Case Report
Case Report

Affiliation:
1Ambulatorio di Allergologia, Struttura Complessa di Dermatologia, Azienda Ospedaliera Universitaria Policlinico di Modena, 41124 Modena, Italy
ORCID: https://orcid.org/0000-0001-5303-3517
Affiliation:
2Allergy and Clinical Immunology Residency, University of Milan, 20122 Milan, Italy
Email: silvio.sartorio@unimi.it
ORCID: https://orcid.org/0009-0008-5936-9757
Affiliation:
1Ambulatorio di Allergologia, Struttura Complessa di Dermatologia, Azienda Ospedaliera Universitaria Policlinico di Modena, 41124 Modena, Italy
Affiliation:
3Operative Unit of Medicine, Angioedema Center, IRCCS Policlinico San Donato, 20097 San Donato Milanese, Italy
4Department of Biomedical Sciences for Health, University of Milan, 20133 Milan, Italy
ORCID: https://orcid.org/0000-0002-7512-4644
Explor Asthma Allergy. 2026;4:1009125 DOI: https://doi.org/10.37349/eaa.2026.1009125
Received: March 04, 2026 Accepted: April 16, 2026 Published: May 08, 2026
Academic Editor: Lawrence DuBuske, George Washington University Hospital, United States
Netherton syndrome (NS) is a rare autosomal recessive disorder caused by SPINK5 mutations, leading to impaired skin barrier function and severe atopic manifestations. Hereditary angioedema due to C1 inhibitor deficiency (HAE-C1-INH) is a rare autosomal dominant disorder characterised by recurrent bradykinin-mediated angioedema. Their coexistence has not previously been reported, and evidence on combined biologic therapy is lacking. We report a 30-year-old woman with confirmed NS and long-standing HAE-C1-INH presenting with severe pruritus, xerosis, widespread eczema, elevated IgE, eosinophilia, and trichorrhexis invaginata. Dupilumab was initiated to target T helper (Th)2-mediated inflammation. Due to persistent angioedema attacks despite prior prophylaxis, lanadelumab was introduced. Dupilumab improved eczema severity, hyperkeratosis, and hair abnormalities over 13 months. Lanadelumab reduced angioedema attacks by 88.50%, allowing dose spacing while maintaining disease control. No adverse effects or drug interactions were observed. This is the first reported case of NS and HAE-C1-INH successfully treated with dual biologic therapy. Targeting distinct immunological pathways simultaneously may represent an effective and safe strategy for complex rare disease phenotypes.
Netherton syndrome (NS) is a rare autosomal recessive genodermatosis [1]. Mutations in the serine protease inhibitor of Kazal type 5 (SPINK5) gene, responsible for encoding the lymphoepithelial Kazal type inhibitor (LEKTI) protein, cause alterations in the epithelial surfaces of the skin [2]. The presence of ichthyosis linearis circumflexa (ILC), serpiginous, polycyclic, itchy, and migratory erythematous patches with double-edged scales, a pathognomonic hair alteration, commonly referred to as bamboo hair (trichorrhexis invaginata), and atopic diathesis, is currently accepted as evidence for clinical NS diagnosis. In the presence of one or a few symptoms, genetic testing is required for diagnosis [1, 3].
Hereditary angioedema due to C1 inhibitor deficiency (HAE-C1-INH) is a rare autosomal dominant disease affecting 1 in 50,000 people worldwide. There are two types of HAE-C1-INH: type 1 caused by C1-INH deficit (85% of patients) and type 2 caused by C1-INH dysfunction (15% of patients) [4]. The mutations responsible for the disease occur in the SERPING1 gene, which codes for the C1-INH, a serine protease inhibitor whose deficiency determines an excessive activation of the contact system with consequent release of bradykinin [5]. Angioedema is characterised by recurrent and unpredictable attacks of edema without hives, with heterogeneous phenotypes in terms of frequency, severity, and site of attacks. The diagnosis is made by complement testing [6]. As for treatment, there are on-demand therapies (plasma-derived C1-INH, recombinant C1-INH, icatibant, ecallantide, and sebetralstat) and preventative prophylaxis (lanadelumab, plasma-derived C1-INH, berotralstat, attenuated androgens, garadacimab, and donidalorsen) [4].
