Original Article
Original Article

Affiliation:
1Faculty of Pharmacy, Applied Science Private University, Amman 11937, Jordan
ORCID: https://orcid.org/0009-0007-7361-0394
Affiliation:
2Faculty of Pharmacy, The University of Jordan, Amman 11942, Jordan
ORCID: https://orcid.org/0000-0002-7861-1958
Affiliation:
1Faculty of Pharmacy, Applied Science Private University, Amman 11937, Jordan
ORCID: https://orcid.org/0000-0003-2742-7285
Affiliation:
3Department of Pharmacy Practice, College of Clinical Pharmacy, Hodeidah University, Al Hodeidah 3114, Yemen
Email: mhzawiah@gmail.com
ORCID: https://orcid.org/0000-0002-3325-1442
Affiliation:
1Faculty of Pharmacy, Applied Science Private University, Amman 11937, Jordan
ORCID: https://orcid.org/0000-0001-8298-4071
Explor Med. 2025;6:1001379 DOI: https://doi.org/10.37349/emed.2025.1001379
Received: September 26, 2025 Accepted: December 08, 2025 Published: December 22, 2025
Academic Editor: Hongzhou Lu, Shenzhen Third People’s Hospital, National Clinical Research Center for Infectious Diseases, China
Aim: Community-acquired pneumonia (CAP) is a leading cause of global morbidity and mortality, and it is often treated with fluoroquinolone antibiotics. Misuse of fluoroquinolones is a known driver of antimicrobial resistance, and de-escalation of antibiotics is not only effective for patient outcomes but also reduces resistance. The aim of this study was to assess the association of fluoroquinolone de-escalation with length of stay (LOS), mortality, and other microbiological culture results in hospitalized adults with CAP.
Methods: A retrospective cohort investigation took place with adult patients suspected of CAP in a tertiary care center in Jordan. The study examined outcomes for fluoroquinolone de-escalation that included hospital LOS, mortality, and examined the relationship between the results of microbial cultures and the outcome of de-escalation.
Results: The study sample consisted of 125 patients with a median age of 73 years [interquartile range (IQR) = 24]. Around 65% (n = 81) of the patients were male, and 35% (n = 44) were female. The fluoroquinolone therapy was mostly levofloxacin (99.2%, n = 124). Fluoroquinolone de-escalation was medically justified in 32.8% (n = 41) of patients. When comparing the rate of successful de-escalation between those with positive and negative cultures (after the exclusion of 3 patients), positive cultures were statistically more likely to de-escalate than negative cultures, 61.5% (16/26) to 26.0% (25/96) (p = 0.002). Patients in the successful de-escalation had a statistically shorter length of hospital stay; 12 days (IQR = 8) against the failed/inappropriate group, 18 days (IQR = 11) (p = 0.004). There was no significant difference in mortality; 70.1% (n = 29) survived in the de-escalated group and 76.5% (n = 62) in the failed/inappropriate group (p = 0.514).
Conclusions: In CAP, fluoroquinolone de-escalation may result in shorter hospital stays but does not alter mortality rates. However, limitations in establishing appropriateness for de-escalation imply the need for further studies to validate the findings.
Community-acquired pneumonia (CAP), a common and serious lung infection, is one of the leading causes of morbidity and mortality worldwide. In the United States alone, CAP results in approximately 1.5 million hospitalizations annually [1], while globally, it accounts for approximately three million deaths each year [2]. CAP is caused by a variety of infectious agents, including bacteria, viruses, and fungi, with bacterial infections being the most prevalent [3].
The rise of microbial resistance is a significant worldwide health issue, leading to more difficult infection treatment, greater morbidity and mortality, and increased healthcare costs. Since the advent of antibiotics, misuse and overuse of antibiotics in healthcare and agriculture have been a significant contributor to the crisis [4–7]. Furthermore, bacterial resistance continues to develop through mutation and horizontal gene transfer [7]. The COVID-19 pandemic has resulted in increased prevalence of antimicrobial resistance. A survey revealed that 40.6% of the individuals who had an antibiotic prescription stopped taking it without consulting a provider, a practice that contributed to an increase in resistance [8].
