Original Article
Original Article

Affiliation:
1Department of Microbiology, College of Medicine, University of Karbala, Karbala 00964, Iraq
Email: aljanabibio@gmail.com
ORCID: https://orcid.org/0000-0002-2479-3282
Affiliation:
1Department of Microbiology, College of Medicine, University of Karbala, Karbala 00964, Iraq
Affiliation:
2Department of Surgery, College of Medicine, University of Karbala, Karbala 00964, Iraq
Explor Med. 2023;4:878–885 DOI: https://doi.org/10.37349/emed.2023.00183
Received: July 14, 2023 Accepted: October 19, 2023 Published: December 06, 2023
Academic Editor: Elizabeth Ann L. Enninga, Mayo Clinic College of Medicine and Science, USA
The article belongs to the special issue Breast Cancer: Basic and Clinical Advances
Aim: Estrogen has an important role in the colonization of Candida through the presence of estrogen receptors (ERs). These ERs are usually used to categorize breast cancer into two types, positive and negative ER breast cancers. The effect of variation in the type of ER and estrogen levels on the biodiversity of Candida in the vagina was investigated.
Methods: A case-control study, consisting of three groups of 30 patients with ER-positive, 29 with ER-negative breast cancer, and 30 healthy individuals, was carried out. The diversity and counting of Candida spp. in the vagina and estrogen levels were identified in all subjects.
Results: The growth of Candida spp. was high in the vagina of patients with ER-positive breast cancer when estrogen was at normal levels. Otherwise, its growth was enhanced by high levels of estrogen in patients with ER-negative breast cancer.
Conclusions: Estrogen levels have no effect on the vaginal content of Candida spp. in patients with ER-positive breast cancer, unlike those with ER-negative breast cancer. The principal recommendation from this study is that vaginal candidiasis and estrogen levels should be checked in patients with ER-negative breast cancer.
Estrogen is a sex hormone typically found in many structural forms that usually have high levels in women and low levels in men [1]. Its activities in human tissues are primarily carried out by the estrogen receptor (ER) [2]. Breast cancer is associated with an increase in estrogen levels, especially in postmenopausal women [2, 3]. From 1970 onwards, breast cancer was divided into two groups based on that ER is present or absent; ER-positive and ER-negative [4]. Positive ER type is more frequently associated with breast cancer than negative ER type [4].
Candida spp. are very common fungi that normally inhabit various parts of the human body [5]. In the vagina, different species of Candida are regarded as resident members of the microbial flora [6, 7]. The most widespread species of Candida in the vagina is Candida albicans (C. albicans), which makes up 70% of all Candida isolates [7]. Candida colonization in the vagina can be influenced by several conditions that can cause an increase or decrease in its number or diversity with a chance to become the pathogenic agent of vaginal candidiasis [6].
Estrogens, along with other steroidal hormones, have been proven to have direct multifunctional effects on a variety of pathogenic microorganisms by controlling microbial replication, colonization, biofilm formation and adherence to host surfaces [8]. Its concentration in the circulation system may affect vaginal Candida spp. through its activity on the state of vaginal immunity [9] or directly on Candida spp. [10]. Experiments in mice revealed that the inhibitory effect of vaginal epithelial cells on the growth of C. albicans was reduced in the presence of estrogen and any decrease in estrogen levels will induce C. albicans to cause vaginal infection [9].
The aim of this study is to fill the gap in knowledge about the influence of estrogen on vaginal Candida and its association with the type of ER. The growth of Candida spp. is known to be promoted by the activation of ERs in vaginal tissues [11–13]. Thus, masking or eliminating these receptors may prevent vaginal infection with Candida species [10]. The increase in ER expression in patients with ER-negative breast cancer could lead to an increase in Candida spp. growth in the vagina [14]. In a previous study, it was found that the type of ER and levels of estrogen were normal in patients with positive-ER, while they were higher in those with negative-ER [15]. From that, the effect of ER type relative to estrogen levels on the number and variety of vaginal Candida spp. of patients with breast cancer was investigated.
Three groups of premenopausal women attending AL-Ammam AL-Hussein Medical City in Karbala province from November 2019 to March 2020 participated in the case-control study. The first group consisted of 30 women (30–59 years) with ER-positive breast cancer. The second group included 29 women with ER-negative breast cancer (30–49 years old). The third group comprised 30 healthy women (20–49 years old) to be considered as a control group without breast cancer. Ethical approval was obtained from the ethical committee of University of Karbala. Breast cancer was clinically diagnosed by oncologists within the oncology unit and confirmed by hospital histopathologists. Women excluded from the study included menopausal and pregnant women, and those on chemotherapy, hormonal contraceptives, or antifungal and/or antibiotic therapy.
