 Commentary
Commentary

Affiliation:
1School of Medicine and Surgery, Catholic University, 00168 Roma, Italy
Email: riccardo.pistelli49@gmail.com
ORCID: https://orcid.org/0000-0003-3776-2482
Affiliation:
2GSK Medical Department, GSK Italy, 37135 Verona, Italy
Affiliation:
2GSK Medical Department, GSK Italy, 37135 Verona, Italy
ORCID: https://orcid.org/0000-0001-8731-5029
Affiliation:
3Unit of Allergy and Clinical Immunology, SS Annunziata Central Hospital, 74121 Taranto, Italy
Affiliation:
4Department of Biomedical Sciences, Humanitas University, 20072 Milan, Italy
5Asthma & Allergy Unit, Humanitas Research Hospital-IRCCS, 20089 Milan, Italy
ORCID: https://orcid.org/0000-0001-8467-2557
Explor Asthma Allergy. 2026;4:1009117 DOI: https://doi.org/10.37349/eaa.2026.1009117
Received: September 28, 2025 Accepted: February 06, 2026 Published: March 12, 2026
Academic Editor: Makoto Hoshino, International University of Health and Welfare Atami Hospital, Japan
APPaRENT2 was a multi-country, cross-sectional, online survey of patients with asthma and physicians conducted in five countries (Argentina, Brazil, France, Mexico, and Italy), aimed at assessing physicians’ and patients’ preferred treatment strategies and goals. Education level, age, and place of residence differed between European and Latin American patients; furthermore, most Italian doctors worked within the Public Health Service. For the purpose of identifying the critical issues in the management of asthma in Italy, the data were analysed in greater detail, comparing those collected in Italy with those from Latin American countries and those provided by Italian patients and doctors. The data are reported as frequencies or means. The differences found in comparing data were not analysed for statistical significance, given the absence of any a priori hypothesis in the original paper. The Italian results were consistently within the range of the Latin American countries’ results. In Italy, despite the physicians’ prioritization of symptom control, many patients had poor asthma control but gave a surprisingly optimistic evaluation of their disease, given the high frequency of symptoms and limitations in everyday life. Physicians and patients had quite different evaluations of symptoms and outcomes of asthma. Finally, the combination of ICS/LABA with SABA as needed was the preferred treatment compared with the maintenance and reliever therapy (MART) strategy, suggested as preferential in the Global Initiative for Asthma (GINA) document. In conclusion, the absence of shared assessments and expectations between doctors and patients appears to be the primary issue to address in order to improve asthma treatment in Italy.
Patients suffering from asthma and doctors sampled in Italy for the APPaRENT2 survey had very divergent opinions on the severity of the disease and its most important manifestations.
Doctors largely used judgments based on their personal intuition to evaluate the effectiveness of asthma treatments. The assessment of treatment adherence in their patients was largely overestimated compared with the reality reported in national statistics.
The MART strategy, defined as preferential in the GINA document, was quite rarely prescribed, the consolidated association of ICS/LABA with SABA as needed was the treatment of choice in most patients.
The APPaRENT2 study [1] was a multi-country, cross-sectional, online survey of patients with asthma and physicians (primary care and specialists) that aimed to describe the reality of asthma treatment and how it aligned with the recommendations of the Global Initiative for Asthma (GINA) [2] available at the time of the survey in five countries: Argentina, Brazil, France, Mexico, and Italy. All participants were sampled and recruited using panels certified by the International Organization for Standardization between August and November 2021. Based on the methodology used, the samples studied in APPaRENT2 (330 patients and 216 physicians in each country) could be considered reasonably representative of patient and physician populations in the countries participating in the survey. Notably, sampled Italian patients were older, had a lower level of schooling, and were less often living in large urban areas than patients sampled in Latin American countries (Table 1). Similarly, sampled Italian physicians were slightly older, less frequently operating in large urban areas, and much more frequently operating within the national health system. Given these sample characteristics, it seemed relevant to analyse the Italian data in further detail in order to: 1) describe similarities and discrepancies in asthma symptoms, severity, and treatment protocols between Italy and the other countries; and 2) highlight critical issues in the management of patients with asthma in Italy. Since this study was a secondary analysis conducted on an already existing and anonymous database, further submission to the judgment of an ethics committee was not deemed necessary.