Due to the increased concern for antimicrobial resistance, antibiotic stewardship initiatives such as antibiotic de-escalation have emerged to be an essential part of clinical decision-making [9]. De-escalation of antibiotic therapy typically consists of adopting empirical broad-spectrum antibiotics and waiting for the results of pathogen susceptibility testing before employing a targeted therapy [10, 11]. The philosophy behind this approach is to reduce unnecessary antibiotic exposure while still providing effective clinical treatment, thus improving patient care and outcomes [9–11]. The evaluation of antibiotic de-escalation strategies has primarily focused on hospital length of stay (LOS) and mortality rates [12].
Fluoroquinolones, such as ciprofloxacin, levofloxacin, and moxifloxacin, are broad-spectrum antibiotics used to treat pneumonia due to their potent activity against a range of bacterial pathogens [13–15]. Although current Infectious Diseases Society of America (IDSA) guidelines recommend beta-lactams as the first empiric therapy for most patients with CAP, fluoroquinolones continue to be used in many practices [13–15]. In consideration of the fluoroquinolone’s broad-spectrum antibiotics and the emerging concern of resistance, especially among pathogens like Escherichia coli and Pseudomonas aeruginosa, it is important to examine its management [16]. Because of the growing resistance, it is timely to examine effective antibiotic management strategies, like de-escalation, to minimize the risk of further resistance.
Although antibiotic de-escalation has documented benefits for reducing antimicrobial resistance and improving patient outcomes in select situations, there is limited evidence regarding the use of antibiotic de-escalation in fluoroquinolone therapy for pneumonia patients. For this reason, this study aims to evaluate the rate and outcomes of antibiotic de-escalation in additional CAP patients treated with fluoroquinolones and de-escalated to a narrower spectrum with 48 h of culture and sensitivity results. In particular, we are examining the clinical outcomes of patients who experienced adherence to de-escalation successfully and then consider the outcomes of patients in whom de-escalation was not appropriate, examining hospital LOS and all-cause mortality.
This was a retrospective cohort observational study conducted at Jordan University Hospital (JUH) to assess the rate and outcomes of fluoroquinolone de-escalation in patients who were diagnosed with CAP from December 2022 to March 2024. The population of interest was adults aged ≥ 18 years with a suspected diagnosis of CAP (CAP is defined as an acute infection of the pulmonary parenchyma acquired in the community or within 48 h of admission). We only included those patients who had a positive CAP diagnosis using the ICD-10 diagnostic codes. Other inclusion criteria were: the patients had blood and sputum cultures ordered, received a fluoroquinolone regimen of therapy as the empiric treatment regimen, and were admitted to the hospital until cultures and sensitivity were performed. We excluded patients who were pregnant, were not certain of their diagnosis, and/or had incomplete data. Severity of illness was not assessed in the study.
The Raosoft sample size calculator was used to calculate the sample size for this study with a 10% margin of error, a 95% confidence level, and an expected proportion of successful de-escalation of 50%. Based on these parameters, the minimum sample size required was calculated to be 96 patients.
The study was conducted in accordance with the principles outlined in the World Medical Association Declaration of Helsinki. It received approval from the JUH Institutional Review Board (approval number 10/2024/1389). To ensure patient confidentiality, all data were de-identified and anonymized. Given the retrospective, observational design, the ethical committee granted a waiver for informed consent.
Data collection comprised the gathering of extensive information from the medical records of eligible patients using a planned data collection form. Collected data included demographic data such as age, gender, admission date, discharge date, and LOS. We gathered clinical data, including diagnoses, empiric antibiotic therapy (including name, route of administration, and duration of therapy), and information related to targeted antibiotics after culture results. We also collected laboratory data that included blood and sputum cultures and their sensitivity results to study the susceptibility patterns of the microbiological pathogens that caused CAP.
The main aim of this research is to assess the rate of antibiotic de-escalation in patients with CAP who were treated with fluoroquinolones. The term de-escalation means moving from broad-spectrum antibiotics (fluoroquinolones) to a narrower spectrum of antibiotics based on final culture and sensitivity results. The narrower-spectrum antibiotics to consider would be cephalosporins, penicillins, trimethoprim/sulfamethoxazole, vancomycin, or linezolid. This approach is used to decrease antibiotic use, and de-escalation might also include discontinuation of antibiotics if cultures do not demonstrate any infection, ideally within 48 h of culture results. Patients were grouped together for analysis into two primary groups based on whether or not they required de-escalation. Patients were down-graded based on final culture and sensitivity results. Patients with positive cultures for atypical bacteria or MRSA were not considered possible candidates for fluoroquinolone de-escalation because fluoroquinolones could likely be indicated as part of the treatment of patients with atypical bacteria or MRSA. Patients categorized as requiring de-escalation were further divided into successful de-escalation, failed de-escalation, and inappropriate de-escalation.
