Original Article
Original Article

Affiliation:
1Department of Neurostimulation, Cuban Center for Neurosciences, Havana 10600, Cuba
Email: rigf58@yahoo.com
ORCID: https://orcid.org/0000-0003-0863-7893
Affiliation:
2Department of Epilepsy, Institute of Neurology and Neurosurgery, Havana 10400, Cuba
Affiliation:
1Department of Neurostimulation, Cuban Center for Neurosciences, Havana 10600, Cuba
ORCID: https://orcid.org/0000-0002-3631-4269
Affiliation:
1Department of Neurostimulation, Cuban Center for Neurosciences, Havana 10600, Cuba
ORCID: https://orcid.org/0000-0002-5840-3537
Affiliation:
2Department of Epilepsy, Institute of Neurology and Neurosurgery, Havana 10400, Cuba
ORCID: https://orcid.org/0000-0002-2019-5859
Affiliation:
2Department of Epilepsy, Institute of Neurology and Neurosurgery, Havana 10400, Cuba
ORCID: https://orcid.org/0000-0002-3815-2136
Affiliation:
2Department of Epilepsy, Institute of Neurology and Neurosurgery, Havana 10400, Cuba
ORCID: https://orcid.org/0000-0003-1805-7200
Affiliation:
1Department of Neurostimulation, Cuban Center for Neurosciences, Havana 10600, Cuba
ORCID: https://orcid.org/0000-0002-4406-444X
Explor Neurosci. 2024;3:144–155 DOI: https://doi.org/10.37349/en.2024.00041
Received: September 25, 2023 Accepted: January 18, 2024 Published: April 12, 2024
Academic Editor: Jinwei Zhang, University of Exeter Medical School, UK
The article belongs to the special issue Epilepsy
Aim: The aim of this paper is to discuss the main features and first outcomes of a therapeutic platform proposed to implement a public health therapeutic service for patients suffering refractory epilepsy.
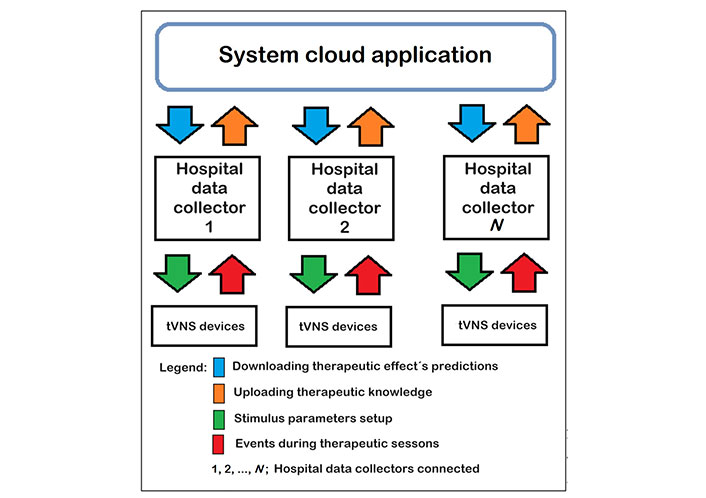
Methods: The proposal is a three-layer system composed by a new portable therapy device and two software applications. The therapy is transcutaneous electrical vagus nerve stimulation, known as tVNS. The primary layer is composed of tVNS devices, configured for each patient according to the instructions provided by the specialists. The middle layer is named “hospital data collector” (HDC), its main tasks are the patient enrollment, the device setup, and the database maintenance to store therapeutic parameters and session events together with the information cited previously. Each hospital center runs a HDC that is connected to a cloud application named “system cloud application (SCA)” which concentrates all the data supplied by the HDCs. Artificial intelligence methods are integrated in the SCA to predict the treatment effectiveness for every new patient based on the accumulated knowledge from the enrolled previously.
Results: A version of the proposed system is running at the Institute of Neurology and Neurosurgery. The sensitivity of the therapeutic device with the proposed treatment protocol reaches 83.33% in the 18-patient pilot trial carried out.