Vaginal and blood samples were collected from all subjects. Candida spp. were isolated by collecting vaginal swabs and cultured on Sabouraud dextrose agar (HiMedia, India). Cultures were incubated at 30°C for 48 h. Growing colonies were counted as colony forming units (cfu/mL). The primary diagnosis of Candida spp. was dependent on the morphological features of the yeast under microscopic examination, and then the species was diagnosed by VITEK® 2 instrument with VITEK® 2 Yeast Identification Cards (bioMérieux, France).
Estradiol (E2) concentration was measured in serum for all subjects using fully automated Cobas E411 analyzer of E2 biochemical kit (DIPO, U.S.A.). The normal range of E2 was 12.5–166 ng/mL. Type of ER was determined by ER immunohistochemical assay (Dako Denmark A/S, Denmark).
The study was conducted in accordance with the Helsinki Declaration and was approved by the local ethics committee of the University of Karbala No. 112 in July 2019. Written informed consent was obtained from all subjects in advance of their admission to the study.
Data of all tests were expressed as mean ± standard deviation (SD). The values were statistically analyzed with one-way Analysis of variance (ANOVA) using Microsoft Excel for Windows version 10. The minimum level of P < 0.05 was considered significant.
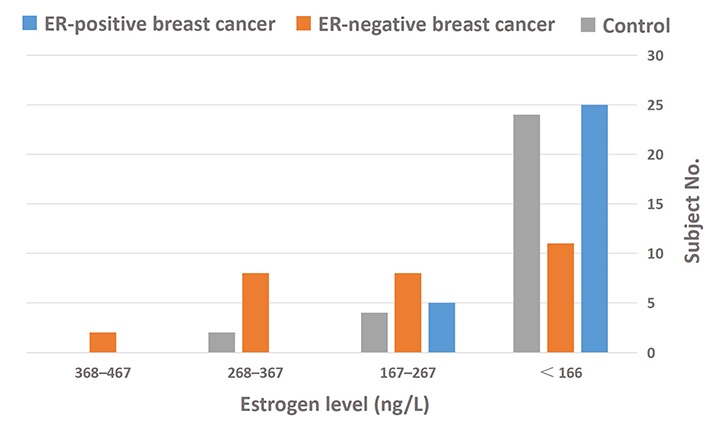
The age mean of enrolled subjects was 39.5 years. Blood samples from all groups were analyzed for estrogen levels. It was at normal levels in 69.7% of subjects and high in 30.3%. Most patients with ER-positive breast cancer as well as those in the control group had significantly normal estrogen levels (29.2% and 32.3%, respectively). In contrast, estrogen levels were elevated in a number of ER-negative patients (20.2%) (Table 1). Estrogen concentrations of 167–267 ng/mL were common in all subjects and were significantly higher in many patients with negative ER breast cancer (Figure 1).
Patient’s characteristics
| Character | Estrogen levels | Subject no. | |
|---|---|---|---|
| Normal | High | ||
| Age mean (years) | 39.5 | ||
| ER-positive breast cancer | 26*’ ** (29.2%) | 4 (4.5%) | 30 |
| ER-negative breast cancer | 11 (9.23%) | 18*’ ** (20.2%) | 29 |
| Control | 25*’ ** (32.30%) | 5 (5.6%) | 30 |
| Total no. | 62 (69.7%) | 27 (30.3%) | 89 |
* A significant difference between subject groups with the same estrogen level at P < 0.05; ** A significant difference between estrogen levels within the same subject group at P < 0.05
Candida spp. was found to be high in all subject groups who had normal estrogen levels. A count of 201–360 cfu/mL was observed significantly in patients with positive ER breast cancer who had normal estrogen levels. Also, the association between the high growth of Candida spp. and the high level of estrogen was clearly demonstrated in patients with ER-negative breast cancer (Table 2).
Correlation between colony count of Candida spp. and estrogen level
| Subject group | Estrogen level | Subject no. (%) | Total no. (%) | ||||
|---|---|---|---|---|---|---|---|
| Colony count (cfu/mL) | |||||||
| 1–100 | 101–200 | 201–360 | > 360 | No growth | |||
| ER-positive breast cancer | Normal | 3* (3.3) | 1* (1.2) | 12* (13.5) | 2* (2.2) | 8 (9) | 26 (29.2) |
| High | 0 | 0 | 2 (2.2) | 0 | 2 (2.2) | 4 (4.5) | |
| ER-negative breast cancer | Normal | 0 | 0 | 9 (10.1) | 0 | 2 (2.2) | 11 (9.23) |
| High | 0 | 9 (10.1) | 7 (7.8) | 0 | 2 (2.2) | 18 (20.2) | |
| Control | Normal | 0 | 0 | 10 (11.2) | 0 | 15 (16.9) | 25 (32.30) |
| High | 0 | 0 | 2 (2.2) | 0 | 3 (3.3) | 5 (5.6) | |
| Total no. (%) | 3 (3.3) | 10 (11.2) | 42 (47.1) | 2 (2.2) | 32 (36) | 89 | |
* A significant difference between colony counts within the same estrogen level of one subject group at P < 0.05
The lack of growth of Candida spp. was most frequently found in healthy individuals and in patients with ER-positive breast cancer who had normal estrogen levels (16.9% and 9%, respectively). Meanwhile, the absence of Candida spp. in subjects with high estrogen levels was observed mainly in healthy individuals (3.3%) and in 2.2% of patients with either ER-positive or negative breast cancer (Table 2).