Failed de-escalation pertains to interventions where empiric antibiotics were continued after culture results yielded no definitive evidence to continue antibiotic therapy and/or when broad-spectrum antibiotics were continued after the patient was cultured and a narrower-spectrum antibiotic was more appropriate. Inappropriate de-escalation corresponds to errors or missed opportunities that deteriorate patient care. For example, in the case of negative culture results related to inappropriate de-escalation, transition to narrower-spectrum antibiotics could occur when the very best approach would have been to discontinue antibiotic therapy altogether. In contrast, if positive culture results were obtained, a scenario of inappropriate de-escalation could be where antibiotics are discontinued instead of switched to more directed therapy when more directed therapy would have been of greater benefit for patient care.
Assessment of the adequacy or appropriateness of antibiotics was based on culture and sensitivity, as well as the IDSA guidelines. It should be noted that the decision regarding adequacy or appropriateness of antibiotic therapy did not incorporate patient-specific clinical variables such as the severity of illness or other comorbidities.
The secondary outcomes of the study included assessing various factors among patients who underwent successful de-escalation compared with those who did not successfully de-escalate treatment or performed de-escalation incorrectly after excluding inappropriate de-escalation of antibiotics (e.g., antibiotics were stopped instead of de-escalating towards a narrower spectrum medication following a positive culture). Secondary outcomes assessed included the LOS and in-hospital mortality, which was defined as any death occurring while the patient was still admitted and did not have to be related to the reason for admission. The study also assessed the success rates of fluoroquinolone de-escalation among patients with a positive culture versus a negative culture.
Analysis of the data was conducted using version 26 of the IBM SPSS software. Descriptive statistics presented frequencies and percentages for categorical variables and medians and interquartile range (IQR) for continuous variables. Normality of the data was tested using the Shapiro-Wilk test. Fisher’s exact test was used to compare all-cause in-hospital mortality between patients who were successfully de-escalated and those who failed or were inappropriately de-escalated. The Mann-Whitney U test was used to describe the LOS. To assess the association between the microbial culture results and de-escalation practice, the Chi-square test was used. All statistical tests were two-tailed, and significance was determined by p < 0.05.
A total of 125 patients met eligibility criteria after screening for inclusion criteria during the study. The median age of participants was 73 years old (IQR = 24). The number of female patients was 44 (35.2%) and 81 male patients (64.8%). The median LOS for all patients was 13 days (IQR = 11). In addition, 93 patients (74.4%) survived the hospital stay, while 32 patients (25.6%) died while in the hospital. Among the patients, 20 (16%) were transferred to the ICU, 100 (80%) stayed in the general ward, and 5 patients (4%) were in the ICU upon admission. Table 1 summarizes the demographic and medical characteristics of the study sample.
Demographic and medical characteristics of the study sample (n = 125).
| Parameter | Median (IQR) | n (%) |
|---|---|---|
| Age (years) | 73.0 (24) | |
| Gender | ||
| Female | 44 (35.2) | |
| Male | 81 (64.8) | |
| Length of stay | 13.0 (11) | |
| In-hospital mortality | ||
| Survival | 93 (74.4) | |
| Died | 32 (25.6) | |
| ICU admission | ||
| Yes | 20 (16.0) | |
| No | 100 (80.0) | |
| Already admitted to ICU | 5 (4.0) | |
IQR: interquartile range.
All patients in the study received therapy utilizing fluoroquinolones, with the great majority receiving levofloxacin (n = 124; 99.2%). A small number of patients received fluoroquinolone monotherapy (n = 12; 9.6%), but most patients received combinations of antibiotics along with fluoroquinolone therapy. A total of 42 patients (33.6%) received two antibiotics, 49 patients (39.2%) received three antibiotics, and 22 patients (17.6%) received four antibiotics. Vancomycin was prescribed most frequently (n = 72; 57.6%) among adjunct antibiotics. The median number of prescribed empiric antibiotics was 3 (IQR = 1.0), with a total of 331 empiric antimicrobial agents prescribed, including fluoroquinolones.