Conclusions: The proposed approach seems a useful therapeutic tool based on the pilot trial outcomes. The developed device is comfortable and suitable for the intended use. The proposed system has created the essential conditions to feed and grow a knowledge, a basic element to predict the treatment effectiveness for each new patient. It is a promising option for a refractory epilepsy therapy service.
According to the World Health Organization (WHO) reports, epilepsy is one of the three most prevalent neurological diseases internationally, affecting 1% of the world’s population [1]. Thirty percent of people suffering from epilepsy do not achieve significant improvement with the current antiepileptic drugs, not even through their combinations, and require other complementary treatments [1, 2]. This disease variant is known as drug resistant epilepsy or refractory epilepsy. A small percentage of these patients reach a better condition through surgery, but they still require complementary treatments and have to meet certain requirements to undergo surgery.
Vagus nerve stimulation (VNS) is one of the most successful complementary therapeutic methods for the treatment of refractory epilepsy today [3–5]. There are two approaches for this therapy, one based on active implanted devices, which was the first used stably, known as VNS based on active implanted devices (iVNS), and another based on external devices, called transcutaneous electrical VNS (tVNS), which popularity has increased in recent years [5]. The automatism of the iVNS devices and their proven effectiveness are important advantages, but their weaknesses are associated with the risks of the required surgery and their manufacturing and implanting costs. The tVNS-based approach excludes the surgery risks because it is an external device and the cost drops down because no special materials or high-specialized technologies are required for manufacturing. At the same time, several researching teams have reported similarity in therapy effectiveness for both approaches [5, 6].
Therapy based on tVNS has had multiple applications in recent years. Kim et al. [7] report twelve investigations about tVNS applied as complementary therapy in subjects suffering from refractory epilepsy. All these studies have had satisfactory results, with sensitivity greater than 60%, but a well-defined standard is not been established for the value of the stimulation parameters.
For the tVNS application in a public health scheme, providing therapeutic services to large populations, it is necessary to minimize costs without giving up the effectiveness of the treatment, so iVNS is not appropriate for this purpose [8]. A better solution is the tVNS because devices are cheaper, surgery is not required and the therapeutic effects have been demonstrated. Thus, the use of iVNS devices is reserved for those patients with greater economic resources [7, 9].
While other authors have been focused on the evaluation of therapeutic devices, in this document two topics are presented. Firstly, a platform to provide a therapeutic service to people suffering from refractory epilepsy is described. It is composed by a novel low-cost tVNS device and two complementary software subsystems, all developed by the authors. Artificial intelligence techniques, such as neural networks and statistical inference, will be applied to predict the treatment effectiveness for each patient. Secondly, the pilot trial carried out to evaluate a therapeutic device, developed by the authors, is explained and the outcomes are discussed. Currently, a first version of the proposal is running at the institute of neurology and neurosurgery of Havana and its growth and expansion to other hospital centers is expected.
The proposed solution is a three-layer system as shown in Figure 1. The low-level layer, or patient layer, is composed by the therapeutic devices assigned to each patient. These devices are for personal use and each patient will apply the therapy at home by himself, following the medical indications. Previously, the patient and his companion were trained to use the device and be able to fill out the crisis and adverse effects diary, supported by International League Against Epilepsy (ILAE). This document is, a follow-up tool to quantify the therapy impact on the patient’s evolution. Furthermore, this document has been used in previous reported researches about the same theme, so an outcome comparison can be set with the described proposal.
The middle layer is a Windows application developed by the authors, named hospital data collector (HDC). Its main objectives are the following:
Enrollment of patients: the general data of each patient and the main information of the clinical record are input and stored in a local database.
Setup of therapeutic devices: each device is connected to this Windows application through a universal serial bus (USB) port to set the therapy parameters, that is, the duration and daily rate of the therapeutic sessions as well as the width, polarity, amplitude and frequency of the therapeutic pulses.
Recording of events associated with therapeutic sessions: the developed device stores in an internal memory the start time of each therapeutic session and its duration. This information is uploaded to the HDC and the specialist can check if the patient is following the medical instructions to apply the therapy.
Data collection from the crisis and adverse events diary: the patient and his companion are trained to fill out this document and this information is stored because it is basic to calculate the monthly seizure rate (MSR), the best variable to quantify whether the treatment is being effective.
