Case Report
Case Report

Affiliation:
Cardiology Department, ZhongDa Hospital of Southeast University, Nanjing 210009, Jiangsu, China
Email: L1991ZY@163.com
ORCID: https://orcid.org/0000-0001-5300-7052
Affiliation:
Cardiology Department, ZhongDa Hospital of Southeast University, Nanjing 210009, Jiangsu, China
Explor Cardiol. 2025;3:101277 DOI: https://doi.org/10.37349/ec.2025.101277
Received: August 16, 2025 Accepted: September 15, 2025 Published: October 23, 2025
Academic Editor: Albert Varga, University of Szeged, Hungary
The diagnosis of acute myocarditis requires the exclusion of coronary artery disease (CAD). Coronary CTA (computed tomography angiography) is usually used to evaluate the coronary arteries in young patients. However, the use of coronary CTA for the diagnosis of myocarditis has been rarely reported. Here we present a Han male clinical myocarditis patient who was 18 years old, had a focus of enhancement in the subcardia, and predominantly involving the lateral wall of the left ventricle with iodinated contrast in coronary CTA. The patient was diagnosed with myocarditis. Immunoglobulin, vitamin C antioxidant, and myocardial nutrition were given to the patient for treatment. During follow-up, the patient’s myocardial enzymes gradually decreased to normal, and the original symptoms disappeared. As a non-invasive rapid examination method that can evaluate coronary artery and myocardial lesions at the same time, the utility of myocardial delayed enhancement on CTA may warrant further investigation.
The diagnosis of acute myocarditis should be made by exclusion of coronary artery disease (CAD). Coronary computed tomography angiography (CTA) is usually used to evaluate the coronary arteries in young patients. Delayed enhancement detection of myocardium in coronary CTA can also evaluate myocardial lesions [1, 2]. However, the application of coronary CTA in the diagnosis of myocarditis is rarely reported.
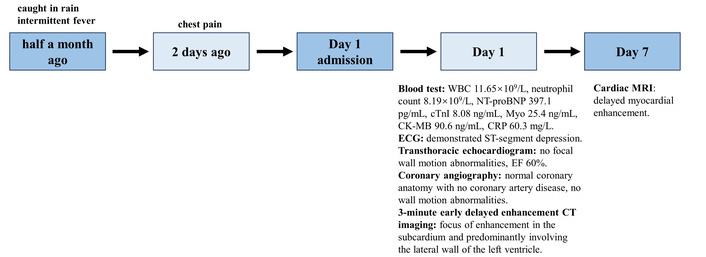
An 18-year-old man was hospitalized due to intermittent fever for half a month and chest pain for 2 days. The patient had a fever half a month ago after being caught in the rain, with a maximum temperature of 40°C. After taking antipyretics, the body temperature could return to normal. Five days ago, the patient suffered a fever again, with a maximum temperature of 40°C, accompanied by a sore throat, cough, and expectoration. Two days ago, the patient experienced chest pain (timeline in Figure 1).
Full blood count: WBC 11.65 × 109/L, neutrophil count 8.19 × 109/L, NT-proBNP 397.1 pg/mL, cTnI 8.08 ng/mL, Myo 25.4 ng/mL, CK-MB 90.6 ng/mL, CRP 60.3 mg/L. ECG demonstrated ST-segment depression. A transthoracic echocardiogram performed 1 day after admission showed no focal wall motion abnormalities and a normal ejection fraction of 60%. CT coronary angiography performed on the same day showed normal coronary anatomy with no CAD, no wall motion abnormalities. Three-minute early delayed enhancement CT imaging demonstrated a focus of enhancement in the subcardia and predominantly involving the lateral wall of the left ventricle (Figure 2). A subsequent cardiac MRI performed 7 days later showed delayed myocardial enhancement seen on the CTA. After resolution of his symptoms and normalization of his cardiac enzymes and function, the patient was discharged home on day 7 with the presumptive diagnosis of viral myopericarditis.