The microbial culture results indicated that 96 of the patients (76.8%) were negative for culture, and 29 of the patients (23.2%) were positive for culture (Table 2). The majority of the positive samples (28/29, 96.6%) underwent susceptibility testing, while one positive sample (3.4%) did not undergo susceptibility testing. The majority of specimens contained pathogens that were resistant to fluoroquinolones (23/28, 82.1%), and the minority of samples were sensitive to fluoroquinolones (3/28, 10.7%). Interestingly, two samples (7.1%) did not undergo susceptibility testing for fluoroquinolones but did undergo antibiotic susceptibility testing (Table 2).
Isolated bacterial pathogens, fluoroquinolone resistance profiles, and antibiotic de-escalation outcomes among patients with suspected CAP and positive cultures (n = 29).
| Patient No. | Specimen type | Bacteria name | Resistance pattern to fluoroquinolones | De-escalation outcome |
|---|---|---|---|---|
| 1 | Blood specimen | Viridans group streptococci | Resistant to levofloxacin | Successfully de-escalated |
| 2 | Sputum specimen | Streptococcus pyogenes (Group A) | Resistant to levofloxacin | Successfully de-escalated |
| 3 | Blood specimen | Staphylococcus species Coagulase | Resistant to levofloxacin | Successfully de-escalated |
| 4 | Blood specimen | Staphylococcus species Coagulase | Resistant to levofloxacin | Successfully de-escalated |
| 5 | Blood specimen | Staphylococcus species Coagulase | NA | Incorrectly de-escalated |
| 6 | Blood specimen | Staphylococcus species Coagulase | Resistant to levofloxacin | Failed de-escalation |
| 7 | Blood specimen | Staphylococcus hominis | Resistant to levofloxacin | Successfully de-escalated |
| 8 | Blood specimen | Staphylococcus hominis | Resistant to levofloxacin | Failed de-escalation |
| 9 | Blood specimen | Staphylococcus hominis | NA | Successfully de-escalated |
| 10 | Blood specimen | Staphylococcus hominis | Resistant to levofloxacin | Failed de-escalation |
| 11 | Blood specimen | Staphylococcus hominis | Resistant to levofloxacin | Failed de-escalation |
| 12 | Blood specimen | Staphylococcus hominis | Resistant to levofloxacin | Failed de-escalation |
| 13 | Blood specimen | Staphylococcus haemolyticus | Resistant to levofloxacin | Successfully de-escalated |
| 14 | Blood specimen | Staphylococcus haemolyticus | Sensitive to levofloxacin | Successfully de-escalated |
| 15 | Blood specimen | Staphylococcus epidermidis | NA | Incorrectly de-escalated |
| 16 | Blood specimen | Staphylococcus epidermidis | Sensitive to levofloxacin | Failed de-escalation |
| 17 | Blood specimen | Staphylococcus epidermidis | Sensitive to levofloxacin | Failed de-escalation |
| 18 | Blood specimen | Staphylococcus aureus | Resistant to levofloxacin | Incorrectly de-escalated |
| 19 | Sputum specimen | Klebsiella pneumoniae | Resistant to levofloxacin | Successfully de-escalated |
| 20 | Blood specimen | Klebsiella pneumoniae | Resistant to levofloxacin | Successfully de-escalated |
| 21 | Blood specimen | Klebsiella pneumoniae | Resistant to levofloxacin | Successfully de-escalated |
| 22 | Blood specimen | Klebsiella pneumoniae | Resistant to levofloxacin | Successfully de-escalated |
| 23 | Blood specimen | Klebsiella pneumoniae and Staphylococcus aureus | Resistant to levofloxacin | Failed de-escalation |
| 24 | Blood specimen | Escherichia coli | Resistant to levofloxacin | Successfully de-escalated |
| 25 | Sputum specimen | Escherichia coli | Resistant to ciprofloxacin | Successfully de-escalated |
| 26 | Blood specimen | Diphtheroids bacilli | Resistant to levofloxacin | Successfully de-escalated |
| 27 | Blood specimen | Diphtheroids bacilli | Resistant to levofloxacin | Failed de-escalation |
| 28 | Sputum specimen | Acinetobacter baumannii | Resistant to ciprofloxacin | Successfully de-escalated |
| 29 | Blood specimen | Acinetobacter baumannii | Resistant to levofloxacin | Failed de-escalation |
CAP: community-acquired pneumonia.