The third layer is called “system cloud application (SCA)”. This application stores all the information collected by the HDCs of the medical centers integrated into the system. In this way, a knowledge base is created as the starting point to predict the therapy effectiveness for each new patient enrolled into the system. The use of the devices can also be optimized taking in count these predictions. The knowledge base will integrate general data, clinical data and data from the therapy itself, mainly stimulation parameters and changes in MSR.
The device used in the pilot trial is the NT1.1 Transcutaneous Stimulator for Epilepsy Treatment, ESTEP, a product of IC Neuronic S.A. branded as ESTEP. This is a new tVNS device characterized by the following features: personal use, portable, rechargeable battery powered, fully configurable stimulus, automatic adjustment of the electrodes to the left ear concha, recording of date, time and duration of each therapeutic session in an internal memory for later review USB communication. Therapeutic electrical stimulation is applied to the left ear concha. Two electrodes, embedded in a plastic piece for adjusting are connected to the patient skin on the concha’s upper part. These electrodes are parts of the stimulation cable; the other extreme ends two connectors to join to the device.
A pilot trial provided the required evidence of the safe use and effectiveness of the ESTEP device so that the Cuban medical devices regulatory body issued its sanitary approval. Previously, patient electrical safety and the accuracy of its parameters were demonstrated in technical tests carried out in a specialized technical laboratory.
The pilot trial was approved by the ethical committees of the two involved scientific institutions: the Cuban Center for Neurosciences and the Institute of Neurology and Neurosurgery of Havana. In addition, the Cuban Center for State Control of Medicines, Equipment and Medical Devices approved the study as the national regulatory body for medical technologies.
A pilot trial was carried out (internal trial registration number: 568/0101822223Q1164 issued by the Center for State Control of Medicines, Medical Equipment and Medical Devices of the Republic of Cuba) with patients aged between 18 years and 48 years. The aim was to demonstrate that the developed device was safe and effective.
Pilot trials can be defined as small versions of the clinical trials. This kind of studies help to test that a medical device works properly in real conditions. Typically, this kind of trial is enough to get the approval of any regulatory body when the medical technology involved is considered as a new implementation of standard technologies.
Eighteen patients with a diagnosis of refractory epilepsy were chosen randomly from neurology services specialized in epilepsy. These patients meet the following inclusion criteria:
Age between 18 years and 65 years.
Confirmed diagnosis confirmed by the interrogation and clinical tests, excluding other processes simulating epilepsy (psychogenic seizures, migraine, simulation, syncope, etc.).
Four or more difficult to control crises per month.
Ineffectiveness of two antiepileptic drugs in monotherapy and of a combination of two antiepileptic drugs.
Two years with antiepileptic drugs-based treatment at least.
Maintain the pharmacological treatment unchanged in terms of doses and medications throughout the pilot trial duration.
Patients undergoing surgery with a diagnosis of non-lesional focal epilepsy who persist with a high seizure frequency and/or seizures that very markedly affect their quality of life.
Voluntary participation in the research expressed through written informed consent.
A candidate was excluded:
If other chronic pathologies of the central nervous system (CNS), cardiovascular, liver, kidney, or blood disorders coexist with epilepsy.
If they have other implanted devices such as cardiac pacemakers or neurostimulators.
If they were pregnant or breastfeeding.
All patients involved in the pilot trial were diagnosed as epileptics previously, so it is not necessary to mention the suffering of progressive diseases that can trigger epilepsy as an exclusion criterion.
The criteria for abandoning the pilot trial were the following:
If recurrences or adverse effects appear that prevent therapy with tVNS.
If the companion or patient do not comply with the instructions given by the research team.
The desire to abandon the pilot trial before it concludes.
To characterize each patient before and after the use of the proposed device, the following tests were applied:
Video electroencepahalogram (EEG): it was used to verify the epilepsy diagnosis and to compare the frequency of epileptiform discharges before and after applying tVNS-based therapy.
Nuclear magnetic resonance: allows a clear evaluation of potentially epileptogenic brain abnormalities; useful to confirm the diagnosis.
