 Review
Review

Affiliation:
1Pediatric Unit, Department of Surgical Sciences, Dentistry, Gynecology and Pediatrics, University of Verona, 37134 Verona, Italy
ORCID: https://orcid.org/0000-0001-7746-8267
Affiliation:
1Pediatric Unit, Department of Surgical Sciences, Dentistry, Gynecology and Pediatrics, University of Verona, 37134 Verona, Italy
ORCID: https://orcid.org/0000-0002-8659-5505
Affiliation:
2Department of Maternal Infantile and Urological Sciences, Sapienza University of Rome, 00161 Rome, Italy
ORCID: https://orcid.org/0000-0002-2476-1790
Affiliation:
3Unit of Pediatrics, Department of Woman, Child and General and Specialized Surgery, University of Campania ‘Luigi Vanvitelli’, 80138 Naples, Italy
ORCID: https://orcid.org/0000-0003-4295-4163
Affiliation:
1Pediatric Unit, Department of Surgical Sciences, Dentistry, Gynecology and Pediatrics, University of Verona, 37134 Verona, Italy
ORCID: https://orcid.org/0000-0002-3537-696X
Affiliation:
1Pediatric Unit, Department of Surgical Sciences, Dentistry, Gynecology and Pediatrics, University of Verona, 37134 Verona, Italy
Email: giorgio.piacentini@univr.it
ORCID: https://orcid.org/0000-0003-1324-4373
Explor Med. 2026;7:1001415 DOI: https://doi.org/10.37349/emed.2026.1001415
Received: December 23, 2025 Accepted: April 16, 2026 Published: July 14, 2026
Academic Editor: Irfan Rahman, University of Rochester Medical Center, USA
The article belongs to the special issue Asthma in Children: Origins, Endotypes and Future Perspectives
Early-life oxidative stress, resulting from an imbalance between reactive oxygen species (ROS) and reactive nitrogen species (RNS) and antioxidant defenses, has increasingly been proposed as an important contributor to the developmental origins of childhood asthma. Prenatal and early postnatal exposures—including pollutants, tobacco smoke, maternal distress, nutritional imbalance, and allergen-derived oxidase activity—may disrupt epithelial integrity and redox-regulated immune pathways, potentially predisposing the developing lung to allergic inflammation. To synthesize current mechanistic and epidemiologic evidence on how oxidative stress during early life may contribute to asthma development, with particular focus on environmental drivers, redox–immune interactions, and gene-environment susceptibility. A structured review of PubMed, Scopus, and Embase identified peer-reviewed English-language studies from birth cohorts, mechanistic models, and biomarker analyses evaluating oxidative stress, antioxidant capacity, and asthma-related outcomes. Environmental oxidants and nutritional deficiencies may increase ROS production, promoting epithelial injury, activation of redox-sensitive pathways such as NF-κB and MAPK, and the release of epithelial alarmins including IL-33, IL-25, and thymic stromal lymphopoietin (TSLP). These signals can influence innate immune activation and antigen-presenting cell function, favoring Th2/Th17-biased immune responses. Genetic variants in antioxidant pathways, including GSTM1, GSTP1, and Nrf2, may further modify susceptibility to oxidant exposures. Epidemiologic studies from birth cohorts report associations between early-life oxidative exposures, reduced lung growth, wheezing, allergic sensitization, and asthma risk. Current mechanistic and epidemiologic evidence suggests that oxidative stress may represent an important biological pathway linking early-life environmental exposures with asthma susceptibility, although further studies are needed to clarify its role within the complex network of factors contributing to asthma development.
