 Review
Review

Affiliation:
1College of Osteopathic Medicine, Kansas City University, Kansas City, MO 64804, USA
ORCID: https://orcid.org/0009-0007-2727-8968
Affiliation:
1College of Osteopathic Medicine, Kansas City University, Kansas City, MO 64804, USA
Affiliation:
2Department of Oncology, Mercy Hospital Joplin, Joplin, MO 64804, USA
Email: Samir.dalia@mercy.net
Explor Dig Dis. 2026;5:1005125 DOI: https://doi.org/10.37349/edd.2026.1005125
Received: February 07, 2026 Accepted: April 16, 2026 Published: June 12, 2026
Academic Editor: Jose C. Fernandez-Checa, Institute of Biomedical Research of Barcelona (IIBB), CSIC, Spain
The article belongs to the special issue Helicobacter Pylori and Infection: Genomics, Diagnosis, Pathogenesis, Antibiotic Resistance, Microbiota, Cancer, Prevention and Therapeutics
Gastric mucosa-associated lymphoid tissue (MALT) lymphoma is an indolent extranodal B-cell lymphoma that arises in close association with chronic Helicobacter pylori (H. pylori) infection and represents a unique paradigm of infection-driven oncogenesis. Persistent H. pylori colonization induces organized lymphoid tissue within the normally lymphoid-poor gastric mucosa, promoting sustained antigen-dependent T-cell-mediated B-cell proliferation and eventual clonal transformation. In contrast to many other lymphoid malignancies, early-stage gastric MALT lymphoma often regresses following microbial eradication, highlighting the central role of antigenic stimulation in disease pathogenesis. This review provides a contemporary overview of H. pylori-associated gastric MALT lymphoma, integrating epidemiology, molecular and immunologic mechanisms of lymphomagenesis, diagnostic evaluation, and modern management strategies. This review gives particular attention to molecular determinants of treatment response, including the t(11;18)(q21;q21)/API2-MALT1 translocation and other NF-κB-activating alterations that promote antigen-independent growth and resistance to eradication therapy. Current therapeutic approaches are reviewed, including antibiotic eradication regimens, radiotherapy, immunotherapy, and systemic treatment strategies for refractory or disseminated disease. By integrating mechanistic insights with clinical practice, this review highlights a precision-based framework for the diagnosis, risk stratification, and management of gastric MALT lymphoma in the modern era.
Gastric mucosa-associated lymphoid tissue (MALT) lymphoma represents a distinct subtype of extranodal marginal zone B-cell lymphoma characterized by its strong association with chronic Helicobacter pylori (H. pylori) infection [1]. Since the landmark observation demonstrating regression of gastric lymphoma following eradication of H. pylori, this malignancy has become a paradigm for antigen-driven lymphoid neoplasia and infection-associated carcinogenesis [1, 2].
Under normal physiologic conditions, the gastric mucosa lacks organized lymphoid tissue. However, persistent H. pylori infection induces chronic gastritis characterized by recruitment of T lymphocytes, macrophages, and proliferating B-cells. This inflammatory milieu promotes the formation of ectopic MALT, providing a microenvironment that supports antigen-dependent B-cell expansion [3].
Over time, sustained immune stimulation can result in clonal B-cell populations that ultimately undergo malignant transformation. Importantly, early-stage gastric MALT lymphoma remains dependent on microbial antigen stimulation, explaining why eradication of H. pylori results in durable lymphoma regression in a large proportion of patients [2]. However, genetic alterations may accumulate during disease evolution, enabling tumor cells to proliferate independently of antigenic stimulation and reducing responsiveness to antibiotic therapy [4].
Because of its unique pathogenesis, gastric MALT lymphoma lies at the intersection of infectious disease, immunology, and oncology. From a pathologic perspective, extranodal marginal zone lymphomas of MALT represent a distinct clinicopathologic entity characterized by small B-cell proliferation, lymphoepithelial lesions, and frequent association with chronic inflammatory stimuli [5]. Understanding the interplay between chronic infection, immune signaling, and genetic alterations is essential for guiding clinical management and developing precision-based treatment strategies.
Gastric MALT lymphoma represents one of the most common forms of extranodal marginal zone lymphoma and constitutes a significant proportion of primary gastrointestinal lymphomas [5]. The geographic distribution of disease parallels global patterns of H. pylori infection, with higher incidence observed in East Asia, Southern Europe, and parts of Latin America [6].