Clinical laboratory tests: blood and urine samples of each patient were analyzed to evaluate the status of each patient before and after applying tVNS-based therapy.
Neuro psychological evaluation: this evaluation aimed to determine if the reduction in the MSR caused a positive psychosocial effect in the patients.
The authors considered not necessary a control group due to the following:
The trial proposed by the authors is a pilot trial. In biomedical research, this type of trial is carried out as the first evaluation phase to test aspects that, failing on a larger scale, would cause significant economic and time losses. In this case, the authors want to evaluate the effectiveness of the proposed device in the implementation of tVNS, an already accepted therapeutic approach, and the rate and type of adverse effects, as well as its stability operating under real conditions.
Usually, uncontrolled trials are used in early phases of therapeutical device’s development to refine the treatment to be applied. They are also useful to identify treatment tolerance and its interaction with medications. It is known that there is no standard for the stimulation parameters used in tVNS, so the authors proposed a set of values that they intend to continue testing in future trials in order to reach a sample size that supports definitive conclusions.
It is known that uncontrolled trials produce higher estimates of the measured effect than those obtained in a controlled trial, since by not having a control group to act as a reference. The results obtained are usually compared with those obtained in previous studies published by other researchers. In this case, Table 3 shows a comparison with other published studies and authors comment the results.
A single-blind pilot trial was carried out. In this type of trial, the subject does not know the treatment group to which he belongs. In this case, there was only one group but the subjects evaluated did not know. They were only informed that a new therapeutic device was being evaluated for the treatment of refractory epilepsy that could be effective or not.
This point of view was discussed and supported by the two ethical committees involved and the Cuban regulator body approved it.
The first six subjects received tVNS for nine months before evaluating their response and the remaining twelve were treated for six months. The change in the pilot trial duration was due, first of all, to the changes that the coronavirus disease 2019 (COVID-19) pandemic caused in everyone’s lives, it was feared that it would be impossible to conclude the trial. In fact, all studied patients did not start simultaneously as was though initially, so the duration of the pilot trial was greater than the planned. If a patient was infected with the COVID-19 virus, he had to abandon the trial and a new one had to be enrolled to keep the same sample size. This real possibility could change the duration of the trial to several years and the planned was nine months. Secondly, the patients who completed the trial in nine months allowed the authors to define that six months could be a good period to define the response of the patients, the adverse effects that occurred and the operation stability of the proposed device in real working conditions.
The main weakness pointed out to tVNS is that although the recognized benefit it produces among epileptic patients, its application has not been standardized as is common in any medical treatment [7, 8]. The authors propose a therapeutic protocol detailed below:
Duration of therapeutic sessions: 60 min.
Therapeutic sessions per day: 3.
Electrical stimulus: bipolar pulses.
Pulse frequency: 25 Hz.
Pulse width: 200 µs.
Amplitude (applied current): between 1.6 mA and 2.6 mA, depending on the patient’s sensitivity to electrical stimulation. The therapy should be comfortable to avoid patient stress.
The proposed therapy was evaluated with adult patients. In this case, they were aged between 16 years and 65 years, had a MSR of four or greater, subjects with previous epileptic surgery who were classified with an Engel scale III or IV after surgery, and were willing to participate on the pilot trial.
At the end of the pilot trial, patient’s classification was as follow:
Subjects responding to treatment (SRT): MSR decreased by more than 50% at the end of the pilot trial.
Subjects non-responsive to treatment (SnRT): MSR decreased by less than 50% at the end of the pilot trial.
Subjects affected by treatment (SAT): MSR increased by 5% or more at the end of the pilot trial.
For three months, each subject, with a companion, was trained to fill out the crisis and adverse events diary. In these three months of preparation for the pilot trial, the MSR was computed for each patient and its average value was taken as an initial reference. The use of the therapeutic device was also explained to subjects and their respective companion.
Once the subject began therapy, monthly consultations were scheduled to follow up on the completion of the crisis and adverse events diary and any questions that the subject or his companion had. A WhatsApp group was set up to clarify any questions during the pilot trial and technical support was available to repair any breakage of the devices used.