Asthma is one of the most common chronic diseases of childhood and represents a major global health burden. Increasing evidence suggests that susceptibility to asthma may originate early in life, during critical periods of lung and immune system development. This concept is consistent with the developmental origins of health and disease (DOHaD) framework, which proposes that environmental exposures during prenatal and early postnatal life can shape long-term respiratory and immune outcomes [1]. Among the biological mechanisms proposed to link early-life exposures to asthma development, oxidative stress has emerged as an important pathway. Oxidative stress refers to an imbalance between the production of reactive oxygen species (ROS) and reactive nitrogen species (RNS) and the capacity of antioxidant defenses to neutralize them. At physiological levels, redox signaling participates in normal cellular communication and immune regulation. However, excessive oxidant generation can disrupt epithelial integrity, modify cellular signaling pathways, and promote inflammatory responses relevant to airway disease [2]. Multiple prenatal and early-life exposures can increase oxidative burden. Air pollution, tobacco smoke, maternal psychological distress, nutritional imbalance, and allergen-derived oxidase activity can all generate ROS within the developing lung. At the same time, antioxidant defense systems in the fetus and young infant are relatively immature, potentially increasing vulnerability to oxidant injury. Genetic variation in key antioxidant pathways, including glutathione S-transferases and the Nrf2 signaling system, may further influence individual susceptibility to these environmental exposures [3, 4]. Experimental and epidemiologic studies increasingly support a role for oxidative stress in shaping respiratory and immune development. Oxidative imbalance has been linked to epithelial barrier dysfunction, activation of redox-sensitive inflammatory pathways, and altered immune programming that favors allergic responses. Birth cohort studies further suggest that early-life oxidant exposures are associated with reduced lung growth, increased wheezing, allergic sensitization, and the subsequent development of asthma [5–7].
The purpose of this review is to synthesize current mechanistic and epidemiologic evidence on the role of oxidative stress in the developmental origins of childhood asthma. We examine environmental and prenatal drivers of oxidative imbalance, genetic susceptibility factors, and emerging insights into how redox signaling interacts with immune programming during early life. Finally, we discuss the potential clinical implications of these findings and highlight key limitations and areas requiring further investigation. The aim of this review is therefore to critically examine current mechanistic and epidemiologic evidence on oxidative stress in early-life asthma development, while acknowledging the complexity and multifactorial nature of the disease.
Oxidative stress in the developing lung reflects the interaction between environmental oxidant exposures and the capacity of endogenous antioxidant defense systems. During fetal and early postnatal life, antioxidant defenses are still maturing, which may increase vulnerability to oxidant injury. Multiple environmental and maternal factors have been associated with increased oxidative burden during these critical developmental periods.
Exposure to ambient air pollution is one of the most consistently studied sources of oxidative stress relevant to asthma development. Pollutants such as particulate matter (PM), nitrogen dioxide (NO2), ozone, and diesel exhaust particles can generate ROS in airway epithelial cells and lining fluids. Epidemiological studies report associations between prenatal or early-life exposure to traffic-related air pollution and impaired lung growth, increased wheezing, and higher asthma risk [8, 9].
Genetic susceptibility may modify these effects. Variants in genes regulating antioxidant defenses, including glutathione S-transferases and the Nrf2 pathway, have been shown to influence vulnerability to oxidant-induced airway injury [5].
Adequate nutrition supports antioxidant systems that protect the lung from oxidative injury. Both enzymatic and non-enzymatic defenses depend on micronutrients such as vitamins C, D, and E, and trace elements including zinc and selenium. Deficiencies in these nutrients may compromise the ability to neutralize ROS [10]. Several epidemiologic studies report associations between maternal dietary patterns and respiratory outcomes in offspring. Diets rich in fruits and vegetables have been linked with lower risks of wheezing or allergic disease in some populations, although findings remain heterogeneous [11].
Tobacco smoke represents a major source of oxidative stress during early life. Maternal smoking during pregnancy has been consistently associated with wheezing, impaired lung function, and childhood asthma. Both prenatal and second-hand smoke exposure may disrupt redox balance in the developing lungs and alter pathways involved in immune regulation and airway growth [12]. Gene-environment interactions have also been described, with variants in antioxidant pathways influencing susceptibility to smoke-related respiratory outcomes [13].