The median age at diagnosis ranges from 50 to 60 years, with a slight female predominance reported in several epidemiologic studies [7]. Risk factors include chronic H. pylori infection, host genetic susceptibility, and bacterial virulence factors such as cytotoxin-associated gene A (CagA) positivity and downstream oncogenic signaling pathways [8, 9].
Clinical presentation is often nonspecific. Patients frequently report dyspepsia, epigastric discomfort, nausea, or early satiety [7]. Less commonly, gastrointestinal bleeding, anemia, or weight loss may occur in advanced disease. Because symptoms overlap with those of chronic gastritis and peptic ulcer disease, many cases are diagnosed incidentally during upper endoscopy performed for evaluation of persistent gastrointestinal symptoms.
Under normal physiologic conditions, the gastric mucosa lacks organized lymphoid tissue. Chronic H. pylori infection induces persistent gastric inflammation characterized by infiltration of CD4+ T-cells, macrophages, and B lymphocytes. These immune cells organize into lymphoid follicles resembling Peyer’s patches, creating ectopic MALT within the gastric mucosa [9].
These structures provide a specialized microenvironment that facilitates antigen presentation and T-cell-dependent B-cell activation. Cytokines and co-stimulatory interactions—including CD40-CD40L signaling—promote proliferation and survival of antigen-specific B-cells, establishing the conditions necessary for clonal expansion.
Early gastric MALT lymphomas demonstrate strong dependence on H. pylori-specific T-cell help. Experimental studies show that lymphoma B-cells proliferate only in the presence of activated T-cells recognizing H. pylori antigens [10]. This antigen-dependent growth explains the remarkable responsiveness of early-stage disease to bacterial eradication therapy.
With disease progression, recurrent chromosomal translocations may arise, enabling tumor cells to proliferate independently of microbial antigen stimulation. The most common abnormality is the t(11;18)(q21;q21) translocation, which produces the apoptosis inhibitor 2 (API2)-MALT1 fusion protein and constitutively activates the nuclear factor kappa B (NF-κB) signaling pathway [6].
Additional genetic alterations—including t(1;14)(p22;q32), t(14;18)(q32;q21), and trisomy 3—have been consistently reported in genomic studies of gastric MALT lymphoma and converge mechanistically on constitutive NF-κB activation and enhanced B-cell survival signaling pathways [11, 12]. These molecular events represent a transition from immune-driven lymphoproliferation to genetically stabilized malignancy.
In addition to API2-MALT1 fusion-mediated NF-κB activation, several additional mechanisms contribute to the progressive evolution from antigen dependence to genetic autonomy. Chronic inflammatory signaling promotes activation of B-cell receptor (BCR) signaling pathways, Toll-like receptor stimulation, and cytokine-mediated survival pathways that collectively sustain lymphoma cell proliferation. Over time, recurrent abnormalities involving B-cell lymphoma/leukemia 10 (BCL10), MALT1, and TNFAIP3 further amplify NF-κB signaling, establishing constitutive activation independent of microbial antigen stimulation. This microenvironmental evolution reflects a transition from immune-driven lymphoproliferation to genetically stabilized malignancy and represents a critical step in disease progression.
The most clinically relevant molecular abnormalities identified in gastric MALT lymphoma, along with their prognostic and therapeutic implications, are summarized in Table 1.
Recurrent molecular abnormalities in gastric MALT lymphoma and associated clinical implications.
| Molecular abnormality | Approximate frequency | Key biologic effect | Response to eradication | Clinical implication |
|---|---|---|---|---|
| t(11;18)(q21;q21)/API2-MALT1 | ~20–30% | Constitutive NF-κB activation | Poor response/resistance | Early consideration of radiotherapy or systemic therapy |
| t(1;14)(p22;q32) | < 5% | BCL10 overexpression | Reduced response | Likely antigen-independent growth |
| t(14;18)(q32;q21) | Rare | MALT1 activation | Variable | Potential need for non-antibiotic therapy |
| Trisomy 3 | ~10–15% | Increased B-cell survival | Intermediate | Close surveillance eradication |
This table summarizes the most frequently reported molecular alterations in gastric MALT lymphoma, their approximate prevalence, underlying biologic effects, predicted response to Helicobacter pylori eradication therapy, and resulting therapeutic considerations. Frequencies are approximate and vary across published cohorts; molecular testing is most commonly performed using fluorescence in situ hybridization. API2: apoptosis inhibitor 2; BCL10: B-cell lymphoma/leukemia 10; MALT: mucosa-associated lymphoid tissue; NF-κB: nuclear factor kappa B.
