Review
Review

Affiliation:
1Department of Neurology, Faculty of Medicine, Selcuk University, Konya 42100, Turkey
Email: dreren42@hotmail.com
ORCID: https://orcid.org/0000-0001-6834-0827
Affiliation:
2Clinic of Neurology, Dr. Ersin Arslan Education and Research Hospital, Gaziantep 27010, Turkey
ORCID: https://orcid.org/0000-0002-9482-6203
Affiliation:
3Clinic of Neurology, Konya City Hospital, University of Health Sciences, Konya 42050, Turkey
ORCID: https://orcid.org/0000-0002-5444-9837
Affiliation:
3Clinic of Neurology, Konya City Hospital, University of Health Sciences, Konya 42050, Turkey
ORCID: https://orcid.org/0000-0001-7755-9409
Affiliation:
1Department of Neurology, Faculty of Medicine, Selcuk University, Konya 42100, Turkey
ORCID: https://orcid.org/0000-0003-3619-2174
Explor Neuroprot Ther. 2022;2:162–173 DOI: https://doi.org/10.37349/ent.2022.00026
Received: May 11, 2022 Accepted: May 31, 2022 Published: August 22, 2022
Academic Editor: Brandon Lucke-Wold, University of Florida, USA
The article belongs to the special issue Emerging Concepts in Subarachnoid Hemorrhage
Delayed cerebral ischemia after subarachnoid hemorrhage is one of the most important causes of mortality and poor functional outcome in patients. Initially, the etiology and treatment of delayed cerebral ischemia focused primarily on cerebral vasospasm. However, recent studies have detected that depolarization, microcirculation, and autoregulation disorder, which spreads together with cerebral vasospasm, also play a role in the etiology. The main treatment strategies in the prevention and treatment of delayed cerebral ischemia are the regulation of blood pressure and the use of calcium channel blockers, especially nimodipine. The main step in the early diagnosis and treatment of the disease is to monitor the neurological clinical status. In addition to transcranial Doppler ultrasonography, computed tomography, or magnetic resonance imaging angiography, continuous electroencephalography and invasive brain multimodal examination may be required in the follow-up period of the disease. In addition to blood pressure regulation, optimization of cardiac output, endovascular interventions, angioplasty, and/or intra-arterial vasodilator infusion are other treatment methods. This review aimed to evaluate delayed cerebral ischemia, one of the most important complications of subarachnoid hemorrhage, in the light of current literature.
Subarachnoid hemorrhage (SAH) is a serious cerebrovascular disease with high mortality and morbidity [1]. Headache is the most common symptom; and post-SAH headache is associated with many factors such as age, analgesia, and sodium levels [2]. Delayed cerebral ischemia (DCI) is defined as a regression in the level of consciousness with a developed neurological deficit or the emergence of new ischemia findings in the affected brain region by radiological techniques [3]. Aphasia, hemianopia, hemiparesis, and neglect may accompany focal neurological findings. However, other than these, many neurological clinical symptomological findings may accompany this process [4]. Although DCI occurs in 30% of SAH patients, it produces cognitive dysfunction, poor quality of life, and varying degrees of motor deficits in most surviving patients [5].
The neurovascular response is a process of endothelial disruption and is significant in its association with DCI following SAH. Endothelial disruption is induced by microvascular inflammatory factors and is intimately involved in the progression of DCI. Numerous immune cells including neutrophils, monocytes, and glymphatic system have an important role after SAH. Glymphatic vessels can become blocked after SAH likely due to microthrombosis and hemorrhagic degradation products [6]. The classic information has been that large vessel vasospasm primarily contributes to DCI, but a recent study is detected that glymphatic blockage can increase the inflammation and microspasm [7]. This leads to the initiation of spreading cortical depolarization, increasing the intracerebral pressure (ICP) and the induction of DCI [8, 9].
