Original Article
Original Article

Affiliation:
Department of Pharmaceutical Health Outcomes and Policy, College of Pharmacy, University of Houston, Houston, TX 77204, United States
ORCID: https://orcid.org/0000-0003-2134-2221
Affiliation:
Department of Pharmaceutical Health Outcomes and Policy, College of Pharmacy, University of Houston, Houston, TX 77204, United States
ORCID: https://orcid.org/0000-0002-1270-0747
Affiliation:
Department of Pharmaceutical Health Outcomes and Policy, College of Pharmacy, University of Houston, Houston, TX 77204, United States
ORCID: https://orcid.org/0009-0007-5857-0443
Affiliation:
Department of Pharmaceutical Health Outcomes and Policy, College of Pharmacy, University of Houston, Houston, TX 77204, United States
Email: smabugho@CougarNet.UH.EDU
ORCID: https://orcid.org/0000-0002-8779-8523
Explor Cardiol. 2026;4:1012110 DOI: https://doi.org/10.37349/ec.2026.1012110
Received: February 12, 2026 Accepted: April 08, 2026 Published: June 09, 2026
Academic Editor: Carmine Gazzaruso, University of Milan, Italy
Aim: Older adults with dyslipidemia often have coexisting diabetes and hypertension, requiring triple therapy with statins, antihypertensives, and oral antidiabetics. Given that statin adherence is a key metric in the Medicare STAR Ratings program, understanding statin use in this population is critical. However, prior studies have focused on adherence to statin monotherapy or composite adherence to triple therapy, with limited evidence on statin-specific patterns in this population.
Methods: We conducted a retrospective cohort study using a Texas-based Medicare Advantage database (2016–2017). Adults receiving concurrent triple therapy (statins, renin-angiotensin system antagonists, and oral antidiabetics) were followed for 12 months. Statin adherence was measured monthly using the proportion of days covered (PDC) and modeled using group-based trajectory modeling (GBTM). Multinomial logistic regression, informed by the Andersen behavioral model, was used to identify sociodemographic and clinical predictors of adherence trajectories.
Results: Among 7,847 patients, three distinct statin adherence trajectories were identified: near-perfect adherence (57.0%), adherent (23.6%), and rapid decline (19.4%). Female sex was associated with higher odds of rapid decline than male sex. Younger age (≤ 65 years) and having at least one prior hospitalization were significant predictors of rapid adherence decline, whereas older age and a greater number of concomitant medications were associated with lower odds of decline. Notably, about 80% of patients were adherent to statin despite lower adherence to the overall triple-therapy regimen.
Conclusions: This study identified three distinct statin adherence trajectories among older adults on triple therapy. By highlighting predictors of rapid adherence decline, including female sex and prior hospitalization, these findings can help clinicians identify high-risk patients and inform targeted interventions to improve adherence and cardiovascular outcomes.
Cardiovascular disease (CVD), including atherosclerotic CVD (ASCVD), remains the leading cause of death in the United States and globally [1]. The burden of ASCVD is largely driven by dyslipidemia, with elevated low-density lipoprotein cholesterol (LDL-C) recognized as a major and modifiable causal determinant of ASCVD [2, 3].
The cornerstone pharmacological treatment for dyslipidemia is statin therapy (3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors) [4]. Statins are the most commonly prescribed lipid-lowering medications and significantly reduce CV events and mortality among patients with ASCVD [4, 5]. These benefits informed guideline recommendations, including the 2013 American College of Cardiology/American Heart Association endorsement of high-intensity statin therapy [6]. Despite increased prescribing [7], high-intensity statin use remained suboptimal by 2017, with only 30–50% of eligible patients treated [8–10].
The clinical effectiveness of statins depends heavily on adherence; however, nonadherence to chronic medications remains common and is associated with poor outcomes and substantial healthcare costs [11]. This challenge is particularly relevant among older adults with ASCVD, who often require multiple concurrent medications for comorbid diabetes and hypertension [12]. Studies indicate that medication nonadherence among older adults ranges from 25% to 74%, while statin discontinuation rates following myocardial infarction may reach 15.4% within six months [13]. Poor adherence to lipid-lowering therapy is associated with increased hospitalizations, recurrent myocardial infarction, and mortality [13, 14].