The positive culture specimens predominantly showed 1 microorganism (28/29, 96.6%); there was 1 specimen (3.4%) that had two pathogens, which had a total of 30 isolated pathogens. The most commonly reported pathogens were Staphylococcus hominis (6/30, 20.0%), Klebsiella pneumoniae (5/30, 16.7%), and Staphylococcus epidermidis (3/30, 10.0%) (see Table 2).
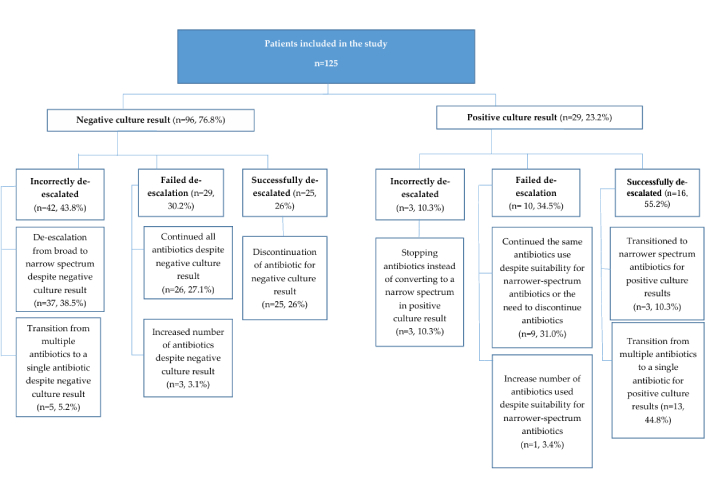
Of the patients suspected to have CAP, 76.8% had a negative blood culture. All patients were then classified into one of three groups depending on the appropriateness of fluoroquinolone de-escalation. There were those who incorrectly de-escalated (42/96, 43.8%), those who had a failed de-escalation (29/96, 30.2%), and those who successfully de-escalated (25/96, 26.0%).
On the contrary, in the sample, 29 patients (23.2%) had a positive culture finding for otherwise suspected CAP (25 positive blood cultures and four positive sputum cultures). All patients required de-escalation. The 29 patients were then stratified into three categories. There were those who incorrectly de-escalated (n = 3, 10.3%), those who failed de-escalation (n = 10, 34.5%), and those who successfully de-escalated (n = 16, 55.2%). These results appear in Figure 1. Likewise, Table 3 includes examples demonstrating the decision process surrounding de-escalation for patients with both positive and negative cultures.
Examples illustrating decisions related to the de-escalation process for patients with positive and negative cultures.
| Decision | Example |
|---|---|
| Incorrectly de-escalated (de-escalation from broad to narrow spectrum despite negative culture result) | An 88-year-old female was admitted to JUH. The patient received intravenous levofloxacin before the results of the blood culture were available. Within 48 h of admission, the culture results showed no bacterial growth. Subsequently, the patient’s treatment was de-escalated to ceftriaxone sodium injection 1 g on the following day, coinciding with the availability of the culture results. |
| Incorrectly de-escalated (transition from multiple antibiotics to a single antibiotic despite a negative culture result) | An 81-year-old male was admitted to JUH. The patient received intravenous levofloxacin and piperacillin/tazobactam injections before the results of the blood culture were available. After more than 72 h of admission, the culture result showed no bacterial growth. Levofloxacin was discontinued, and the patient continued with piperacillin/tazobactam on the same day that the culture results became available. |
| Failed de-escalation (continued all antibiotics despite negative culture results) | A 100-year-old male was admitted to JUH. The patient received intravenous levofloxacin, intravenous vancomycin, and intravenous imipenem before the culture results were available. After more than 72 h of admission, both blood and sputum cultures showed no bacterial growth. The patient’s treatment was maintained with intravenous levofloxacin, intravenous vancomycin, and intravenous imipenem after the culture results became available. |
| Failed de-escalation (increased number of antibiotics despite negative culture result) | A 63-year-old female was admitted to JUH. The patient received intravenous levofloxacin before the results of the blood culture were available. Within 72 h of admission, the blood culture showed no bacterial growth. The patient’s treatment regimen was adjusted, and she began receiving intravenous piperacillin/tazobactam injection in addition to levofloxacin on the same day as the culture results became available. |
| Successfully de-escalated (discontinuation of antibiotic for negative culture result) | A 71-year-old male was admitted to JUH. The patient received intravenous levofloxacin, intravenous piperacillin/tazobactam, and oral amoxicillin/clavulanic acid tablets before the results of the blood culture were available. After more than 72 h of admission, the blood culture showed no bacterial growth. Consequently, the patient’s treatment was de-escalated, and all antibiotics were discontinued on the same day as the culture results became available. |
