Original Article
Original Article

Affiliation:
1Diabetes and Allergy Asthma Therapeutics Specialty Clinic, Allergy and Asthma Treatment Centre, Kolkata 700014, West Bengal, India
2Department of Pharmacology, JMN Medical College, Ranaghat 741201, West Bengal, India
Email: shambo_sa2001@yahoo.co.in
ORCID: https://orcid.org/0000-0002-9199-0905
Affiliation:
3Department of Dermatology, KPC Medical College and Hospital, Kolkata 700032, West Bengal, India
ORCID: https://orcid.org/0000-0003-0841-9597
Affiliation:
4Department of Pulmonary Medicine, Apollo Hospitals, Kolkata 700054, West Bengal, India
ORCID: https://orcid.org/0000-0003-3355-8580
Affiliation:
5Department of Clinical and Experimental Pharmacology, School of Tropical Medicine, Kolkata 700073, West Bengal, India
ORCID: https://orcid.org/0000-0001-9524-1525
Affiliation:
6Department of Medicine, IPGMER & SSKM Hospital, Kolkata 700020, West Bengal, India
ORCID: https://orcid.org/0000-0002-7729-812X
Affiliation:
7Joshi Clinic, Mumbai 400022, Maharashtra, India
ORCID: https://orcid.org/0000-0002-0990-5821
Explor Immunol. 2025;5:1003217 DOI: https://doi.org/10.37349/ei.2025.1003217
Received: December 11, 2024 Accepted: August 12, 2025 Published: September 21, 2025
Academic Editor: Manuela Neuman, University of Toronto, Canada
The article belongs to the special issue Hypersensitivity Syndrome Reactions versus Allergy and Drug
Aim: This retrospective study was performed to evaluate the efficacy and tolerability of cyproheptadine versus montelukast as adjuncts to ongoing second-generation antihistamines in adults with refractory chronic urticaria.
Methods: This study included adult patients diagnosed with chronic urticaria who did not respond to standard treatment, divided into two groups. Group A received antihistamines plus oral cyproheptadine for one month, and group B received antihistamines in addition to standard-dose montelukast daily (10 mg) for four months. The weekly urticaria activity score (UAS7), chronic urticaria quality of life questionnaire (CU-Q2oL), and dermatology life quality index (DLQI) scores were measured at the end of grading after four months.
Results: After four months, both groups showed significant improvements in UAS7 and CU-Q2oL scores, and group A also saw a notable increase in DLQI score compared to baseline. Group A showed more pronounced improvements overall. Both groups saw a reduction in background antihistamine usage, with group A experiencing a more significant decrease. Additionally, more patients in group A reported daytime sedation and weight gain compared to group B.
Conclusions: Cyproheptadine, along with second-generation antihistamines, was found to be efficacious and safe as compared to montelukast along with second-generation antihistamines in patients with chronic urticaria.
Chronic urticaria, or hives, is a dermatological response that results in pruritic wheals. Chronic urticaria refers to welts that last for a duration exceeding six weeks and recur often over extended periods, ranging from months to years. Frequently, the etiology of persistent urticaria remains uncertain [1]. Chronic urticaria is a debilitating disease that considerably affects health-related quality of life (QOL). It disrupts both personal satisfaction and daily activities; the health condition of some sufferers resembles that of individuals with coronary artery disease or severe asthma. Additionally, it disrupts family dynamics, impairs performance at work or school, and diminishes the enjoyment of leisure activities.
There is presently no cure for chronic urticaria, and all available treatment methods aim to manage and avoid the symptoms of this condition. Second-generation H1-antihistamines are the recommended treatments at conventional dosages, and can also be used at high doses as an alternative option. A recent analysis found that only 39% of patients with chronic spontaneous urticaria have a positive response to conventional doses of second-generation H1-antihistamines. However, 63% of those who do not react to the standard dosages see improvement when given higher doses of second-generation H1-antihistamines [2]. Cyproheptadine is a first-generation antihistamine with additional characteristics, such as serotonin receptor antagonism. In addition to its antihistamine properties, cyproheptadine is occasionally employed to enhance appetite and facilitate weight gain [3–5]. Cyproheptadine, despite being a first-generation antihistamine, is sometimes considered in the management of chronic urticaria that is not well-controlled with second-generation antihistamines. Second-generation antihistamines, such as cetirizine, loratadine, and fexofenadine, are typically the first line of treatment due to their efficacy and lower sedative effects compared to first-generation antihistamines [6, 7]. With this background, this study was conducted to evaluate the efficacy and safety of oral cyproheptadine and antihistamine as compared to montelukast and antihistamine in adult patients with chronic urticaria not controlled with the highest dose of at least two antihistamines.
