 Review
Review

Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, Tbilisi 0160, Georgia
ORCID: https://orcid.org/0009-0006-6693-8212
Affiliation:
2Faculty of Medicine, Karachi Medical and Dental College, Karachi 74700, Pakistan
ORCID: https://orcid.org/0009-0006-7518-212X
Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, Tbilisi 0160, Georgia
Email: islam1048@gmail.com
ORCID: https://orcid.org/0009-0007-4855-6226
Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, Tbilisi 0160, Georgia
ORCID: https://orcid.org/0009-0005-2904-4626
Affiliation:
1Faculty of Medicine, Tbilisi State Medical University, Tbilisi 0160, Georgia
ORCID: https://orcid.org/0009-0005-7056-3022
Affiliation:
3Faculty of Medicine, The University of Georgia, Tbilisi 0171, Georgia
ORCID: https://orcid.org/0009-0007-1102-8577
Affiliation:
3Faculty of Medicine, The University of Georgia, Tbilisi 0171, Georgia
ORCID: https://orcid.org/0009-0005-5098-3548
Affiliation:
3Faculty of Medicine, The University of Georgia, Tbilisi 0171, Georgia
ORCID: https://orcid.org/0009-0006-3927-3833
Explor Drug Sci. 2026;4:1008159 DOI: https://doi.org/10.37349/eds.2026.1008159
Received: January 17, 2026 Accepted: March 24, 2026 Published: May 18, 2026
Academic Editor: Prasat Kittakoop, Chulabhorn Graduate Institute, Thailand
Antimicrobial resistance (AMR) poses a growing global health threat, progressively undermining the clinical effectiveness of conventional antibiotic therapies. Despite their proven efficacy and standardized clinical frameworks, antibiotics exert strong selective pressures that accelerate resistance, disrupt host microbiota, and limit treatment options for chronic, biofilm-associated, and multidrug-resistant infections. Bacteriophage therapy has re-emerged as a potential adjunct or alternative approach, offering pathogen-specific antibacterial activity, preservation of commensal microbiota, and the capacity for co-evolution with bacterial hosts. This focused review critically compares antibiotics and bacteriophage therapy across mechanistic foundations, preclinical and clinical evidence, translational readiness, and real-world implementation challenges. While preclinical models consistently demonstrate robust antibacterial activity of bacteriophages, clinical evidence remains heterogeneous, with few randomized controlled studies available. Key system-level barriers, including regulatory inconsistency, manufacturing complexity, and lack of standardization, currently limit widespread clinical integration. Rather than positioning bacteriophages as replacements for antibiotics, this review emphasizes their potential role as complementary agents, particularly through bacteriophage-antibiotic synergy, to enhance treatment efficacy and mitigate resistance. Addressing methodological gaps, standardizing clinical trial designs, and developing integrated stewardship models will be critical to defining the future role of bacteriophage therapy in modern infectious disease management.
Antimicrobial resistance (AMR), which is now acknowledged as a danger to world health, is progressively reducing the efficacy of standard therapies for bacterial infections [1–4]. According to data from the European Commission, there are around 33,000 AMR-related deaths in the European Union (EU) each year [2]. Higher mortality, prolonged hospitalization, and increased healthcare costs are associated with resistant organisms, disproportionately affecting low- and middle-income countries (LMICs) [2, 5].
However, the development of novel antibiotics has slowed markedly, reflecting a prolonged stagnation of the antibiotic pipeline driven by scientific challenges, complex regulatory requirements, and inadequate economic incentives [2, 4, 6]. The focus has shifted back to non-traditional antibacterial tactics as current treatments become less effective [4, 7, 8]. Due to its potential for targeted bacterial killing and compatibility with antimicrobial stewardship principles, bacteriophage therapy, originally explored prior to the antibiotic era, has re-emerged in contemporary research [1, 3, 8–10]. The clinical role of bacteriophage therapy remains uncertain due to the gap between a strong biological rationale and limited high-quality clinical evidence. Historically, enthusiasm for bacteriophage therapy has resurfaced during periods of antibiotic scarcity, only to wane as challenges related to standardization, regulatory approval, and clinical scalability emerged. These recurring translational failures underscore the importance of critically examining not only biological efficacy but also system readiness.
In light of this, it is essential to evaluate bacteriophage therapy critically. This scoping review aims to critically evaluate the role of bacteriophage therapy as a potential adjunct or alternative to antibiotics within modern infectious disease frameworks. It synthesizes mechanistic, preclinical, and clinical evidence to assess therapeutic potential, while identifying key translational, regulatory, and implementation barriers that influence real-world applicability [3, 4]. Bacteriophage therapy and traditional antibiotics are compared in three areas: mechanisms of action, clinical results, and implementation limitations [6, 7, 11]. The review summarizes the existing body of research, points out knowledge gaps, and emphasizes obstacles to clinical translation using a scoping methodology. This scoping approach focuses on mapping mechanistic, preclinical, and clinical evidence rather than quantitatively synthesizing outcomes.
