenic amines (such as putrescine, cadaverine, and urocanic acid) that can enhance and prolong symptom severity [1].
Ingestion of contaminated fish leads, within minutes to hours, to the onset of pseudo-allergic manifestations including flushing, urticaria/angioedema, bronchospasm, abdominal pain, vomiting, diarrhea, and hypotension [1–3]. Certain symptoms may suggest the diagnosis of scombroid syndrome, such as headache, flushing, and a characteristic metallic, bitter, or peppery taste of the fish [1, 2]. Symptoms are generally mild and self-limited, resolving spontaneously or with antihistamines, which represent the treatment of choice [1, 2]. In rare cases, however, scombroid syndrome may mimic true anaphylaxis and cause life-threatening complications, including marked hypotension, angina, and cardiac involvement such as Kounis syndrome [3–8].
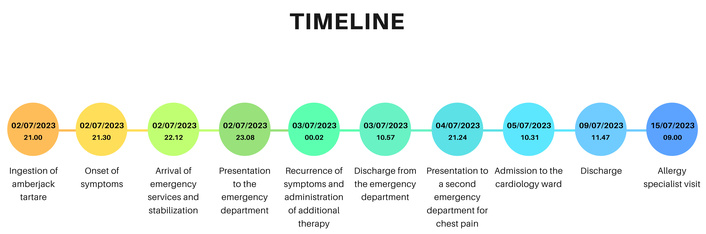
The chronological sequence of clinical events following amberjack tartare ingestion is summarized in Figure 1.
We describe the case of a 19-year-old Caucasian woman with a history of allergic rhinoconjunctivitis. While dining at a restaurant in the Emilia-Romagna region of Italy, she consumed a serving of raw amberjack tartare without any seasoning. She immediately noticed an abnormal taste and decided not to eat further; none of her dining companions tasted the dish. Approximately 30 minutes after ingestion, she developed a pulsating headache followed by tremor, generalized pruritic rash, facial edema, a sensation of throat tightness, and dyspnea.
Emergency medical services found her in respiratory distress. Her blood pressure was 90/50 mmHg, heart rate 168 bpm, oxygen saturation 91%, and respiratory rate 40 breaths/min. She received nebulized adrenaline, intravenous corticosteroids, and fluid resuscitation, with initial improvement in hemodynamic parameters and resolution of cutaneous symptoms.
She was transferred to the Emergency Department of M. Ceccarini Hospital, where after approximately 3 hours from the meal, she experienced a recurrence of cutaneous symptoms and an episode of dyspnea, followed by two episodes of diarrhea. She received 0.5 mg intramuscular adrenaline, corticosteroids, and antihistamines, with subsequent clinical improvement. Blood tests revealed no significant abnormalities, and she was discharged the following day.
On the following day, she presented to the Emergency Department of Auxologico San Luca Hospital in Milan with persistent chest pain. The electrocardiogram (ECG) showed biphasic T waves in lead DIII and diffuse ST-segment straightening (Figure 2). Troponin levels rose from 3 ng/L to 26 ng/L, accompanied by elevated liver transaminases (Table 1). She was admitted to the cardiology unit with suspected Kounis syndrome. Echocardiography and cardiac MRI, however, revealed no significant abnormalities. After normalization of ECG findings and laboratory results, she was discharged with the diagnosis of “chest pain following recent anaphylactic shock”.
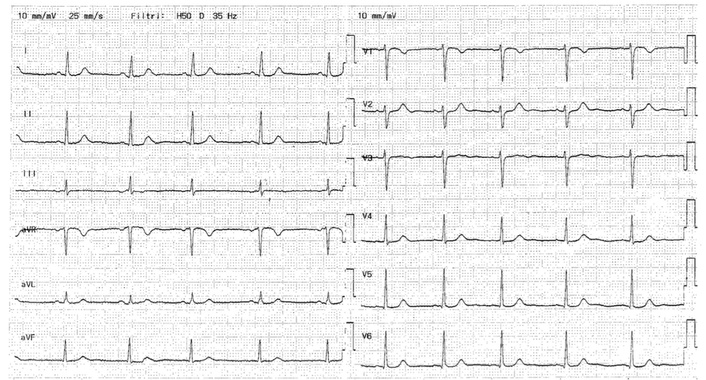
ECG performed for chest pain showed biphasic T waves in lead DIII and diffuse ST-segment straightening.