At the end of the pilot trial, each subject was informed how they were classified: SRT, SnRT or SAT. The tests carried out at the beginning of the pilot trial were repeated and the results were compared. Those who responded to treatment continued using this device and they are evaluated every two months.
Eighteen patients were studied in a single blind randomized pilot trial to demonstrate the effectiveness of a proposed therapeutic device. The average age was 29.94 years and they average suffering epilepsy was 19.44 years. The sex representation was almost similar, despite the random nature of the studied sample. General data are shown in Table 1.
General data from patients
| Subject ID | Age | Sex | tVNSstarting date | Years suffering epilepsy | Starting MSR | Location of the epileptic focus |
|---|---|---|---|---|---|---|
| P-01 | 27 | F | 05/16/21 | 8 | 12.50 | Right frontal |
| P-02 | 27 | M | 05/16/21 | 26 | 4.00 | Left parietal |
| P-03 | 44 | M | 06/11/21 | 30 | 6.50 | Occipital |
| P-04 | 32 | F | 06/11/21 | 31 | 173.50 | Right frontal |
| P-05 | 29 | F | 08/15/21 | 9 | 4.50 | Bilateral frontal |
| P-06 | 29 | F | 07/22/21 | 7 | 4.00 | Parietal bilateral |
| P-07 | 18 | F | 02/04/22 | 10 | 5.00 | Mesial bilateral parietal |
| P-08 | 21 | M | 01/14/22 | 11 | 58.00 | Left frontal |
| P-09 | 37 | M | 04/08/22 | 22 | 4.00 | Mesial bilateral |
| P-10 | 19 | M | 04/08/22 | 18 | 4.00 | Left frontal |
| P-11 | 30 | M | 05/06/22 | 16 | 38.00 | Frontral temporal post surgery |
| P-12 | 48 | M | 06/10/22 | 47 | 6.00 | Right frontal |
| P-13 | 33 | F | 05/13/22 | 28 | 9.00 | Temporal mesial bilateral |
| P-14 | 47 | M | 05/20/22 | 31 | 7.00 | Right temporal mesial |
| P-15 | 22 | M | 05/20/22 | 20 | 138.00 | Right frontal |
| P-16 | 21 | M | 05/20/22 | 16 | 163.00 | Left frontal post surgery |
| P-17 | 32 | F | 06/14/22 | 25 | 6.00 | Bilateral frontal |
| P-18 | 23 | F | 06/10/22 | 4 | 65.00 | Bilateral frontal |
F: female; M: male
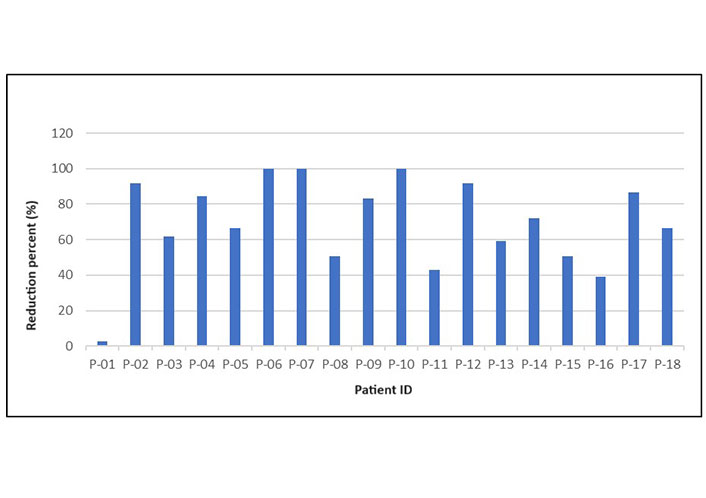
The graph in Figure 2 illustrates the decrease in MSR for each patient.
Other results of the pilot trial are the following:
The monthly seizure-free days increased in all patients classified as SRT, which represents an increase in their quality of life.
Comparing the initial video-EEG test with the same at the pilot trial end, the authors observed a decrease of the epileptiform discharges frequency in all patients who reacted as “responders to the therapy”.
The neuropsychological tests applied conclude that patients classified as SRT demonstrate a greater willingness to social integration and face epilepsy more optimistic, they feel protected with the tVNS.