This scoping review was conducted to map the available mechanistic, preclinical, and clinical evidence on bacteriophage therapy in the context of AMR. A structured literature search was performed in PubMed/MEDLINE, Embase, Scopus, and Web of Science for articles published between January 2014 and November 2025. The search combined controlled vocabulary and free-text terms, including (“bacteriophage therapy” OR “bacteriophage therapy” OR “bacteriophage-antibiotic synergy”) AND (“antimicrobial resistance” OR “multidrug-resistant” OR “biofilm”) AND (“clinical trial” OR “case series” OR “observational study” OR “compassionate use” OR “preclinical”). Reference lists of relevant articles were manually screened to identify additional eligible studies. Only full-text articles published in English were included.
Studies were included if they reported clinical, preclinical, or mechanistic data relevant to therapeutic bacteriophage use, bacteriophage-antibiotic synergy (PAS), or translational aspects of bacteriophage therapy in human infectious disease. Eligible designs included randomized trials, observational studies, case series, case reports, and experimental models. Articles without primary data (editorials, commentaries), conference abstracts without full text, veterinary-only studies without human relevance, and studies involving exclusively temperate bacteriophages without therapeutic intent were excluded. Titles and abstracts were screened for relevance, followed by full-text review of potentially eligible studies. Data were charted using a predefined framework including study design, infection type, pathogen, treatment characteristics, comparator when available, and reported outcomes. Evidence was synthesized descriptively, and studies were categorized according to level of evidence based on study design.
This review followed the methodological framework for scoping reviews and was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR). The objective was to characterize the scope, quality, and limitations of existing evidence rather than to perform quantitative meta-analysis. Findings were organized into thematic domains, including mechanistic foundations, preclinical evidence, clinical outcomes, PAS, and system-level barriers. Particular emphasis was placed on critical appraisal of study design, risk of bias, comparator availability, and generalizability of clinical findings to routine practice.
Antibiotics represent the pharmacological cornerstone of antibacterial treatment, operating through highly standardized and predictable mechanisms to inhibit bacterial growth or induce cell death. There are two types of drugs: bactericidal agents, like β-lactams and fluoroquinolones, kill the target cells, and bacteriostatic agents stop replication and rely on the host immune system to get rid of pathogens [12]. Antibiotic efficacy derives from predictable targeting of bacterial structures and processes essential for survival, including cell wall synthesis, protein synthesis, and nucleic acid replication [13].
Despite initial effectiveness, antibiotics exert strong selective pressure that accelerates bacterial resistance. Genetic mutations can change the drug target site or make the membrane less permeable. Moreover, horizontal gene transfer lets bacteria acquire mobile resistance genes, which are often enzymes that break down drugs like β-lactamases or efflux pumps [14].
Furthermore, biofilm formation and persistence are key components in resistance. A protective extracellular matrix in biofilms shields bacteria from high drug concentrations [14]. Furthermore, the broad-spectrum properties of various antibiotics cause significant collateral damage to the host microbiota, disrupting beneficial commensal populations and creating conditions favorable for opportunistic pathogen proliferation or secondary infection [15, 16].
The mechanistic foundation of conventional antibiotic therapy exposes inherent constraints, particularly in the treatment of complex and chronic infections. The diminished effectiveness in biofilms and chronic infections is a critical concern, as insufficient drug penetration into these safeguarded, stationary bacterial aggregates limits treatment efficacy [14]. Pharmacokinetic and penetration issues, including insufficient drug concentration at the infection site, complicate the management of chronic infections. The widespread use of antibiotics exerts considerable selective pressure that exacerbates the global AMR crisis, diminishing the effective lifespan of current medications [17, 18]. Despite these mechanistic limitations, antibiotics retain decisive clinical advantages, including suitability for empiric therapy, standardized dosing, predictable exposure-response relationships, and immediate availability in acute care settings, features that bacteriophage therapy currently lacks.
Bacteriophages are classified as temperate or virulent. Temperate bacteriophages integrate into the bacterial genome as prophages, establishing a heritable lysogenic state that can alter host biology and may be induced to enter lytic replication under cellular stress. Virulent bacteriophages replicate exclusively via the lytic cycle. Consequently, clinical bacteriophage therapy is restricted to obligately lytic bacteriophages, as temperate bacteriophages are excluded due to safety concerns associated with genomic integration and virulence modulation [19]. Although obligately lytic bacteriophages are preferentially selected for therapeutic use, concerns remain regarding generalized or specialized transduction and the inadvertent mobilization of bacterial genetic material, necessitating rigorous genomic screening of therapeutic bacteriophage preparations.