The study was performed at one treatment centre specially dedicated to atopic individuals in Kolkata, West Bengal. Patients were categorised according to the treatment they had received during standard clinical practice from 1st January through 30th June 2023.
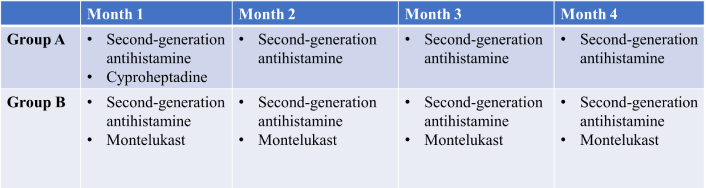
This retrospective study comprised two groups of patients with chronic urticaria who were treated with background second-generation antihistamines for four months. This study was conducted at a single treatment centre. Patients were categorised according to the treatment they had received during standard clinical practice from January through June 2023. Group A: Oral cyproheptadine (4 mg two times a day) manufactured by Geno Pharmaceuticals Pvt. Ltd. was administered as an adjunct for the first month alone, along with ongoing second-generation antihistamines for 4 months. Group B: Oral montelukast (10 mg/day) was given continuously for 4 months, along with second-generation antihistamines. All the outcome measures [weekly urticaria activity score (UAS7), chronic urticaria QOL questionnaire (CU-Q2oL), and dermatology life quality index (DLQI)] were measured at baseline and the end of follow-up at 4 months in both groups (Figure 1). This design was intended to capture real-world prescribing practice in which short-term treatment with cyproheptadine is preferred for tolerability reasons. Adjunct treatments were selected by physicians based on clinical judgment, considering factors like prior response, sedation tolerance, and appetite. All patients met uniform eligibility criteria.
Adult subjects of both sexes with chronic urticaria lasting for over one year and who had failed sequential therapy using the maximum tolerated licensed dose of at least two separate second-generation antihistamines were enrolled. Switching to a new antihistamine rather than up-dosing a single agent was based on the basis of prevailing institutional practice at the time of the study. We acknowledge that this is not the same as the existing guideline-recommended practice of up-dosing a single second-generation antihistamine up to fourfold in non-responders [8].
Baseline demographic information and medical and treatment histories of the participants were also recorded. Levels of immunoglobulin E and total eosinophil count were measured at baseline in all patients.
The CU-Q2oL: This questionnaire helps to measure the effect of chronic urticaria on a person’s QOL. The total score determines the degree of severity of chronic urticaria symptoms for a specified period. The sequential changes of CU-Q2oL scores reflect the overall burden of chronic urticaria on patients in multiple aspects, including spontaneous symptoms during disease remissions and relapses.
UAS7: A validated symptom severity score defined by the presence of hives or wheals occurring at least once weekly for 6 weeks.
CU-Q2oL: Reflects the burden of disease across multiple QOL domains.
DLQI: A general dermatology QOL measure used to assess the impact on daily functioning.
The main endpoint of the study was an improvement of urticaria symptoms and QOL, measured using three validated questionnaires: UAS7, CU-Q2oL, and DLQI, during a four-month follow-up.
The DLQI is the most common type of questionnaire for determining QOL in patients with skin diseases. It is an often-used instrument in dermatology for both clinical research and practice to assess how much skin diseases affect different aspects of daily life. It should be noted that the DLQI itself is not specific to chronic urticaria but rather relevant across a variety of dermatological conditions. The background second-generation antihistamine use (names and doses) was collected for both groups. Data on patient-reported adverse events were also noted.
All data were obtained from the medical records of the patients. Descriptive statistics were employed. The normalcy was assessed using the Kolmogorov-Smirnov test. A paired t-test was conducted to compare the differences within the group. An unpaired t-test was used to compare the differences between the groups. No subgroup analysis was performed. All statistical analysis was performed with SPSS version 18.0 (IBM, Chicago). A p-value of < 0.05 was considered statistically significant.
Initial data collection was conducted from the baseline data from patient medical records, demographics, and pre-treatment history. Follow-up was done through the data on UAS7, CU-Q2oL, and DLQI scores collected during a four-month follow-up by telephonic assessment.
Ethical considerations are included due to the use of medical records and adherence to statistical analysis protocols. This study also received the institutional ethics committee of the concerned institution (approval no. HREC-AARC/37). The work was conducted at the Department of Pharmacology, Allergy and Asthma Treatment Centre, Moulali, Kolkata, West Bengal, India.