Four species of Candida were diagnosed, including C. albicans, C. glabrata, C. kefyr, and C. famata. C. albicans was the most common species in all study groups (91.2%), followed by C. kefyr (5.2%). The presence of C. albicans was observed in a large number of ER-positive breast cancer patients and in healthy individuals with normal levels of estrogen (26.3% and 17.5%, respectively). Meanwhile, patients with ER-negative breast cancer with elevated levels of estrogen had higher content of C. albicans (24.5%) than the other two groups studied. Species other than C. albicans were observed individually in a patient with positive ER breast cancer who had normal levels of estrogens, while C. kefyr was diagnosed in a patient with ER-negative breast cancer with high estrogen levels (3.5%) (Table 3).
Correlation of isolated species of Candida with estrogen level
| Subject group | Estrogen level | Subject no. (%) | Total no. (%) | |||
|---|---|---|---|---|---|---|
| Candida species | ||||||
| C. albicans | C. glabrata | C. kefyr | C. famata | |||
| ER-positive breast cancer | Normal | 15 (26.3) | 1 (1.8) | 1 (1.8) | 1 (1.8) | 18 (31.5) |
| High | 2 (3.5) | 0 | 0 | 0 | 2 (3.5) | |
| ER-negative breast cancer | Normal | 9 (15.7) | 0 | 0 | 0 | 9 (15.7) |
| High | 14* (24.5) | 0 | 2 (3.5) | 0 | 16 (28.0) | |
| Control | Normal | 10 (17.5) | 0 | 0 | 0 | 10 (17.5) |
| High | 2* (2.5) | 0 | 0 | 0 | 2 (2.5) | |
| Total no. (%) | 52 (91.2) | 1 (1.8) | 3 (5.2) | 1 (2.5) | 57 | |
* A significant difference between colony counts with the same species of Candida at P < 0.05
Findings from this study indicated that most breast cancer patients had normal levels of estrogen. These results were in contrast to many other studies. Breast cancer is associated with a high level of estrogen, and any increase in estrogen levels can increase the risk of developing cancer, as demonstrated by numerous studies [2, 3]. The validity of this relationship in postmenopausal women has been validated by many other meta-analysis retrospective studies [16]. The rate of breast cancer can be increased by 6.8 folds when E2 is elevated to 2.7 ng/mL in women [17]. Both premenopausal and postmenopausal women are likely to develop breast cancer if they have high levels of estrogen [18].
Estrogen levels were found high in some patients of this study who had negative ER breast cancer. Many studies were conducted in postmenopausal women, while patients in this study were in premenopausal state. Androstenedione as a form of estrogen was found in a low association with breast cancer in premenopausal women when it was low [19]. The risk of elevated levels of estrogens in the development of breast cancer has been demonstrated in women with positive ER-type breast cancer compared to that with negative ER-type [4]. In some cases, an ER-negative patient may also be considered at high risk for breast cancer [20].
Vagina could be considered an environment suitable for various kinds of organisms, including bacteria, fungi and parasites. Yeasts, as one form of fungi, represented by Candida species are one of the most common resident organisms in the vagina, which are highly susceptible to transformation into a pathogen under specific conditions [21]. The vaginal content of fungi requires further study as little is known about the living conditions of this organism in the vagina compared to the bacterial community [7]. C. albicans is considered the most common species of Candida that is capable of living as a mycobiont in the vagina [7, 22, 23].
According to the results of this study, C. albicans was the most often isolated species, from a large number of breast cancer patients, particularly those with a positive ER type. Several studies have shown that C. albicans is the most commonly occurring species in the vagina of healthy women and patients with various diseases [22]. It typically accounts for 70% of all Candida spp. within the vagina [7]. C. albicans was also observed in 91% of asymptomatic adolescents [24] with a frequency of 44.2% of all Candida spp. isolated from a variety of clinical specimens [22]. However, the vaginal content of Candida spp. showed variable strains of C. albicans with differing virulence for causing the disease [23].