Antibacterial strategies distinct from conventional antibiotics are gaining attention as ways to overcome resistance. Mechanisms like enzymatic bacterial lysis, such as bacteriophage-derived endolysins, directly degrade essential components of the bacterial cell wall, leading to rapid cell death and a low likelihood of cross-resistance with antibiotics [20]. Another advantage is their activity against dormant or biofilm-embedded bacteria. Unlike antibiotics that target active metabolism, lytic enzymes and bacteriophages can kill slow-growing “persister” cells and disrupt biofilm structures, which are major contributors to chronic infections [21]. Finally, co-evolutionary dynamics play a key role: Bacteriophages and bacteria evolve together, meaning bacterial resistance can be countered by bacteriophage adaptation, unlike static antibiotic molecules [22]. Importantly, bacteriophage-derived enzymes such as endolysins represent a distinct therapeutic category with pharmacological properties that differ substantially from whole-bacteriophage therapy, including reduced immunogenic complexity and greater dosing predictability.
These agents often act on specific bacterial species or strains, minimizing disruption to beneficial commensal microbiota, unlike broad-spectrum antibiotics that can cause dysbiosis [23]. This specificity also leads to reduced off-target effects, lowering the risk of collateral damage to host cells and decreasing side effects associated with systemic antibiotic use [24]. Another key strength is their potential synergy with antibiotics. Bacteriophages and endolysins can enhance antibiotic penetration into biofilms or resensitize resistant bacteria, resulting in improved bacterial clearance when used in combination therapies [25]. Together, these mechanistic characteristics support continued investigation of targeted strategies alongside conventional antibiotics.
Unlike antibiotics, bacteriophages are biologically active entities that interact directly with the host immune system. Systemically administered bacteriophages may be rapidly cleared through innate immune mechanisms, including phagocytosis, complement activation, and hepatic or splenic sequestration. Additionally, adaptive immune responses can generate neutralizing antibodies that reduce bacteriophage efficacy upon repeated administration. These immune interactions complicate dose optimization, limit repeat dosing, and may partially explain variable clinical responses observed across compassionate-use cases.
While antibiotics offer standardized, broad-spectrum coverage suitable for empiric and acute use, bacteriophage therapy provides precision targeting that minimizes collateral microbiome disruption but introduces logistical and biological constraints [26]. This specificity necessitates pathogen identification, bacteriophage matching, and tailored preparation, complicating routine clinical deployment compared with antibiotics’ established, scalable frameworks [27, 28].
In contrast to antibiotics, bacteria-phage interactions are governed by adaptive co-evolution, in which bacterial resistance mechanisms and bacteriophage counter-adaptations emerge concurrently. Bacteria gain resistance through immune systems, such as CRISPR-Cas or surface receptor changes, during phage-bacteria coevolution, while bacteriophages develop new receptor specificities or anti-defense mechanisms to prevent these bacterial defenses. Bacteriophage resistance has been reported in a substantial proportion of in vivo studies, highlighting that resistance evolution is not unique to antibiotics [26, 29]. Thus, resistance dynamics differ qualitatively between antibiotics and bacteriophages: Antibiotic resistance accumulates unidirectionally, whereas bacteriophage resistance exists within a dynamic evolutionary arms race [30]. Taken together, antibiotics and bacteriophages represent fundamentally different therapeutic paradigms: one optimized for population-level scalability and empiric deployment, the other for precision targeting under controlled conditions. These differences shape not only their resistance dynamics but also their feasibility within modern clinical workflows. These mechanistic and clinical distinctions between antibiotics and bacteriophage therapy are summarized in Table 1, highlighting their fundamentally different therapeutic paradigms. The contrasting clinical deployment workflows of antibiotics and bacteriophage therapy are illustrated in Figure 1.
Comparative mechanistic and clinical properties of antibiotics vs. bacteriophages.
| Dimension | Antibiotics | Bacteriophage therapy | Clinical implication |
|---|---|---|---|
| Nature of agent | Small-molecule chemical | Replicating biological entity | Different regulatory and PK frameworks required |
| Target flexibility | Fixed molecular targets | Adaptable receptor targeting | Resistance dynamics fundamentally differ |
| Activity requirement | Active bacterial metabolism | Can act on dormant/biofilm cells | Advantage in chronic infections |
| Dose-response predictability | High | Variable, context-dependent | Limits standardization |
| In vivo amplification | None | Yes (host-dependent) | Complicates PK/PD modeling |
| Resistance trajectory | Accumulative | Oscillatory (coevolution) | Resistance may carry fitness costs |
| Empiric usability | High | Low | Limits acute-care use |
| Clinical scalability | Mature | Experimental | Adoption depends on infrastructure |
PK: pharmacokinetic; PD: pharmacodynamic.