| Failed de-escalation (continued all antibiotics despite colonization, which suggests negative culture results) | A 60-year-old male was admitted to JUH with suspected community-acquired pneumonia and was started empirically on intravenous levofloxacin and piperacillin/tazobactam. Within 48 h, culture results showed Staphylococcus hominis isolated from a non-sterile respiratory sample. Despite this result, which likely represented colonization rather than true infection, the broad-spectrum antibiotics were continued rather than de-escalated or discontinued. |
| Failed de-escalation (increased the number of antibiotics used despite suitability for narrower-spectrum antibiotics) | A 76-year-old female was admitted to JUH. The patient received intravenous levofloxacin, vancomycin, and meropenem before the availability of culture results. More than 72 h after admission, a culture result was received, revealing the presence of Acinetobacter baumannii. Despite suitability of narrower antibiotics, gentamycin was initiated in addition to the ongoing antibiotics levofloxacin, vancomycin, and meropenem. |
| Incorrectly de-escalated (stopping antibiotics instead of converting to a narrow spectrum in culture result) | A 55-year-old female was admitted to JUH. The patient received intravenous levofloxacin in addition to imipenem/cilastatin before the results of the culture were available. After more than 72 h of admission, the culture result showed the presence of Staphylococcus aureus. Subsequently, the patient’s treatment was discontinued, and all antibiotics were stopped, leaving the patient untreated. |
| Successfully de-escalated (transitioned to narrower spectrum antibiotics for positive culture results) | An 88-year-old male was admitted to JUH. The patient received intravenous levofloxacin and imipenem/cilastatin before the culture results were available. After more than 72 h of admission, the culture results showed the presence of Escherichia coli. Subsequently, the patient’s treatment was transitioned from the broad-spectrum levofloxacin to the narrower-spectrum vancomycin in addition to imipenem/cilastatin. |
| Successfully de-escalated (transition from multiple antibiotics to a single antibiotic for positive culture results) | A 65-year-old female was admitted to JUH. The patient received intravenous levofloxacin, meropenem, gentamycin, and ceftazidime/avibactam. Within 72 h of admission, the culture result showed the presence of Klebsiella pneumoniae. Levofloxacin was discontinued, and the patient’s treatment was continued with intravenous meropenem, gentamycin, and ceftazidime/avibactam without levofloxacin. |
JUH: Jordan University Hospital.
Before assessing the study’s secondary objectives, we duly attempted to ensure that cases were included that were relevant to our goals. Consequently, we excluded cases in which de-escalation occurred incorrectly, with particular reference to cases where antibiotics were stopped instead of switching to a narrower spectrum after a positive culture result (3 patients). After excluding these 3 patients, the reduced sample size was 122 patients. Of the 122 patients, 41 were successfully de-escalated and 81 either improperly de-escalated or did not de-escalate.
The study noted that patients who were successfully de-escalated had a median LOS of 12 days (IQR = 8 days) compared to patients who lacked successful de-escalation or proper de-escalation [median LOS 18 days (IQR = 11 days)], with a statistically significant p-value of 0.004 via Mann-Whitney U test.
Regarding mortality at discharge, there was no difference between the two study groups. Among the patients who had successful de-escalation, 29 of 41 (70.7%) survived, whereas of those who had either failed de-escalation or were inappropriately de-escalated, 62 of 81 (76.5%) survived. Fisher’s exact test yielded no significant difference in in-hospital mortality between the two groups for this variable (p = 0.514).
