Original Article
Original Article

Affiliation:
1Allergy Research Center, Shiraz University of Medical Sciences, Shiraz 71936-35899, Iran
ORCID: https://orcid.org/0000-0001-8181-0539
Affiliation:
1Allergy Research Center, Shiraz University of Medical Sciences, Shiraz 71936-35899, Iran
Email: mozhgan.moghtaderi96@gmail.com
ORCID: https://orcid.org/0000-0002-9612-2429
Affiliation:
1Allergy Research Center, Shiraz University of Medical Sciences, Shiraz 71936-35899, Iran
Email: zkanannejad@gmail.com
ORCID: https://orcid.org/0000-0002-6208-9851
Affiliation:
2Sepehr Allergy Clinic, Tehran 19969-13311, Iran
ORCID: https://orcid.org/0000-0002-4699-5440
Affiliation:
1Allergy Research Center, Shiraz University of Medical Sciences, Shiraz 71936-35899, Iran
ORCID: https://orcid.org/0000-0003-4420-3064
Explor Asthma Allergy. 2025;3:100995 DOI: https://doi.org/10.37349/eaa.2025.100995
Received: July 26, 2025 Accepted: September 17, 2025 Published: October 20, 2025
Academic Editor: Laura Bruno, Università degli Studi di Roma, Italy
Aim: Allergic conjunctivitis (AC) is an inflammatory response of the conjunctiva triggered by exposure to common allergens, including pollen, dust mites, and animal dander. This study aimed to identify probable allergens in Iranian patients with AC.
Methods: This cross-sectional study included individuals with AC from Southwestern Iran in 2024. Skin prick tests (SPTs) were performed using commercial extracts of various allergens, including tree mix, weed mix, grass mix, dust mite mix, fungi mix, as well as cat and cockroach allergens.
Results: Among 92 patients with conjunctivitis, with a mean age of 23.66 ± 14.70 years, 80 patients (86.96%) had a positive SPT to at least one of the applied extracts. Sensitization rates detected by SPTs were as follows: weed mix 68.48%, tree mix 58.70%, grass mix 53.26%, dust mite mix 45.65%, cockroach 29.35%, fungi mix 22.83% and cat allergen 17.39%. A significant difference in dust mite sensitization was observed between patients with seasonal and perennial AC (p = 0.023).
Conclusions: This study highlights the allergic sensitization of patients with conjunctivitis and its connections to other allergic conditions. Allergists can play a crucial role in managing conjunctivitis through comprehensive testing and holistic treatment approaches.
Allergic conjunctivitis (AC) is a common ocular disorder and ranks among the most frequently encountered conditions in clinical practice. It includes various subtypes such as seasonal AC (SAC), perennial AC (PAC), vernal keratoconjunctivitis (VKC), and atopic keratoconjunctivitis (AKC). In addition, giant papillary conjunctivitis (GPC) may develop as a result of prolonged contact lens wear or mechanical irritation from ocular prostheses [1–3].
SAC, often referred to as “hay fever eyes”, typically occurs during spring and summer. The main triggers are tree, weed, and grass pollens, though the specific allergens vary by region. In contrast, PAC persists year-round but often worsens in autumn, primarily due to indoor allergens like dust mites, pet dander, and mold spores. PAC is less common and usually milder than its seasonal counterpart. Although PAC can occur in isolation, it frequently coexists with other allergic disorders, including allergic rhinitis (AR), atopic dermatitis, and asthma [4, 5]. The precise etiology of VKC remains unclear, though research suggests it arises from the interplay of environmental factors and allergic triggers. Both IgE-mediated hypersensitivity and T-cell-driven immune responses contribute significantly to its pathogenesis. This condition predominantly affects children aged 5 to 10 years, with a strong association observed in those having pre-existing atopic conditions or asthma [3, 6]. AKC is a rare, bilateral ocular disorder strongly associated with pre-existing atopic dermatitis (occurring in over 90% of cases) and frequently coexisting with asthma. Although its exact cause remains uncertain [3, 7], AKC shares some immunological markers with other AC subtypes despite differing clinically and pathologically from SAC and PAC. Separately, GPC develops secondary to mechanical irritation from contact lenses or ocular prostheses [8].