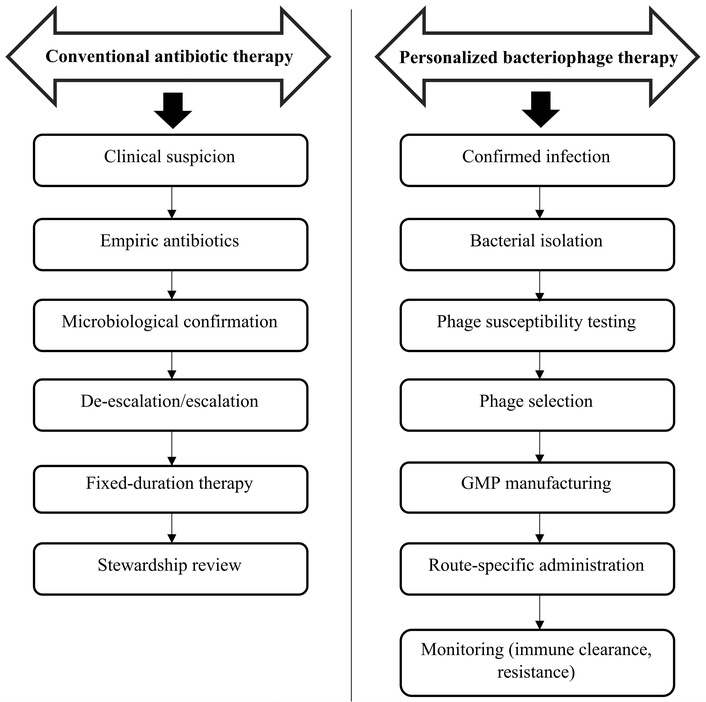
Therapeutic workflow comparison: antibiotics vs bacteriophage therapy. GMP: Good Manufacturing Practice.
Despite their established role, antibiotics are limited by progressive resistance development, ecological disruption of the microbiome, and reduced efficacy in biofilm-associated infections, as previously described [14, 17]. In contrast, bacteriophage therapy faces fundamentally different constraints, including narrow host specificity, dependence on pathogen identification, immunogenic clearance, and lack of standardized dosing frameworks [27]. While antibiotics are constrained by biological resistance, bacteriophage therapy is primarily limited by logistical, regulatory, and scalability challenges [28]. This distinction highlights that the barriers to these modalities are not equivalent but operate at different levels, biological versus system-level.
Preclinical investigations consistently demonstrate that bacteriophage therapy possesses robust antibacterial activity across a wide range of experimental systems. In vitro studies and animal infection models show effective bacterial killing, reduction in bacterial burden, and improved survival across multiple pathogens, including multidrug-resistant (MDR) organisms. Systematic reviews and meta-analyses of preclinical studies report reproducible efficacy of bacteriophage therapy in models of systemic infection, pneumonia, skin and soft tissue infection, and biofilm-associated disease [31]. Notably, bacteriophages and bacteriophage-derived lytic enzymes demonstrate activity against biofilm-embedded and slow-growing bacterial populations that are often refractory to antibiotics. These findings provide strong biological plausibility and support continued investigation of bacteriophages as antibacterial agents [30].
Despite these encouraging results, the translational relevance of preclinical bacteriophage models remains limited. Experimental systems frequently employ simplified infection settings that do not reflect the spatial, immunological, and microbiological complexity of human disease. Preclinical studies often use unrealistically high multiplicities of infection, short treatment durations, mono-microbial infections, and abbreviated follow-up periods that fail to capture relapse, resistance emergence, or immune-mediated clearance [32]. In addition, outcome measures such as bacterial load reduction or short-term survival do not reliably predict durable clinical cure. As a result, preclinical efficacy frequently overestimates real-world effectiveness, contributing to the discrepancy between strong laboratory performance and inconsistent clinical outcomes [31]. A central limitation to translation lies in the absence of standardized pharmacokinetic and pharmacodynamic (PK/PD) frameworks for bacteriophage therapy. Unlike antibiotics, whose dosing strategies are guided by well-characterized exposure-response relationships, bacteriophage behavior in vivo is influenced by complex and poorly defined variables, including host immune clearance, tissue penetration, bacterial density, and in situ replication dynamics.
Systemically administered bacteriophages may be rapidly neutralized or cleared before reaching target sites, an effect rarely captured in preclinical models. Variability in dosing strategies, routes of administration, and resistance monitoring further complicates cross-study comparison and trial design [33]. Addressing these PK/PD uncertainties through integrated preclinical models that incorporate immune responses and clinically relevant endpoints will be essential for improving translational predictability and enabling rigorous clinical evaluation [31, 34, 35]. Despite consistent antibacterial activity in experimental models, the clinical translatability of preclinical bacteriophage studies remains limited, as simplified study designs and a lack of immune-system integration frequently lead to overestimation of real-world effectiveness.