Age, gender, and ICU admission status were not significantly different between the two groups (p ≥ 0.05 for all). Further details can be found in Table 4.
Comparison of patient demographics and clinical outcomes between successful and failed/inappropriate antibiotic de-escalation groups.
| Parameter | Successfully de-escalated (n = 41) | Failed/Inappropriate de-escalated (n = 81) | P-value |
|---|---|---|---|
| Age (years), median (IQR) | 74.0 (20.0) | 71.0 (25.0) | 0.659^ |
| Gender, n (%) | |||
| Female | 15 (36.6%) | 27 (33.3%) | 0.721# |
| Male | 26 (63.4%) | 54 (66.7%) | |
| ICU admission, n (%) | |||
| Yes | 8 (19.5%) | 12 (14.8%) | 0.324# |
| No | 33 (80.5%) | 64 (79.0%) | |
| Already admitted to ICU | 0 (0%) | 5 (6.2%) | |
| Length of hospital stay (days), median (IQR) | 12 (8.0) | 18 (11.0) | 0.004*^ |
| In-hospital mortality, n (%) | |||
| Survived | 29 (70.7%) | 62 (76.5%) | 0.514# |
| Died | 12 (29.3%) | 19 (23.5%) | |
*: Significant at 0.05 significance level; ^: using Mann-Whitney U test; #: using Chi-square/Fisher exact test. IQR: interquartile range.
Among patients with a positive culture, 16 of 26 patients (61.5%) had successful de-escalation. Of those patients with negative cultures, 26.0% (n = 25) had successful de-escalation. Chi-square analysis demonstrated a significantly greater rate of de-escalation success with positive cultures compared to negative cultures (p = 0.002). The details are displayed in Table 5.
Assessing the association between cultural results and de-escalation practice.
| Microbial culture result | Positive culture result (n = 26) | Negative culture result (n = 96) | P-value |
|---|---|---|---|
| Successfully de-escalated | 16 (61.5%) | 25 (26.0%) | 0.002*# |
| Failed/Inappropriate de-escalated | 10 (38.5%) | 71 (74.0%) |
*: Significant at 0.05 significance level; #: using Chi-square test.
This study assessed the rate and effectiveness of fluoroquinolone de-escalation in 125 adult patients diagnosed with CAP at a tertiary teaching hospital in Jordan. Levofloxacin, a broad-spectrum respiratory fluoroquinolone, was the most commonly used antibiotic (99.2%) in our cohort. It is often used because it is effective against typical pathogens like Streptococcus pneumoniae, and atypical pathogens such as Mycoplasma pneumoniae and Chlamydophila pneumonia. Nevertheless, the research revealed concerning, high rates of toxin-associated resistance to levofloxacin at 82.2% across the many strains of bacteria. The rate is concerning and emphasizes the shared importance of appropriate use and antimicrobial stewardship, especially when selecting for empiric therapy patients. Microbial surveillance is a reasonable approach where frequent evaluations of resistance patterns inform empiric treatment guidelines and reduce the use of broad-spectrum antibiotics when they are not applicable [17, 18].
We discovered a success rate of fluoroquinolone de-escalation at 32.8%, which aligns with data from previous studies. For instance, Deshpande et al. [19] reported de-escalation rates of 2–35% in a 14,170 patient multicenter study. Joung et al. [20] found a de-escalation rate of 32.1%. We found a significant difference in de-escalation success rates with negative cultures (26%) and positive cultures (61%) (p = 0.002). We suspect this difference is due to positive cultures identifying the pathogen, allowing the clinicians to de-escalate from broad-spectrum to narrower-spectrum antibiotics. For negative cultures, it is likely that clinicians are unsure of the causative pathogen, so they continue to use broad-spectrum antibiotics, consequently decreasing the chances of de-escalation.
An important finding of this study was that three patients with positive cultures stopped all antibiotics rather than de-escalating to narrower spectrum alternatives. This is an alarmingly concerning practice as it may lead to inadequate treatment, longer LOS in the hospital, treatment failure, and increase the risk of complications, including the emergence of antibiotic resistance. These findings demonstrate the significance of de-escalating protocols to ensure appropriate antibiotic treatment is maintained during treatment.