Maternal health conditions during pregnancy, including asthma and psychological stress, may contribute to oxidative imbalance in the fetal environment and influence immune programming [14]. Certain allergens, such as house dust mite and pollen extracts, can also promote oxidative stress in airway epithelial cells and enhance innate immune activation [15, 16]. Some medications and environmental exposures have been proposed to influence oxidative balance during early life. For example, epidemiological studies have reported associations between early-life acetaminophen exposure and asthma risk, possibly related to glutathione depletion [17, 18]. However, findings remain inconsistent, and causal relationships are uncertain. In summary, a range of prenatal and early-life exposures—including pollution, tobacco smoke, nutritional factors, maternal health conditions, allergens, and certain medications—may contribute to oxidative imbalance during critical stages of lung and immune development. These exposures likely interact with genetic susceptibility and other biological pathways to influence respiratory outcomes later in life.
Evidence from birth cohort and epidemiological studies increasingly suggests that oxidative stress may contribute to the development of asthma and related respiratory outcomes during childhood. Early-life exposure to environmental oxidants—including air pollution, tobacco smoke, and other pro-oxidant factors—has been associated with impaired lung growth, increased wheezing, allergic sensitization, and a higher risk of asthma in several longitudinal studies [1]. Traffic-related air pollution is among the most consistently studied exposures in this context. Findings from large prospective cohorts such as the Children’s Health Study (CHS) in California [19], the BAMSE cohort in Sweden [20], and the ALSPAC birth cohort in the United Kingdom [21] have reported associations between prenatal or early-life exposure to PM and NO2 and increased respiratory symptoms, allergic sensitization, and asthma development. These pollutants are known to generate ROS within airway epithelial cells and lung lining fluids, potentially contributing to oxidative injury and inflammatory signaling [21]. Gene-environment interactions may further influence susceptibility to oxidant exposures. Variants in genes regulating antioxidant defenses, including GSTM1 and GSTP1P, have been shown to modify the respiratory effects of air pollution and tobacco smoke in several cohort analyses. Children with reduced antioxidant capacity appear to be more vulnerable to oxidant-induced airway inflammation and impaired lung development [22, 23]. Nutritional factors may also influence oxidative balance during early life. Some birth cohort studies have reported associations between maternal or early childhood dietary patterns and respiratory outcomes, with diets rich in antioxidant-containing foods—particularly fruits and vegetables—being linked to lower prevalence of wheezing or allergic disease in certain populations, although findings remain heterogeneous [24]. Overall, epidemiological evidence supports the concept that oxidative exposures during critical periods of lung and immune development may influence respiratory trajectories and asthma susceptibility. However, findings across birth cohort studies are not entirely consistent, reflecting differences in exposure assessment, population characteristics, genetic susceptibility, and study design. Conversely, enhanced antioxidant defenses confer protection. Unconjugated bilirubin, a potent endogenous antioxidant and ROS scavenger, shows inverse dose-dependent associations with recurrent wheeze and childhood asthma in ECHO-CREW birth cohorts, with higher concentrations correlating with fewer wheezing episodes and lower asthma risk at 5–6 years [25]. Diet modulates respiratory health through oxidative stress pathways. It has been shown that eating fresh fruit can improve lung function in children [26]. In 2359 children from the Swedish birth cohort BAMSE, higher total antioxidant capacity of the diet at age 8 years was associated with a decreased risk of developing sensitization to inhalant allergens and asthma from childhood to adolescence [24]. In school-aged children, a high intake of fruit was associated with a significantly lower incidence of new respiratory allergic symptoms, including asthma and rhinitis. Moreover, among children who already had asthma at baseline, those with higher fruit consumption showed a greater likelihood of symptom remission over the four-year follow-up [27]. Those findings indicate that fruit-rich diets may contribute not only to the prevention of allergic and asthmatic symptoms but also to their potential regression. On the other hand, high intake of refined carbohydrates increases asthma prevalence and severity through elevated OS, glycolytic metabolism shifts, and reduced antioxidant defenses [28], thereby amplifying the impact of environmental stressors. High intake of refined carbohydrates promotes a glycolytic shift, whereby airway epithelial cells and immune cells increasingly rely on glycolysis rather than mitochondrial oxidative phosphorylation for energy production. This metabolic reprogramming is driven by excess glucose availability and insulin-mediated signaling, leading to increased lactate production, intracellular acidification, and reduced mitochondrial efficiency. All those findings suggest that diet can either worsen or protect against the OS pathways that contribute to asthma. Although these epidemiologic associations are consistent with mechanistic evidence linking oxidative stress to airway inflammation, the largely observational nature of current studies limits causal inference and highlights the need for further integrative research.