Clinical analyzes remained without significant changes at the end of the pilot trial.
All data associated with the test is stored in a properly secured repository. The original of manually completed documents is preserved, for example crisis and adverse event diaries. The information captured by the proposed system or digitally imported is stored in a Structured Query Language (SQL) database designed by the authors.
The authors classify the pilot trial outcomes as preliminary due to the sample size, although it is comparable with that of other previously published trials [10, 11]. However, it should be noted that the reached sensitivity confirms the hypothesis that the tested device is a promising tool for refractory epilepsy therapy based on tVNS.
The size of the pilot trial sample was computed using the equation 1:
Here, N is the size of the trial sample, ρ is tabulated coefficient associated with the confidence level; the value 1.96 is assumed, representing a two-tailed test with α = 0.05, S is the standard deviation, e is the maximum allowable error.
The standard deviation of the time suffering from epilepsy of the patients studied was 11.41, and a maximum permissible error of four was assumed. The N value obtained in this way was 13.89 and was extended to 18 for practical considerations. Besides, when reviewing similar trials published from 2012 to date, several reports are based on N values between 12 and 20 patients [12–18].
The MSR behavior throughout the pilot trial is shown in Table 2. In this way, the reader can see that the first six patients were studied for nine months, while the remaining twelve were studied for six months as explained above; that is the meaning of the blank cells.
Seizure monthly rate evolution
| ID | SMSR | M1 | M2 | M3 | TAR1 | M4 | M5 | M6 | TAR2 | M7 | M8 | M9 | TAR3 | SR (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P-01 | 13 | 21 | 13 | 27 | 20.33 | 9 | 23 | 9 | 13.67 | 9 | 6 | 23 | 12.67 | 2.56 |
| P-02 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0.33 | 91.67 |
| P-03 | 7 | 4 | 7 | 4 | 5 | 6 | 5 | 10 | 7 | 5 | 0 | 3 | 2.67 | 61.9 |
| P-04 | 174 | 173 | 49 | 46 | 89.33 | 45 | 52 | 51 | 49.33 | 31 | 30 | 21 | 27.33 | 84.29 |
| P-05 | 5 | 2 | 3 | 1 | 2 | 1 | 0 | 2 | 1 | 3 | 2 | 0 | 1.67 | 66.67 |
| P-06 | 4 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 100 |
| P-07 | 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 100 |
| P-08 | 58 | 34 | 34 | 40 | 36 | 37 | 21 | 28 | 28.67 | - | - | - | - | 50.57 |
| P-09 | 4 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0.67 | - | - | - | - | 83.33 |
| P-10 | 4 | 0 | 1 | 0 | 0.33 | 0 | 0 | 0 | 0 | - | - | - | - | 100 |
| P-11 | 39 | 38 | 18 | 18 | 24.67 | 22 | 28 | 17 | 22.33 | - | - | - | - | 42.74 |
| P-12 | 12 | 8 | 2 | 3 | 4.33 | 2 | 0 | 1 | 1 | - | - | - | - | 91.67 |
| P-13 | 9 | 1 | 5 | 4 | 3.33 | 4 | 3 | 4 | 3.67 | - | - | - | - | 59.26 |
| P-14 | 12 | 8 | 6 | 3 | 5.67 | 2 | 4 | 4 | 3.33 | - | - | - | - | 72.22 |
| P-15 | 163 | 98 | 67 | 150 | 105 | 75 | 95 | 72 | 80.67 | - | - | - | - | 50.51 |
| P-16 | 6 | 5 | 12 | 5 | 7.33 | 0 | 7 | 4 | 3.67 | - | - | - | - | 38.89 |
| P-17 | 65 | 30 | 19 | 6 | 18.33 | 6 | 17 | 3 | 8.67 | - | - | - | - | 86.67 |
| P-18 | 170 | 126 | 146 | 39 | 103.67 | 32 | 61 | 78 | 57 | - | - | - | - | 66.47 |
The MSR behavior throughout the pilot trial. ID: subject identification; SMSR: starting seizure monthly rate; M1, …, M9: month 1 until 9; TAR: trimestral average rate; SR: seizure rate reduction in percent; -: not computed
The pilot trial outcomes are promising. All the recruited patients completed the planned pilot trial time without changes in their antiepileptic drug treatment. A MSR reduction was observed in 17 of them, only a patient kept its MSR almost unchanged. However, two patients with MSR reduction did not classify as SRT because they did not meet the criteria; their MSR did not decreased by more than 50%. No patients worsened their condition after participating in the pilot trial. The graph in Figure 2 illustrates the decrease in MSR for each patient.