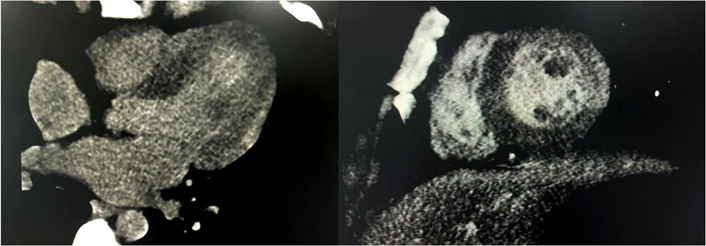
Three-minute early delayed enhancement CT imaging demonstrated a focus of enhancement in the subcardia and predominantly involving the lateral wall of the left ventricle.
Myocarditis is a serious and life-threatening disease that may be caused by viral, bacterial, autoimmune reactions, or other etiologies. Myocarditis needs to be distinguished from acute coronary syndrome and other cardiomyopathies. At present, diagnosis is made by combining clinical manifestations, serum cardiac biomarkers, and echocardiography, and myocardial biopsy remains the gold standard. Myocardial biopsy can determine the cause of myocarditis and also the type of inflammation based on the biopsy results, and eventually guide further treatment [1, 2]. But it is an invasive procedure with a false negative rate.
CTA is a non-invasive examination method that can perform multi-modal imaging, including static imaging, dynamic imaging, and enhanced scanning. Static imaging can provide static anatomical information of the heart and coronary artery, while dynamic imaging can observe the movement and function of the heart. Delayed myocardial enhancement of CTA can be used to detect and evaluate myocardial infarction, myocardial activity, and fibrosis [3]. MRI has excellent soft tissue resolution and can detect areas of late gadolinium enhancement (LGE) and diagnose myocardium. However, cardiac magnetic resonance (CMR) is limited in clinical application due to its long scanning time and contraindications [4].
Similarly, both CT iodine contrast agent and MR gadolinium-based contrast agent are extracellular space contrast agents, with almost the same pharmacological effects. Based on iodine-based myocardial CT with late iodine enhancement-CT (LIE-CT) and LGE-MRI, they share the same pathological and physiological principles. Previous studies have shown that at the segmental level, the correlation between CTA and CMR delayed enhancement in diagnosing myocarditis is 0.90 [5]. The delayed enhancement site of acute myocarditis is mostly epicardial or transmural, and can also be patchy, which is different from the delayed enhancement manifestation of myocardial infarction [6, 7]. All of these expand the clinical application scope of CTA, which is no longer limited to the anatomical diagnosis of coronary artery-related diseases, and make it possible to diagnose myocarditis. In hospitals without emergency CMR or a lack of ability to perform MRI timely, CTA delayed contrast-enhanced scanning is more convenient and faster to diagnose myocarditis. On the other hand, in emergency settings, acute myocarditis is often misdiagnosed as acute myocardial infarction, prompting urgent coronary angiography, while coronary CTA is rarely performed. CTA is considered an alternative option in selected situations.
The patient in this case has a focus of enhancement in the subcardia and predominantly involving the lateral wall of the left ventricle. Based on the patient’s medical history, laboratory tests, echocardiography, and CTA, the final diagnosis was acute myocarditis. So, immunoglobulin, vitamin C antioxidant, and myocardial nutrition were given to the patient for treatment. After treatment, the patient’s myocardial enzymes gradually decreased to normal, and the original symptoms disappeared.
In hospitals without emergency CMR or CMR examination, CTA delayed contrast-enhanced scanning is more convenient and faster, providing a timely and accurate basis for the diagnosis of myocarditis.
CAD: cardiovascular disease
CMR: cardiac magnetic resonance
CTA: computed tomography angiography
LGE: late gadolinium enhancement
ZL: Conceptualization, Funding acquisition, Resources, Supervision, Writing—original draft, Writing—review & editing. YW: Conceptualization, Methodology, Formal analysis. Both authors read and approved the submitted version.
The authors declare that there are no conflicts of interest.
The study complies with the Declaration of Helsinki (2024 version). This study was approved by the Ethics Committee of ZhongDa Hospital of Southeast University (2018ZDSYLL134-P01).
Informed consent to participate in the study was obtained from the participant.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
The data of this manuscript could be available from the corresponding authors upon reasonable request.
This work was supported by the Natural Science Foundation of Jiangsu Province [BK20190352] and the National Natural Science Foundation of China [82302875], from Zhuyuan Liu, the corresponding author. The funder(s) had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 2460
Download: 158
Times Cited: 0