A total of 103 participants were included. SPSS version 18.0 was used for testing purposes. Tests run include the Kolmogorov-Smirnov test on normality, the paired t-test to compare within groups for differences, and unpaired t-test that compare differences between groups. Values at p < 0.05 were considered significant.
The total sample size fulfilled the eligibility criteria and was considered for analysis. The average age of the patients was 40.9 ± 13.8 years, and 48.5% of the patients were males. There was no missing data. The demographic characteristics, medical history, and treatment history of the patients are enumerated in Table 1. The demographic characteristics of the patients in the two groups did not differ significantly at baseline. Loratidine was the most common antihistamine used in both groups.
Baseline characteristics of the study population.
| Parameters | Group A (n = 48) | Group B (n = 55) |
|---|---|---|
| Age (years) | 41.5 ± 14.4 | 40.4 ± 13.3 |
| Gender (% male) | 26 (54.2%) | 24 (43.6%) |
| Occupation | Business 10 (20.8%)Professional 10 (20.8%)Retired 12 (25%)Service 8 (16.7%)Student 5 (10.4%)Daily wage worker 3 (6.3%) | Business 11 (20%)Professional 18 (32.7%)Retired 13 (23.6%)Service 9 (16.4%)Student 2 (3.6%)Daily wage worker 2 (3.6%) |
| Education | School 5 (10.4%)Graduate 33 (68.8%)Postgraduate 10 (20.8%) | School 10 (18.2%)Graduate 38 (69.1%)Postgraduate 7 (12.7%) |
| Body mass index (kg/m2) | 22.80 ± 3.23 | 22.58 ± 3.08 |
| Present medical history | Diabetes mellitus 24 (50%)Chronic obstructive pulmonary disease 16 (33.3%)Arthritis 4 (8.3%)Hypertension 12 (25%)Others 8 (16.7%) | Diabetes mellitus 30 (54.5%)Chronic obstructive pulmonary disease 21 (38.2%)Arthritis 4 (7.3%)Hypertension 13 (23.6%)Others 10 (18.2%) |
| Family history of chronic urticaria | 24 (50%) | 29 (52.7%) |
| Duration of chronic urticaria (in years) | 5.88 ± 2.5 | 6.04 ± 2.62 |
| Immunoglobulin E (IU/mL) | 610.98 ± 194.44 | 607.40 ± 185.05 |
| Eosinophil count (/cu mm) | 564.74 ± 95.04 | 574.84 ± 83.47 |
| Antihistamine used | ||
| Loratadine | 24 (50%) | 29 (52.7%) |
| Desloratadine | 12 (25%) | 10 (18.2%) |
| Cetirizine | 6 (12.5%) | 9 (16.4%) |
| Levocetirizine | 10 (20.8%) | 10 (18.2%) |
| Fexofenadine | 12 (25%) | 13 (23.6%) |
| Baseline weekly urticaria activity score | 35.74 ± 3.70 | 35.38 ± 3.80 |
| Baseline chronic urticaria quality of life questionnaire score | 96.16 ± 11.67 | 94.16 ± 10.79 |
| Baseline dermatology life quality index score | 22.92 ± 3.70 | 23.14 ± 4.34 |
The totals for “Present medical history” and “Antihistamine used” exceed the number of patients because individuals may have multiple comorbid conditions and/or were prescribed multiple antihistamines concurrently. Here, “Graduate” refers to completion of a university undergraduate degree, while “School” refers to completion of school-level education (up to 12th standard or equivalent).
At the end of four months, there were significant improvements in the UAS7 and CU-Q2oL scores in both groups and the DLQI score in group A as compared to the corresponding baseline values. However, the improvements were more marked in group A, as confirmed by the significant differences in the inter-group scores between the two groups at the end of 4 months (Table 2). There was a 69.4% reduction in the UAS7 in group A as compared to 39.9% in group B (difference of 29.5%). There was a 62.5% reduction in the CU-Q2oL score in group A as compared to 26.5% in group B (difference of 36%). There was a 73.7% reduction in the DLQI score in group A as compared to 12.5% in group B (difference of 61.2%). The background second-generation antihistamines used at the end of four months are detailed in Table 3.