Here we report a case of a 30-year-old female patient affected by two rare genetic diseases, NS and HAE-C1-INH, treated with two monoclonal antibodies, dupilumab, anti-interleukin (IL)-4 and IL-13, for NS, and lanadelumab, anti-kallikrein (KLK), for HAE. Informed consent was obtained from the patient to publish the case report along with all accompanying visual elements.
A 30-year-old female NS patient was referred to our clinic with intractable pruritus, scaling, dry skin, and generalised eczematous lesions resistant to corticosteroid, emollients, and anti-bacterial atopic dermatitis (AD) therapies.
Upon physical examination, the patient’s skin was dry with erythematous scaly patches on the face, inguinal, intergluteal regions, and the abdominal area under the breasts, with signs of infection. Patient’s scalp, hair, eyebrows, and lashes were bristly, short, dry, and sparse. Patient’s hands and legs were markedly eczematous (Figure 2).

Clinical presentation at the first visit. Dry skin with erythematous, scaly patches involving (A) the inframammary folds, (B) the face, and (C) the legs.
Video-microscopical evaluation of the patient’s hair revealed trichorrhexis invaginata. Eosinophilia (880 cells/microliter) and elevated total IgE levels (5,030 IU/mL, measured with immunoturbidimetric assay) were recorded.
Standard AD severity evaluations were performed and were within the high ranges (Table 1). Both Eczema Area and Severity Index (EASI) and SCORing Atopic Dermatitis (SCORAD) were particularly high (50.20 and 88.10).
Measurement of Eczema Area and Severity Index (EASI), Dermatology Life Quality Index (DLQI) [9], Validated Investigator Global Assessment scale (vIGA) [10], SCORing Atopic Dermatitis (SCORAD), Numeric Rating Scale (NRS) pruritus [11], and NRS sleep disturbance [12] scores at baseline (T0), 3 months (T1), 4 months (T2), 13 months (T3) after initiation of dupilumab treatment, including percentage changes from T0 to T2 and T0 to T3.
| Visit | T0 | T1 | T2 | T3 | Difference between T0 and T2 (%) | Difference between T0 and T3 (%) |
|---|---|---|---|---|---|---|
| Month | 0 | 3 | 4 | 13 | ||
| EASI | 50.20 | 28.70 | 22.70 | 13.40 | 54.80 | 73.30 |
| DLQI | 16.00 | 15.00 | 5.00 | 9.00 | 68.80 | 43.80 |
| vIGA | 4.00 | 3.00 | 3.00 | 3.00 | 25.00 | 25.00 |
| SCORAD | 88.10 | 69.10 | 58.10 | 43.60 | 34.10 | 50.50 |
| NRS pruritus | 9.00 | 6.00 | 5.00 | 3.00 | 44.40 | 66.70 |
| NRS sleep disturbance | 6.00 | 5.00 | 4.00 | 0.00 | 33.30 | 100.00 |
As the patient did not respond to continuous topical treatment and her quality of life was significantly impaired, we decided to initiate systemic therapy. Dupilumab was selected due to its targeted action against T helper (Th)2-mediated inflammation, which plays a central role in the disease pathophysiology, particularly given the limited effective treatment options and the scarcity of reports available at the time. We started with an initiation dose of 600 mg in July 2021, followed by a maintenance dosage of 300 mg every 14 days. At 4 and 13-month follow-up, we observed an improvement for all scores (Table 1).
After 13 months of uninterrupted dupilumab treatment, clinical manifestations and dermoscopic images of the patient’s hair were documented to be longer, smoother, and thicker, with a reduced incidence of “bamboo” hair. Skin lesions were healing.