DCI after SAH is a dynamic process that starts to emerge especially on the 3rd–4th days and reaches its maximum level in the 7th–8th days. It may occur as late-onset DCI, although sometimes less frequently, towards the end of the second week. However, despite all this dynamic process, it is expected to recover from the 21st day after SAH [10, 11]. In approximately 70% of patients with SAH, vasospasm is detected with transcranial Doppler ultrasonography (TCD) or digital subtraction angiography (DSA) on the 4th to 12th day of SAH. However, it is controversial whether this is a natural process of the disease or a pathological condition. It is more accurate to judge the importance of cerebral vasospasm together with clinical neurological evaluation [12, 13]. Because DCI occurring in some of these patients is associated with increased neurological disability and mortality [14].
Treatment in the neurological intensive care unit affects the prognosis of DCI positively. To prevent the development of DCI and improve its prognosis, the underlying etiological factors should be recognized. Evidence-based scientific methods should be applied to prevent the development of DCI. Intervention should be made before the ischemic process progresses with early diagnosis methods [15, 16]. Neuromediators such as interleukin 6 and many neuroradiological diagnosis methods are used for early diagnosis of cerebral vasospasm [15–17]. In this review, we planned to make an assessment to provide optimum care with DCI management.
DCI may develop in approximately 30% of SAH patients. However, detecting this condition depends on access to neuroimaging methods and detailed evaluation of the neurological examination. In some patient groups, although there is no significant radiological finding of vasospasm with neuroimaging methods, DCI can be detected with clinical and neurological examination. Current studies show that age, high neurological disability, female gender, increased blood volume in the subarachnoid area, and diabetes mellitus are associated with poor prognosis. Patients with these characteristics have also been at a higher risk for the development of DCI [18].
The main clinical features of DCI after SAH are neurological focal deficits, impaired consciousness at different levels, and fluctuations. If the DCI process is thought to occur as a result of SAH, increased body temperature and white blood cells can be detected. These findings support the diagnosis of DCI. However, other possible causes must be ruled out before a diagnosis of DCI. It is important to demonstrate that encephalopathy is not caused by any other factor. In particular, systemic disorders such as hypotension and hypoglycemia, and local or systemic infective disorders should also be evaluated [19, 20]. The increased neurological deficit as a result of all these evaluations supports the diagnosis of DCI and also contributes to the increase in mortality. Therefore, even if neuroimaging is normal, patients should be evaluated in detail with periodic neurological examinations.
It is essential to provide SAH stabilization and hemorrhage control. For this, the blood pressure must first be stabilized at the beginning. Before detection and treatment of the hemorrhage, systolic blood pressure should be kept below 160 mmHg. After hemorrhage control, the target systolic blood pressure should be kept between 140–220 mmHg. Antihypertensive treatment options that should be preferred in particular are nicardipine or labetalol [21–24].
Nimodipine, a calcium channel blocker of the dihydropyridine group, is one of the major treatments that prevent the progression of vasospasm. There are studies detecting that 60 mg oral nimodipine administered at 4-hour intervals for 21 days after SAH reduces poor functional outcomes and mortality [10–12, 21]. Although intravenous nimodipine is also used in the treatment regimen in some countries, the main current treatment is oral nimodipine. This treatment should be administered at 30 mg every 4 h in patients at risk of hypotension [21].
Hemorrhagic materials may induce vasospasm after SAH. Many studies have been carried out to ensure the elimination of the blood in the subarachnoid area. It is thought that this situation may reduce cerebral vasospasm. Randomized controlled trials evaluating the efficacy of intraoperatively administered tissue plasminogen activator (tPA) treatment could not demonstrate efficacy [22]. There are different results on lumbar drainage of cerebrospinal fluid (CSF), cisternal irrigation, and the efficacy of urokinase [23, 24]. Therefore, there is insufficient evidence for the routine use of these treatments.