Skin prick test (SPT) is one of the most informative and safe diagnostic methods for detecting IgE-mediated sensitization to allergens. This simple and minimally invasive test helps identify specific allergens responsible for a patient’s symptoms, thereby guiding effective management strategies [9].
Although AC rarely causes vision loss, it can substantially reduce patients’ quality of life. The present study aimed to identify causative allergens in Iranian patients with AC using SPT, with the goal of informing tailored therapeutic approaches such as allergen avoidance, pharmacotherapy, and immunotherapy.
This cross-sectional study enrolled patients diagnosed with AC during 2024 from two tertiary care centers in Shiraz, Iran: the Imam Reza Allergy Clinic and the Ali-Asghar Hospital Allergy Clinic (affiliated with Shiraz University of Medical Sciences). AC diagnosis was confirmed through a comprehensive clinical evaluation, including a detailed medical history, symptom assessment, and ophthalmologist-supervised physical examination. Exclusion criteria comprised: (1) current use of systemic corticosteroids, immunosuppressants, or tricyclic antidepressants; (2) presence of dermatographism; (3) severe atopic eczema; and (4) a diagnosis of VKC or AKC. Additionally, we excluded other types of conjunctivitis, such as bacterial, viral, and autoimmune conjunctivitis.
Demographic information was recorded, including age, gender, parental allergy history, and the presence of other allergic diseases such as AR, asthma, and atopic eczema. Participants were also asked about the types of AC, specifically seasonal and perennial, as well as ophthalmologist visit during the previous year. SAC is characterized by symptoms that occur during specific seasons and typically last for a limited period, whereas PAC is characterized by symptoms that occur year-round.
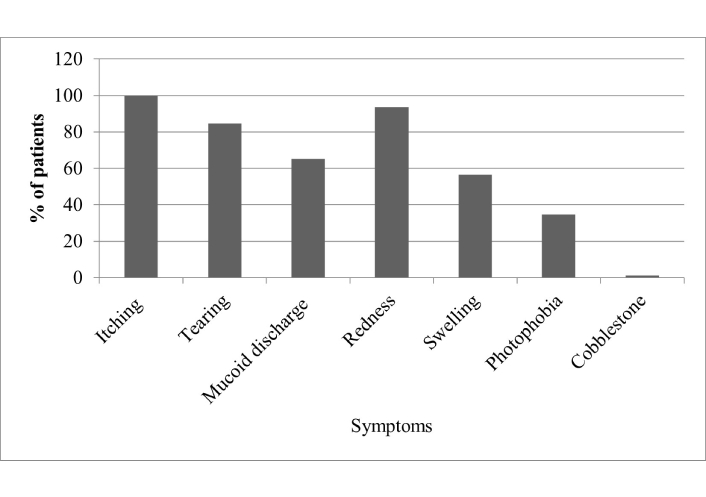
A questionnaire was used to collect information from patients regarding their eye allergic reactions, which included symptoms such as itching, redness, as well as tearing and mucoid discharge. Additionally, the questionnaire addressed swelling, photophobia, and the presence of a cobblestone appearance in the conjunctiva.
SPTs were performed on the forearms using various allergen mixes, including tree mix (birch, elm, maple, oak, palm, cypress, sycamore, ash, olive), weed mix (plantain, lamb’s quarter, Russian thistle), grass mix (Bermuda, Kentucky, ryegrass, timothy, wheat), mite mix (Dermatophagoides pteronyssinus and Dermatophagoides farinae), fungi mix (Alternaria, Aspergillus niger, Cladosporium, Penicillium), as well as cat and cockroach allergens. The allergen extracts were from the same manufacturer (Immunotek, Spain). The selection of allergens was based on common allergens in the studied area. Allergen extracts were administered on the volar surface of the forearm using sterile lancets, maintaining a minimum 2 cm distance between test sites to prevent cross-reactivity and false-positive interpretations. Histamine (10 mg/mL) and normal saline were concurrently applied as positive and negative controls, respectively, to validate test reliability. Results were examined after 15 min and were considered positive if the wheal was ≥ 5 mm in diameter compared to the negative control. Topical corticosteroids were discontinued one day prior to testing, and individuals were instructed not to take any antihistamine medication for five days before the tests. Polysensitization was defined as a positive skin test result to two or more different groups of allergens.