Demographic characteristics of Italian and Latino American countries.
| Demographic characteristics | Italy | Latino American countries |
|---|---|---|
| Patients (n) | 330 | 330 in each country |
| Mean age (years) | 43 | 32–36 |
| College/University (%) | 34 | 66–81 |
| Living in a large city (%) | 32 | 71–78 |
| Physicians (n) | 216 | 216 in each country |
| Mean age (years) | 47 | 42–47 |
| Working in a large city (%) | 51 | 81–87 |
| Working within NHS (%) | 68 | 28–33 |
NHS: National Health Service.
The data reported in this study are the result of a descriptive analysis and are presented as proportions for categorical variables and means for continuous variables. The sample sizes reported in Table 1 were used to calculate all means and proportions. No use was made of statistical analysis of differences between means and proportions. The data dispersion ranges among Latin American countries were used to describe the position of the Italian data with respect to the same data collected in those countries characterized by substantially different health care systems.
According to patients, and using a three-level (mild, moderate, severe) Likert scale, the frequency of severe asthma in Italy was 6% (reference range 1–9%), and 65% of patients attributed the evaluation of the severity of asthma to their physicians (reference range 67–84%). In the opinion of patients, asthma was partially or even better controlled in 91% of the cases (reference range 90–92%). However, 44% of patients reported a relevant limitation of their working ability (reference range 42–55%); 47% reported shortness of breath three or more times a week (reference range 42–55%); 47% reported nocturnal awakenings due to asthma at least once a week (reference range 56–67%). Moreover, 60% of patients reported using a short-acting bronchodilator as a reliever two or more times in a week (reference range 67–82%). Analyzing the disease experience of Italian patients in more detail, surprisingly, reducing the risk of exacerbations, which is the primary and most important outcome of many recent asthma clinical trials [3–7], was clearly no more impacting than maintaining a satisfactory lung function or reducing the impact of daily symptoms, these three outcomes being quite or very important for 48%, 47%, and 42% of all patients, respectively.
Physicians and asthma of their patients: According to physicians, and using a five-level (mild, moderate, severe, unclear, fluctuating) Likert scale, in Italy the frequency of patients with severe asthma was 15% (reference range 9–11%) and the frequency of at least one exacerbation per year in those patients was 72% (reference range 64–67%). However, patients with mild or moderate asthma also had high frequencies of exacerbations: 38% (reference range 33–44%) and 50% (reference range 45–52%), respectively. Italian physicians reported estimating asthma control using heterogeneous instruments: from frequency of reliever use (used by 58% of respondents) to standardized tools such as the GINA-recommended tool [2], the Asthma Control Test (ACT) [8], and the Asthma Control Questionnaire (ACQ) [9], used by 33%, 26%, and 26% of physicians respectively, or fractional exhaled nitric oxide (FeNO), used by 10% of physicians. For Italian physicians, reducing symptom severity and exacerbation frequency were equally the most important treatment goals in patients with severe asthma, while improving symptom control was the most important outcome in patients with mild to moderate asthma. On the contrary, maintaining a good lung function, improving the daily and nocturnal quality of life, and reducing the frequency of a reliever use were important treatment goals for a minority of physicians across all levels of asthma severity.
In Italy, 28% of patients used only a daily controller (reference range 21–34%); 28% used both a daily controller and a different rescue inhaler when needed (reference range 23–29%); 10% used the same inhaler for both daily controller use and rescue when needed according to the maintenance and reliever therapy (MART) strategy (reference range 10–14%); and 34% used only a rescue inhaler when needed (reference range 29–45%). In Italy, 83% of patients reported being satisfied with their asthma treatment; however, 30% experienced relevant side effects, and 28% reported some negative impact of treatment on their daily life during the past year. In total, 41% of patients reported a modification of treatment decided by their doctor during the last year. The persistence of important symptoms, relevant side effects, device-related problems, and frequent exacerbations were the reasons to change the treatment in 43%, 25%, 17%, and 11% of cases, respectively. Finally, 30% of patients admitted that they often forgot about therapy. The MART strategy for the treatment of asthma was known by 50% of Italian patients. That information was due primarily to the doctor (78%) but also to the pharmacist (12%), while the remainder was due to many heterogeneous sources.