Excessive natriuresis and inappropriate antidiuretic hormone (ADH) syndrome that develops after SAH results in hyponatremia and hypovolemia. This occurs frequently after SAH and has been associated with increased DCI [25]. Studies have reported that fluid restriction, which is the treatment of inappropriate ADH syndrome, may induce DCI status. Therefore, fluid restriction is not recommended in the treatment of this disease [26]. Isotonic crystalloid treatment should be administered to maintain normovolemia and normal serum sodium levels. Fludrocortisone implementation (0.2–0.4 mg/day) has been reported to reduce hyponatremia and treat DCI. However, its effect on cerebral ischemia and functional improvement has not been demonstrated [13, 27]. There is anecdotal evidence that treatment of symptomatic hyponatremia with hypertonic saline (3%) is effective [13].
As a result of studies performed after SAH, the efficacy of some treatments has been demonstrated and they have been reported to prevent DCI [12]. These treatment strategies and features are summarized in Table 1.
The prevention of DCI after SAH
| Parameters | Explanation |
|---|---|
| BP, after hemorrhage control | SBP 140–220 mmHg |
| Antihypertensive treatment | Nicardipine or labetalol |
| ICP control | Osmotic treatment and/or EVD |
| Osmotic treatment | Hypertonic saline or mannitol |
| Targeted hemoglobin level | More than 9 mg/dL |
| Intravenous solution treatment | Isotonic solutions are used for euvolemia |
| Oral nimodipine treatment | 30 mg every 2 h (no risk of hypotension)Reduced to 30 mg every 4 h (risk of hypotension) |
| Avoided parameters | HyperglycemiaHyperthermiaDehydrationHypoxiaHypocapnia |
BP: blood pressure; SBP: systolic blood pressure; EVD: external ventricular drainage
Many experimental and clinical studies have been organized for prevention of DCI after SAH. Some of these have been reported to be effective. However, the effectiveness of most of them has not been demonstrated clearly. It has been reported that aspirin, one of the antiaggregant treatments, has no effect on neurologic disability and prevention of new lesion development [28]. Similarly, the effect of enoxaparin on the development of DCI or the Glasgow outcome scale (GOS) at the 3 months has not been demonstrated [29]. Magnesium, nicardipine, and statins have no effect on clinical improvement [30–32]. No effect of prophylactic hypervolemia and angioplasty on new neurological deficits or GOS was detected [33, 34]. Some treatment options studied on the development of DCI after SAH are listed in Table 2.
Non-protective treatment options in DCI after SAH
| Treatments | Explanation |
|---|---|
| Aspirin | Not effective on new lesion |
| Enoxaparin | Not effective on DCI |
| Magnesium | Not effective in mRS at 3 months |
| Nicardipine | Not effective on neurological state at 3 months |
| Statins | Not effective on DCI and mRS at 3 months |
| Prophylactic hypervolemia | Not effective on neurological state at 3 months |
| Prophylactic angioplasty | Not effective on neurological state at 3 months |
mRS: modified Rankin Scale
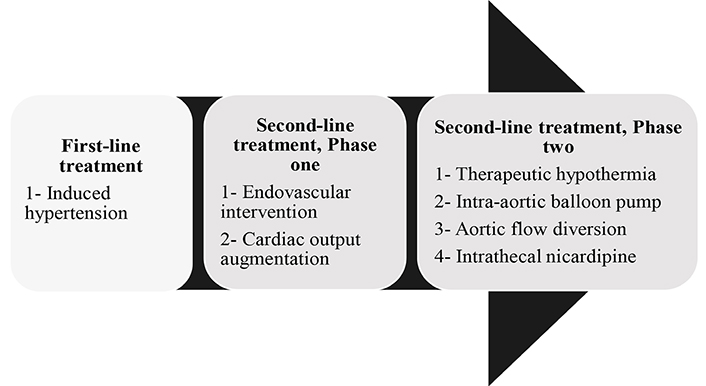
SAH after DCI is a complex status. Therefore, the follow-up of these patients in specific centers working on neurological intensive care contributes significantly to the prognosis [35]. In addition to the fact that the treatment of the disease varies according to patient-based individual criteria, a stepwise treatment approach is also recommended [13]. These are divided into 2 groups as first-line and second-line treatment approaches. At the same time, second-line treatment is further divided into two subgroups as step-one and step-two. The stepwise treatment approaches to the development of DCI after SAH and the characteristics of these steps are summarized in Figure 1. These treatments are applied systematically. DCI associated with SAH is treated with first-line treatments and after second-line treatments in stages.