Outcome parameters at 4 months.
| Parameters | Group A (n = 48) | Percentage reduction from baseline (group A) | Intra-group p-value (group A) | Group B (n = 55) | Percentage reduction from baseline (group B) | Intra-group p-value (group B) | Inter-group p-value |
|---|---|---|---|---|---|---|---|
| 4 months UAS7 | 10.94 ± 2.28* | 69.4% | < 0.05 | 21.26 ± 3.65* | 39.9% | < 0.05 | < 0.001 |
| 4 months CU-Q2oL | 36.06 ± 5.94* | 62.5% | < 0.05 | 69.24 ± 13.67* | 26.5% | < 0.05 | < 0.001 |
| 4 months DLQI | 6.02 ± 1.85* | 73.7% | < 0.05 | 20.24 ± 5.28 | 12.5% | < 0.05 | < 0.001 |
Group A received cyproheptadine for 1 month + antihistamines; group B received montelukast for 4 months + antihistamines. Both groups continued second-generation antihistamines throughout. *: p < 0.05 corresponding to the baseline values. UAS7: weekly urticaria activity score; CU-Q2oL: chronic urticaria quality of life questionnaire; DLQI: dermatology life quality index.
Background antihistamine used at the end of four months.
| Group A | Group B | ||
|---|---|---|---|
| Antihistamine used (%) | Loratadine | 38.7 | 33.3 |
| Desloratadine | 25.8 | 26.7 | |
| Cetirizine | 9.7 | 11.1 | |
| Levocetirizine | 19.4 | 11.1 | |
| Fexofenadine | 6.5 | 17.8 | |
| Total | 100 | 100 | |
| Median dose of antihistamine used (mg/day) | Loratadine | 10 | 10 |
| Desloratadine | 5 | 5 | |
| Cetirizine | 10 | 20 | |
| Levocetirizine | 5 | 10 | |
| Fexofenadine | 60 | 180 | |
Regarding the patient-reported adverse events, there was a significant increase in the proportion of patients in group A as compared to those in group B who complained of daytime sedation and weight gain at the end of 4 months. The distributions of other adverse events (nausea and vomiting, abdominal pain, dry mouth, and blurred vision) were similar in both groups. A detailed distribution of patient-reported adverse events in both groups is provided in Table 4.
Distribution of patient-reported adverse events in both groups.
| Adverse drug reaction | Group A (n = 48) | Group B (n = 55) | p-value |
|---|---|---|---|
| Nausea and vomiting | 4 (8.3%) | 5 (9.1%) | 0.18 |
| Abdominal pain | 3 (6.3%) | 5 (9.1%) | 0.23 |
| Daytime sedation | 30 (62.5%) | 12 (21.8%) | 0.02 |
| Dry mouth | 15 (31.3%) | 18 (32.7%) | 0.54 |
| Weight gain (> 10%) | 5 (10.4%) | 1 (1.8%) | 0.04 |
| Blurred vision | 10 (20.8%) | 8 (14.5%) | 0.13 |
The totals exceed the number of patients because individual patients could report more than one adverse event.
Chronic urticaria presents a continuous difficulty, characterised by recurring hives and/or angioedema that remain for more than six weeks. Although second-generation antihistamines are widely used in treatment protocols, some patients do not receive sufficient relief or have side effects that they cannot tolerate. As a result, it is necessary to explore other therapeutic techniques [9, 10]. Our study, to the best of our knowledge, for the first time, demonstrated a significant improvement in patients treated with cyproheptadine after 4 months of UAS7 when compared to patients with standard of care (SOC) only. It is well established that treatment with antihistamines significantly reduces the UAS7 compared to non-treated patients [11, 12]. Second-generation antihistamines such as cetirizine, loratadine, fexofenadine, levocetirizine, and desloratadine are commonly prescribed due to their effectiveness and minimal sedative effects, certain individuals with chronic urticaria may experience resistance to these medications or encounter undesirable side effects [9, 13–15].
Cyproheptadine, a first-generation antihistamine that also blocks serotonin receptors, shows promise as a potential treatment for chronic urticaria that does not respond to second-generation antihistamines. Cyproheptadine, unlike other first-generation antihistamines, has a dual mode of action that can provide distinct benefits in some situations, despite the common sedative effects associated with this class of drugs [16, 17]. Our data also showed significant improvement in the CU-Q2oL value in cyproheptadine-treated patients as compared to the patients with SOC, which corroborates previous studies [18, 19]. Cyproheptadine’s inhibition of the histamine H1 receptor specifically targets the histaminergic aspect of urticaria, effectively alleviating itching and the formation of raised, red skin lesions known as wheals [20–22]. Moreover, its ability to counteract the effects of serotonin receptors may enhance its effectiveness in situations where serotonin is involved in the development of chronic urticaria [23, 24]. Cyproheptadine is still readily available and, in much of the country where the study was done, is available over the counter, which explains its persistent use in ordinary clinical practice where more recent biologic therapies might be less readily available.