Traditional adherence measures, such as proportion of days covered (PDC), provide limited insight into longitudinal adherence behavior [15]. Group-based trajectory modeling (GBTM) has emerged as a more informative approach by identifying distinct adherence patterns over time [16, 17]. A previous study by Cheruvu et al. [18] applied GBTM to this high-risk population to evaluate adherence patterns to the composite outcome of concomitant triple therapy [defined as the simultaneous use of oral antidiabetics, renin-angiotensin system (RAS) antagonists, and statins], identifying four distinct trajectories. Given evidence linking statin adherence with CV risk-factor control and its inclusion in Medicare STAR quality measures, evaluating statin-specific adherence trajectories in patients with comorbid hypertension and diabetes is warranted [19].
Building on this prior work, this study used GBTM to characterize statin adherence patterns among adults receiving concurrent triple therapy in a Medicare Advantage population and to examine their clinical and sociodemographic predictors in comparison with composite regimen adherence.
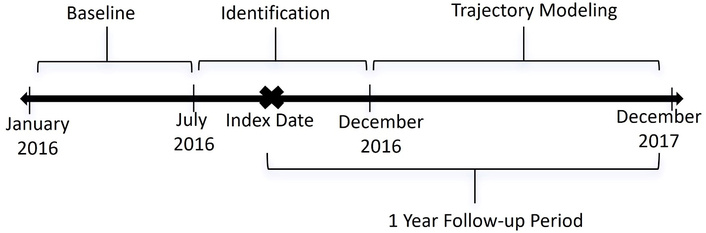
This study employed a longitudinal, retrospective cohort design, analyzing data from a Texas-based Medicare Advantage database spanning January 2016 through December 2017 (Figure 1). The database provided comprehensive patient records organized across several electronic files, including demographic and Centers for Medicare & Medicaid Services (CMS) risk score information (member summary), clinical utilization data [institutional and professional claims containing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes, admission, and discharge dates], and detailed prescription records (pharmacy files, including fill dates, supply duration, and dosing).
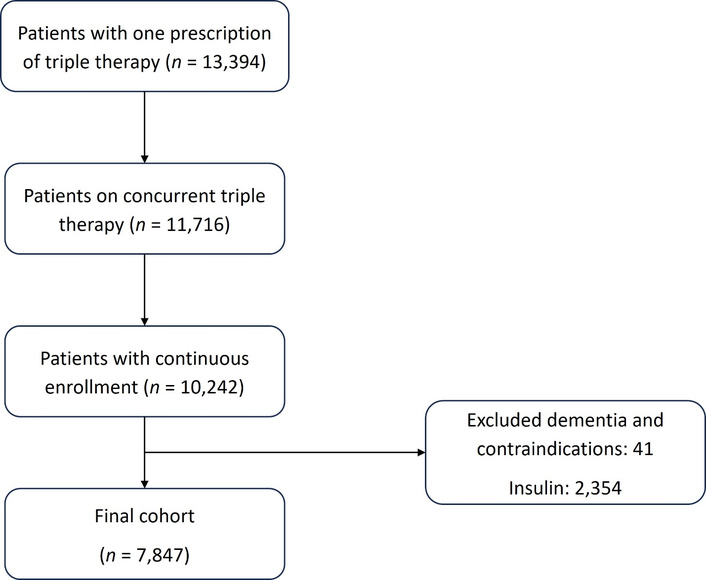
The cohort consisted of adults enrolled in the Medicare Advantage plan. Patients were selected based on continuous enrollment throughout the study period (January 2016 to December 2017) and confirmed use of concurrent triple therapy (Figure 1). Concurrent triple therapy was defined as having at least one prescription each of an oral antidiabetic, a statin, and a RAS antagonist during a 6-month index period (July 2016 to December 2016). The antidiabetic classes included in the study are biguanides, dipeptidyl peptidase-4 inhibitors, meglitinides, sodium-glucose cotransporter 2 inhibitors, sulphonylureas, and thiazolidinediones. Antihypertensives included RAS antagonists. The drug classes included for RAS antagonists in the study were angiotensin converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), and direct renin inhibitors. Lipid-lowering drug classes included in the study were statins. Crucially, these drug classes constitute the core adherence quality measures utilized in the Medicare STAR rating program for Medicare Advantage plans. The study required an overlap of at least one month of all three medication classes within the index period, with continuation indicated by a second prescription for each component after the index date. A 6-month period preceding the index date was designated as the baseline period for identifying predictor variables. The 12-month follow-up period for adherence measurement commenced immediately after the index date. Exclusion criteria were applied to enhance cohort homogeneity and prevent confounding. Patients with a diagnosis of dementia or any insulin use during the study period were excluded. Furthermore, patients with baseline contraindications to either ACEIs/ARBs (e.g., angioedema, hyperkalemia, renal artery stenosis) or a documented history of myopathy indicative of statin intolerance during the baseline period were excluded (Figure 2).