Dermatological scores, as well as skin and hair appearance, remained stable over the years, maintaining disease control to the present day.
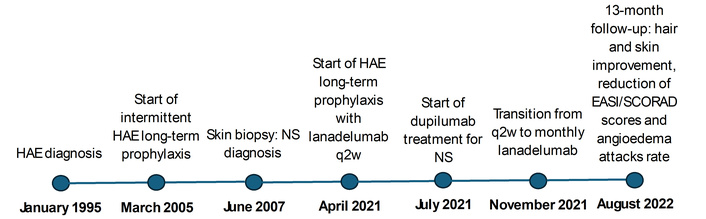
The patient was also affected by HAE-C1-INH. While growing up, the first manifestations were colicky symptoms and cutaneous swelling.
Throughout the years, she continued experiencing abdominal and cutaneous angioedema with increasing frequency. Since 2005, she had been intermittently on long-term prophylaxis: tranexamic acid first (discontinued for lack of efficacy), then stanazolol (suspended because of menses alterations), and eventually twice-weekly self-administered plasma-derived C1-INH (1,000 U), reporting a mean of four angioedema attacks per month.
In April 2021, the patient started a long-term prophylaxis with lanadelumab (a subcutaneously self-administered drug) 300 mg every two weeks. After four months, the patient reported a mean of one attack per month. From October 2021, lanadelumab 300 mg was administered monthly with an attack rate of 0.75/month (Table 2).
Monthly frequency of angioedema attacks from 2016 to present.
| Observation period | T0 | T1 | T2 | Difference between T0 and T1 (%) | Difference between T0 and T2 (%) |
|---|---|---|---|---|---|
| Frequency of attacks (per month) | 6.50 | 4.00 | 0.75 | 38.50 | 88.50 |
Attack rates are shown across three clinical management phases: T0 (2016–September 2019, no prophylaxis), T1 (September 2019–April 2021, long-term prophylaxis with plasma-derived C1-INH), and T2 (April 2021–present, long-term prophylaxis with lanadelumab). Variations were −38.50% from T0 to T1 and −88.50% from T0 to T2. Data before T2 were retrospectively collected from the patient’s clinical history and medical records. C1-INH: C1 inhibitor.
Patient’s NS was diagnosed at the age of 16, when a skin biopsy was performed and revealed the total absence of LEKTI protein, as per a SPINK5 mutation. No family history of skin disorders was recorded. Whereas, since HAE was already diagnosed in her family, at 4 years old she was tested for C1-INH and C4, showing pathological values: functional C1-INH was 16.00% (normal range 70.00–130.00%; measured with chromogenic assay), antigenic C1-INH was 54.00% (normal range 70.00–115.00%; measured with radial immunodiffusion) and C4 38.00% (normal range 60.00–140.00%; measured with radial immunodiffusion).
“Living with both Netherton syndrome and hereditary angioedema has meant constant itching, visible skin lesions, fragile hair, and unpredictable swelling attacks that caused pain and anxiety since childhood. These conditions deeply affected my daily life and self-confidence. With dupilumab, my skin and hair gradually improved, and with lanadelumab, angioedema attacks became rare and more manageable. Receiving both treatments has significantly improved my quality of life and helped me regain a sense of control”.
The LEKTI deficiency leads to unopposed KLK-related peptidases (KLK5, KLK7, and KLK14) activity, which leads to protease-activated receptor 2 (PAR-2) stimulation, eventually causing the production of thymic stromal lymphopoietin (TSLP) cytokine and tumor necrosis factor (TNF) [1]. TSLP is involved in Th0 cells’ differentiation into Th2 cells, producing cytokines like IL-4 and IL-13, which are associated with B cell differentiation and IgE production. The possible mechanism of dupilumab successfully treating NS is that by blocking IL-4/IL-13 signalling, as an IL-4 receptor alpha antagonist, it can control the Th2-mediated inflammation and skin barrier defects [13].