Continuous variables are expressed as mean ± standard deviation (SD), while categorical variables are summarized as frequencies and percentages. Associations between qualitative variables were assessed using the chi-square (χ2) test. All analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA), with statistical significance set at p < 0.05.
Ninety-two patients with AC were enrolled in the study, consisting of 47 females and 45 males. Their ages ranged from 4.5 to 52 years, with a mean age of 23.66 ± 14.70 years. Among the total of AC patients, 36 (39.13%) had seasonal AR, 34 (36.96%) had perennial AR, while 22 (23.91%) had no AR. Additionally, 18 (19.57%) patients had no type of atopy, including AR, asthma, and eczema. Table 1 presents the main characteristic data of patients who had AC.
Main characteristic data of 92 studied patients with allergic conjunctivitis.
| Characteristic data | Patients with conjunctivitis |
|---|---|
| Age, years (mean ± SD) | 23.66 ± 14.70 |
| Sex, n (%) | |
| Female | 47 (51.09) |
| Male | 45 (48.91) |
| Type of conjunctivitis, n (%) | |
| Perennial | 53 (57.61) |
| Seasonal | 39 (42.39) |
| Allergic rhinitis, n (%) | |
| Yes | 70 (76.09) |
| No | 22 (23.91) |
| Asthma, n (%) | |
| Yes | 52 (56.52) |
| No | 40 (43.48) |
| Atopic eczema, n (%) | |
| Yes | 23 (25.00) |
| No | 69 (75.00) |
| Parental allergy, n (%) | |
| Yes | 38 (41.30) |
| No | 54 (58.70) |
| Visit by ophthalmologist, n (%) | |
| Yes | 43 (46.74) |
| No | 49 (53.26) |
Among the 92 patients with AC, all reported experiencing itching, which was followed by redness and tearing. The least common symptom observed was cobblestone. This information is illustrated in Figure 1.
Among patients with AC, 24 patients (26.09%) were mono-sensitized to any of the plant allergens (tree, grass, or weed), while poly-sensitization to pollens was seen in 75 (81.52%). Mono-sensitization to mites was observed in 5 patients (5.43%), to cockroach in 3 patients (3.26%), and to fungi and cat allergens in 1 patient each (1.09% each). Additionally, 12 patients (13.04%) showed no sensitization to the studied allergens. Table 2 shows the frequency of positive SPTs to seven applied allergens in patients with AC.
Frequency of positive skin tests to applied allergens in 92 patients with allergic conjunctivitis.
| Allergens | n (%) |
|---|---|
| Tree mix | 54 (58.70) |
| Weed mix | 63 (68.48) |
| Grass mix | 49 (53.26) |
| Mite mix | 42 (45.65) |
| Fungi mix | 21 (22.83) |
| Cat | 16 (17.39) |
| Cockroach | 27 (29.35) |
This study showed that 53 patients had PAC and 39 had seasonal type. There was no significant relationship was observed between sex (p = 0.650), AR (p = 0.40), asthma (p = 0.79), eczema (p = 0.18), or parental allergy (p = 0.96) and the type of AC. The frequency of allergens in patients with AC is compared between SAC and PAC in Table 3. There was a significant difference in allergen sensitization between the two groups with mite sensitization (p = 0.028).