As AMR has intensified, increasing emphasis has been placed on optimizing and reducing antibiotic use. Reducing antibiotic use in the acute hospital context presents particular obstacles, including the need for rational decision-making before full diagnostic test findings are available, uncertainty about diagnosis and severity of illness, and a high-pressure environment [36]. Reducing antibiotic duration is one of the most widely applied antibiotic stewardship methods documented in the literature, and it is also regarded as the safest and most acceptable by practicing clinicians. This involves shorter courses for established bacterial infections, avoiding bacterial infections, and quickly discontinuing antibiotic prescriptions once bacterial infections have been eliminated. The customary principle for antibiotic duration was to treat beyond clinical improvement to prevent both infection return and antibiotic resistance development [37].
Effective antimicrobial prescribing requires accurate diagnosis, distinction between empiric and definitive therapy, timely de-escalation, and selection of the narrowest effective agent for the shortest appropriate duration. Understanding medication properties unique to antimicrobial drugs (such as pharmacodynamics and efficacy at the site of infection), accounting for biologic influences that impact antimicrobial activity, and, finally, recognizing the negative consequences of antimicrobial agents on the host [38]. The use of PK/PD modelling and simulation can increase the quantity of therapeutically valuable information acquired from a small number of patients, directing optimal therapy and fully aligning with the goals of personalized medicine [39]. Innovative trial designs have been developed to define duration–response relationships, enabling evidence-based optimization of antibiotic therapy. Larger randomized trials will enable significant findings for patient subsets with diverse host and pathogen features [37, 40].
Reduced microbial diversity, altered microbiota functional characteristics, and the emergence and selection of antibiotic-resistant strains that make hosts more vulnerable to infection with pathogens like clostridium difficile are just a few of the detrimental effects of antibiotic-induced changes in microbial composition on host health [41]. Long-term changes in the microbiome brought on by antibiotics may potentially have an indirect impact on health. The human body’s mutualistic microorganisms participate in immunological and metabolic homeostasis regulation and interact with several physiological processes. Antibiotic exposure can thereby change many fundamental physiological balances, which can lead to chronic illness. Despite well-established efficacy and regulatory frameworks, antibiotic therapy is increasingly constrained by resistance evolution, ecological disruption, and diminishing therapeutic durability [42]. These limitations provide the clinical context in which alternative or adjunctive approaches, including bacteriophage therapy, are being explored.
The clinical contexts in which bacteriophage therapy is most appropriately positioned, relative to conventional antibiotics, are summarized in Table 2.
Clinical positioning of bacteriophage therapy relative to antibiotics.
| Clinical scenario | Antibiotics | Bacteriophage therapy | Recommended role |
|---|---|---|---|
| Acute sepsis | First-line | Impractical | Insufficient evidence for routine use in acute sepsis |
| MDR infection | Limited | Potential | Adjunct/salvage |
| Biofilm-associated | Often ineffective | Active | Targeted adjunct |
| Implant infection | Partial | Local efficacy | Combined therapy |
| Recurrent infection | Resistance-prone | Adaptive | Case-dependent |
| Empiric therapy | Standard | Impossible | Contraindicated |
MDR: multidrug-resistant.
The literature search identified a limited number of clinical publications evaluating bacteriophage therapy in human infections, consisting predominantly of case reports, case series, retrospective observational studies, and compassionate-use programs, with very few controlled trials available. Most reported clinical applications involve patients with refractory, MDR, or biofilm-associated infections in whom conventional antibiotic therapy had failed, reflecting the current role of bacteriophage therapy as a salvage or adjunctive intervention rather than a first-line treatment. The available studies demonstrate biological feasibility and occasional clinical success; however, the evidence base remains heterogeneous in study design, patient selection, bacteriophage preparation, dosing strategy, and outcome definitions, limiting the ability to draw firm conclusions regarding comparative effectiveness relative to standard antibiotic therapy [43–47].
Several reports describe personalized bacteriophage therapy administered after pathogen isolation and in vitro susceptibility testing, often in combination with antibiotics. While these approaches reflect the precision-targeted nature of bacteriophage therapy, they also introduce substantial variability that complicates cross-study comparison and reduces external validity. In contrast to antibiotic trials, most bacteriophage studies lack standardized endpoints, predefined treatment protocols, and comparator arms, making interpretation of reported success rates challenging. Consequently, the current clinical literature should be interpreted primarily as proof-of-concept evidence rather than definitive efficacy data. The characteristics, study design, and level of evidence of the principal clinical reports identified in this review are summarized in Table 3.
Summary of clinical studies of bacteriophage therapy.
| Study | Design | N | Infection type | Comparator | Route of administration | Reported outcome |
|---|---|---|---|---|---|---|
| Pirnay et al. [44] | Multicenter retrospective observational study | 100 | Mixed refractory infections | None | Local/IV/topical | Variable response; feasibility demonstrated |
| Gibb & Hadjiargyrou [45] | Case series/observational | 236 | Skeletal/postsurgical infections | None | Local/subcutaneous/drains | about 92% infection control reported |
| Dedrick et al. [46] | Compassionate-use case series | 20 | Drug-resistant mycobacterial infections | None | IV/aerosol/combined | Mixed response; acceptable safety |
| Metsemakers et al. [47] | Observational clinical review | — | Musculoskeletal/SSTI | None | Various | Feasibility but limited comparative data |
IV: intravenous; —: none specified; SSTI: skin and soft tissue infections.