Statin medication adherence was the primary outcome of interest and was quantified using the PDC over the 12-month follow-up. PDC was calculated monthly (number of days supplied/the total number of days in the analysis period). Monthly binary indicators of full statin adherence were generated, defined as a PDC ≥ 0.8 (i.e., ≥ 24 days of supply per month) versus non-adherence. These twelve-monthly binary indicators were then analyzed using logistic GBTM, a latent variable modeling technique, to empirically map distinct, dynamic patterns of statin adherence over the one-year period.
The optimal number of trajectory groups was determined by evaluating the Bayesian information criterion (BIC), with the model demonstrating the smallest BIC chosen as the best fit for the data, using the second-order polynomial function of time [16]. Model selection was further supported using the logged Bayes factor, approximated by 2*ΔBIC. Throughout the selection process, clinical interpretability and a minimum 5% group membership requirement were maintained.
The accuracy and robustness of the final GBTM solution were assessed using established methodological criteria recommended by Nagin and Odgers [16]. The model’s performance was validated against the following: (1) an average group posterior probability of at least 0.7 for all identified trajectories; (2) the odds of correct classification exceeding 5 for all groups; and (3) minimal divergence between the estimated group probability (π) and the actual proportion of individuals assigned to the group (P). Model validation confirms that the identified trajectories are accurate, generalizable, and robust, thereby enhancing the reliability of the findings and their applicability in real-world settings (Table S1). Individuals were definitively assigned to the trajectory group for which they possessed the highest posterior probability of membership.
The selection of all baseline predictor variables was systematically informed by the Anderson behavioral model, which is widely utilized to understand health care utilization and behavioral patterns [20]. This framework organizes factors influencing adherence into three fundamental domains, determined during the baseline period.
The first domain, predisposing factors, describes the patient’s propensity to use health services. These included age (categorized as ≤ 65, 66–69, 70–74, and ≥ 75 years), sex, the total number of other medications, and regimen complexity. Regimen complexity was quantitatively defined as the mean doses taken per day multiplied by the total number of unique medications. This calculation captures the primary weighted components of the Medication Regimen Complexity Index (MRCI), including dosing frequency and medication count, as validated by George et al. [21], and maintains methodological consistency with our previously published analysis of this cohort [18]. The second domain, enabling factors, encompasses the resources available to patients. This was primarily assessed by health plan status, specifically the presence or absence of a low-income subsidy (LIS), which acts as a proxy for financial access and assistance. The final domain, need factors, reflects the perceived or objective illness level. This included baseline comorbidities such as a diagnosis of depression, the patient’s history of CV events (e.g., myocardial infarction, stroke), the number of prior hospitalizations (≥ 1 vs. none), and the CMS risk score, which is used to account for the overall medication burden and disease severity. The baseline comorbid conditions were identified using ICD-10-CM codes.