The study also found a significant difference in hospital LOS between the successfully de-escalated group (median 12 days) and the failed or inappropriate de-escalated group (median 18 days), highlighting the potential benefits of de-escalation in reducing hospital stays and improving hospital resource utilization [21]. This is consistent with other studies, such as Giantsou et al. [22], which showed a reduction in LOS among patients who underwent successful de-escalation. However, our results contrast with those of Knaak et al. [23], who reported no significant difference in LOS between de-escalated and non-de-escalated patients. These discrepancies suggest that factors like disease severity, comorbidities, and hospital protocols may influence outcomes, emphasizing the need for individualized treatment plans and tailored antibiotic management strategies.
While our study found no significant difference in mortality rates between the successful and failed de-escalation groups, López-Cortés et al. [24] also reported no significant difference in mortality. They showed no significant differences in mortality between those with and without de-escalation [24]. In contrast, Joung et al. [20] observed lower mortality rates in the de-escalated group, suggesting that de-escalation may be more beneficial for certain patient populations. One potential reason for the lack of difference in mortality is that mortality is driven by multiple factors, including baseline disease severity, baseline comorbidities, and overall clinical status—all of which are not fully captured in this retrospective study. Consequently, mortality alone may not be sensitive enough to detect the de-escalation’s benefits. Other outcomes that measure clinical value might include total LOS, and the right use of antibiotics is a more valuable indicator. In summary, the findings of this study should provide reassurance to clinicians that appropriate de-escalation, including in cases of uncertainty or when a culture is negative, does not adversely affect patient safety.
While these findings are important, the retrospective nature of the study, single-center delivery, and small sample size are important limitations of the study in the context of generalizability. The aforementioned may introduce bias due to incomplete or inaccurate medical records. The study also could not control for every possible confounding factor, such as disease severity or common comorbidities that may have affected the results. Lack of data precluded adjustment for potential confounders that may have had a bearing on clinical outcomes (e.g., length of hospital stay). Also, this study has a limitation in that no information on biomarkers such as neutrophil-to-lymphocyte ratio and C-reactive protein was obtained, as they may contain some important information about the inflammatory response and could prove helpful in predicting patient outcomes during an antibiotic de-escalation.
In addition, CAP cases were identified based on ICD-10 diagnostic codes rather than standardized clinical or radiologic criteria. This could have led to the inadvertent inclusion of patients with non-bacterial etiologies such as viral pneumonia. When patients have negative cultures, it is invariably difficult to know if they truly had a viral infection or a bacterial infection that could not be microbiologically confirmed because diagnostic sensitivity for determining the presence and extent of infection sometimes limits diagnostic accuracy. That ambiguity could have directly influenced any of the assessments of de-escalation appropriateness and potentially created a level of uncertainty for clinical decision-making.
In conclusion, we found that fluoroquinolone de-escalation in patients with CAP was associated with a shorter LOS without any evidence of increased mortality. We want to clarify that our definitions of de-escalation appropriateness were primarily formed from cultural results (due to the nature of our retrospective analysis and limitations in clinical documentation), so our findings should be interpreted accordingly. Future prospective studies with standardized diagnostic criteria and clinically contextually defined appropriate de-escalation criteria are needed to validate these associations and in order to develop the field of stewardship practice based on the highest quality of evidence.
CAP: community-acquired pneumonia
IDSA: Infectious Diseases Society of America
IQR: interquartile range
JUH: Jordan University Hospital
LOS: length of stay
AAA: Conceptualization, Methodology, Writing—original draft, Writing—review & editing, Data curation. KAH: Conceptualization, Methodology, Writing—original draft, Writing—review & editing, Data curation. AA: Conceptualization, Methodology, Writing—original draft, Writing—review & editing. MZ: Conceptualization, Methodology, Writing—original draft, Writing—review & editing. RKAF: Conceptualization, Methodology, Writing—original draft, Writing—review & editing, Data curation. All authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
The study was conducted in accordance with the principles outlined in the World Medical Association Declaration of Helsinki. It received approval from the JUH Institutional Review Board (approval number 10/2024/1389).
To ensure patient confidentiality, all data were de-identified and anonymized. Given the retrospective, observational design, the ethical committee granted a waiver for informed consent.
Not applicable.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This study did not receive any funding support.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 2390
Download: 42
Times Cited: 0