An observational series involving 236 patients with skeletal and postsurgical infections treated with bacteriophage preparations reported infection control in approximately 92% of cases; however, the absence of a control group, heterogeneous treatment protocols, and inclusion of patients after failure of conventional therapy introduce substantial selection bias and limit interpretation of efficacy [45]. Outcome definitions were not standardized, and long-term follow-up was limited, making it difficult to distinguish bacteriophage-specific effects from concomitant surgical or antibiotic interventions.
Compassionate-use treatment of 20 patients with drug-resistant mycobacterial infections demonstrated the feasibility of intravenous or aerosolized bacteriophage administration with acceptable short-term safety, but treatment regimens were individualized, no comparator arm was available, and response criteria were inconsistent, restricting generalizability [46]. Similarly, a multicenter retrospective analysis of personalized bacteriophage therapy in 100 cases showed clinical feasibility but highlighted substantial variability in bacteriophage selection, dosing, and infection type, reflecting the current use of bacteriophage therapy primarily in specialized salvage settings rather than standardized clinical practice [44].
Overall, the available clinical literature is dominated by uncontrolled observational reports in refractory infections, with heterogeneous protocols and limited external validity. Consequently, reported success rates should be interpreted cautiously and cannot establish comparative effectiveness relative to conventional antibiotic therapy.
The current clinical evidence for bacteriophage therapy is limited by substantial selection bias, as most reported cases involve refractory infections after failure of conventional antibiotics, restricting comparison with routine clinical populations [43, 44]. Publication bias is also likely, and marked heterogeneity in bacteriophage preparation, dosing, administration route, and outcome definitions limits reproducibility across studies [44, 47].
Another major limitation is the scarcity of randomized controlled trials (RCT) with active comparator arms. Most available studies lack standardized clinical endpoints, long-term follow-up, and pharmacokinetic or pharmacodynamic evaluation, reducing confidence in reported efficacy [43, 47]. Notably, RCT evaluating bacteriophage therapy remain extremely limited. Existing trials are often small, underpowered, or lack standardized endpoints and comparator arms. This contrasts sharply with antibiotic development, where large-scale, multi-center randomized trials define efficacy, dosing, and safety. The absence of robust randomized evidence represents a major barrier to regulatory approval and clinical adoption. In addition, the individualized nature of bacteriophage therapy, while biologically advantageous, limits scalability and external validity, as results from specialized centers with curated bacteriophage libraries may not be generalizable to routine practice [48].
Overall, current clinical data support feasibility in selected refractory infections but remain insufficient to establish comparative effectiveness relative to conventional antibiotic therapy, underscoring the need for standardized, controlled trials with clearly defined endpoints [43, 47]. Taken together, current clinical evidence supports feasibility but not comparative effectiveness, reinforcing that bacteriophage therapy remains investigational rather than a standardized therapeutic alternative.
Despite increasing clinical interest, bacteriophage therapy is constrained by manufacturing challenges, as effective treatment typically requires matching bacteriophages to patient-specific bacterial strains. While this specificity underlies their potential efficacy, it also increases the production time and limits their rapid availability in acute or life-threatening infections. Bacteriophage therapy has primarily been explored as a treatment option for difficult-to-treat infections, including chronic wound and diabetic foot infections [3]. Economic considerations remain underexplored, including the cost-effectiveness of personalized bacteriophage preparation, laboratory infrastructure requirements, and turnaround time relative to acute infection timelines.
Ethical and regulatory frameworks governing compassionate bacteriophage use vary substantially across jurisdictions. Globally, only a limited number of specialized centers currently provide access to clinical bacteriophage therapy [48]. High development costs, limited scalability, and uncertain regulatory pathways have reduced commercial investment in bacteriophage therapeutics. There are also difficulties involving patenting bacteriophage therapies. Available clinical data suggest an acceptable safety profile, although systematic long-term safety data remain limited. Quality control represents a major barrier to widespread adoption [49]. Unlike antibiotics, which follow standardized industrial manufacturing and regulatory pathways, bacteriophage therapy challenges conventional frameworks due to its biological variability and personalized nature [3, 49]. The requirement for strain-specific matching conflicts with batch standardization principles underlying current Good Manufacturing Practice (GMP) systems [49]. This creates a fundamental tension between regulatory expectations for uniformity and the adaptive, patient-specific nature of bacteriophage therapy. As a result, existing regulatory models may be inherently misaligned with bacteriophage therapeutics, necessitating the development of flexible, adaptive approval pathways [3, 48]. The biological nature of bacteriophages complicates batch-to-batch consistency, stability testing, and regulatory classification. The absence of harmonized GMP standards limits reproducibility, regulatory approval, and clinical scalability [49]. Regulatory ambiguity remains a central barrier to clinical integration, as bacteriophage therapies may be classified variably as biological products, personalized medicines, or investigational agents across jurisdictions. This leads to inconsistent regulatory pathways across countries and causes a delay in the approval, unlike antibiotics, which have a standardized clinical framework. Practical usage of bacteriophage therapy is restricted by diagnostic and infrastructural limitations [50–52].