Upper gastrointestinal endoscopy with multiple biopsies remains the cornerstone of diagnosis. Endoscopic findings are variable and may include erythema, nodularity, mucosal thickening, erosions, or ulceration.
Histopathologic examination typically reveals dense lymphoid infiltrates in the lamina propria, lymphoepithelial lesions, and centrocyte-like cells. Immunophenotyping demonstrates expression of CD20 and B-cell markers with the absence of CD5, CD10, and cyclin D1 [12].
Molecular testing using fluorescence in situ hybridization (FISH) is often performed to detect the API2-MALT1 translocation, particularly in patients with advanced disease or those who fail eradication therapy.
The recommended diagnostic workup for suspected gastric MALT lymphoma is summarized in Table 2.
Diagnostic evaluation of suspected gastric MALT lymphoma.
| Diagnostic test | Clinical purpose |
|---|---|
| Upper gastrointestinal endoscopy with multiple biopsies | Primary diagnostic procedure used to identify suspicious gastric lesions and obtain tissue for histologic analysis |
| Histopathologic examination | Confirms lymphoma by demonstrating lymphoepithelial lesions and dense B-cell infiltrates in the gastric mucosa |
| Immunohistochemistry (CD20, CD5, CD10, cyclin D1) | Defines B-cell phenotype and helps differentiate MALT lymphoma from other lymphoid malignancies |
| Fluorescence in situ hybridization (FISH) | Detects chromosomal translocations such as t(11;18)(q21;q21)/API2-MALT1 |
| Cross-sectional imaging (CT or PET/CT) | Evaluates disease extent and identifies nodal or extranodal involvement |
This table shows that the diagnostic evaluation of gastric MALT lymphoma requires integration of endoscopic, histopathologic, immunophenotypic, and molecular testing. These modalities collectively establish the diagnosis, evaluate disease stage, and guide treatment decisions. MALT: mucosa-associated lymphoid tissue.
First-line treatment consists of H. pylori eradication therapy using proton pump inhibitor-based multidrug regimens. Standard approaches include clarithromycin-based triple therapy, bismuth-based quadruple therapy, and alternative regimens such as sequential therapy, concomitant therapy, or levofloxacin-containing salvage regimens, depending on regional antibiotic resistance patterns [13]. These regimens are typically administered for 10–14 days and achieve bacterial eradication in the majority of patients [13].
Following successful eradication, complete histologic remission occurs in approximately 70–80% of patients with stage I gastric MALT lymphoma, although lymphoma regression may be delayed for up to 12–18 months [14–16]. Consequently, careful endoscopic surveillance is recommended before initiating additional oncologic therapy.
Patients with persistent disease following eradication therapy or those harboring the API2-MALT1 translocation frequently require oncologic treatment.
Involved-site radiotherapy is an effective treatment option for patients with localized gastric MALT lymphoma who do not achieve remission following H. pylori eradication therapy [17]. Testing for the t(11;18)(q21;q21)/API2-MALT1 translocation is increasingly incorporated into diagnostic workflows because its presence predicts reduced responsiveness to H. pylori eradication therapy and supports earlier consideration of radiotherapy or systemic treatment [17].
Systemic therapy is generally reserved for disseminated or relapsed disease. Treatment options include rituximab monotherapy or rituximab-based chemoimmunotherapy regimens such as rituximab plus chlorambucil or bendamustine [18]. Systemic therapies, including immunotherapy and chemoimmunotherapy regimens, may be considered for patients with relapsed, refractory, or disseminated marginal zone lymphoma when local therapies are insufficient [19].
Long-term outcomes for gastric MALT lymphoma are generally favorable. Five-year overall survival exceeds 90% in most contemporary cohorts treated with eradication therapy and risk-adapted oncologic approaches [20]. Despite excellent outcomes, long-term surveillance remains essential because patients remain at risk for disease relapse and secondary gastric adenocarcinoma [21]. Current guidelines recommend periodic endoscopic evaluation with mapping biopsies following treatment.
Reported remission rates associated with commonly used treatment modalities for gastric MALT lymphoma are illustrated in Figure 1.