In many case series and clinical observations, it has been reported that induced hypertension contributes to the success of treatment and reduces disability and mortality in patients with SAH. The use of vasopressors to induce hypertension is the major primary approach to prevent the development of DCI. Primarily, a bolus of normal saline solution (15 mL/kg over 1 h) increases cerebral blood flow (CBF) [36]. Hypertension induced by norepinephrine [37], phenylephrine [38], or dopamine [39] has been reported to improve CBF and/or cerebral oxygenation and reduce neurological disability in the patients with major disability. Norepinephrine is preferred in first-line treatment because of its alpha and beta agonistic effect and absence of significant tachycardia. Arginine-vasopressin has also been reported to be a safe agent in patients with SAH [40]. Although the target blood pressure in patients varies according to the basal blood pressure level, the systolic blood pressure is usually aimed at 160 mmHg to 180 mmHg.
Most centers use a maximum target value of approximately 120 mmHg for cerebral perfusion pressure, 140 mmHg for mean arterial pressure, and 220 mmHg for systolic blood pressure. However, patients should be closely monitored for complications such as heart failure. The safety of induced hypertension in patients with non-ruptured aneurysms has been confirmed by recent studies [41]. There is insufficient data in the literature on the duration of treatment, reduction, and discontinuation of these treatments for induced hypertension. It is recommended to gradually reduce the treatment after at least 24–48 h of stable neurological status, with close monitoring of the neurological clinical process.
Cerebral monitoring of patients is recommended before second-line treatment. However, it is also used before first-line treatment and to evaluate prognosis. Monitoring of cerebral vascular spasm in patients with SAH has an important factor in predicting for prognosis of DCI and treatment planning. Some methods are used to monitor this process. Computed tomography (CT) angiography, magnetic resonance imaging (MRI) angiography, CT or MRI perfusion studies are some of these methods. Although these imaging methods allow the monitoring of the disease quite successfully, they are impractical in daily routine. These tests can be used specifically to evaluate moderate or severe vasospasm [42]. Evaluation of vasospasm with TCD can provide very useful and practical information. The advantages of this examination and evaluation are primarily that it is non-invasive and easily accessible. In addition, it allows to be followed at certain periods together with bedside installation. Therefore, TCD is an important imaging method in the follow-up of vasospasm. However, this method also has some problems in sensitivity and specificity. It is very useful for this purpose in the neurological intensive care unit. However, it does not contribute to the solution of all problems encountered. Diagnosis of vasospasm may vary according to the clinician’s experience in this area, localization and severity of vasospasm, anatomical features and variations of vascular structures, characteristics of the anatomical window, severity of increased intracranial pressure, fluctuation of vascular structures, and hematological variables. A negative diagnosis of vasospasm after the tests does not definitively exclude the disease [42–44].
Although the frequency of follow-up of vasospasm with TCD varies according to the clinical condition of the patients and the progression of the disease, it is recommended daily or every other day. However, daily TCD follow-up is recommended starting from the 3rd day after SAH. In measurements made over the middle cerebral artery (MCA), flow velocity is divided into 3 groups as 100–120, 120–200, and above 200 cm/s, and vasospasm is divided into 3 groups as mild, moderate, and severe [45]. Apart from this measurement, the internal carotid artery (ICA) flow velocity is also measured together with the MCA. It can be used in diagnosis and follow-up by calculating the MCA/ICA ratio. If this ratio is calculated as more than 3, it supports cerebral vasospasm. If this ratio is calculated above 6, it supports severe cerebral vasospasm. This ratio has been reported to have a very high sensitivity of 88.9% [44, 46]. In another study, the flow velocities ratios of the basilar artery and the vertebral artery in the extracranial area were evaluated. A ratio of basilar artery and vertebral artery flow velocity above 2 supports cerebral vasospasm [47].