In Italy, the physician’s estimates of patients’ adherence to treatment were 66% for mild persistent asthma and 77% for moderate/severe asthma, respectively. However, those estimates were obtained using non-objective and very heterogeneous methods. Only 2% of physicians answered “never” to the question about the frequency of use of a written action plan for asthma with their patients, which they were supposed to adhere to at least partially in 95% of cases. In Italy, regular dosing ICS/LABA with or without SABA as a reliever was prescribed as initial treatment by 61% of physicians (reference range 52–66%) and by 50% of physicians as follow-up treatment if patients remained uncontrolled with the initial treatment (reference range 45–70%). In detail, for mild persistent asthma, ICS/LABA with or without SABA was the first choice for 29% of physicians; for moderate or severe asthma, it was the first choice for 80% of physicians. ICS/formoterol as needed or according to the MART strategy was the preferred choice for 29% of physicians in patients with mild persistent asthma, but only 14% of physicians selected that strategy as the first choice in patients with moderate or severe asthma. Finally, it should be highlighted that, in 56% of cases, the MART strategy in Italy was associated with the use of a SABA as a second reliever to be used when needed, and in complete disagreement with the guiding principle of the MART strategy.
Contrary to expectations, despite the respondents’ greater age, lower education, and residence outside large urban centres, the Italian data were in general within or very close to the limits of the range of data collected in other countries participating in APPaRENT2 [1]. In brief, the frequency of severe asthma according to the knowledge of patients was quite low (6%), and almost all patients declared their asthma was at least partially controlled. Most patients reported being satisfied with their current treatment, while admitting they frequently forgot to use it despite frequent limitations in everyday life and a substantial number of exacerbations, even among patients with mild disease. According to the physician survey, the frequency of severe asthma among Italian patients was much higher (15%) than the frequency estimated in the survey of patients. According to physicians, the majority of patients had a written action plan for their asthma to which they were adherent in the majority of cases. In particular, the adherence of patients to the pharmacological treatment was quite high, according to the opinion of physicians, but clearly at odds with the last National Drugs Report [10], which estimated high adherence to respiratory therapy in no more than 22% of patients. The physicians’ treatment strategy was mostly based on a regular use of ICS or ICS/LABA with or without SABA as a reliever when needed. ICS/formoterol as needed or according to the MART strategy was prescribed in a minority of cases. However, according to the survey of patients in Italy, a SABA when needed was the only treatment used by 34% of all cases, but only 17% of mild cases and 1% of moderate/severe cases, according to the physician survey. In summary, separate surveys of patients and physicians in Italy produced conflicting results. Satisfactory asthma control was overestimated in patients who simultaneously reported frequent symptoms and limitations in daily activities. Physicians, however, were much less optimistic about the control of asthma in patients, but that evaluation was quite often based on personal opinion and not supported by standardized tools. In all chronic diseases, adherence to treatment is crucial to achieve the best results, but difficult to achieve and monitor in the long term. In this case, however, the level of adherence was extremely overestimated when compared with the drug possession data derived from national registries. Of course, all surveys performed by questionnaires administered online, and without any objective measurement, may be affected by an intrinsic weakness in defining event frequencies in a population using small sample sizes. However, clear and frequent communication between physicians and patients, their sharing of treatment objectives in an alliance relationship, and the measurement of the outcomes obtained using standardized tools are essential for improving the management of any chronic pathology. When a chronic disease has a high prevalence such as asthma, it seems reasonable to approach its treatment within a chronic disease management model conceptual framework [11–13]. This is probably not the case in Italy, where the management of asthma seems not to have improved much since the late 1990s [14, 15]. A result about which there were no substantial discrepancies between patients and physicians was the low frequency of use of the MART strategy for the treatment of asthma. Moreover, the MART strategy was often coupled to the use of a short-acting SABA as a second reliever, thereby completely distorting the logic underlying the MART strategy. It can be hypothesized that the low frequency of use of the MART strategy may be attributed to several causes: poor understanding of the method’s potential benefits, inadequate knowledge of the supporting scientific evidence, and patients’ failure to follow their doctor’s advice. Patients’ habit of having a medication available on demand, different from the maintenance therapy, may be a plausible explanation for the inappropriate prescribing of a SABA associated with the MART strategy. However, since the APPaRENT2 survey was carried out shortly after the clear indication of preference for the MART strategy in the GINA recommendations [2], we attempted to verify whether the low use of the MART strategy in Italy had changed after the survey date. Analysing the prescriptions of inhalers containing the combination of ICS/formoterol, which are the only ones that can be used for the MART strategy, 12 months before and 12 and 24 months after the publication of the GINA 2021 report, we found no relevant increase in their share compared with other ICS/LABA, as highlighted in Figure 1. On this basis, it is possible to hypothesize that the use of the MART strategy in Italy is still infrequent compared to the consolidated proactive regular treatment with ICS/LABA and SABA as a reliever of proven efficacy for the long-term treatment of asthma.