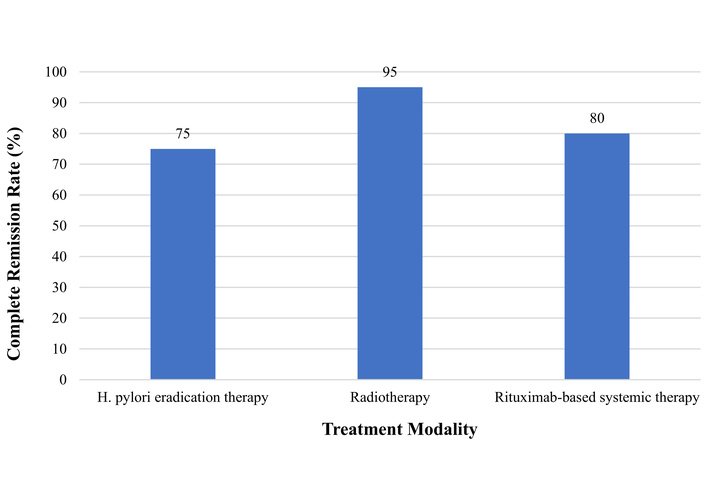
Treatment outcomes in gastric mucosa-associated lymphoid tissue (MALT) lymphoma. The figure shows the reported remission rates associated with commonly used treatment modalities for gastric MALT lymphoma. Eradication of Helicobacter pylori (H. pylori) induces complete histologic remission in the majority of early-stage cases, while radiotherapy achieves excellent local control in eradication-refractory disease. Systemic therapies such as rituximab-based regimens are typically reserved for disseminated or relapsed lymphoma.
Gastric MALT lymphoma occupies a unique position at the intersection of chronic infection, immune dysregulation, and oncogenesis, distinguishing it from most other lymphoid malignancies. Unlike genetically driven high-grade lymphomas, gastric MALT lymphoma often represents a biologically reversible disease process in its early stages, provided that the underlying antigenic stimulus is effectively eliminated [22, 23]. This feature has profound implications for both clinical management and our broader understanding of tumor–microenvironment interactions.
Gastric MALT lymphoma represents a unique model of infection-associated carcinogenesis in which chronic microbial antigen stimulation drives lymphoid proliferation and malignant transformation [13]. These pathogen-associated immune mechanisms highlight the broader role of chronic antigenic stimulation in the development of marginal zone lymphomas, including gastric MALT lymphoma [17]. Unlike most malignancies that arise primarily from intrinsic genetic instability, early gastric MALT lymphoma remains dependent on microenvironmental signals derived from H. pylori-specific immune responses [18, 24]. This antigen-dependent phase of lymphomagenesis is closely linked to chronic H. pylori-driven immune activation within the gastric mucosa, which promotes persistent lymphoid stimulation and contributes to the development of gastric MALT lymphoma [25, 26].
Over time, selective pressures favor the acquisition of genetic alterations that confer antigen independence. The transition toward antigen-independent growth is further supported by dysregulated BCR signaling pathways that promote lymphoma cell survival and proliferation in marginal zone lymphoma [27]. Recent experimental studies demonstrate that progressive genetic evolution within the tumor microenvironment facilitates a transition from antigen-dependent to antigen-independent growth. Activation of the NF-κB signaling pathway—most commonly through the API2-MALT1 fusion protein—promotes constitutive B-cell survival signaling, thereby enabling lymphoma progression even after microbial eradication [6, 12].
Therapeutically, gastric MALT lymphoma illustrates fundamental principles of indolent lymphoma biology, including radiosensitivity, immune responsiveness, and prolonged disease control despite minimal cytotoxic intervention. The efficacy of localized radiation and immunotherapy in later disease stages highlights the continued relevance of immune-targeted strategies even after antigen independence has emerged [19, 20]. These clinical characteristics reflect the indolent biology of gastrointestinal MALT lymphomas, which typically demonstrate favorable responses to localized therapies and prolonged disease control when treated with risk-adapted strategies [18, 24].
Beyond lymphoma control, long-term disease biology is shaped by persistent mucosal inflammation and epithelial remodeling within the chronically infected gastric mucosa, reflecting the broader inflammatory microenvironment that characterizes gastric MALT lymphoma [8, 11]. This shared inflammatory milieu suggests overlapping pathogenic pathways between lymphoid and epithelial neoplasia within the chronically infected stomach.