Candida spp. may be associated with different types of cancer developing in the human body [25]. This association was evidently noticed after Candidal infection was found in progress with a significantly increased risk of cancer as with hematological malignant cancer, skin, pancreas and neck and head cancer [26]. The assessment of the presence of Candida spp. in cancer patients in Jordan showed that it was diagnosed in 72.6% of them, particularly C. albicans, while it was found in 33.8% of healthy people [27]. However, the ability of C. albicans to adhere to human cervical cancer cells (SiHa) makes this yeast more pathogenic than other species [28]. Although thoughts have focused on the fact that the growth of Candida spp. in cancer patients results mainly from immunosuppressive drug therapy, there is new evidence that C. albicans has the ability to promote cancer development by many mechanisms such as the synthesis of carcinogenic by-products, induction of Th17 response, and initiation of inflammation [25].
The vagina tends to be affected by the level of blood-circulating estrogen and any change in this level can easily be observed in the vaginal structure, particularly during the menstrual cycle [11]. The effects of estrogens on the vagina are mediated by the presence of ER in vaginal tissues [11–13]. In postmenopausal women, decreased estrogen levels cause vaginal atrophy characterized by increased dryness, low pH and tissue thinning [11]. Thus, the presence of C. albicans in the vagina may be affected by estrogen levels and may advance to fungal infection [29]. Stimulating the growth of Candida spp. could be multiplied by 8.6 in the vagina because of the effect of E2 [30]. C. albicans was found to survive and to be vital in the rat vagina for up to 10 days following treatment with E2 cypionate, compared to the untreated group [10]. However, vaginal or vulvovaginal atrophy (VVA) is the most common type of candidiasis that may develop under the effects of low estrogen levels [11, 13].
Based on the findings of this study, Candida spp. were more frequently isolated in subjects with normal estrogen levels, while high C. albicans content was observed in patients with negative ER breast cancer who have high estrogen levels. The ER can be found in variable vaginal layers and its concentration is unaffected by estrogen level, but it was affected by the ER site and menstrual period [12]. In patients with ER-negative breast cancer, the elevated vaginal content of C. albicans may be related to the expression of ER in premenopausal women, which is higher than in postmenopausal women [14]. Greater numbers of C. albicans, associated with high level of estrogen in the vagina of breast cancer patients, may be related to the increasing role of estrogen on the glycogen content of the vagina [11, 13]. Elevated levels of glycogen under the effect of estrogen encourage vaginal bacteria to develop an acidic environment, which will increase the growth of Candida spp. [11].
The strength of this study is that it was prospectively observed that the vagina of ER-negative breast cancer patients experienced an increase in the colonization of Candida species due to high levels of estrogen. In contrast, vaginal Candida in patients with ER-positive breast cancer is not affected by estrogen levels. Thus, variation in estrogen levels may be influenced by breast cancer type based on ER, which ultimately affects vaginal fungal colonization. Also, patients with ER-negative breast cancer have a higher chance of developing vaginal candidiasis.
The main limitation of this study is that the number of patients participating in this study is low, which may be related to the difficulty in following up all the requirements of such a study in a large number of patients. Only patients from a small city in Iraq (Karbala) were involved, and the geographical area should be expanded in the future. Another limitation is that it is challenging to select breast cancer patients who have not been treated with any steroid or estrogen medication or those with a balanced Candida flora in their vagina without vaginal candidiasis.
In conclusion, Candida spp., particularly C. albicans are more frequently found in the vagina of patients with positive ER breast cancer who have a normal estrogen level. High estrogen levels play an effective promotion role in the growth of Candida spp. in the vagina of women with ER-negative breast cancer. Finally, this study recommends that physicians should check for vaginal candidiasis and estrogen levels in ER-negative breast cancer patients, while for ER-positive breast cancer patients check should focus solely on vaginal candidiasis.
C. albicans: Candida albicans
E2: estradiol
ER: estrogen receptor
AAHSAJ: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. RKMJ: Investigation. ARKH: Validation, Supervision. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Ethical approval was obtained from the ethical committee of University of Karbala (No. 112).
Written informed consent was obtained from all subjects in advance of their admission to the study.
Not applicable.
All data is contained within the manuscript.
Not applicable.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 6105
Download: 29
Times Cited: 0
Danila Coradini, Federico Ambrogi
Banashree Bondhopadhyay ... Vishakha Kasherwal
Nadia Islam, Suneela Vegunta
Spoorthi Marada ... Yi Lu
Danila Coradini
Remo Poto ... Gilda Varricchi
Kaoutar Anouar Tadlaoui ... Moulay Mustapha Ennaji