In addition to regulatory and manufacturing challenges, the feasibility of bacteriophage therapy in LMICs remains uncertain. Effective clinical use requires access to rapid microbiological diagnostics, bacteriophage-host matching facilities, and laboratories capable of maintaining curated bacteriophage libraries, resources that are often limited outside specialized centers [48, 50]. The need for individualized bacteriophage selection, quality-controlled production, and compliance with GMP standards further increases cost and infrastructure requirements, potentially restricting availability in resource-constrained settings [49, 52]. Regulatory heterogeneity across countries may also delay approval and limit cross-border sharing of therapeutic bacteriophage preparations. Although regional bacteriophage banks and centralized production facilities have been proposed as potential solutions, their implementation remains limited, and the scalability of bacteriophage therapy in LMICs’ healthcare systems has not yet been established [48].
Currently, there are very few effective treatments for refractory infections; with GMP, we can overcome this barrier. Investment in infrastructure, standardized manufacturing, and curated bacteriophage libraries will be necessary before bacteriophage therapy can be responsibly integrated into routine clinical practice [49]. Collectively, these constraints indicate that current barriers to bacteriophage therapy are predominantly system-level rather than biological.
PAS has emerged as a potential strategy to enhance antibacterial efficacy while limiting resistance development. Experimental studies demonstrate that subinhibitory concentrations of certain antibiotics, particularly β-lactams and fluoroquinolones, can alter bacterial morphology, increase cell elongation, or modify surface receptor expression, thereby facilitating bacteriophage adsorption and increasing bacteriophage replication efficiency [51]. In addition, antibiotic-induced stress responses may enhance bacteriophage burst size and promote bacterial lysis, leading to greater bacterial clearance compared with either agent alone [53, 54].
However, PAS is not universal and depends on pathogen species, antibiotic class, and treatment timing. Sequential administration can influence outcomes, as early antibiotic exposure may reduce bacterial density and limit bacteriophage amplification, whereas bacteriophage-first strategies may increase bacterial susceptibility to antibiotics by selecting for receptor mutations that reduce bacterial fitness or restore antibiotic sensitivity [51, 55]. Conversely, antagonistic interactions have also been reported, particularly with bacteriostatic agents that suppress bacterial metabolic activity and thereby impair bacteriophage replication, highlighting the importance of dosing sequence and pharmacodynamic context [52, 54]. These timing-dependent and pathogen-specific effects contribute to the variable reproducibility of PAS across experimental models and limit direct extrapolation to clinical practice.
Despite strong mechanistic rationale, clinical evidence supporting bacteriophage-antibiotic combinations remains limited and heterogeneous. Most reported applications derive from case reports, compassionate-use programs, or small observational series in MDR or biofilm-associated infections, where bacteriophages are used as adjuncts to ongoing antibiotic therapy [51, 53, 55]. Although potential benefit has been described, interpretation is limited by the absence of comparator arms, individualized bacteriophage selection, and inconsistent outcome definitions.
Translation of PAS into routine practice is further complicated by the lack of standardized protocols for bacteriophage selection, dosing, sequencing, and treatment duration. The optimal timing of antibiotic administration relative to bacteriophage exposure remains uncertain, and synergistic effects observed in vitro are not consistently reproduced in vivo or across different pathogens [52, 54]. In addition, the need for pathogen-specific bacteriophage matching and laboratory susceptibility testing restricts rapid clinical use, particularly in acute infections requiring empiric therapy.
Given these limitations, bacteriophage-antibiotic synergy should be considered a promising but still experimental approach requiring evaluation in controlled trials with standardized endpoints and clearly defined treatment protocols. Integration into antimicrobial stewardship frameworks will be necessary to ensure rational use and to prevent uncontrolled empirical application [51, 54].
Despite increasing biological and clinical interest, the future integration of bacteriophage therapy into mainstream infectious disease practice is constrained by several unresolved knowledge gaps that extend beyond preclinical efficacy and system-level feasibility. One of the most critical limitations is the absence of rigorously designed, standardized clinical trials. The majority of available clinical data are derived from case reports, compassionate-use programs, and small observational series, characterized by substantial heterogeneity in bacteriophage selection, dosing strategies, routes of administration, and outcome definitions [43, 44, 47]. RCT remain scarce, and few studies employ active comparators or clinically meaningful endpoints such as durable cure, relapse, or resistance emergence. Without harmonized trial designs and consensus endpoints, it remains impossible to establish comparative effectiveness, non-inferiority, or optimal clinical indications for bacteriophage therapy relative to antibiotics [31, 56].