The European Society of Intensive Care Medicine and Neurocritical Care Society recommends the use of multimodal imaging modalities [ICP, partial brain tissue oxygen (PbtO2), and interstitial fluid microdialysis] in patients at risk for DCI and ischemia after SAH [48]. The evidence of CBF monitoring is insufficient. Monitoring probes are inserted through a multi-lumen placed in a single burrhole through the skull. Intracortical electroencephalography recordings can be performed in the same multi-lumen bolt. These recordings are more sensitive for the detection of seizures and ischemia. It provides more information about cortical depression [49, 50].
Endovascular treatment is not the phase-one treatment for all DCI patients. Although hemodynamic stabilization is provided, neurologic deficits may progress in some SAH patients. It may be necessary for endovascular treatments, especially in patients whose clinical disability progresses despite the medical treatments [51]. In recent years, studies have increased even more with the rapid development of endovascular treatments and the increase in the number of centers applying this treatment. Endovascular intra-arterial treatments should be applied, especially in cases of heart failure, myocardial ischemia, and other complications [52]. Endovascular intra-arterial treatments are divided into two subgroups. These are mechanical dilatation and infusion of intra-arterial vasodilator medications. Mechanical dilatation is the mechanical relaxation of vasospastic vessels involved in the etiology of DCI by percutaneous transluminal balloon angioplasty (PTCA). This technique is particularly applied to cerebral proximal vessels, including segments of the internal carotid artery, vertebral, basilar, MCA M1-M2, anterior cerebral artery (ACA)-A1, and posterior cerebral artery (PCA)-P1. In many case series, the treatment success rate is over 90% [53]. However, in some cases, there is a possibility of recurrent vasospasm and endovascular treatments may be required again and again [54]. Early endovascular treatments, particularly within the first two hours after the onset of neurological progression, have been associated with a better prognosis [55]. However, since this is an invasive treatment method, it has a complication rate of about 5%. These complications are distal embolism, thrombosis, dissection, and vascular rupture. The mortality of all these complications is also quite high [34]. However, despite all these risks, PTCA is an important and effective treatment option in patients with neurological progression and cerebral ischemia.
Many case series have demonstrated that cerebral vasospasm can be treated with intra-arterial vasodilator treatments. Many agents, especially verapamil, papaverine, milrinone, nicardipine, nimodipine, fasudil, and amrinone, have been used for this treatment. However, these agents have not been tested in a large-scale, prospective, and case-control study. Compared to PTCA, intra-arterial vasodilator therapies have many advantages. In particular, it has a better distal penetration and safety profile. However, this treatment also has some complications. Some of these are recurrent vasospasm, increased intracranial pressure secondary to vasodilation, and systemic hypotension due to the short duration [56]. The most common treatments in clinical practice are intra-arterial nicardipine or verapamil [57]. More often, after PTCA is applied to the proximal vessels, a combination of intra-arterial vasodilator treatment is applied to the distal vascular structures.
Observational studies about endovascular treatment after SAH are very important. Because the results of observational studies define the mechanisms and provide impetus to future research [58]. Clot removal after SAH is another important treatment method. Kanat et al. [59, 60] and Yolas et al. [61] reported that this treatment method is effective in the experimental studies. However, they stated that there is insufficient evidence for the use of this treatment in routine clinical practice [59–62]. More and multicenter studies are needed about clot removal as a treatment option after SAH.
Increasing cardiac output with fluid infusion and positive inotropic agents can normalize cerebral perfusion by reducing the DCI after SAH [63]. Induction of cardiac output with dobutamine can increase cerebral perfusion by 50% compared with phenylephrine [38]. Milrinone has a more effective inotropic agent than dobutamine in myocardial stupor induced by SAH-induced beta-receptor desensitization [64]. In a published case series, milrinone has been reported to regulate cerebral microcirculation and be effective on DCI [65]. Some authors and clinicians state that the administration of treatment to increase cardiac output should be in the phase-two treatment option rather than the phase-one. In particular, transpulmonary thermodilution or pulmonary artery catheterization, which objectively tests cardiac output, is recommended [66].