Oxidative stress has increasingly been recognized as an important modulator of immune responses involved in allergic disease. Rather than acting as an isolated pathogenic factor, oxidative imbalance may create a biological environment that facilitates allergic sensitization and airway inflammation [29]. Experimental studies in both animal models and humans suggest that increased oxidative burden can influence epithelial signaling, innate immune activation, and adaptive immune responses relevant to asthma development [30]. This study demonstrates that pre-existing inadequate antioxidant defenses create a permissive biological environment that facilitates allergic sensitization, establishing oxidative vulnerability as a prerequisite rather than a consequence of allergy development. OS is not merely a bystander in allergic disease—it is an active initiator and amplifier of immune dysregulation. OS triggers innate immune activation at mucosal surfaces, reprograms antigen-presenting cell metabolism and signaling, and guides adaptive immune polarization toward Th2/Th17-biased allergic responses. Through innate epithelial activation, antigen-presenting cell metabolic reprogramming, and adaptive immune skewing, ROS creates a self-reinforcing loop of allergic inflammation as illustrated in Figure 1 and described below.
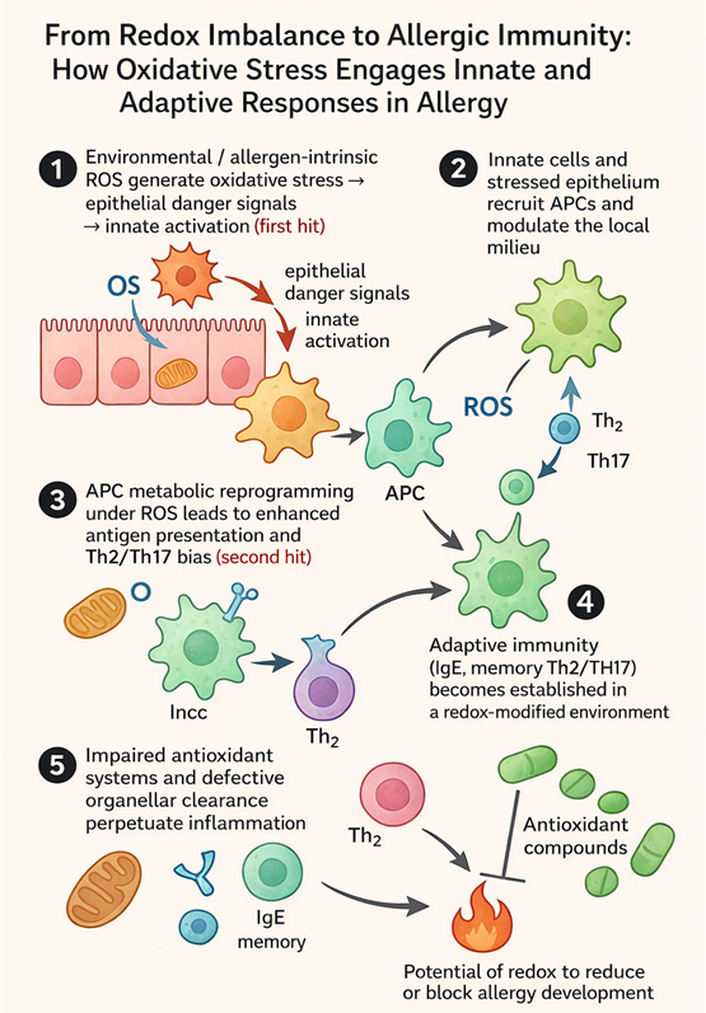
Sequential steps in OS-driven allergy sensitization development. (1) Environmental or allergen-derived reactive oxygen species (ROS) induce epithelial oxidative stress, leading to the release of danger signals and activation of innate immunity (first hit). (2) Activated epithelial and innate immune cells recruit and modulate antigen-presenting cells (APCs), shaping the local inflammatory milieu. (3) Under ROS conditions, APCs undergo metabolic reprogramming, enhancing antigen presentation and promoting a Th2/Th17-skewed response (second hit). (4) This environment supports the development of adaptive immunity characterized by IgE production and memory Th2/Th17 responses. (5) Impaired antioxidant defenses and defective organelle clearance sustain oxidative stress and chronic inflammation. Antioxidant compounds may counteract these processes and reduce or prevent allergy development.