In this study, we found that cyproheptadine significantly improved the QOL in patients with chronic urticaria as evidenced by the improvements in UAS7, CU-Q2oL, and DLQI scores. As compared to montelukast, cyproheptadine treatment led to 29.5% higher reduction in the symptom’s severity, 36% reduction in the impact of chronic urticaria on the QOL, and 61.2% higher reduction in the impact of skin diseases on the QOL among patients with chronic urticaria. As a result, individuals experience a reduction in the frequency and severity of hives, leading to improved sleep, decreased anxiety, and an overall enhancement in their QOL. The ability of cyproheptadine to address the troublesome symptoms of chronic urticaria underscores its importance in the management and treatment of this challenging condition, allowing patients to regain control and enjoy a more comfortable and fulfilling daily life. The only adverse effect noted was sedation, which is rather beneficial in patients with chronic urticaria. Cyproheptadine is notable for its ability to stimulate hunger. This feature might benefit patients with chronic idiopathic urticaria who experience weight loss or lack of appetite, either because it is directly due to the disease processes or treatment options in use [25, 26]. Although the evidence supporting the use of cyproheptadine in chronic urticaria is not as extensive as that for second-generation antihistamines, studies have demonstrated promising results, suggesting potential advantages for patients who do not respond to second-generation antihistamines [27–30]. Although first-generation antihistamines may have the potential to benefit, consideration should be given to the sedative side effects of cyproheptadine. Patients should be warned that sleepiness can occur, and they should not engage in cognitive vigilance tasks. Cyproheptadine may be a useful adjuvant or adjunct to second-generation antihistamines in the treatment of refractory chronic urticaria. It is independent because of its bireceptor [histamine and 5-hydroxytryptamine (5-HT)] dualism, in addition to being an appetite stimulant. However, the use of cyproheptadine should be decided on a case-by-case basis with appropriate patient assessments and potential adverse effects.
Chronic urticaria is a “potentially disabling” affliction that inefficiently managed, might compromise the well-being of patients, highlighting further emphasis on evaluating economic implications. Its goal is to fill an important treatment gap by comparing the therapeutic effect and safety of cyproheptadine and montelukast when added to a second-generation antihistamine. It uses a retrospective design, which means that no intervention takes place and the work only makes use of existing data to help drive discussion on real-world insights. It uses full and validated measurement instruments such as UAS7, CU-Q2oL, or DLQI to evaluate not only disease severity but also QOL. The statistical analysis is complete, using the correct techniques and SPSS software. Including percentage score reductions and adverse events, results on the effectiveness of treatments were given in great detail.
This study had some limitations. It was a retrospective analysis, based on likely biased medical records, and the lack of randomisation introduces selection bias. It is often difficult to determine the effects of these treatments in isolation without a control group. It is possible that the 4-month follow-up period was insufficient to capture longer-term effects, and adverse event grades are not reported. For example, the analysis may be underpowered to detect differences as a result of its small sample size, and this single-institution study might not reflect results from other practices. To conclude, oral cyproheptadine, along with second-generation antihistamines, was found to be efficacious and safe as compared to montelukast along with second-generation antihistamines in patients with chronic urticaria. However, use of cyproheptadine must be weighed against side effects, especially sedation and increased appetite, that are likely to compromise compliance and everyday functioning. Additional investigation is necessary to determine the most effective dosage schedules and uncover certain characteristics of patients who may experience the greatest advantages from using cyproheptadine for the treatment of chronic urticaria.
CU-Q2oL: chronic urticaria quality of life questionnaire
DLQI: dermatology life quality index
QOL: quality of life
SOC: standard of care
UAS7: weekly urticaria activity score
We thank Monkwriter (https://monkwriter.com/) for providing professional assistance in scientific writing of this article.
SSS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing—original draft. AD: Data curation, Formal analysis, Validation, Writing—review & editing, Supervision. S Moitra: Methodology, Resources, Supervision, Writing—review & editing. S Mukherjee: Investigation, Resources, Writing—review & editing. NC: Resources, Validation, Writing—review & editing. SRJ: Supervision, Project administration, Funding acquisition. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The study was approved by the Institutional Ethics Committee, Allergy and Asthma Treatment Centre, Moulali, Kolkata, West Bengal, India (approval no. HREC-AARC/37). Because of the retrospective design, the requirement of informed consent was waived. Our study was conducted in accordance with the principles outlined in the Declaration of Helsinki (2024 revision) as adopted by the World Medical Association.
As this was a retrospective study based on existing records, individual informed consent was waived by the Institutional Ethics Committee.
Not applicable.
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
This study was funded by “Geno Pharmaceuticals Pvt. Ltd.”. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 4317
Download: 27
Times Cited: 0