Subject P-01 is the only one who practically remains unchanged at the end of the pilot trial, it can be observed in Figure 2. All the others, 17 in total, had a MSR decrease by more than 35%, although the threshold to classify as SRT was set at 50%.
The reported adverse effects did not cause permanent harm or cause any patient to abandon the trial. Five patients reported adverse effects, three presented redness in the stimulation, it was eliminated by slightly moving the placement of the electrodes in the left ear concha. Two other patients reported isolated headache events that disappeared with mild analgesics and did not prevent the treatment application. Similar adverse effects were reported previously [12, 14, 15].
Several studies have been published in the last two decades on the use of tVNS in different pathologies, including refractory epilepsy [12–18]. In the majority of clinical reports or trials, the effectiveness, tolerability and safety of tVNS is determined from the use of different values for the stimulation parameters, which makes it difficult to establish comparisons [8, 19]. However, scientific community agrees that there is a decrease in seizure rate in patients with drug-resistant epilepsy.
The set of a standard for the tVNS treatment is a target to reach, but therapeutic outcomes have demonstrated its utility [19]. The therapeutic sessions and their duration vary, the duration between 20 min and 60 min and the number of sessions between three and five. The frequency of the therapeutic pulses in all the trials reviewed is 20 Hz or 25 Hz, while the pulse width varies between 150 µs and 250 µs. The same current intensity has been applied to all studied patients in some trials, but others have changed this parameter depending of the patient. All studies agree that the therapeutic effects stabilize after the third month, defining by the sixth month whether patients will respond positively to the treatment or not [14–18].
Barbella et al. [14], used very low stimulation currents, between 0.6 mA and 0.8 mA, and a third of their patients decreased their MSR by more than 30% at the end of six months of the trial. This result is very poor compared to those reported by other groups of researchers, so the authors of this paper consider that this outcome is due to the low applied current and propose that this parameter never be less than 1.6 mA.
The 4 mA current applied by Liu et al. [18] seems high for comfortable stimulation sessions, but the duration of these is 20 min, the shortest reported. The authors of this paper consider that patient comfort improves substantially when the applied current is lower. In this way, the therapy is prevented from being stressful for the subject.
Several comparisons are made between tVNS and iVNS. Recently, several scientific teams reported that both approaches involved the same anatomical pathways. Although the mode of action of is unknown, it is thought that it could inhibit the synchronization of the different nuclei that must be discharged in unison for normal electrical activity to become epileptogenic activity [20, 21].
Based on stated above, the selection of stimulation parameters made by the authors seems to be a valid proposal. More than 80% of patients respond to the therapy and only 27.78% of the subjects reported mild adverse effects, without having to abandon the test or causing permanent damage or consequences.
Patients who responded to treatment continue with the tVNS therapy and their MSR are computed every two months. It has been observed a slower MSR decrease, demonstrating a trend to keep stable. Authors considered that patients who did not meet the SRT criteria and continue decreasing their MSR could be classified as “slowly responder to tVNS”.
The outcomes of this research with the corresponding to other previously published is compared in Table 3. The main variable to compare is the “responders” because they reflect the therapeutic effect of the tested device.