Environmental oxidants—including air pollutants, tobacco smoke, and allergen-derived oxidase activity—can generate ROS within the airway epithelium and lining fluids. In addition to causing cellular injury, these reactive molecules also function as signaling mediators that activate redox-sensitive transcription pathways such as NF-κB and AP-1. Activation of these pathways promotes the production of inflammatory mediators and can alter epithelial barrier integrity, both of which are important early events in allergic airway disease [31].
Airway epithelial cells represent a key interface between environmental exposures and the immune system. Oxidative stress within the epithelium can stimulate the release of epithelial-derived cytokines and danger signals—including IL-33, IL-25, and thymic stromal lymphopoietin—which are known to activate innate immune pathways associated with type-2 inflammation. These signals promote the recruitment and activation of immune cells such as dendritic cells, eosinophils, mast cells, and group-2 innate lymphoid cells, thereby amplifying local inflammatory responses [31]. ROS may also contribute to mitochondrial stress and the generation of oxidized lipids and nucleotides, which can further stimulate innate immune signaling and inflammasome activation. Together, these processes may create an inflammatory airway environment that favors allergic sensitization [32].
Oxidative stress can also influence the function of antigen-presenting cells. Dendritic cells exposed to oxidant stress or oxidatively modified proteins may display altered antigen processing and cytokine production. Experimental studies suggest that oxidative conditions can promote the expression of costimulatory molecules and inflammatory cytokines that favor T-helper cell differentiation toward allergic immune responses [31]. In addition, oxidative modification of proteins may generate neo-antigens that enhance immune recognition. These changes may increase the likelihood that environmental allergens trigger adaptive immune activation [33].
Through these mechanisms, oxidative stress may contribute to immune polarization toward type-2 and type-17 responses, both of which are implicated in asthma pathophysiology. Reduced activity of antioxidant pathways—such as diminished glutathione availability or impaired Nrf2 signaling—may further amplify inflammatory signaling and sustain airway immune activation [34]. Although these processes have been demonstrated primarily in experimental models, they provide a biologically plausible framework linking environmental oxidant exposures to the development of allergic inflammation.
Individuals with reduced antioxidant capacity may be less able to counteract oxidant-induced immune activation. Genetic variation in antioxidant pathways, chronic environmental exposures, or metabolic factors may contribute to persistent redox imbalance. Sustained oxidative stress may therefore promote prolonged inflammatory signaling, airway remodeling, and chronic disease progression [35]. Overall, current evidence suggests that oxidative stress may influence multiple stages of allergic immune development, from epithelial barrier disruption to innate immune activation and adaptive immune polarization. While oxidative imbalance is unlikely to act as a single causal mechanism, it may represent an important biological pathway through which environmental exposures interact with host susceptibility to shape asthma risk [4].