Advances in molecular diagnostics and immune profiling are expected to further refine biologic risk stratification. Large-scale genomic studies have revealed substantial molecular heterogeneity within marginal zone lymphomas, including mutations in genes regulating chromatin remodeling, immune signaling, and BCR pathways, further underscoring the complexity of disease pathogenesis [19, 26]. Recent advances in molecular diagnostics are improving our understanding of disease heterogeneity. Emerging approaches—including next-generation sequencing and circulating tumor DNA analysis—may enable earlier detection of molecular resistance mechanisms and facilitate more personalized treatment strategies [23].
The clinical management of H. pylori-associated gastric MALT lymphoma requires a coordinated multidisciplinary approach involving gastroenterologists, pathologists, and oncologists. Clinicians should maintain a high index of suspicion in patients presenting with persistent dyspeptic symptoms, atypical gastric lesions, or treatment-refractory gastritis, particularly in regions with high H. pylori prevalence. Early recognition is critical because timely eradication of H. pylori can induce durable lymphoma regression and may eliminate the need for oncologic therapy in many patients. Multiple clinical series have confirmed that antibiotic eradication therapy alone can achieve complete remission in a substantial proportion of patients with early-stage gastric MALT lymphoma, emphasizing the importance of identifying infection-driven disease prior to initiating oncologic therapy [24].
Comprehensive diagnostic evaluation should extend beyond histopathologic confirmation to include molecular testing—particularly assessment for API2-MALT1 translocation—given its strong association with resistance to antibiotic eradication and implications for treatment selection. Following eradication therapy, clinicians should anticipate delayed histologic responses and avoid premature escalation of treatment in the absence of clinical or endoscopic progression, as persistent lymphoid infiltrates may reflect immune remodeling rather than treatment failure [16, 19].
Structured post-treatment surveillance is critical and should incorporate serial endoscopy with mapping biopsies rather than reliance on a single response modality. For patients with eradication-refractory disease or molecular predictors of antigen independence, early referral for involved-site radiotherapy provides highly effective local disease control with minimal long-term toxicity. Systemic therapies, including rituximab-based regimens, should be reserved for disseminated or relapsed disease.
Importantly, even after successful lymphoma regression, patients require lifelong endoscopic surveillance due to the persistent risk of relapse and secondary gastric adenocarcinoma. This necessity reinforces the concept of gastric MALT lymphoma as a chronic, inflammation-associated disease process rather than a discrete oncologic event, underscoring the importance of coordinated longitudinal care.
Gastric MALT lymphoma represents a distinctive model of infection-driven oncogenesis in which chronic microbial antigen stimulation drives lymphoid proliferation and malignant transformation. Eradication of H. pylori remains the cornerstone of therapy for early-stage disease, while molecular alterations such as the API2-MALT1 translocation identify patients more likely to require radiotherapy or systemic treatment. Advances in molecular diagnostics and immune profiling are improving risk stratification and enabling more individualized therapeutic approaches. Continued integration of molecular biomarkers with clinical management strategies will further refine precision-based care for patients with gastric MALT lymphoma. Contemporary international guidelines increasingly emphasize risk-adapted management strategies that integrate molecular findings, stage-specific therapy, and long-term surveillance to optimize outcomes for patients with marginal zone lymphoma [28, 29].
API2: apoptosis inhibitor 2
BCR: B-cell receptor
FISH: fluorescence in situ hybridization
MALT: mucosa-associated lymphoid tissue
NF-κB: nuclear factor kappa B
The authors thank the Department of Hematology and Oncology at Mercy Hospital Joplin for academic support.
VK: Conceptualization, Writing—original draft, Writing—review & editing. JNP: Conceptualization, Writing—original draft, Writing—review & editing. SMD: Supervision, Conceptualization, Writing—review & editing. All authors read and approved the final manuscript.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 1138
Download: 21
Times Cited: 0
Luiza Gilmanovna Bektemirova ... Vasiliy Ivanovich Reshetnyak
Elias Kouroumalis ... Argyro Voumvouraki
Rosabel Corrales ... Rafael Llanes
Natalia V. Baryshnikova ... Alexander N. Suvorov
Tatyana Anatolievna Kuchmenko ... Arina Kopaeva
Surbhi Dumra, Abhishek Ray
Sophia Strukel ... Vikrant Rai