Descriptive statistics were used to summarize the clinical and demographic characteristics of the overall cohort. Bivariate analysis, utilizing Chi-square tests (categorical variables) and analysis of variance (ANOVA, continuous variables), was performed to assess differences in patient characteristics across the identified statin adherence trajectory groups.
The predictors of statin adherence patterns were identified using multinomial logistic regression. The outcome variable for this model was the final assigned statin adherence trajectory group, with the adherence group selected as the reference category. Predictor variables were included based on the Anderson behavioral model. Prior to modeling, a correlation assessment was performed among the independent variables. All statistical analyses were conducted using SAS version 9.4 (SAS Institute), with a significance level set at p < 0.05. The Institutional Review Board (IRB) at the University of Houston granted approval for this study.
Table 1 presents the baseline characteristics of 7,847 patients stratified by adherence trajectory. Overall, 52.5% of the participants were female, and those between the ages of 66–69 had the highest percentage (35%). Sex distribution varied significantly across groups (p < 0.0001), with females more likely to be in the rapid decline (56.0%) compared with the adherent group (49.2%). Age also differed significantly (p = 0.0397), as younger patients (≤ 65 years) were more represented in the rapid decline group, while those aged 70–74 years were more common among adherent patients. The mean CMS risk score differed across adherence trajectories (p = 0.0065), being lowest in the rapid decline group (mean = 1.24 ± 0.74).
Patient demographics and clinical characteristics (n = 7,847).
| Variables | Total patients (n = 7,847) | Rapid decline (n = 1,400) | Near-perfect adherent (n = 3,713) | Adherent (n = 2,734) | p-value |
|---|---|---|---|---|---|
| Sex | < 0.0001* | ||||
| Male | 3,728 (47.5%) | 616 (44.0%) | 1,722 (46.4%) | 1,390 (50.8%) | |
| Female | 4,119 (52.5%) | 784 (56.0%) | 1,991 (53.6%) | 1,344 (49.2%) | |
| Age, years | 0.0397* | ||||
| ≤ 65 | 1,021 (13.0%) | 205 (14.6%) | 481 (13.0%) | 335 (12.3%) | |
| 66–69 | 2,747 (35.0%) | 521 (37.2%) | 1,273 (34.3%) | 953 (34.9%) | |
| 70–74 | 2,127 (27.1%) | 337 (24.1%) | 1,021 (27.5%) | 769 (28.1%) | |
| ≥ 75 | 1,952 (24.9%) | 337 (24.1%) | 938 (25.3%) | 677 (24.8%) | |
| Health plan | 0.3548 | ||||
| No subsidy | 4,153 (52.9%) | 756 (54.0%) | 1,934 (52.1%) | 1,463 (53.5%) | |
| Low-income subsidy | 3,694 (47.1%) | 644 (46.0%) | 1,779 (47.9%) | 1,271 (46.5%) | |
| No. of prior hospitalizations | 0.1112 | ||||
| 0 | 7,560 (96.3%) | 1,336 (95.4%) | 3,589 (96.7%) | 2,635 (96.4%) | |
| ≥ 1 | 287 (3.7%) | 64 (4.6%) | 124 (3.3%) | 99 (3.6%) | |
| Depression | 0.1202 | ||||
| No | 7,826 (99.7%) | 1,396 (99.7%) | 3,699 (99.6%) | 2,731 (99.9%) | |
| Yes | 21 (0.3%) | 4 (0.3%) | 14 (0.4%) | 3 (0.1%) | |
| CV events | 0.5985 | ||||
| No | 7,589 (96.7%) | 1,358 (97.0%) | 3,594 (96.8%) | 2,637 (96.5%) | |
| Yes | 258 (3.3%) | 42 (3.0%) | 119 (3.2%) | 97 (3.5%) | |
| CMS risk score, mean (SD) | 1.29 (0.77) | 1.24 (0.74) | 1.31 (0.77) | 1.31 (0.80) | 0.0065* |
| Total number of other medications, mean (SD) | 6.53 (4.21) | 6.29 (4.15) | 6.59 (4.18) | 6.60 (4.29) | 0.0522 |
| Regimen complexity, mean (SD) | 21.12 (38.8) | 20.78 (37.28) | 21.04 (37.49) | 21.40 (41.26) | 0.8769 |
*indicates statistical significance at p < 0.05. CV: cardiovascular; CMS: Centers for Medicare & Medicaid Services.