Persistent oxidative stress may contribute not only to asthma initiation but also to disease progression and severity [36]. Elevated urinary bromotyrosine—a stable eosinophil-derived oxidative marker—predicts poor asthma control and exacerbations in children better than conventional markers (IgE, eosinophils, spirometry, exhaled nitric oxide), conferring an 18.1-fold increased risk of inadequate control and a 4.0-fold increased exacerbation risk [37]. In house dust mite-challenged patients, baseline oxidative damage (elevated 4HNE-protein adducts, carbonylated proteins) correlates with greater late-phase FEV1 decline, indicating that preexisting redox imbalance primes airways for exaggerated allergen responses [38]. Excessive ROS impairs the protective Nrf2 pathway while activating NF-κB signaling, increasing inflammatory mediator release and overstimulating airway smooth muscle cells, promoting hypertrophy and hypercontractility that amplify inflammation and bronchial obstruction [39]. Increased production of ROS in the airway can promote epithelial injury, mucus hypersecretion, and airway remodeling, processes that are associated with chronic inflammation and reduced lung function in children with asthma [40]. Clinically, this raises concern that processes set in motion by repeated or early-life exacerbations—cumulative airway injury, remodeling and progressive airflow limitations— may not be fully reversible and can progress despite standard anti-inflammatory treatment. Consistent with this, the CAMP study found that about one quarter of children experienced significant annual declines in post-bronchodilator FEV1 % predicted, with similar trajectories in the budesonide and placebo groups, indicating that routine inhaled corticosteroid (ICS) dosing did not avert long-term functional deterioration [41]. The children with significant lung function decline did not have more severe symptoms or greater medication use but showed higher airway eosinophilia during ICS washout, indicating that residual inflammation and remodeling persist despite corticosteroid therapy. Declines began early in life, suggesting airway structural changes develop before or independently of corticosteroid-responsive inflammation, likely because underlying mechanisms such as OS-driven remodeling or corticosteroid-insensitive inflammation remain unaddressed. Confirming this mechanism, Baraldi et al. [42] clearly demonstrate that OS persists in asthmatic children despite treatment with ICSs. Using exhaled 8-isoprostane as a noninvasive marker of lipid peroxidation, the authors found that both steroid-naïve and steroid-treated children with asthma had significantly elevated 8-isoprostane levels compared with healthy controls, with no significant difference between the two asthmatic groups. This indicates that ICS therapy, though effective in suppressing airway inflammation and reducing nitric oxide levels, does not attenuate the oxidative component of airway injury. Consistent with this, findings from the CAMP study show that asthmatic children treated with ICS who are exposed to air pollutants experience greater bronchial hyperreactivity than the placebo group [43]. This effect can be explained biologically by the fact that ICS improves airway caliber and ventilation, thereby increasing the volume of inhaled pollutants that reach the distal airways. Pollutants such as CO, NO2, and O3 generate ROS/RNS that amplify OS, which corticosteroids cannot counteract. The resulting activation of redox-sensitive pathways (e.g., NF-κB and MAPK) enhances airway smooth-muscle contractility and hyperresponsiveness [39]. Oxidative imbalance may also amplify inflammatory signaling pathways involved in asthma exacerbations. Activation of redox-sensitive transcription factors, including NF-κB, can enhance the production of pro-inflammatory cytokines and chemokines, sustaining airway inflammation and contributing to disease persistence. Although asthma is primarily a respiratory disorder, systemic effects of oxidative stress have also been suggested. Some studies indicate that chronic airway inflammation may be associated with systemic inflammatory responses [44]. However, evidence linking pediatric asthma with broader systemic outcomes remains limited, and further research is needed to clarify the clinical relevance of these observations.
Although the evidence linking oxidative stress to asthma development is largely mechanistic and observational, it has important implications for preventive strategies in pediatric practice. Because many sources of oxidative stress arise from modifiable environmental exposures, early-life risk reduction represents a realistic clinical target.
First, minimizing exposure to environmental pollutants is critical. Prenatal and early childhood exposure to traffic-related air pollution, tobacco smoke, and indoor pollutants has consistently been associated with increased oxidative stress and higher asthma risk. Counseling families regarding smoking avoidance, improvement of indoor air quality, and reduction of exposure to heavy traffic environments represents an important preventive measure [6, 7]. Maternal health and nutrition during pregnancy may also influence oxidative balance in the developing fetus. Diets rich in fruits, vegetables, and micronutrients with antioxidant properties have been associated with improved respiratory outcomes in several birth cohort studies [45, 46]. Although direct antioxidant supplementation lacks sufficient evidence to be recommended for asthma prevention, encouraging balanced maternal nutrition remains a reasonable strategy. In childhood, dietary patterns characterized by high intake of fruits, vegetables, and whole foods may support endogenous antioxidant defenses and potentially mitigate oxidative stress–related airway inflammation. Conversely, diets high in refined carbohydrates and ultra-processed foods may contribute to oxidative imbalance and inflammatory metabolic shifts [10]. Taken together, these observations support the concept that reducing early-life oxidative burden through environmental control and healthy lifestyle strategies may represent an important component of asthma prevention [11]. Future clinical trials will be necessary to determine whether targeted antioxidants or metabolic interventions can further modify disease risk.