Laboratory findings at the time of the second emergency department presentation for chest pain.
| Test name | Result | Normal range | Interpretation |
|---|---|---|---|
| White blood cells | 7.70 × 109/L | 4.30–10.50 × 109/L | Normal |
| Erythrocytes | 3.38 × 1012/L | 4.09–5.20 × 1012/L | Reduced |
| Hemoglobin | 107 g/L | 119–160 g/L | Reduced |
| Platelets | 123 × 109/L | 140–450 × 109/L | Reduced |
| C-reactive protein | 0.62 mg/dL | < 1 mg/dL | Normal |
| Creatinine | 0.63 mg/dL | 0.50–0.95 mg/dL | Normal |
| Aspartate aminotransferase | 29 U/L | < 40 U/L | Normal |
| Alanine aminotransferase | 55 U/L | < 40 U/L | Increased |
| Gamma-glutamyl transferase | 24 U/L | < 40 U/L | Normal |
| Cardiac troponin T | 26 ng/L | < 14 ng/L | Increased |
| Immunoglobulin E | 3 kU/L | < 100 kU/L | Normal |
She was subsequently evaluated at our allergy clinic at L. Sacco Hospital. She had been prescribed an epinephrine autoinjector upon discharge from the Emergency Department, and she had eliminated fish and shellfish from her diet. Specific immunoglobulin E (IgE) testing for cod, anisakis, and shrimp extracts, as well as molecular components Gad c 1 (cod β-parvalbumin) and Pen a 1 (shrimp tropomyosin), was negative. Baseline tryptase levels were within normal limits (Table 2). Skin-prick testing with fresh raw amberjack (prick-by-prick) was also negative.
Results of the tests performed after the allergological evaluation.
| Test name | Result | Normal range | Interpretation |
|---|---|---|---|
| Immunoglobulin E | 157 kU/L | < 100 kU/L | Increased |
| Cod extract IgE | < 0.1 kU/L | < 0.1 kU/L | Negative |
| Anisakis extract IgE | < 0.1 kU/L | < 0.1 kU/L | Negative |
| Shrimp extract IgE | < 0.1 kU/L | < 0.1 kU/L | Negative |
| Gad c 1 IgE | < 0.1 kU/L | < 0.1 kU/L | Negative |
| Pen a 1 IgE | < 0.1 kU/L | < 0.1 kU/L | Negative |
| Basal tryptase | 3 ng/mL | < 5 ng/mL | Normal |
The toxic, non-allergic nature of her reaction was explained to the patient, and a supervised oral challenge with amberjack was proposed; however, she declined due to fear related to the severity of the previous reaction. She was therefore advised, as a precautionary measure, to avoid fish consumption until a food challenge could be performed in a safe setting, without the need to avoid trace exposure or cross-contamination, while reintroducing shellfish at home, which she had voluntarily excluded from her diet following the event. The patient remains under follow-up with our unit and has been encouraged to contact us should she reconsider or require further support. In the meantime, she has successfully reintroduced shellfish without any adverse reactions.
Despite the absence of provocation testing, the characteristic initial symptoms, together with negative skin tests and IgE assays, supported the diagnosis of scombroid syndrome-induced anaphylaxis with suspected cardiac involvement.
At the time of the second emergency department presentation, a comprehensive laboratory assessment was performed, and the main findings are summarized in Table 1. Laboratory parameters obtained during the subsequent allergological evaluation are presented in Table 2.