To identify the optimal number of groups, we systematically tested models ranging from 2 to 5 trajectories using a second-order polynomial function of time [16]. The selection of the final 3-group model was based on achieving a significant 2*ΔBIC (2*ΔBIC > 2), and maintaining clinical interpretability. Although models with 4 and 5 groups yielded improved BIC values, they were rejected because they resulted in trajectory groups with less than 5% membership (3.15% and 1.32%, respectively) (Table S2), violating our pre-specified stability criteria. The final identified trajectories, illustrated in Figure 3, included: (1) rapid decline (19.4%), (2) near-perfect adherence (57.0%), and (3) adherent (23.6%). These trajectories represent the predicted probability of achieving a monthly PDC ≥ 0.8 at each time point over the 12-month follow-up period, consistent with the logistic modeling approach.
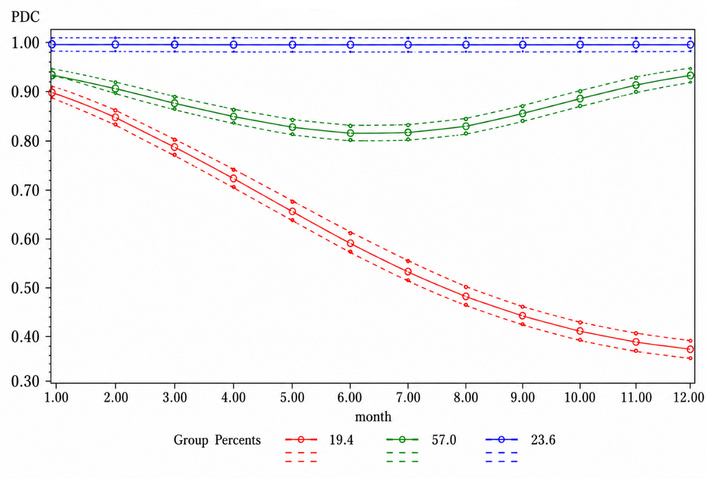
Group-based trajectories of statin adherence over 12 months. The trajectory groups included rapid decline adherence (19.4%), near-perfect adherence (57.0%), and adherent trajectory (23.6%). PDC: proportion of days covered.
Table 2 summarizes factors associated with adherence trajectories using the adherent group as the reference. Female patients had significantly higher odds of belonging to both the rapid decline [odds ratio (OR) = 1.35, 95% CI 1.19–1.55; p < 0.0001] and near-perfect adherence (OR = 1.20, 95% CI 1.09–1.33; p = 0.0004) groups compared with males. Compared with patients aged ≤ 65 years, those aged 66–69 years (p = 0.0307), 70–74 years (p = 0.0002), and ≥ 75 years (p = 0.0157) were significantly less likely to experience a rapid decline in adherence. A history of hospitalization was also predictive, as patients with at least one prior hospitalization had higher odds of belonging to the rapid decline group (OR = 1.43, 95% CI 1.02–2.01; p = 0.0385) compared with the adherence group. Additionally, a higher number of other medications was associated with reduced odds of rapid adherence decline (OR = 0.98, 95% CI 0.961–0.996; p = 0.016).