Comparison of allergens by skin testing in two groups of patients with allergic conjunctivitis.
| Allergens | Perennial conjunctivitisn = 53 | Seasonal conjunctivitisn = 39 | p value |
|---|---|---|---|
| Tree mix, n (%) | 30 (56.60) | 24 (61.54) | 0.635 |
| Weed mix, n (%) | 38 (71.70) | 25 (64.10) | 0.438 |
| Grass mix, n (%) | 27 (50.94) | 22 (56.41) | 0.604 |
| Mite mix, n (%) | 19 (35.85) | 23 (58.97) | 0.028 |
| Fungi mix, n (%) | 9 (16.98) | 12 (30.77) | 0.119 |
| Cat, n (%) | 10 (18.87) | 6 (15.38) | 0.663 |
| Cockroach, n (%) | 12 (22.64) | 15 (38.46) | 0.100 |
While AC is usually diagnosed clinically, skin allergy testing confirms sensitization to specific allergens. Our patients with AC had sensitization to allergens as follows: plant allergens 75 (81.52%), dust mites 42 (45.65%), cockroach 27 (29.35%), fungi 21 (22.83%), and cat 16 (17.39%).
Pollen grains become airborne during certain seasons and come in contact with the ocular surface. An aerobiological survey was carried out in the atmosphere of Shiraz, Iran, during 2012, which showed that 82.44% of the pollen was tree type, 7.24% was weed, and 10.32% was grass type [10]. This study demonstrated that pollen is a major trigger for AC, and strategies such as minimizing outdoor activities during peak pollen times could be beneficial for affected individuals.
In predisposed individuals with atopy, the immune system recognizes pollen proteins as foreign. In a study of 656 patients with allergies (asthma, AR, and eczema) from Southwestern Iran, pollens were identified as the most common type of aeroallergen. Among pollens, the frequency of sensitization was higher for weeds, followed by grasses and trees [11]. In the present study, positive sensitization was most common for weeds, followed by trees and grasses. The protein structures of weed pollens may trigger a stronger immune response, leading to increased sensitization. The flowering times of weeds may coincide with periods of higher outdoor activity, leading to greater exposure. For example, certain weeds may release their pollen during times when individuals are more likely to be outdoors, increasing the likelihood of sensitization. The immunological response of the eye to tree pollen proteins may be particularly more pronounced than that to grass pollens, potentially due to the distinct protein structures and the quantity of pollen released during specific seasons.
The prevalence of dust mite sensitization among our patients with AC reveals significant insights into the role of indoor allergens in exacerbating allergic responses. A systematic review and meta-analysis indicated a sensitization of 33.4% to house dust mites among individuals with allergies in major cities of Iran [12]. While this is noteworthy, our findings highlight a higher rate of 45.65% among patients specifically presenting with AC. This disparity may reflect regional differences in environmental conditions and indoor allergen exposure levels across various parts of Iran.
Unlike seasonal allergens such as pollen, dust mites are a perennial concern [13]. Our finding that mite sensitization is more common in patients with SAC presents an intriguing aspect of allergic disease and highlights the complexity of allergic responses. Many individuals with SAC may have a multifaceted allergic profile, meaning they are sensitized to both seasonal (like pollen) and perennial (like mites) allergens. This dual sensitization can lead to overlapping symptoms, complicating the clinical picture. Additionally, exposure to mites is common in the indoor environment, and for some patients, sensitization to mites can exacerbate symptoms during allergy seasons, even if the primary triggers are perennial. Our data underscores the importance of addressing indoor allergen control in managing of SAC.
The findings from Do et al. [14] regarding cockroach allergen levels in homes of asthmatic patients emphasize a significant indoor environmental risk factor for asthma exacerbation. With a sensitization rate of approximately 30% to cockroach among our patients with AC, this aligns with similar studies conducted in the region on 656 patients with allergy [11]. This consistency suggests that an effective management strategy include measure to reduce cockroaches’ population through improved sanitation, pest control, and education for patients about maintaining an allergen-free environment.
Fungal allergens can represent a significant concern in AC, with approximately one fourth of our patients demonstrating sensitization to these allergens. This is consistent with existing literature that links fungal exposure to various allergic conditions [15, 16].
Animal allergens, particularly from pets like cats, are significant triggers for allergic reactions, especially in urban areas where cats are common [17]. In our area, cats are especially common in the inner city. As a result, contact with cats—and exposure to their allergens—is frequent in our study area. Managing exposure to these allergens is essential for protecting public health, especially for those with AC.