If clinical neurological disability continues to progress despite all treatments, it may be necessary to use these treatment options. These treatments should be applied especially in appropriate centers with monitoring and in intensive care conditions. Hypertonic fluid infusion has been reported to improve CBF in some patients with higher disability and poor consciousness [67]. If DCI and increased intracranial pressure coexist in SAH patients, this treatment option should be considered. Increased body temperature is associated with poor prognosis and increased mortality in SAH. Therefore, hyperthermia control should be provided. It should be aimed to maintain body temperature between 33°C and 35°C with or without barbiturate [68]. Mild therapeutic hypothermia is protective in SAH [69]. Despite such a recommendation, there is not sufficient scientific evidence on the efficacy and safety of this treatment. Some experimental studies have been carried out on this subject. Intra-aortic balloon pump (IABP), aortic flow diversion (AFD), and intrathecal nicardipine are some of these experimental studies. Aortic flow manipulation is an interventional treatment method that aims to increase CBF by partially reducing the directing of some of the cardiac output to the descending aorta. With this method, cerebral perfusion and microcirculation can be increased [70]. This treatment is still under investigation and there is insufficient data for using routine clinical practice. It has also been demonstrated that intrathecal nicardipine administered via an intraventricular catheter, as an endovascular interventional treatment method, is also effective within 8 h of treatment and may be a treatment option in the treatment of resistant DCI [71]. Similarly, intrathecally administered nitroprusside is thought to be a treatment option for resistant vasospasm [45]. These treatment options can also be the latest treatment method for DCI [72].
It has been revealed that DCI is the leading factor that correlates the clinical process with poor prognosis and contributes to mortality in SAH patients. Treatment options with efficacy and safety in the light of literature data are nimodipine treatment and normovolemia with appropriate fluid treatment. Neurological examination may be sufficient in patients with stable clinical status in DCI follow-up after SAH. However, multimodal-imaging methods should be preferred for predicting the prognosis and planning the treatment, especially before second-line treatment. Appropriate treatment options with early diagnosis play a key role in treatment. Among the first-line treatment options, induced hypertension should be preferred first. Second-line treatment, which is the next step of treatment, is divided into two subgroups as phase-one and phase-two treatments. The phase-two treatment consists of endovascular treatments and augmentation of cardiac output. Although clinicians do not have enough data to apply the second-line treatments in routine clinical practice, second-line treatments can be applied to patients who do not respond enough to all first-line treatment options. The pathophysiology of DCI in SAH patients has complex features. In particular, impaired autoregulation, diffuse depolarization and neuro-inflammation due to microcirculation disorder form the basis of this pathophysiological process. This pathophysiological understanding will pave the way for the development of new treatments. Especially with the rapid development of technology, the use of newly developing imaging methods will allow to have more information about DCI. However, considering that there is a patient group in which current treatment methods may be insufficient, the investigation of the pathophysiological process and treatment options continues.
AFD: aortic flow diversion
CBF: cerebral blood flow
CO: cardiac output
DCI: delayed cerebral ischemia
ICP: intracerebral pressure
MCA: middle cerebral artery
PTCA: percutaneous transluminal balloon angioplasty
SAH: subarachnoid hemorrhage
TCD: transcranial doppler ultrasonography
FE: planning, organization, writing, and editing. ATY, SEY, AD, CO: planning, writing, and editing. All authors contributed to manuscript revision, read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2022.
Copyright: © The Author(s) 2022. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Eric J. Panther, Brandon Lucke-Wold
Stephan Quintin ... Brandon Lucke-Wold
Gonçalo Januário
Andrés Ricaurte-Fajardo ... Nathalia Melo Gonzalez
Mohammed A. Azab ... Brandon Lucke-Wold