Despite growing interest in oxidative stress as a contributor to asthma pathogenesis, several important limitations should be acknowledged. First, much of the epidemiologic evidence linking oxidative stress to asthma development is observational. Birth cohort studies consistently demonstrate associations between oxidant exposures, oxidative biomarkers, and respiratory outcomes, but these findings cannot establish direct causality. Environmental exposures often coexist with other social, nutritional, and genetic factors that may confound these associations. Second, biomarkers of oxidative stress remain heterogeneous and imperfect. Measures such as isoprostanes, oxidized lipids, and glutathione-related metabolites capture only specific components of redox imbalance and may vary depending on sampling methods, biological matrices, and timing of measurement. Standardization of oxidative stress biomarkers remains an important challenge for the field. Third, genetic susceptibility to oxidative injury varies across populations. Variants in genes regulating antioxidant defenses—including GSTM1, GSTP1, and Nrf2—modify the effects of environmental exposures. However, the magnitude and consistency of these gene–environment interactions differ between cohorts, reflecting population heterogeneity and methodological differences.
Finally, interventional studies targeting oxidative stress have produced mixed or inconclusive results. Trials of single antioxidant supplementation have generally failed to demonstrate clear clinical benefit in asthma prevention or treatment. These findings suggest that oxidative stress likely interacts with multiple biological pathways—including immune regulation, microbiome composition, and epigenetic programming—rather than acting as an isolated causal factor. Recognizing these limitations is essential to place current findings within an appropriate scientific context. Oxidative stress should therefore be viewed not as a single causal mechanism, but as part of a broader network of environmental and biological processes contributing to asthma development.
The evidence reviewed here indicates that oxidative stress is an important biological pathway linking prenatal and early-life environmental exposures to asthma susceptibility. Pollutants, tobacco smoke, nutritional factors, maternal health conditions, and allergens can generate oxidative imbalance during critical windows of lung and immune development, potentially influencing epithelial integrity, immune programming, and respiratory growth trajectories. Epidemiologic studies consistently demonstrate associations between early-life oxidant exposures, reduced antioxidant defenses, and increased risk of wheeze, allergic sensitization, and asthma. At the same time, enhanced antioxidant capacity—through endogenous mechanisms or diet—appears to confer partial protection in several cohort studies. While oxidative stress likely represents a significant contributor to asthma pathogenesis, it should be considered within a complex network of interacting environmental, genetic, metabolic, and immunologic factors. Further longitudinal and interventional studies are required to clarify the causal role of oxidative pathways and to determine whether targeted strategies aimed at reducing early-life oxidative burden can effectively prevent asthma development.
ICS: inhaled corticosteroid
NO2: nitrogen dioxide
PM: particulate matter
RNS: reactive nitrogen species
ROS: reactive oxygen species
MP: Conceptualization, Methodology, Data curation, Resources, Writing—original draft, Writing—review & editing. MZ: Resources, Writing—review & editing. AMZ: Resources, Writing—review & editing. CC: Resources, Writing—review & editing. ALB: Conceptualization, Supervision, Writing—review & editing. GP: Conceptualization, Supervision, Writing—review & editing. All authors read and approved the submitted version.
Attilio L. Boner reports that a close family member owns a company producing nutraceutical products with antioxidant properties (including Auxilie Immuplus tablets and sachets). The author has no direct financial involvement in the company, and the present work was conducted independently of any commercial influence. The other authors declare no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
The authors received no specific funding for this work.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 281
Download: 9
Times Cited: 0
Hannah Norman-Bruce ... P. Jane McDowell
Michele Piazza ... Diego Peroni