Multinomial logistic regression to assess predictors associated with each trajectory (n = 7,847).
| Variable | Rapid decline vs. adherent [OR (95% CI)] | p-value | Near-perfect adherent vs. adherent [OR (95% CI)] | p-value |
|---|---|---|---|---|
| Sex (female vs. male) | 1.354 (1.186–1.546) | < 0.0001* | 1.202 (1.086–1.330) | 0.0004* |
| Age (Ref: ≤ 65) | ||||
| 66–69 | 0.792 (0.641–0.978) | 0.0307* | 0.910 (0.770–1.077) | 0.2722 |
| 70–74 | 0.661 (0.530–0.823) | 0.0002* | 0.908 (0.765–1.077) | 0.2664 |
| ≥ 75 | 0.760 (0.609–0.950) | 0.0157* | 0.941 (0.790–1.120) | 0.4937 |
| Low-income subsidy (yes vs. no) | 0.977 (0.854–1.117) | 0.7349 | 1.036 (0.935–1.148) | 0.4967 |
| ≥ 1 prior hospitalization (yes vs. no) | 1.432 (1.019–2.012) | 0.0385* | 0.925 (0.697–1.227) | 0.5877 |
| Depression (yes vs. no) | 2.469 (0.545–11.193) | 0.2411 | 3.354 (0.959–11.727) | 0.0581 |
| CV event (yes vs. no) | 0.839 (0.570–1.234) | 0.3723 | 0.933 (0.701–1.240) | 0.6318 |
| CMS risk score | 0.921 (0.837–1.013) | 0.0886 | 1.016 (0.948–1.088) | 0.6579 |
| Total other medications | 0.978 (0.961–0.996) | 0.016* | 0.995 (0.981–1.008) | 0.4174 |
| Regimen complexity | 1.000 (0.998–1.002) | 0.9829 | 1.000 (0.999–1.001) | 0.8425 |
*indicates statistical significance at p < 0.05. OR: odds ratio; CV: cardiovascular; CMS: Centers for Medicare & Medicaid Services.
This study utilized GBTM to identify distinct longitudinal adherence patterns to statin therapy among older adults on concurrent triple therapy enrolled in a Medicare Advantage plan. Our analysis identified three distinct statin adherence trajectories over 12 months: near-perfect adherence (57.0%), adherent (23.6%), and rapid decline (19.4%). Multinomial logistic regression identified female sex, prior hospitalization, total other medications, and age as significant predictors of these patterns. Although this study did not directly evaluate CV outcomes, prior evidence has consistently shown that poor adherence to and discontinuation of statin therapy are associated with significantly higher risks of myocardial infarction, stroke, and all-cause mortality compared to sustained adherence [22, 23]. Therefore, membership in the “rapid decline” group (19.4%) likely represents a critical window of elevated clinical risk, warranting early identification and targeted intervention.
The study’s strengths include the use of longitudinal trajectory modeling to capture dynamic adherence behavior rather than reliance on single summary measures, the focus on a clinically important high-risk population receiving cardiometabolic triple therapy, and the identification of patient-level predictors that may inform targeted interventions within Medicare quality improvement efforts. However, certain limitations should be acknowledged. The retrospective design limits causal inference, and pharmacy refill claims may not fully reflect actual medication use. In addition, exclusion of patients with dementia or contraindications and the absence of detailed sociodemographic variables may affect generalizability and introduce residual confounding. Furthermore, the prevalence of certain comorbidities, such as depression (0.3%), was notably lower than national estimates for Medicare beneficiaries. The low prevalence likely reflects significant undercoding in administrative claims. This is consistent with findings by Noyes et al. [24] (2011), who demonstrated that Medicare claims data significantly underestimate the true prevalence of depression among older adults when compared to direct patient assessments. These factors should be considered when interpreting the findings and in guiding future research.
These findings complement and extend our earlier work on adherence to the overall triple therapy regimen among the same cohort of individuals taking triple therapy (comprising statins, RAS antagonists, and oral antidiabetics) [18]. This statin-only analysis identified three trajectory groups compared to four in the composite outcome analysis, which included an additional gradual decline group. This suggests that adherence to statins as a single therapeutic class is often dichotomous, with patients either sustaining therapy or discontinuing early, unlike the dynamic fluctuation observed in managing a multidrug regimen.