Our case showed that not only could dupilumab improve the eczema and hyperkeratosis, but it could also improve bamboo hair (evaluated through clinical photography and dermoscopic images). In contrast to the other known cases [13], our patient obtained a partial and slow response. The data is below the 85.10% of EASI 50 response of the global observed efficacy of dupilumab in AD [14] after 16 weeks of treatment. This may be explained by the underlying genetic barrier defect in NS, which differs from classic AD and may limit treatment responsiveness. In fact, dupilumab addresses the inflammatory consequences rather than correcting the underlying genetic defect [15]. Nevertheless, her quality of life greatly improved with treatment.
As for patients’ HAE-C1-INH, it is known that the absence of C1-INH favours the activation of the contact system, producing plasma KLK from prekallikrein, which releases bradykinin from high-molecular-weight kininogen, with consequent edema [5]. Thus, inhibition of plasma KLK is thought to be effective in controlling angioedema symptoms. As a matter of fact, lanadelumab, a monoclonal antibody targeting plasma KLK, successfully reduced angioedema attacks by 93.00% in very high disease activity patients in real-world data [16]. Our patient reached a reduction of frequency of attacks of 88.50% compared to the no prophylaxis period, which motivated her to continue the administration of the drug.
The co-occurrence of these two rare autosomal recessive (NS) and autosomal dominant (HAE-C1-INH) conditions in this patient represents an extremely rare coincidence. SPINK5 is located on chromosome 5q32 [1], while SERPING1 is located on chromosome 11q12–q13.1 [5]. The involvement of KLK in both diseases represents a convergence of two distinct proteolytic pathways that share a common enzyme family but operate in completely different anatomical and biochemical contexts. Both LEKTI and C1-INH are serine protease inhibitors, but they have non-overlapping substrate specificities. LEKTI inhibits tissue KLKs (KLK5, KLK7, and KLK14), while C1-INH (a serpin) regulates plasma KLK, activated factor XII, and complement proteases. Thus, the contact activation system is distinct from the epidermal KLK proteases in NS [1, 5]. The successful concurrent use of both biologics suggests these represent independent disease processes requiring distinct therapeutic approaches. Accordingly, no adverse influence of either therapy on the condition for which it was not indicated was anticipated: dupilumab is not expected to enhance bradykinin sensitivity or exacerbate angioedema attacks, and lanadelumab does not cross-react with or inhibit tissue KLKs. In our view, no additional monitoring specific to the combination was required beyond the standard monitoring recommended for each agent individually.
This is the first reported case of a patient with HAE-C1-INH and NS, as well as of concomitant use of dupilumab and lanadelumab. Treatments were fully tolerated for a strict observation time of 56 weeks and up to the present day. No serious adverse events were reported. Further evaluation is needed, as more biological drugs are available, patients with rare diseases could benefit from the use of concomitant biological drugs.
AD: atopic dermatitis
EASI: Eczema Area and Severity Index
HAE-C1-INH: hereditary angioedema due to C1 inhibitor deficiency
IL: interleukin
KLK: kallikrein
LEKTI: lymphoepithelial Kazal type inhibitor
NS: Netherton syndrome
SPINK5: serine protease inhibitor of Kazal type 5
Th: T helper
TSLP: thymic stromal lymphopoietin
MBG: Conceptualization, Validation, Writing—review & editing. SS: Investigation, Writing—original draft. MR: Investigation, Writing—original draft. AZ: Validation, Writing—review & editing, Supervision. All authors read and approved the submitted version.
Andrea Zanichelli received speaker/consultancy fees from and/or was a member of advisory boards for Astria Therapeutics, BioCryst, CSL Behring, KalVista Pharmaceuticals, Pharming, Pharvaris, Otsuka, and Takeda. The other authors declare no conflicts of interest.
The study complies with the Declaration of Helsinki. Ethical approval is not required for a case report study according to the local ethics committee.
Informed consent to participate in the study was obtained from the participant.
Informed consent to publication was obtained from the participant.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Not applicable.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 550
Download: 21
Times Cited: 0