In our study, 12 patients (13.04%) showed no sensitization to any of the allergens tested. Some patients with AC exhibit negative results on SPT and serum-specific IgE tests [18]. Bonini [19] found that approximately 50% of patients with ocular AC had negative SPT results. Masrur et al. [20] reported that in a cohort of 150 cases in Pakistan, 61.3% tested negative for allergens. SPT has limitations in sensitivity, and some allergens may not be included in the testing panel, leading to false negatives. In cases of negative SPT despite the presence of AC, it is advisable to use additional diagnostic methods, such as serum-specific IgE testing or conjunctival provocation tests. Furthermore, it is important to note that some patients may experience AC driven by mechanisms that do not involve IgE antibodies, such as T-cell mediated responses. These mechanisms will not be detected by SPT.
Poly sensitization refers to the condition where an individual is sensitized to multiple allergens and an 81.5% rate of poly-sensitization among our patients indicates a significant prevalence of multiple sensitivities. This may involve avoiding outdoor activities during high pollen season for management. Over-the-counter or prescription antihistamines and topical ocular medications can help alleviate symptoms. In some cases, a combination immunotherapy may be necessary to address multiple allergens simultaneously.
AC often coexists with other allergic conditions, highlighting the interconnected nature of allergic responses [21]. Notably, 76% of our patients also had AR, reinforcing the link between AC and this common respiratory allergy. The shared pathophysiology of IgE-mediated hypersensitivity reactions suggests that exposure to allergens can elicit responses in both the conjunctiva and nasal passages.
Allergies can have a hereditary component [22]. Inherited immune responses can lead to heightened sensitivity to allergens, making individuals more susceptible to allergic reactions. In our study, 41% of patients with AC had a paternal allergy. This suggests a genetic predisposition to atopy, where individuals may be more susceptible to multiple allergic disorders.
Ophthalmologists can assess the severity of eye symptoms and differentiate them from other conditions. Among our patients with AC, about half of them refer to an ophthalmologist before our visit. Aside from seeing an ophthalmologist, patients with ocular allergies should consult an allergist to define whether they have AC and if they need a SPT or immunotherapy.
The low number of patients is a significant limitation for generalizability of our findings. Future studies with larger, multi-center cohorts will be valuable to confirm and expand upon our findings. SPT results may not accurately reflect the exact immune response in the conjunctiva, leading to potential mis-diagnosis or under-diagnosis of ocular allergens. The extracts used for the SPT were sourced from Spain. If we had utilized standard extracts specific to the local region, the results might have been more relevant. Additionally, other diagnostic methods, such as serum-specific IgE or provocation tests, may also be beneficial in diagnosing AC. Further research is necessary to explore the specific types of tree or weed pollen and their immunological impact on ocular health.
Our study sheds light on the allergic sensitization of AC and its connections to other allergic conditions. Allergists can play a crucial role in managing AC through comprehensive testing and holistic treatment approaches.
AC: allergic conjunctivitis
AKC: atopic keratoconjunctivitis
AR: allergic rhinitis
GPC: giant papillary conjunctivitis
PAC: perennial allergic conjunctivitis
SAC: seasonal allergic conjunctivitis
SPTs: skin prick tests
VKC: vernal keratoconjunctivitis
The authors thank all the participants in this study.
SHN: Conceptualization, Methodology, Investigation, Data curation, Writing—original draft. MM: Visualization, Supervision, Project administration, Writing—original draft. ZK: Project administration, Data curation, Writing—review & editing. KD: Methodology, Formal analysis, Validation. NS: Investigation, Data curation. All authors reviewed the results and approved the final version of the manuscript.
The authors declare that they have no conflicts of interest.
Ethical approval for this study (Ethical Committee IR.SUMS.REC.1403.391) was provided by the Ethical Committee of Shiraz University of Medical Sciences, and this study complies with the Declaration of Helsinki (2024 version).
Informed consent to participate in the study was obtained from all participants (for patients under 18 years of age, consent was obtained from their parents or legal guardians).
Not applicable.
The data of this manuscript could be available from the corresponding authors upon reasonable request.
The Shiraz University of Medical Science [Grant no: 31802] financially supported this study. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 3158
Download: 36
Times Cited: 0