Another key distinction is the overall adherence rate. Only 42.5% of patients maintained adherence to the composite triple therapy (PDC ≥ 80% for all three medications), whereas 80.6% of the cohort maintained either near-perfect (57.0%) or adherent (23.6%) to statin therapy alone throughout the follow-up period. This suggests that adherence patterns can vary between individual medications and the combined regimen, underscoring the challenges of maintaining high adherence across multiple therapies simultaneously. This finding has implications for Medicare STAR program quality improvement efforts, as a patient labeled non-adherent based on the composite metric may still be highly compliant with specific therapies, such as statins.
Consistent with the composite triple-therapy analysis, female patients were significantly more likely to exhibit a rapid decline in statin adherence. The persistence of this effect across both models suggests that sex differences reflect broader behavioral and psychosocial mechanisms rather than therapy-specific factors. Prior studies have reported that females generally have lower adherence to statins and other chronic medications than males [25, 26]. Several explanations have been proposed: women often report more medication-related concerns, a greater influence of medication-related beliefs, and greater competing family or caregiving responsibilities, all of which may contribute to intentional or unintentional non-adherence [27–29]. In patients with hyperlipidemia (specifically hypercholesterolemia), women demonstrate poorer statin adherence and may be more likely to discontinue therapy because of perceived or actual statin-related side effects, as highlighted by Venditti et al. [30]. Taken together, these findings indicate that sex-related differences in risk perception, daily role demands, and side-effect experiences may collectively explain the higher likelihood of adherence decline observed among female patients in this cohort.
In both models, having at least one prior hospitalization was associated with higher odds of rapid decline. This finding aligns with evidence that hospital discharge is a high-risk period for medication discontinuation. Studies show that statin adherence declines after hospitalization for CV events, likely due to disrupted routines and poor medication reconciliation. For instance, Booth et al. [13] found that adherence to high-intensity statins among Medicare beneficiaries declined markedly within two years after myocardial infarction, highlighting the persistent vulnerability during the post-discharge period. Consistently, other evidence indicates that statin discontinuation occurs early and frequently after hospitalization, with nearly 40% of patients discontinuing therapy within the first year following ischemic stroke, a pattern associated with significantly increased mortality (HR = 2.78) [31]. For practicing physicians, this “rapid decline” in adherence following hospitalization represents a critical window for intervention to prevent adverse outcomes. These findings highlight the critical need for improved continuity of care and adherence support during the transition from hospital to outpatient settings. Prior studies have demonstrated the importance of maintaining medication continuity after discharge [32], while pharmacist-led transitional care interventions and early post-discharge follow-up have been shown to improve post-hospitalization medication management and continuity of care [33].
Conversely, this study found that older age and total number of other medications were associated with lower odds of belonging to the rapid decline trajectory for statins, even though these factors were not significant predictors of adherence to the composite triple therapy. While some studies have reported poorer adherence among very old adults in patients taking only statins [34, 35], the older adults in our cohort were significantly less likely to be in the rapid decline group. One possible explanation is that patients concurrently managing hypertension, diabetes, and dyslipidemia may receive more consistent longitudinal care, including more frequent provider contact and medication monitoring, which could reinforce adherence behaviors. In contrast, younger patients may face competing work or lifestyle priorities, lower perceived need for long-term therapy, or treatment fatigue, as suggested in prior adherence research [36].
Although all patients in this cohort were on concurrent RAS antagonist, oral antidiabetic, and statin therapies, the total number of other medications was paradoxically associated with better adherence to statins. This finding may reflect differences in how patients manage complex conditions. Individuals taking more medications often have more frequent healthcare encounters and structured follow-up, which can enhance their engagement and reinforce the perceived importance of statins for CV protection. However, maintaining equally high adherence across all therapies may be challenging, leading some patients to prioritize medications they view as most beneficial or strongly emphasized by providers, such as statins in this case, while adherence to the overall regimen declines. Prior studies have reported mixed associations between polypharmacy and adherence (with most reporting a negative association) due to these reasons [37].