Comparison with other published trial outcomes
| Investigation | Seizure | Recruited patients | Patients ending the trial | Duration (months) | Responders | Sensitivity (%) | Seizure freedom |
|---|---|---|---|---|---|---|---|
| Stefan et al. [12], 2012 | Focal/Generalized | 10 | 7 | 9 | 5 | 51.42 | 0 |
| He et al. [15], 2013 | Focal/Generalized | 14 | 13 | 6 | 7 | 53.84 | 4 |
| Aihua et al. [13], 2014 | Focal/Generalized | 60 | 47 | 12 | 24 | 51.06 | N/A |
| Rong et al. [10], 2014 | Focal | 50 | 47 | 6 | 20 | 42.55 | N/A |
| Bauer et al. [9], 2016 | Focal/Generalized | 76 | 58 | 5 | 15 | 25.86 | N/A |
| Barbella et al. [14], 2018 | Focal | 20 | 20 | 6 | 2 | 10.00 | 0 |
| Song et al. [17], 2018 | Focal | 52 | 52 | 1 | 38 | 0 | 0 |
| Liu et al. [18], 2018 | Focal/Generalized | 24 | 17 | 6 | 11 | 64.71 | 0 |
| Current study | Focal | 18 | 18 | 6–9 | 15 | 83.33 | 3 |
N/A: not available
Song’s [17] outcomes demonstrates that one month of therapy is insufficient to see positive results. Reviewing the rest of the trials, six months seem an acceptable time to determine if a patient will respond to tVNS-based therapy. Another aspect to highlight is that tVNS-based therapy only manages to eradicate all seizures as an exception; its main effect is a considerable decrease in the MSR, taking into account that all patients classified as responders decreased their MSR value by more than 50%.
When seeing the results obtained by the authors in Table 3, the sensitivity value stands out, is the highest among the compared trials. This is a partial result because the studied sample is small to set definitive conclusions. The authors will increase the size with new trials under the same conditions.
Outcomes on treatment result predictions are not presented yet because the prediction model need a bigger knowledge base that the available nowadays. The proposed model is based on the multivariate regression standard; it combines variables from the clinical records with age, sex, years suffering epilepsy and the MSR at the beginning of the treatment. The expectation is to get reliable predictions when knowledge base includes information about several hundred of patients with a continuous improvement.
The outcomes demonstrate that the proposed approach is effective. The developed device got the sanitary approval for its clinical use issued by a regulatory body that has approval with those of other countries. A comfortable and effective device was developed and tested successfully; patients learn its use quickly and feel good using this device.
The proposed platform has not been fully evaluated, but the design is flexible and can be adjusted to different scenarios. In fact, in this initial phase the upper layer only stores information to create the knowledge base and does not issue predictions of therapeutic effectiveness for new patients enrolled. The two lower layers have been the basis for the evaluation of the proposed device and have worked satisfactorily, without errors occurring that prevented the development of the pilot test.
The papers reviewed by the authors focus on the testing of a device while the present document discuss a working platform and the evaluation of the therapeutic device are presented.
The proposed system is a promising option for the implementation of a refractory epilepsy therapy service based on tVNS. Nevertheless, new trials are being preparing to reinforce the outcomes with a greater solid statistic.
HDC: hospital data collector
iVNS: vagus nerve stimulation based on active implanted devices
MSR: monthly seizure rate
SCA: system cloud application
SRT: subjects responding to treatment
TAR: trimestral average rate
tVNS: transcutaneous electrical vagus nerve stimulation
VNS: vagus nerve stimulation
RIGF: Conceptualization, Investigation, Writing—original draft. VRV: Conceptualization, Investigation, Validation. JGPB, EVR, and LPH: Conceptualization, Investigation. ASS and JGG: Validation, Supervision. JLHC: Conceptualization, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The pilot trial carried out was approved by the Cuban regulatory body for medical technology and the ethics committees of the Cuban Center for Neuroscience and the Institute of Neurology and Neurosurgery of Havana. Also, the trail complies with Declaration of Helsinki.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
The datasets for this manuscript are not publicly available because of the internal policy of the Cuban regulatory body. Requests for accessing the datasets should be directed to [Rene Ivan Gonzalez-Fernandez, rigf58@yahoo.com].
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Srilaxmi Vityala ... Swathi Nenavath
Joham Choque-Velasquez ... Alder Fernando Valenzuela-Rangel
Kabir Sheikh ... Jeffrey Raskin
Eva Žerovnik
Christine Walker, Chris L. Peterson
Swati Banerjee, Viktor Jirsa
Darrell O. Ricke
Fumiki Yamashita ... Mari Wataya-Kaneda
Jinwei Zhang