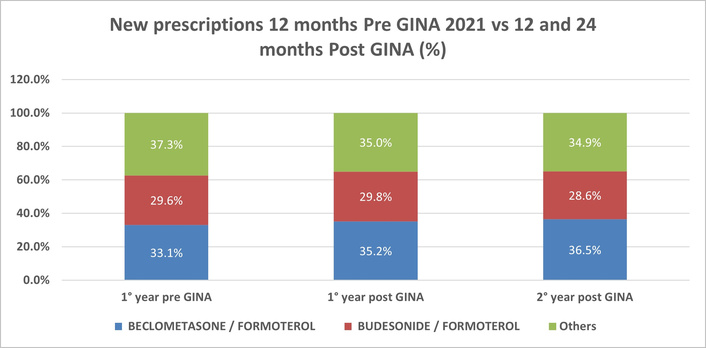
Percentage breakdown of inhaler prescriptions for new asthma patients 12 months before the publication of the GINA 2021 report, and 12 and 24 months after the publication of the GINA 2021 report. 1°: first; 2°: second; GINA: Global Initiative for Asthma.
The results of the APPaRENT2 study, as far as the Italian data are concerned, suggest the need for more effective communication between physicians and patients suffering from bronchial asthma. The sharing of results from standardized instruments such as the ACT or ACQ, administered before each visit, could be an essential tool for such communication. In fact, even in the presence of frequent and structured contacts, according to what was declared by the physicians, the patients had an unsatisfactory awareness of the severity of their disease and an optimistic evaluation of their clinical conditions, not aligned with their reporting of symptoms and limitations of daily living. The consolidated proactive regular treatment with ICS/LABA, and SABA when needed, appears to be the preferred strategy in patients with moderate, severe, or fluctuating severity asthma, despite being defined as a second non-preferential choice in GINA documents from 2021 onwards. Furthermore, the frequent co-prescription of the MART therapy with a SABA suggests there is some relevant misunderstanding of reliever strategies in the general practice and the need for a more effective diffusion of the new messages, from the specialist scientific societies to general practitioners, in Italy.
ACQ: Asthma Control Questionnaire
ACT: Asthma Control Test
GINA: Global Initiative for Asthma
MART: maintenance and reliever therapy
RP and DV: Conceptualization, Writing—original draft. FA and CD: Writing—review & editing. GWC: Supervision, Writing—review & editing. All authors read and approved the submitted version.
Giorgio Walter Canonica, who is the Editor-in-Chief of Exploration of Asthma & Allergy, had no involvement in the decision-making or the review process of this manuscript. GWC: reports research or clinical trials grants paid to his Institution from Menarini, AstraZeneca, GSK, Sanofi Genzyme, and fees for lectures or advisory board participation from Menarini, AstraZeneca, Celltrion, Chiesi, Faes Farma, Firma, Genentech, Guidotti-Malesci, GSK, HAL Allergy, Innovacaremd, Novartis, OM Pharma, Red Maple, Sanofi-Aventis, Sanofi-Genzyme, Stallergenes, and Uriach Pharma. RP: former employee and now consultant of GSK. DV: employed by GSK, holds financial equities in GSK. FA: ing and anonFormer employee in GSK. CD: fees for board participations, educational events, consulting fees, presentations from GSK, Menarini, Novartis, Astrazeneca, and Neopharmed.
Since this study was a secondary analysis conducted on an already existing and anonymous database, further submission for review is not required according to the local ethics committee.
Since this study was a secondary analysis conducted on an already existing and anonymous database, informed consent to participate is not required according to the local ethics committee.
Not applicable.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
The APPaRENT2 study was funded by Glaxo Smith Kline (GSK study [214325]). The founder had no role in the design of this study, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2026.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 982
Download: 23
Times Cited: 0