Another distinction between adherence to triple therapy and statin-only therapy involves economic access factors, particularly the Medicare LIS. The LIS program under Medicare Part D helps reduce or eliminate prescription costs for beneficiaries with limited income by covering premiums, deductibles, and copayments. In our previous composite-therapy analysis, LIS recipients were less likely to experience rapid adherence decline, reflecting the role of financial support in sustaining complex, multi-drug regimens [18]. However, in the current statin-specific model, LIS showed no significant association with adherence. This may reflect the relatively low cost and widespread availability of generic statins, which may lessen the influence of financial barriers even among non-LIS patients. Prior studies have demonstrated that the LIS program is associated with improved adherence, particularly for medications with greater out-of-pocket costs [38, 39].
This study provides insight into the dynamic nature of medication adherence among older adults prescribed statins, RAS antagonists, and oral antidiabetic agents, therapies central to chronic disease management and Medicare STAR measures. Identification of distinct adherence trajectories, including a subgroup with rapid decline despite initial adherence, demonstrates that adherence evolves over time in response to patient and clinical factors. These patterns create opportunities for proactive, targeted interventions, such as post-discharge follow-up, medication synchronization, and pharmacist-led counseling or digital adherence monitoring.
Subgroups at higher risk of rapid decline, particularly younger patients, females, and those with prior hospitalization, may benefit from tailored engagement strategies. Motivational interviewing has demonstrated effectiveness in improving medication adherence by addressing patient beliefs, motivation, and self-efficacy [40]. Integrating such behavioral interventions into routine care and leveraging trajectory-based monitoring within Medicare plans could enable early identification of disengagement, support targeted outreach, and improve both patient outcomes and quality performance.
Future investigations should develop and test targeted interventions that address the distinct adherence trajectories identified in this analysis. Incorporating behavioral and contextual insights into such interventions could enhance their effectiveness, particularly among subgroups at risk of early adherence decline. Qualitative research is also warranted to explore the patient- and system-level factors that shape medication-taking behaviors over time. Furthermore, extending follow-up beyond the 12-month observation window is necessary to bridge the gap between adherence patterns and disease course. Future research should examine how these 12-month adherence trajectories are associated with major adverse CV events in this Medicare Advantage population, to better inform clinicians about the prognostic value of early adherence monitoring.
This study identified three distinct statin adherence trajectories among older adults on triple therapy. By identifying key predictors of rapid decline, such as female sex and prior hospitalization, clinicians can better recognize and target patients at higher risk of nonadherence. Improving adherence in these subgroups is not only a quality metric but may represent a critical step toward reducing the long-term burden of CV disease and improving patient outcomes.
2*ΔBIC: logged Bayes Factor
ACEIs: angiotensin converting enzyme inhibitors
ARBs: angiotensin receptor blockers
ASCVD: atherosclerotic cardiovascular disease
BIC: Bayesian information criterion
CMS: Centers for Medicare & Medicaid Services
CV: cardiovascular
CVD: cardiovascular disease
GBTM: group-based trajectory modeling
ICD-10-CM: International Classification of Diseases, Tenth Revision, Clinical Modification
LIS: low-income subsidy
OR: odds ratio
PDC: proportion of days covered
RAS: renin-angiotensin system
The supplementary tables for this article are available at: https://www.explorationpub.com/uploads/Article/file/1012110_sup_1.pdf.
SCO: Data curation, Formal analysis, Investigation, Visualization, Writing—original draft. SSC: Conceptualization, Formal analysis, Investigation, Writing—review & editing. IO: Investigation, Writing—review & editing. SA: Conceptualization, Methodology, Supervision, Writing—review & editing. All authors read and approved the submitted version.
The authors declare no conflicts of interest.
This study was approved by the Institutional Review Board (IRB) at the University of Houston (Protocol ID: STUDY00004473). The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Informed consent to participate is waived because this is a retrospective study involving the analysis of de-identified secondary data with no direct patient interaction, as approved by the ethical committee.
Not applicable.
The data analyzed in this study were obtained from a third-party Medicare Advantage database. Requests for access to these datasets and the SAS codes used for this study should be directed to the corresponding author.
No funding was received for conducting this study.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 669
Download: 7
Times Cited: 0