A second major gap lies in the limited development of precision-matching frameworks for bacteriophage selection. While bacteriophages are inherently strain-specific, current approaches to bacteriophage-host matching rely largely on labor-intensive in vitro susceptibility testing and curated bacteriophage libraries maintained by specialized centers [44, 48]. Predictive models linking bacterial genotype or phenotype to bacteriophage susceptibility and clinical response are underdeveloped, and standardized algorithms for cocktail design, resistance monitoring, and adaptive bacteriophage substitution are lacking [35, 56]. Advances in rapid pathogen sequencing, machine-learning-assisted bacteriophage selection, and integrated multi-omics approaches hold promise for enabling personalized infectious disease therapy; however, these tools remain largely experimental and unvalidated in prospective clinical studies [35]. Without reliable and scalable precision-matching systems, the individualized nature of bacteriophage therapy will continue to limit reproducibility and broad clinical implementation.
Finally, the role of bacteriophage therapy within antimicrobial stewardship frameworks remains poorly defined. While bacteriophage therapy has theoretical potential to reduce reliance on broad-spectrum antibiotics and mitigate selective pressure for resistance, formal stewardship models incorporating bacteriophage selection, resistance surveillance, ecological impact assessment, and clinical governance have not yet been established [51, 54]. Current clinical use is largely ad hoc, confined to salvage scenarios without standardized oversight, raising concerns regarding inappropriate deployment, resistance amplification, or erosion of stewardship principles. The development of multidisciplinary guidelines integrating microbiology, infectious diseases, regulatory science, and stewardship expertise will be essential to ensure that bacteriophage therapy is used judiciously and complements, rather than undermines, existing antimicrobial strategies [52, 56].
Collectively, these gaps underscore that the primary challenges facing bacteriophage therapy are no longer limited to biological feasibility, but instead lie in the generation of high-quality comparative evidence, the development of scalable precision-matching frameworks, and the establishment of stewardship-integrated clinical pathways. Addressing these domains will be critical to defining whether bacteriophage therapy can transition from experimental salvage intervention to a reproducible and responsibly deployed component of modern infectious disease management.
Antibiotic therapy remains the foundation of modern infectious disease management because of its standardized development pathways, predictable pharmacology, and extensive clinical validation. However, the accelerating burden of AMR, along with reduced efficacy in biofilm-associated and chronic infections and the ecological consequences of broad-spectrum use, exposes fundamental limits to continued reliance on existing antibiotic classes alone. These challenges highlight the need for complementary strategies that extend antibiotic effectiveness rather than attempt to replace it. Bacteriophage therapy represents a mechanistically distinct approach, offering pathogen-specific activity, biological adaptability, and potential efficacy against antibiotic-resistant and biofilm-embedded bacteria. While preclinical studies consistently demonstrate antibacterial activity and early clinical experiences support feasibility in selected refractory infections, the current evidence base remains insufficient for routine clinical adoption. While evidence gaps remain, system-level barriers continue to restrict broader clinical implementation.
Rather than competing modalities, antibiotics and bacteriophage should be viewed as potentially complementary therapies. Their differing mechanisms of action and resistance dynamics create opportunities for rational combination strategies, including bacteriophage-antibiotic synergy, that may enhance treatment efficacy while mitigating resistance. Defining the clinical role of bacteriophage therapy will require standardized trials, regulatory harmonization, and integration within antimicrobial stewardship frameworks.
Ultimately, the clinical adoption of bacteriophage therapy will depend not only on biological efficacy but also on successful integration into standardized regulatory, manufacturing, and stewardship frameworks. Without harmonized trial designs, scalable production models, and stewardship-guided implementation, bacteriophage therapy risks remaining confined to niche, compassionate-use settings rather than achieving widespread clinical adoption.
AMR: antimicrobial resistance
GMP: Good Manufacturing Practice
LMICs: low- and middle-income countries
MDR: multidrug-resistant
PAS: bacteriophage-antibiotic synergy
PK/PD: pharmacokinetic and pharmacodynamic
RCT: randomized controlled trials
RHAR: Conceptualization, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing. DEN: Visualization, Writing—original draft, Writing—review & editing. AWI: Supervision, Validation, Visualization, Writing—review & editing. SIA: Writing—original draft, Writing—review & editing. KMSA: Writing—original draft, Writing—review & editing. ASF: Writing—original draft, Writing—review & editing. MSA: Writing—original draft. MAZ: Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 1336
Download: 17
Times Cited: 0