“The episode was sudden and terrifying, particularly the difficulty breathing and the feeling of losing control shortly after eating. When the symptoms returned, and I later developed chest pain, I became deeply frightened that something serious was happening to my heart. Even though the doctors explained that the reaction was not allergic and the tests were reassuring, I am still afraid of a recurrence. This fear has led me to avoid fish and to decline further testing, although continued medical follow-up has helped me feel somewhat more supported.”
This case carries several noteworthy implications. Although scombroid syndrome is typically mild and self-limiting, our patient experienced an unusually severe presentation characterized by significant hypotension and respiratory compromise. While most cases reported in the literature involve mild to moderate symptoms, numerous cases of anaphylaxis-like presentations, including cardiovascular collapse, have been described [3–8]. This underscores how scombroid poisoning can closely mimic IgE-mediated anaphylaxis, highlighting the diagnostic challenge posed by histamine fish poisoning.
However, a biphasic evolution—as observed in our patient approximately three hours after ingestion—is not characteristic of scombroid syndrome. To our knowledge, this represents the first reported case of biphasic recurrence in the context of histamine fish poisoning.
This observation may have important clinical implications: in selected cases with severe initial symptoms, prolonged post-treatment observation may be warranted, similar to recommended practice in anaphylaxis.
Several mechanisms could account for the delayed symptom flare. A high degree of fish contamination could lead to prolonged or secondary toxic effects [1]. Impaired activity of endogenous histamine-degrading enzymes—such as diamine oxidase and histamine-N-methyltransferase—may also contribute, and interindividual variability in these enzymatic pathways, including potential genetic differences, has been increasingly recognized [5]. Furthermore, experimental murine models have demonstrated that urocanic acid may induce mast-cell degranulation and endogenous histamine release, although this mechanism has not yet been confirmed in humans [9]. Delayed antihistamine administration may have further contributed to the biphasic course observed.
Cardiac involvement in this case remains uncertain. Although Kounis syndrome was initially suspected, the diagnosis was not confirmed upon discharge. The transient ECG abnormalities and troponin elevation observed the following day may have been related to recent intramuscular epinephrine administration [10] or may represent nonspecific findings. Nevertheless, these observations underscore that cardiac symptoms in the context of scombroid poisoning warrant careful evaluation.
This case highlights the importance of considering toxic etiologies such as scombroid syndrome in the differential diagnosis of severe food-related reactions, even when symptoms closely resemble IgE-mediated anaphylaxis. Key diagnostic clues include gustatory alterations, flushing, and headache in individuals without a prior history of fish allergy [1]. The diagnosis is further supported by negative skin-prick testing (both with commercial extracts and fresh fish) and by the absence of specific IgE sensitization, while measurement of histamine levels in the implicated fish, when feasible, can provide additional confirmation [11].
Beyond the acute phase, psychological support plays an essential role in the management of patients who experience sudden and severe hypersensitivity-like reactions, regardless of their underlying mechanism. Such episodes can trigger persistent anxiety, hypervigilance, and avoidance of entire food groups or social situations involving meals. This fear of recurrence may substantially affect daily functioning and overall quality of life [12]. Providing clear information, reassurance, and accessible follow-up helps patients regain confidence, promotes safe reintroduction of previously avoided foods when appropriate, and prevents long-term psychological distress [13]. Integrating structured psychosocial support into routine care is therefore crucial to ensuring both medical stabilization and emotional recovery.
ECG: electrocardiogram
IgE: immunoglobulin E
CPR: Conceptualization, Methodology, Data curation, Project administration, Writing—original draft. MC: Resources, Data curation, Writing—original draft. AB, ACG, and EB: Methodology, Resources, Investigation. LC, VGRO, and EI: Data curation, Validation, Supervision, Writing—review & editing. All authors read and approved the submitted version.
The authors declare no conflicts of interest.
The study complies with the Declaration of Helsinki. Ethical review for the case report study is not required according to the local committee.
Informed consent to participate in the study was obtained from the participant.
Informed consent to publication was obtained from the participant.
Data supporting the findings of this study are available upon request from the corresponding author.
This research received no external funding.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1466
Download: 15
Times Cited: 0